Embed Size (px)
Citation preview

Case report
Fever in a patient with
ANCA-associated vasculitis

*Hypertension: Enalapril, Furosemide
*Dyslipidemia: Pravastatin
*Ischemic heart disease: 2008 Angina
73 years-old white woman
PRIOR MEDICAL HISTORY

*ANCA-associated vasculitis (MPO):
#Jan/2011: (2 months) asthenia, anorexia, fever of unknown origin
(37º-38ºC), arthralgia and myalgia
CRP: 12 mg/dl ESR: 110 mm/h
-Renal involvement (Proteinuria: 510 mg/24h, 4-10 RBC/f)
Focal necrotizing glomerulonephritis with extracapillary
proliferation
-Neurological involvement: Mononeuritis multiplex
-Immunology: p-ANCA, MPO 222 IU/ml
-Microbiology (blood, urine, sputum): negative
-CT body: Normal


Treatment: MYCYC Trial
Prednisone (1 mg/kg/day) +
Mycophenolate mofetil (1g bid) +
Cotrimoxazol 800/160 mg/3 times per week
During admission:
*Acute coronary syndrome without ST elevation
#Coronary angiography: critical lesion of descending artery
and stent was placed.
Bisoprolol, Aspirin, Clopidogrel
*H1N1 Flu: treated with oseltamivir.

At 3 months, complete remission was achieved.
Clinically without symptoms (only paresthesia)
CRP: 1 mg/dl ESR: 28 mm/h
-Renal involvement (Proteinuria: 153 mg/24h, 1-3 RBC/f)
-Immunology: ANCA MPO 29 IU/ml
Treatment: Prednisone (12.5 mg/day + MMF [1 g bid])
*ANCA-associated vasculitis (MPO):

CURRENT DISEASE:
#June/2011: (2 weeks) fever (38ºC), arthralgia and malaise
-Physical examination: Alert, oriented.
No skin lesions. No signs of arthritis. No lymphadenopathies.
Normal breath sounds.
Rhythmic heart sounds without murmurs or signs of heart failure.
Abdomen: soft, painful deep palpation diffusely. No masses nor organomegaly.
Preserved bowel sounds.
Neurologic: Normal (paresthesia without changes)
Preserved distal pulses. No signs of deep vein thrombosis.
Thyroid size and consistency normal.

#Blood test: (abnormal results)
-PCR 3.6 mg/dl (<1mg/dl). ESR 50 mm/h.
-BCC: Leukocytes 8.61 109/l (80% neutrophils), Erythrocytes 3.15 1012/l,
hemoglobin 92 g/L, MVC 95 fl, Reticulocyte 4.5%. Iron 44 mcg/dl, folic acid and
vitamin B12 normal.
-Haptoglobin 2.92 g/l, Ferritin 341 ng/dl, Transferrin 2 g/l.
-Creatinine 1.1 mg/dl, Liver function test normal. LDH 420 IU/L.
Protein 50 g/l, Albumin 31 g/l.
-Proteinogram: Increase of a-globulins 1 and 2 fractions (no monoclonality)
-Urinalysis: Leucocytes 4-10/field, Erythrocytes 1-3/field.
-24-hour Urine Collection: Protein 81 mg/24h. Prot-creat ratio 124 mg/g.
-Beta 2 microglobulin 5 mg/l (0.1-2.3 mg/l)
-ANCA MPO 14.8 IU/l, ANCA PR3 Negative.


In your opinion, this patient had…..
1.Urinary infection, of course
2.Probably, she had a vasculitis flare
3.She had fever as adverse event of MMF
4.Fever secondary to neoplasm (solid or hematological)
5.It doesn't matter! systemic steroids should be immediately
increased

In addition to diagnostic work-up, what
would you do?
1. I’m sure that she had an urinary infection and antibiotics
should be initiated
2. Vasculitis flare is the most probable option and
corticosteroids should be increased
3. Be patient!! Paracetamol and wait for the results of
diagnostic work-up
#Microbiology:
-Blood Culture x 2: Negative.
-Urine Culture: Negative.
-Sputum Culture: Negative.
#Echocardiogram: Normal. No vegetation.
#Abdomino-pelvic CT: Normal.
#Colonoscopy: Normal.
Diagnostic work-up and……

After 20 days of admission, the patient persisted with fever……but clinically
without changes
CRP: 2.4 mg/dl ESR: 54 mm/h
#Microbiology:
-Blood Culture x 4: negative
-Urine Culture x 3: negative
-Sputum Culture: negative
-Serology (EBV, CMV, Coxiella): negative
#Gallium bone scan: Normal
#Sinuses CT: Partial occupation of ethmoid air cells bilaterally
#PET-CT: Normal
Evolution……


In your opinion, this patient had…..
1. An infection, I suppose
2. I was right!!, she had a vasculitis flare!!
3. A drug fever is a real option
4. Don’t forget neoplasm (solid or hematological)!!
5. This patient is the typical case of factitious fever

The patient had vasculitis activity
Treatment: PDN 17.5 mg/day + MMF 3 g/day (MYCYC)
Discharged at home….
In our opinion……

But…
• #Thoracic CT: Multiple pulmonary embolism and….• #Doppler: Deep venous thrombosis in both legs
– Right: Superficial femoral, popliteal, posterior tibial and peroneal veins thrombosis– Left: Superficial femoral vein thrombosis

Eureka!!!! PE is obviously the cause of the
unknown fever
1. Yes, I’m sure. ANCA-associated vasculitis are associated with
high risk of thrombosis.
2. PE is only an incidental finding.
3. PE does not explain the unknown fever.

Fever persisted without clinical and laboratory changes…..
Evolution……
LMWH was started and…….
Gastrointestinal bleeding in the form of rectal bleeding
(enterorrhage)
Gastrointestinal endoscopy: gastric and duodenal ulcers


Fever persisted without clinical and laboratory changes…..
Evolution……
A diagnostic test was performed……..
LMWH was started and…….
Gastrointestinal bleeding in the form of rectal bleeding
(enterorrhage)
Gastrointestinal endoscopy: gastric and duodenal ulcers
#Pathologic study of ulcers: CMV inclusions
#Microbiologic study: CMV PCR blood +
16,788 copies/ml
Treatment:
Ganciclovir with improvement of the patient
Enterocolitis by CMV
PE + DVT
ANCA-vasculits

Discussion
CMV infection
PE + DVT
ANCA-vasculitis
Discussion
CMV infection
PE + DVT
ANCA-vasculitis

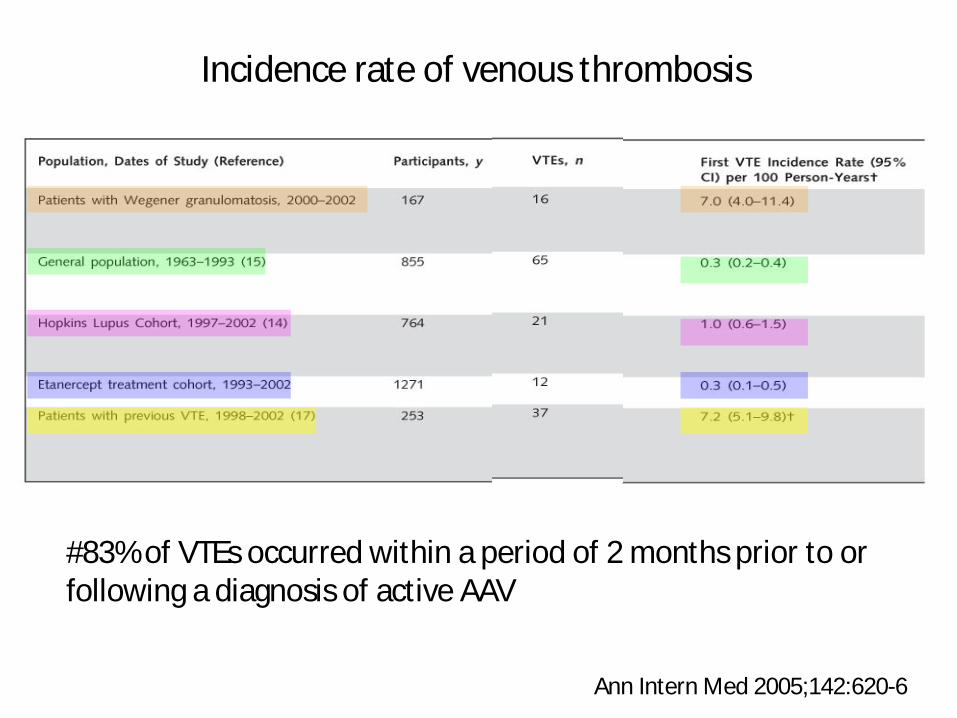
Incidence rate of venous thrombosis
Ann Intern Med 2005;142:620-6
#83% of VTEs occurred within a period of 2 months prior to or following a diagnosis of active AAV

198 patients: 143 WG, 34 MPA, 21 RLV
Median follow-up period since diagnosis of AAV: 6.1 yrs
(range: 0.2–17.6 yrs).


Incidence of AAV-associated VTE during active and inactive disease
Rheumatology 2008;47:530-4
Healthy population (same age) 0.3
#52% of VTEs occurred within a period of 3 months prior to or following a diagnosis of active AAV

#Etiology
*Endothelial lesion
*Hypercoagulability
*Relationship between WG and genetic factors predisposing to thrombotic events??
*CYC and corticosteroids??
#Chronic inflammation does not seem to be an independent factor to thrombosis
Activity phase

Discussion
CMV infection
PE + DVT
ANCA-vasculitis

• CMV in patients with AASV is lower than that in transplantation
• 2.2% of patients
• Although valganciclovir and surveillance polymerase chain reaction (PCR) is available and used in transplant patients at a high risk of developing CMV, there are no recommendations for their use in patients with autoimmune disease on immunosuppression.

535 AAV patients (1995-2002)
Median duration of follow-up was 5.2 years
133 (25%) deaths were recorded

Causes of death within and after the first year of follow-up

Discussion
CMV infection
PE + DVT
ANCA-vasculitis

• Reported in the medical literature almost 100 times• Theories:
– CMV triggers thrombosis by enhancing platelets and leukocytes adhesion to infected endothelial
– CMV increases the circulatory levels of factor VIII. – CMV transiently induces production of anti-phospholipid antibodies
• Incidence of thrombosis among acute CMV infection hospitalized patients: 6.4%
• Incidence of acute CMV infection among thrombosis hospitalized patients: 1.9–9.1%. Most (n=64; 65.9%) reported patients were immunocompetent
• Mean age of reported patients was 39.7±14.9 years. Female– male ratio was 1:1
• DVT/PE, splanchnic vein thrombosis and splenic infarction were the most prevalent thromboses associated with acute CMV infection

Discussion
CMV infection
PE + DVT
ANCA-vasculitis

-Three patients with AAV (1 WG and 2 MPA) and PE-DVT associated with CMV infection.
-All three patients were under treatment with CYC and CS (high dose).
-CMV Reactivation: 2 cases (flu-like syndrome) 1 case (assymptomatic).
-Probable etiology:
Endothelium infection lead recruitment of inflammatory cells
*Endothelial cells are infected by CMV and endothelium is the main reservoir of CMV during acute infection
-Patients with AAV and active CMV infection should be treated with prophylactic anticoagulation.

Conclusions
*Increased incidence rate of VTE in AAV.
*Relationship with activity of AAV.
*Etiology unknown.
*CMV infection in AAV patients is rare.
*There are no recommendations for the use of CMV PCR and prophylactic valganciclovir in patients with autoimmune disease on immunosuppression.
*There are no recommendations of prophylactic anticoagulation in AAV patients with CMV infection.

Thank you for your attention






![Dengue Fever/Severe Dengue Fever/Chikungunya Fever · Dengue fever and severe dengue (dengue hemorrhagic fever [DHF] and dengue shock syndrome [DSS]) are caused by any of four closely](https://img.dokumen.tips/doc/110x75/5e87bf3e7a86e85d3b149cd7/dengue-feversevere-dengue-feverchikungunya-dengue-fever-and-severe-dengue-dengue.jpg)






















