Embed Size (px)
Citation preview

AAIM Audio Series
Gordon R Cumming MD, FRCPC, FACC
moderator: Marianne E Cumming MSc, MD
March 5, 2014
Case studies: congenital heart
disease

2
Table of Contents / Agenda
Coarctation of the aorta
Ventricular septal defect
Tetralogy of Fallot
Transposition of the Great Arteries
Select short cases
historical treatment
optimal treatment today
favorable / unfavorable factors
optimal testing/information for underwriting
long-term complications
long-term outcome, challenges with limited data
future considerations
3
Congenital heart disease: considerations

Coarctation of the aorta
repair at age 6 (1979)
operative report not obtained
BMI 32.5 kg/m2, treated BP and lipids
Rx lisinopril, simvastatin
BP: 130's/80's throughout APS
majority measured with left arm or unspecified
No exercise stress test in file
Current cardiac MRI and chest MRA performed
4
Case 1: 41 year old male, life insurance
applicant
5
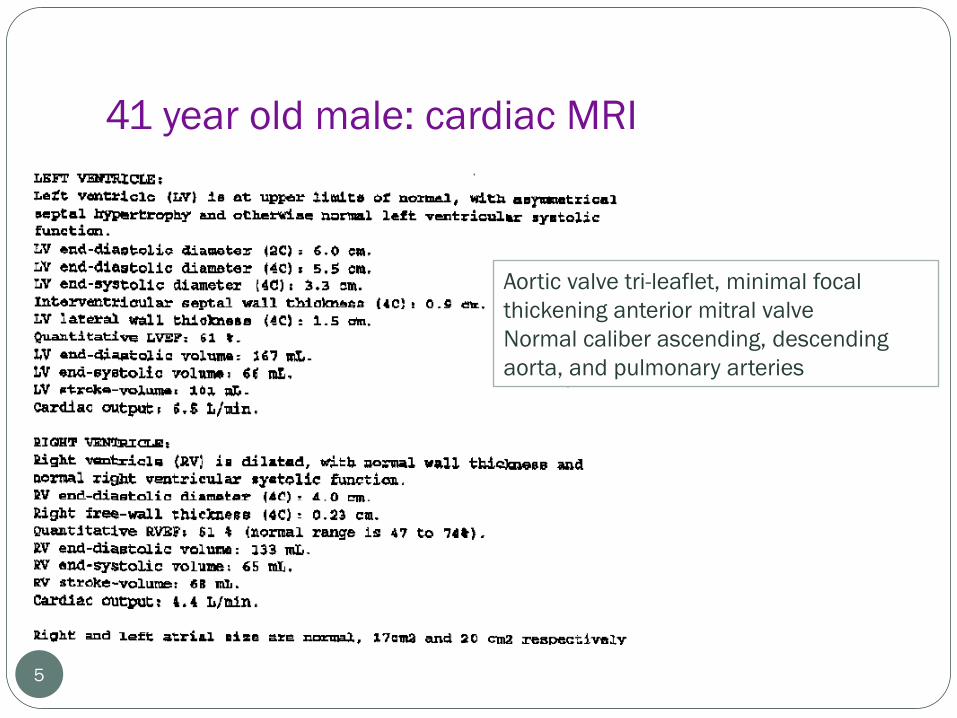
41 year old male: cardiac MRI
Aortic valve tri-leaflet, minimal focal
thickening anterior mitral valve
Normal caliber ascending, descending
aorta, and pulmonary arteries
6
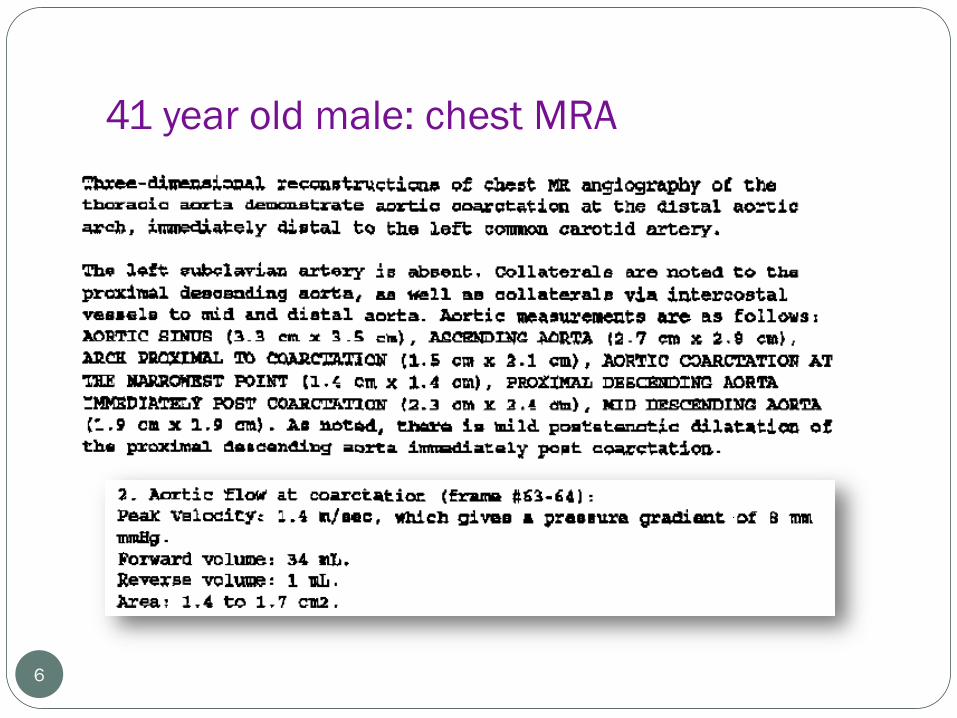
41 year old male: chest MRA

Ventricular septal defect
1964 – Pulmonary banding
1968 - VSD repair (age 4)
No current cardiac evaluation despite recent
cervical spine surgery
APS: "Heart - normal", BPs <120/<80, BMI 24
Agent:
Applicant:
7
Case 2: 49 year old male, life insurance
applicant

Standard of care, 1960's for large VSD
pulmonary artery banding followed by definitive repair age 4
Patient selection in 1960's
Potential long-term complications:
residual pulmonary artery narrowing, possibly elevated RV
pressures
aortic regurgitation or sub-aortic stenosis
arrhythmias
Ideal current follow-up:
resting EKG, Holter, exercise stress test, echocardiogram
VSD standard of care in 2014:
8
49 year old male, VSD
Case 3: 39 year old male, life insurance
applicant
9
Tetralogy of Fallot (TF) was an incidental finding
hospitalized at Johns Hopkins 1977 (age 3) for severe
burn
patch VSD closure with no outflow patch
EKG: complete RBBB, QRS .13; Holter and exercise
EKG: no ectopy
Echocardiogram:
mild-moderate RV enlargement, RVSP 26
moderate pulmonary and mild-moderate tricuspid
regurgitation
no outflow tract obstruction, aortic root 3.8, small PFO

Tetralogy of Fallot; anatomic details
10
Ventricular septal defect (VSD), large*
Right ventricular (RV) outflow obstruction*
Anterior displacement of aorta (overriding aorta)
Right ventricular hypertrophy (RVH)
RV obstruction:
Subvalvular (infundibular) pulmonary stenosis (PS),
both subvalvular and valvular PS or valvular PS only
R-L shunt severity determined by PS severity;
severe PS, large R-L shunts with severe early cyanosis
vs. mild PS, possibly no cyanosis

TF: interventions
11
Palliative (not repair): Blalock-Taussig, Waterston, Potts shunts
Palliative followed by repair:
Before 1980, repair usually postponed until age 5-6 unless cyanosis
With cyanosis, palliative/ central Gortex shunt followed by repair, subsequent
repair often complicated by anomalies, scarring created by shunt, not always able
to correct
Palliative shunts still may be used in severe cases (hypoplastic PA)
Repair:
VSD patch closure
RV outflow tract obstruction relief
removal excess muscle bundles, possible valvotomy
possible outflow tract patch (potential significant PR)
Ideal timing 4 months (although with only mild PS, may delay)
Surgical mortality currently 2% range, long term favorable but
limited follow-up

complete transposition, arterial switch 1989, age 3
weeks
Exam: I/VI short SEM, EKG normal, no symptoms
Echocardiogram:
No additional testing
12
Case 4: 23 year old female, life insurance
applicant

transposition, atrial switch (Mustard operation)
1986, age 2 years
13
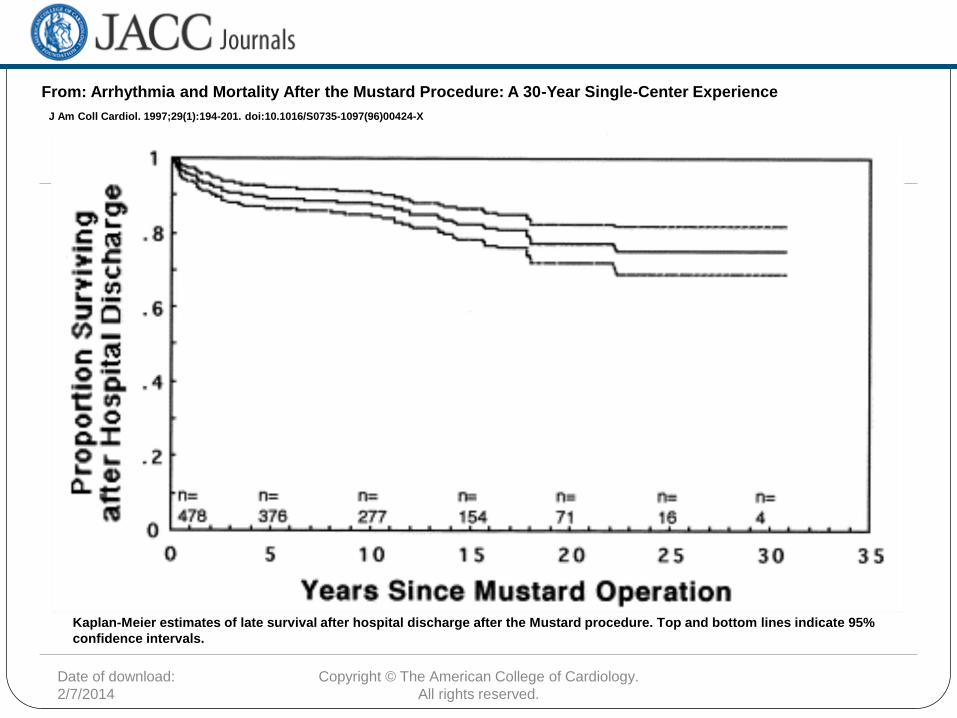
Case 5: 30 year old male, life insurance
applicant
Date of download:
2/7/2014
Copyright © The American College of Cardiology.
All rights reserved.
From: Arrhythmia and Mortality After the Mustard Procedure: A 30-Year Single-Center Experience
J Am Coll Cardiol. 1997;29(1):194-201. doi:10.1016/S0735-1097(96)00424-X
Kaplan-Meier estimates of late survival after hospital discharge after the Mustard procedure. Top and bottom lines indicate 95%
confidence intervals.
Figure Legend:
Bicuspid aortic valve (BAV)
with or without dilatation of the aortic root
imaging: echocardiography and MRI
15
Case 6: 25 year old male, life insurance
applicant

Total anomalous pulmonary venous
return (TAPVR)
Partial anomalous pulmonary venous return
(PAPVR)
Anomalous left coronary arteries
AV canal, repaired Primum ASD Subvalvular aortic
stenosis
Dextrocardia: echo findings
Valvular pulmonary stenosis
Rastelli operation in TGA
16
Short cases