Embed Size (px)
DESCRIPTION
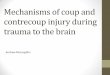
Case studies in neuro trauma. Goals. Brief anatomy review Discuss important exam findings in brain and spine trauma Discuss key management principles in brain and spine trauma Case study of Epidural Hematoma Case study of Diffuse Axonal Injury Case study of Cervical Spinal Cord Injury. - PowerPoint PPT Presentation
Citation preview

Saving Lives By Strengthening Our Region’s Trauma Care System
December 5, 2013 KELLI CASPER, APNP
CASE STUDIES IN
NEURO TRAUMA

GOALS
• Brief anatomy review• Discuss important exam findings in brain and
spine trauma• Discuss key management principles in brain and
spine trauma• Case study of Epidural Hematoma• Case study of Diffuse Axonal Injury• Case study of Cervical Spinal Cord Injury

ANATOMY REVIEW




TRAUMATIC BRAIN INJURY
• A traumatic brain injury occurs every 7 seconds and results in death every 5 minutes in the US
• TBI accounts for 1/3 of all trauma related deaths in the US
• Annual cost of TBI medical care in the US – approximately $56 billion
• (Heegaard & Biros, 2007)

MANY “FLAVORS” OF BLUNT TBI
• Skull fractures• Brain contusions• Hematomas/Intracerebral hemorrhages• Epidural Hematoma• Subdural Hematoma• Traumatic SAH• Diffuse axonal injury

CATEGORIZING HEAD INJURY
Minimal: GCS= 15, No loss of consciousness, No amnesia
Mild: GCS= 14 OR GCS= 15 plus EITHER: Brief LOC < 5 min OR impaired alertness or memory
Moderate: GCS 9-13 OR LOC > 5 min OR Focal neurologic deficit
Severe: GCS 5-8
Critical: GCS 3-4
(Greenberg, 2010)

TBI PATHOGENESIS
• Primary injury: immediate impact injury• Secondary injury: ensuing neuropathologic processes after
initial injury
Our job in the hospital is to intervene and disrupt these processes and secondary mechanisms

SECONDARY BRAIN INJURY
Amino acid and cytokine release
Free radicals formed
Mitochondrial damage
BBB damageAltered CBF
Increased ICP
Brain damage/cell deathFunctional deficits

INTERVENING FACTORS IN TBI
• Hypoxia• Hypotension• Cerebral edema• Increased ICP• Reduced cerebral blood flow• Electrolyte imbalance

PRACTICE GUIDELINE DEFINITIONS• Level I: High degree of clinical certainty• Level A: Based on consistent Class I evidence (well-designed, prospective
randomized controlled studies)
• Level B: Single Class I study or consistent class II evidence when circumstances preclude clinical trials
• Level II: Moderate degree of clinical certainty• Level C: Usually derived from Class II evidence (one or more well-designed
comparative clinical studies or less well-designed randomized studies) or a preponderance of Class III evidence
• Level III: Unclear clinical certainty• Level D: Generally based on Class III evidence (case series, historical controls,
case reports and expert opinion). Useful for educational purposes and to guide future research
• (Greenberg, 2010)

CASE STUDY #1
• 51 y/o male fell down a flight of cement stairs after domestic altercation striking the left temporal area. Lost consciousness for about 10 minutes.
• By the time EMS arrived, the patient was fully awake. He was brought to the ED for evaluation. GCS 15 in ED. CT scan without contrast of head showed a small left temporal epidural hematoma and left temporal bone fracture.

EPIDURAL VS SUBDURAL HEMATOMAS
Epidural• 1% of head trauma
admissions• Arterial source (MMA)
(85% of cases)• Can expand rapidly• More often requires
surgical evacuation• Mortality 20-55%• “Classic presentation”
Subdural• Seen in 10-20% of head
trauma cases• Usually venous source of
bleeding (bridging veins)• Usually expand less rapidly
than EDH• More often has associated
underlying brain injury (contusions, SAH)

• Epidural: Usually produces more “mass effect”• Subudural: Usually more diffuse and concave
appearance



Small epidural hematoma (< 1 cm maximum thickness)

CASE STUDY #1
• Patient was admitted to ICU for observation• EDH can rapidly expand• Moderate head injury
• Neuro checks every hour• HOB elevated 40 degrees• NPO status• Seizure prophylaxis started
• Temporal region associated w/higher seizure risk
• Minimize sedation!• Avoid hypertension

UNFOLDING EVENTS
• Overnight becoming increasingly agitated followed by increasing somnolence and difficulty arousing• Thrashing of left extremities only• No longer following commands and not speaking• Left pupil 5mm and fixed, Right pupil 2mm, responsive to
light• Neurosurgeon being called• Patient declined rapidly, developing respiratory distress• Rapid response called and patient emergently intubated• OR was called for emergent craniotomy and evacuation of
hematoma.

DISCUSSION OF EVENTS
• Agitation/Restlessness is often first sign of increasing ICP• Somnolence and hemiparesis will follow as ICP
continues to rise• Pupil dilates (late sign)


TREATMENT COURSE
• Surgical evacuation via Craniotomy with evacuation of EDH
• He eventually regained consciousness and able to ambulate and use right hand

CASE STUDY #2
• 47 y/o male in MCA on highway, lost control, no helmet, thrown from motorcycle. Unresponsive at scene, CPR initiated
• Intubated at scene, arrived to ED GCS 3, chemically paralyzed and sedated.
• Neuro exam very limited

DIFFUSE AXONAL INJURY

INITIAL PERTINENT CLINICAL INFORMATION
• SBP on admit to ICU 140’s. MAP 80’s.• Pupils unequal, R= 4mm, reactive to 2mm,
L= 8mm, non-reactive to light.• Sodium: 141• H/H: 13.3/38.8• Platelet: 227,000• PCO2 = 37, PO2 = 129

INITIAL TREATMENT COURSE
• Arterial line inserted. Central line inserted.• HOB elevated 40 degrees• Sedated with propofol / fentanyl drips• Loaded with Cerebyx (Fosphenytoin) 20 mg PE/kg, then TID• ICP bolt placed by Neurosurgeon. Initial ICP’s 7-9mm Hg.
CPP 60’s• Mannitol 25 gm IV every 6 hours started• Stress ulcer prophylaxis, Protonix 40 mg IV daily• Bilateral SCD’s placed for DVT prophylaxis• Serum electrolytes / osmolality q 6 hrs

DISCUSSION OF TREATMENT• ICP monitoring & goals• CPP monitoring & goals• Sedation goals• Mannitol treatment• 3% saline treatment• DVT prophylaxis• Stress ulcer prophylaxis (SUP)• Nutrition goals• Refractory increased ICP• Barbituate coma• Decompressive Craniectomy

TYPES OF ICP MONITORING DEVICES
Goal ICP < 20

CEREBRAL PERFUSION PRESSURE
• Importance of Cerebral Perfusion Pressure• CPP = Mean arterial pressure (-) Intracranial
pressure• Goal > 60 mm Hg, prefer > 70 mm HG

MANNITOL(LEVEL II RECOMMENDATION FOR INTRACRANIAL HTN AFTER SEVERE TBI)
Pro’s• Increases cerebral blood
flow by it’s plasma expansion and osmotic effect
• Reduces ICP within minutes
• Possible free radical scavenging
• (Greenberg, 2010)
Con’s• Risk of acute renal
failure• Risk of hypotension• May draw more fluid into
CNS causing worsening cerebral edema
• Electrolyte disturbances due to excessive urinary output

HYPERTONIC SALINE
Pro’s• Effective at reducing ICP
through osmotic effects similar to Mannitol
• Less risk of hypovolemic hypotension
• (Greenberg, 2010)
Con’s• May cause severe
hypernatremia• Electrolyte disturbances• Not enough convincing
evidence to support use over Mannitol
• No changes in neurologic outcome over Mannitol

SUPPORTIVE CARE
• Sedation / Pain management• Nutrition• Stress Ulcer prophylaxis• DVT prophylaxis• Skin care• Oral hygiene

CONTINUED HOSPITAL COURSE• IVC filter placed (DVT risk with ICH)• Percutaneous bedside tracheostomy placed, dobbhoff placed for
nutrition• Required a few days of Levophed for goal CPP > 60• ICP’s remained relatively normal• Gradually began to open eyes, and although not commanding,
localized purposefully to stimulus• ~ 12 days post-injury, nodding to questions, trying to mouth
words, began sitting on edge of bed• ~ 18 days post-injury, speaking more sense, less agitation,
progressing in PT/OT/Speech, trach removed• Discharge to a brain rehab facility ~ 3 weeks post-injury

SPINAL CORD INJURY
• 12,000 new cases each year• Average age at time of injury ~ 40 years
• 77% of these are males
• $4 Billion spent annually on acute and chronic care of spinal cord injured patients
• (Chittiboina, et al. 2012)

CAUSES OF SCI
Cause%
MVC'sFallsViolenceOther/unknownSports
(Chittiboina, et al. 2012)

CASE STUDY #3
• 22 y/o male dove into shallow lake. Friends pulled him out of water, patient unable to move arms or legs. In ED, cervical CT scan showed at C7 burst fracture.

CT CERVICAL SPINE

MRI CERVICAL SPINE

INITIAL NEUROLOGICAL EXAM
• Alert and oriented with normal speech• CN II – XII grossly intact• Motor exam showed preserved biceps 3+/5,
triceps 2/5 bilaterally, Hand intrinsics absent on right side, subtle finger movement on left side
• No motor or sensory perception below C7• + priapism

DISCUSSION
• “Level of Injury”• “Complete Injury vs Incomplete Injury• Spinal shock

LEVEL OF INJURY
• Some use level of completely normal function
• Some use most caudal segment with motor function at least 3/5
• Know the major spinal nerve root motor distribution
• Know the major spinal nerve root sensory dermatomes

MAJOR SPINAL NERVE ROOT MOTOR DISTRIBUTIONSSegment Muscle Action to TestC1 – C4 Neck muscles
C3, C4, C5 Diaphragm Inspiration/FEV1
C5, C6 Deltoid, Biceps Abduct arm, Elbow flexion
C6, C7 Extensor carpi radialis Wrist extension
C7, C8 Triceps, Extensor digitorum, hand intrinsics
Elbow Extension, Finger Extension
L2, L3 Iliopsoas Hip flexion
L3, L4 Quadriceps Knee extension
L4, L5 Medial hamstrings, tibialis anterior
Ankle dorsiflexion
L5, S1 Lateral hamstrings, posterior tibialis, extensor hallucis longis
Foot inversion, great toe extension, ankle plantarflexion

MUSCLE STRENGTHGrade Strength0 No contraction
1 Flicker or trace contraction
2 Movement with gravity eliminated
3 Movement against gravity
4 Movement against resistance 4 – slight resistance 4 moderate resistance 4+ strong resistance
5 Normal strength

SENSORY DERMATOMES

DISCUSSING SPECIAL REFLEXES IN SCI
• Priapism• Cremasteric reflex• Anal cutaneous reflex (“anal wink”)• Bulbocavernous reflex

COMPLETE VS INCOMPLETE SCI
Incomplete lesion• Any residual motor or
sensory function more than 3 segments below the level of injury
• Sensation or voluntary movements in LE’s
• Preserved sensation around anus, voluntary rectal sphincter contraction
Complete lesion• No preservation of any
motor and/or sensory function more than 3 segments below the level of injury

SPINAL SHOCK
• Hypotension following spinal cord injury• Interruption of the sympathetics (implies
injury above T1)• Loss of vascular tone below level of injury• Leaves parasympathetics relatively unopposed causing a
relative bradycardia
• Loss of muscle tone results in venous pooling
• Blood loss from other associated wounds

TREATMENT COURSE• Cervical immobilization with rigid collar initially• Methylprednisolone drip started per protocol• Placed in cervical tongs by Neurosurgeon in ICU• Central/Arterial lines placed• Levophed drip used in ICU for maintaining SBP > 90• SCD’s for DVT prophylaxis• Foley catheter insertion• NPO• SUP: Protonix 40 mg IV daily• Anxiety & Pain control with small doses Ativan/Fentanyl as needed• Pre-operative readiness for surgical stabilization

CERVICAL TRACTION
• Level III recommendation• Purpose: to restore anatomic alignment• Complications:
• Skull penetration of pins• Reduction of cervical dislocations may cause neurologic
deterioration (i.e. retropulsed disc)• Higher level injuries (C1-C3) need caution (fragments
pulled toward canal)• Infection (Osteomyelitis) – good pin care is essential

SURGICAL STABILIZATION

HOSPITAL COURSE / OUTCOME
• Early physical and occupational therapies• Improving left hand intrinsics by POD 2• Transferred to a Spinal Cord Rehab facility
by POD 3

STEROID PROTOCOL IN SCI
• Still highly controversial• Considered Level III Recommendation• Asserted that beneficial (sensory & motor)
effects at 6 weeks, 6 months and 1 year are seen for both complete and incomplete injuries only if given within 8 hour of injury
• (Greenberg, 2010)

STEROID PROTOCOL
• Administration:• 16 Gm/256 ml bacteriostatic water• 30 mg/kg initial IV bolus over 15 minutes, followed by 45
minute pause, then maintenance drip at 5.4 mg/kg/hour x 23 or 47 hours**
• (Greenberg, 2010)

DVT PROPHYLAXIS IN SCILevel I Recommendation
Level II Recommendations
Level III Recommendations
* LMW heparin, rotating bed, adjusted dose heparin or some combination of these measures* Low dose heparin + pneumatic compression stockings or electrical stimulation
• Not recommended: low-dose heparin used alone
• Not recommended: oral anticoagulation alone
• Duplex doppler ultrasound, venography are recommended as diagnostic tests for DVT in patients with SCI
• Vena Cava interruption filters for patients who do not respond to or are not candidates for anticoagulation
*Titrate dose of SQ heparin q 12 hours to a PTT of 1.5 x control*Heparin 5000 units q 12 hours
(Greenberg, 2010)

EVALUATING STABILITY

TYPES OF VERTEBRAL FRACTURES

BRACING OPTIONS

REFERENCES• Blumenfeld, H. Neuroanatomy through Clinical Cases. Sinauer
Associates, Inc., Sunderland, Massachusetts; 2002.• Fix, J.D. Neuroanatomy. Lippincott Williams & Wilkins, 3rd edition, 2002.• Greenberg, M.S. Handbook of Neurosurgery. Thieme Publishing, 7th
edition, 2010.• Heegard, W. & Biros, M. (2007). Traumatic Brain Injury. Emergency
Medicine Clinics of North America, 25, 655-678.• Lindsay, K.W., Bone, I. & Callander, R. Neurology and Neurosurgery
Illustrated. Churchill Livingstone, 4th edition, 2004.• Ling, G. & Marshall, S. A. (2008). Management of Traumatic Brain Injury
in the Intensive Care Unit, Neurologic Clinics, 26, 409-426.• Chittibonia et al. (2012). Head and Spinal Cord Injury. Neurology Clinics,
30 (1), 241-276.











![[PPT]INTRODUKSI NEURO IMAJING - CARDIO | … · Web viewAbdomen : obstruction--- small, large bowel. perforasi . trauma --- blunt/ penetrating . Extremitas : Atas dan bawah ; Trauma---](https://img.dokumen.tips/doc/110x75/5aee43787f8b9a6625912bcc/pptintroduksi-neuro-imajing-cardio-viewabdomen-obstruction-small.jpg)
















