Embed Size (px)
Citation preview

AbstractMullerian adenosarcoma (MA) of ovary with sarcomatous(rhabdomyoblastic) overgrowth is an extremely raremalignant type of female genital tract neoplasm. Thesetumours are highly aggressive and presence ofheterologous elements is associated with worseprognosis. A 44 year old female presented with lowerabdominal pain and distension. She had history ofremoval of tumour from pouch of Douglas in 2006 forwhich she did not receive any additional treatment nordid she keep continuous follow up. Current preoperativeradiological examination revealed bilateral ovarianmasses. She underwent abdominal hysterectomy withbilateral oophorectomy. Microscopic examinationrevealed biphasic tumours exhibiting sarcomatousovergrowth with rhabdomyoblastic differentiation.Review of the previous biopsy revealed low gradeMullerian adenosarcoma without sarcomatousovergrowth. Hence the current tumour was consideredrecurrent. This report highlights the aggressive nature ofMA even with low grade morphological features andemphasizes the importance of continuous follow up andadditional treatment.
Keywords: Mullerian adenosarcoma, sarcomatousovergrowth, rhabomyoblastic differentiation, extrauterine.
IntroductionMalignant mesenchymal neoplasms account for 1-3% ofall female genital tract tumours and MullerianAdenosarcoma (MA) constitute 8-10% of thesemalignancies.1-3 MAs commonly arise in the uterus andpresents as a polypoid mass. However, they can alsoinvolve extrauterine sites and ovary is the most commonamong these sites. Other extrauterine sites include pelvis,vagina, fallopian tube, peritoneum, intestine, liver, etc.1-3
According to the classical description of Clement and
Scully, MA is a mixed neoplasm comprising of malignantstromal and benign epithelial component.1,4,5 MA withsarcomatous overgrowth is defined as partial overgrowthof an otherwise typical adenosarcoma by pure high gradesarcoma occupying at least 25% of the tumour mass.Further classification of MA depends upon differentiationof mesenchymal elements; Homologous tumours arecomposed of nonspecific spindle shaped sarcomatouscells, whereas heterologous tumours are associated withmyoid, chondroid and osteoid differentiation.2,3 Tumourswith sarcomatous overgrowth have aggressive clinicalcourse as compared to tumours without sarcomatousgrowth.2
Case PresentationAn abdominal hysterectomy and bilateral oophorectomyspecimen was received at Histopathology Section,Department of Pathology and Laboratory Medicine, AgaKhan University Hospital, Karachi in April 2017. Patient wasa 44 year old female who presented to the gynaecologistwith complaint of lower abdominal pain. On clinicalexamination, a tender mass was palpable in the lowerabdomen. Her preoperative ultrasound revealed acomplex mass in right adnexa. MRI scan of pelvis showedbilateral ovarian masses. Right ovarian mass measured 8.5x 8 cm with solid enhancing and cystic necroticcomponents. Left ovarian solid mass measured 5 x 4.5 cm.Uterus was bulky and contained multiple well definedhypo intense masses (Fibroids). There was no evidence ofpelvic visceral, omental and peritoneal involvement. Pelviclymphadenopathy was also not seen. Her serum CA-125level was 50.9 u/ml. She underwent total abdominalhysterectomy with bilateral oophorectomy.
Gross examinations showed the uterus, cervix, fallopiantubes and multiple separate light brown, soft to firm,irregular pieces of tumour tissue. The largest of thesetissue pieces measured 13 x 7 cm and the rest measured11 x 9 cm in aggregate. On sectioning, cut surface was tanto light brown and exhibited areas of haemorrhage,necrosis and multiple cystic spaces. Uterus, cervix andfallopian tubes were grossly not involved by tumour.Myometrium also showed three fibroids.
Vol. 68, No. 8, August 2018
1263
CASE REPORT
Low grade Mullerian adenosarcoma of pouch of Douglas recurring as bilateralovarian high grade Mullerian adenosarcoma with rhabdomyosarcomatousovergrowth after 11 yearsSanddep Kumar, Muhammad Raza, Muhammad Usman Tariq
Section of Histopathology, Department of Pathology and Laboratory Medicine,Aga Khan University Hospital, Karachi.Correspondence: Muhammad Usman Tariq.Email: [email protected]

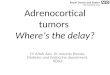
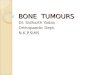
Microscopic examination oftumour tissue pieces revealed anextensively necrotic tumour. Theviable areas showed a biphasicgrowth pattern comprising ofpredominant stromal componentand scattered irregular, ectatic andcompressed glands lined by blandlooking columnar cells showingnuclear stratification. The stromacomponent showed markedhypercellularity with areas ofnecrosis and myxoid change. Atsome areas stromal cells appearedcondensed around the glands(Figure 1A-D). Stromal cells werespindle to stellate in shape andexhibited prominentrhabdomyoblastic differentiation.Immunohistochemical (IHC) stainsDesmin and myogenin alsoconfirmed the rhabdomyoblasticnature of stromal cells (Figure 2A-D). The nuclei were highlypleomorphic and hyperchromatic.Frequent mitotic figures(approximately 22/10 HPF) werealso appreciated. At foci, thebackground stroma showedhyalinized plaques resembling"collagen rossettes". Endometriosisand ovarian sex cord like elementswere not found. Focally, normalovarian stroma was also identified.Hence, the case was diagnosed as"Mullerian adenosarcoma withr h a b d o m y o s a r c o m a t o u sovergrowth".
Later the patient also revealed thatshe had undergone laparotomyand excision of a tumour in thepouch of Douglas in 2006. Therewas no evidence of disease in theovaries, other pelvic organs andomentum at that time. The slidesof the previous biopsy werereviewed which also revealed lowgrade adenosarcoma without anyother lineage differentiation.Hence, we consider our case to berecurrence of the initial tumour.Since the patient belonged to a
J Pak Med Assoc
1264 S. Kumar, M. Raza, M. U. Tariq
Figure-1: (A) Low power view of biphasic tumour exhibiting cystic spaces. Normal ovarian tissue is also appreciableon left side. (B) Medium power view showing condensation of stromal component around dilated glandularstructures. (C) Medium power view showing compression of epithelial component by adjacent stromal component.(D) High power view showing benign low columnar epithelial lining surrounded by low grade sarcomatouscomponent.
Figure-2: (A) Medium power view and (B) High power view of areas showing rhadomyosarcomatous overgrowth. (C)Desmin and (D) Myogenin IHC stains demonstrating positive expression and confirming rhabdomyoblastic differentiation oftumour cells.

remote rural area of the country, she neither keptcontinuous follow up nor received additional treatmentat that time.
Patient was disease free 4 months after the removal ofthe recurrent tumour. Since the tumour had acquiredhigh grade and sarcomatous overgrowth, patient wasoffered adjuvant radiotherapy which she refused dueto financial reasons. She was then advised to keepclose follow up with her gynaecologist andoncologist.
DiscussionThe term "Mullerian adenosarcoma" was used first in 1974by Clement and Scully for a distinctive uterine tumourcharacterized by a malignant, usually low grade, stromalcomponent, and a generally benign, but occasionallyatypical, glandular epithelial component.5 Since that time,similar cases have been reported from various places inthe literature, most of which include a small number ofpatients.1-3,6-8 The largest series on MA included only 40patients.2
MA can occur at any age including adolescence.Extrauterine MAs occur at younger age than their uterinecounterparts as seen in our patient. Median age foruterine tumours is 71 years as compared to 53 years forextrauterine tumours. In vast majority (97.5%) of casesmay tend to occur unilaterally.2 In contrast, the ovarieswere bilaterally involved in our case. The commonpresenting manifestations include abdominal pain,abdominal distention with palpable mass and irregularvaginal bleeding as also observed in our case.3 Some ofthese extrauterine tumours have been associated withand presumably arise from endometriosis. While othersare not associated with endometriosis, they are thoughtto arise from surface epithelium, ovarian stroma, orperitoneal mesothelium as part of secondary Mulleriansystem.6,7
Mullerian adenosarcoma of ovary is generally similarmicroscopically to uterine adenosarcoma except a fewdifferences like sarcomatous overgrowth is seen in 30% ofovarian cases as compared to 8% in uterineadenosarcoma and SCLE (Sex cord like elements) wereseen in 15% of ovarian cases as compared to 7% in theiruterine counterparts.2,4
Almost all endometrioid tumours of the ovary arecarcinomas except for rare tumour types i.e.adenofibroma and MA. Adenofibroma resembles MAexcept that the stroma of adenofibroma lacks nuclearpleomorphism and mitotic activity found inadenosarcoma. The differential diagnosis in any
individual case depends on the morphologic featuressuch as presence or absence of heterologouselements, sex cord like elements, and sarcomatousovergrowth. The differential diagnosis of MA withsarcomatous overgrowth also includes endometrialstromal sarcoma [ESS], immature teratoma, malignantmullerian mixed tumours (MMMT) and pure sarcomaswhen heterologous elements are present. ESS occursin same age group as mullerian adenosarcoma and isusually unilateral. ESS resembles stromal componentof adenosarcoma but lacks its glandular component.Thorough sampling should be done to search forepithelial component of MA as the prognosis of MA isworse than ESS. Immature teratoma can be excludedon the basis of age as these tumours most commonlyoccur in the first three decades of life and are almostnonexistent after menopause, and contain embryonalneuroectodermal elements and endodermal derivatesin almost all cases. In contrast to MA, malignantmullerian mixed tumours (MMMT) typically have ahigh grade mesenchymal component and an invasivecarcinomatous component. The presence of typicaladenosarcoma areas rule out the possibilities of puresarcomas.1,2,7 Ovarian MAs have poor prognosis,higher recurrence and higher mortality rates than theirmore common uterine counterparts. Five year diseasefree survival is less than 25%.8,9 The main reason isprobably related to the location of tumours withrespect to the abdominal cavity and the lack of ananatomic barrier to spread. Another reason may alsobe the result of the larger size, higher stage, andhigher frequency of rupture of the ovarian tumours.Surgery is the mainstay of treatment and additionalchemotherapy and/or radiotherapy is administered ina proportion of patients.2
ConclusionMAs of ovary are rare aggressive tumours which canpresent with recurrence after many years, even with lowgrade morphological features. Additional aggressivetreatment modalities and close clinical follow up shouldbe considered in all cases.
Disclaimer: None to declare.
Conflict of Interest: All authors declare that here is noconflict of interests.
Funding Disclosure: This study has not been funded.
References1. Clement PB, Scully RE. Extrauterine Mesodermal (Mullerian)
adenosarcoma. A clinicopathologic analysis of five cases. Am JClinPathol 1978; 69: 276-83.
2. Eichhorn JH, Young RH, Clement PB, Clement PB, Scully R.
Vol. 68, No. 8, August 2018
Low grade Mullerian adenosarcoma of pouch of Douglas recurring as bilateral ovarian high grade... 1265

Mesodermal (Mullerian) adenosarcoma of the ovary. Aclinicopathologic analysis of 40 cases and a review of theliterature. Am J Surg Pathol 2002; 26: 1243-57.
3. Can B, Kucukali T, Ahyan A, Ozkaya O, Durukan T. PrimaryExtrauterine adenosarcoma: Report of 2 cases. Turkish J Cancer2008; 38: 26-9.
4. Clement PB, Scully RE. Mullerian adenosarcoma of the uterus: aclinicopathologic analysis of 100 cases with a review of theliterature. Hum Pathol 1990; 21: 363-81.
5. Clement PB, Scully RE. Mullerian adenosarcoma of theuterus: A clinicopathologic analysis of ten cases of adistinctive type of mullerian mixed tumour. Cancer 1974; 34:1138-49
6. McCluggage WG. Mullerianadenosarcoma of the Female genital
tract. Adv Anat Pathol 2010; 17:122-9.7. Patel T, Gupta A, Trivedi P, Shah M. Osteoid differentiation in
Mesodermal (Mullerian) adenosarcoma of ovary. J Cancer ResTher 2013; 9: 529-31.
8. Daskalaki A, Xenaki S, Athanasakis E, Chrysos E, Chalkiadakis G.Advanced Mesodermal (mullerian) adenosarcoma of the ovary:Metastasis to lung, mouth, and Brain. Case Rep Surg 2015; 2015:403-31.
9. Ellenson LH, Carinelli SG, Cho KR, Kim KR, Kupryjanczyk J, Prat J, etal. Mixed epithelial and mesenchymal Tumours of Ovary. In:Kurman RJ, Carcangiu ML, Herrington CS, Young RH, eds. WHOClassification of Tumours of Female Reproductive Organs. 4th ed.Lyon, France: International Agency for Research on Cancer (IARC)Press, 2014; pp 42-3.
J Pak Med Assoc
1266 S. Kumar, M. Raza, M. U. Tariq