Embed Size (px)
Citation preview

Case:Health care to patients with
Coronary Heart Disease
Partly based on a Norwegian report (RHF South, 2002)
Nov 5th -2007Grete Botten

What is included in Health Needs Assessment?
• Defining the medical problem (need)
• Know the prevalence/incidence of the problem• Know the number that should be served
• Know the medical guidelines for examination and treatment - “state of the art”- evidence
• Know the patents’ situation and preferences
• Know the services available and their cost
• Argue for establishing services according to the need

Patients with coronary hearth disease • Illustrate several aspects of need assessment
• Changing epidemiology • Different patients groups
– screening for risk factors – preventive treatment – acute care – long-time care
• Cut-off problems• New (expensive) technology is being developed
– invasive – drugs

Defining the patients
• Population (screening)• Identified risk persons (high cholesterol, high blood
pressure, smokers…)• Sudden cardiac collapse• Patients with symptoms, chronically and acute - with
different EKG-pictures– Stabile angina– Unstable angina– Acute infarct with (most serious) or without ST-elevation
• Heart Failure (due to arteriosclerosis) --- both specific medical treatment and palliation

Prevalence/Incidence
• Prevalence relevant for chronically disease– preventive treatment – angina– cardiac failure
• Incidence relevant for– heart infarction (acute)
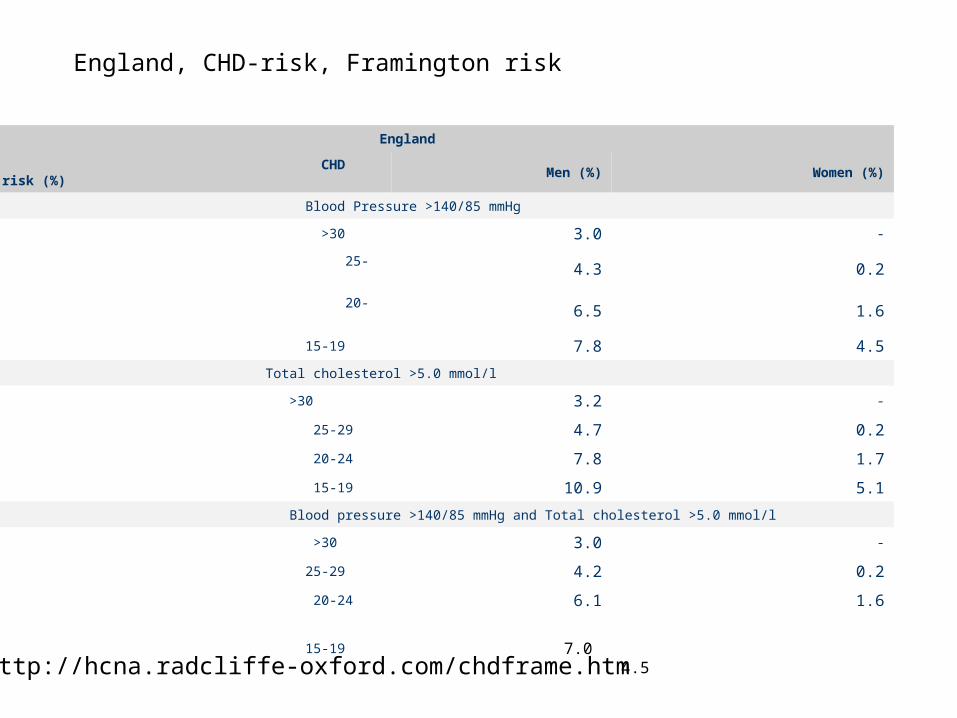
England
CHD absolute risk (%) Men (%) Women (%)
Blood Pressure >140/85 mmHg
>30 3.0 -
25-29 4.3 0.2
20-24 6.5 1.6
15-19 7.8 4.5
Total cholesterol >5.0 mmol/l
>30 3.2 -
25-29 4.7 0.2
20-24 7.8 1.7
15-19 10.9 5.1
Blood pressure >140/85 mmHg and Total cholesterol >5.0 mmol/l
>30 3.0 -
25-29 4.2 0.2
20-24 6.1 1.6
15-19 7.0 4.5
http://hcna.radcliffe-oxford.com/chdframe.htm
England, CHD-risk, Framington risk

Tables from
• http://hcna.radcliffe-oxford.com/chdframe.htm
• Tab 3 , 5,6,7,8,12

The population to be served
• Demography (the total number)– Age structure (increasing with age)– Sex (more common among men)– Ethnicity?
• Projection– The elderly population
Intervention possibilities• Screening of the healthy population (program/ wild)• Treatment of patients with identified risk factor
– High blood cholesterol/hypertension (by GP/specialists) • evidence for treatment • cut-off values for treatment • price for treatment, priority….
• Treatment of patients with symptoms (angina)– Drug therapy (aspirin, statins, ACE-inhibitor)– Revascularization
• Services for treating acute infarction– Ambulance with skilled personnel and equipment (emergency call)
• Distance to acute facilities, resuscitation – In patient
• Number of beds/intensive care units– Drugs (several, acute and prolonged therapy)– Revascularization (PCI, Bypass surgery)
• Rehabilitation• Heart failure

Mapping information together
• Make a plan to develop good services to all patient groups at all service level according to – Their need (medical and social)– Effective services (evidence based)
• Cost – benefit analyses
• Priority of resources

Health South Report in about services to Patients with
coronary health diseases. 2002
• Evaluate the capacity and quality of existing services to those patients in RHF South
• Develop future good and equal services for all the patients in RHF South
Focus
• Treatment of coronary arteriosclerosis
• Capacity according to need
• Localization – Qualified personnell– Distance for patients

Trends
• Declining mortality
• Declining incidence ?
• Increased prevalence

Defining the Patient group
• Care of patients with manifest coronary disease – Prevention not included
• Several symptoms, chronicle and acute - with different EKG-pictures– Stabile angina– Unstable angina– Acute infarct without ST-elevation– Acute infarct with ST-elevation
• Several new methods for examination and intervention/treatment

Examination/treatment
• Coronary angiography with contrast
• PCI- widening of the coronary vessel with a balloon
• Stent (drug diluting ?)
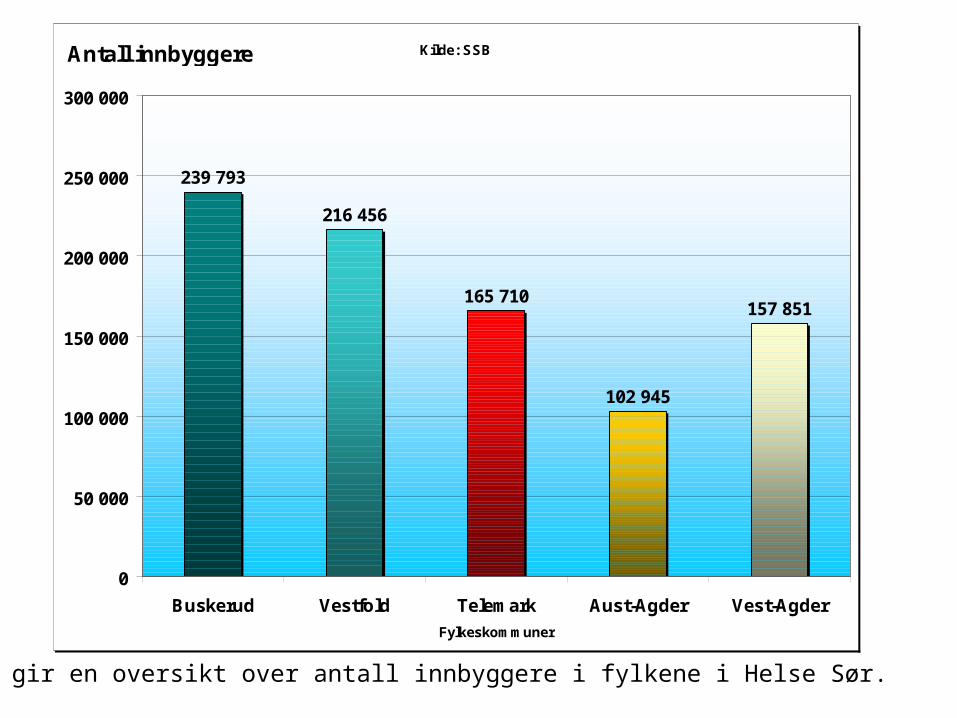
Kilde: SSB
239 793
216 456
165 710
102 945
157 851
0
50 000
100 000
150 000
200 000
250 000
300 000
Buskerud Vestfold Telemark Aust-Agder Vest-Agder
Fylkeskommuner
Antall innbyggere
Grafen gir en oversikt over antall innbyggere i fylkene i Helse Sør.

OSLO
Tonstad
Flekkefjord
Farsund
Mandal
Kristiansand
GrimstadArendal
EvjeTvedestrand
Risør
Valle
Kragerø
HaukeligrendRjukan
Seljord
Geilo
Gol
Hønefoss
Sande-fjord
Skien TønsbergHorten
DrammenKongsberg
Porsgrunn Larvik
Notodden
Rondeslottet2178
1881
Buskerud
Telemark
Aust-Agder
Vest-Agder
Vest-fold
X
Sykehus med akuttfunksjonSykehus uten akuttfunksjon
Rikshospitalet / Radiumhospitalet
X
X
X
X
X
500 100 150 km
239 793
165 710
157 851
102 945
216 456

Kilde: SSB
0
2000
4000
6000
8000
10000
12000
14000
I alt
4 år
9 år
14 år
19 år
24 år
29 år
34 år
39 år
44 år
49 år
54 år
59 år
64 år
69 år
74 år
79 år
84 år
89 år
94 år
99 år
104 år
109 år
114 år
Alder
Totalt Menn Kvinner
Antall innbyggere

Kilde: SSB
0
10 000
20 000
30 000
40 000
50 000
60 000
70 000
80 000
Alder
2002 55726 59899 60177 54201 53644 58065 64115 64254 62228 61929 60473 54912 39156 33467 32001 30851 23631 12624 4597 942
2005 56814 59987 62174 58015 53376 53814 63384 67271 63867 62991 60344 61272 45315 35787 30999 28098 24516 13374 5088 1084
2010 58941 60883 62519 63655 57560 52591 56702 66772 69522 64844 63105 59741 59925 43622 32874 26497 21359 15259 5812 1333
2015 61482 63020 63450 63989 62962 56621 55593 59883 68917 70528 65065 62593 58592 57691 40320 28457 20488 13587 6786 1551
2020 64291 65606 65634 64958 63245 61775 59669 58845 61956 69854 70768 64684 61575 56646 53506 35243 22429 13330 6202 1844
0 - 4 år
5 - 9 år
10 - 14 år
15 - 19 år
20 - 24 år
25 - 29 år
30 - 34 år
35 - 39 år
40 - 44 år
45 - 49 år
50 - 54 år
55 - 59 år
60 - 64 år
65 - 69 år
70 - 74 år
75 - 79 år
80 - 84 år
85 - 89 år
90 - 94 år 95+
Antall innbyggere

Kilde: SSB
-15 000
-10 000
-5 000
0
5 000
10 000
15 000
20 000
25 000
30 000
Alder
2002 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
2005 1088 88 1997 3814 -268 -4251 -731 3017 1639 1062 -129 6360 6159 2320 -1002 -2753 885 750
2010 3215 984 2342 9454 3916 -5474 -7413 2518 7294 2915 2632 4829 20769 10155 873 -4354 -2272 2635 1288 391
2015 5756 3121 3273 9788 9318 -1444 -8522 -4371 6689 8599 4592 7681 19436 24224 8319 -2394 -3143 963 2262 609
2020 8565 5707 5457 10757 9601 3710 -4446 -5409 -272 7925 10295 9772 22419 23179 21505 4392 -1202 706 1678 902
0 - 4 år 5 - 9 år10 - 14
år15 - 19
år20 - 24
år25 - 29
år30 - 34
år35 - 39
år40 - 44
år45 - 49
år50 - 54
år55 - 59
år60 - 64
år65 - 69
år70 - 74
år75 - 79
år80 - 84
år85 - 89
år90 - 94
år95+
Antall innbyggere

1996 1997 1998 1999 2000 2001 20020
200
400
600
800
1000
Prognose basert på januar-november
Pasienter innlagt med ustabil angina og non-ST elevasjons hjerteinfarkt
213321
419 464
634711
966

1999 2000 2001 20020
50
100
150
200
250
300
Pasienter behandlet med PCI forST elevasjons hjerteinfarkt
Prognose basert på januar-november
275
170
80
25

In Norway
• 2000: 15 122 coronary angiography– 336/100 000– 5% annual increase
• 2001: 7 381 PCI, 162/100 000
• 2001: 3 299 coronary bypass, 73/100 000
• Each doctor need a certain volum

32303500
4026 4200
51705511
7381
2882 29453222 3207 3104 3021
3299
0
1000
2000
3000
4000
5000
6000
7000
8000
1995 1996 1997 1998 1999 2000 2001
PCI ACB
Antall pasienter
Figur 11: Antall PCI og ACB i Norge fra 1995 – 2001. (Kilde: Norsk Thoraxkirurgisk forening.)
-
100 000
200 000
300 000
400 000
500 000
600 000
700 000
800 000
900 000
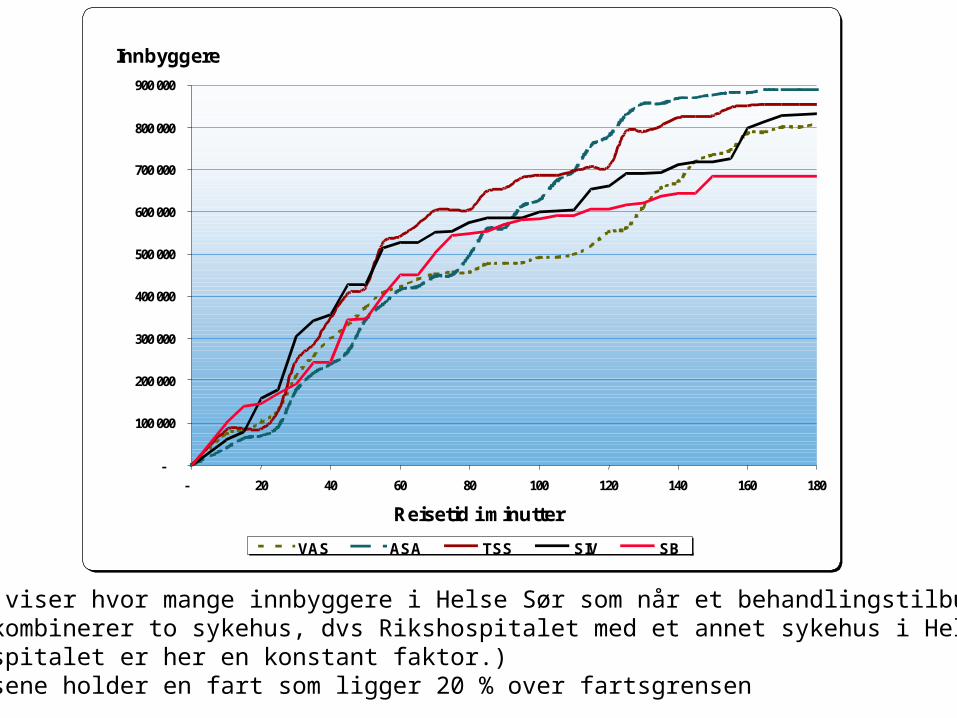
- 20 40 60 80 100 120 140 160 180
Reisetid i minutter
Innbyggere
VAS ASA TSS SIV SB
Figuren viser hvor mange innbyggere i Helse Sør som når et behandlingstilbud når en kombinerer to sykehus, dvs Rikshospitalet med et annet sykehus i Helse Sør. (Rikshospitalet er her en konstant faktor.) Ambulansene holder en fart som ligger 20 % over fartsgrensen

Present fascilities
• Local hospitals– Stable angina, too long waiting time (3-6 months,
50%<3), should be max 6-8 weeks
• Invasive centers– Elective coronary examination/PCI; waiting time 5-6
weeks, Feiring (private non-profit) 8-10– Unstable angina: should be 2-3 days for PCI– Capacity: Ok
• Heart operation (centers) (bypass)– Capacity: Ok, some to Denmark (Agder)

Available/distance
• Too long waiting time for stable angina locally
• PCI mostly acceptable waiting time
• Surgery, too long waiting time for elective patients, mostly ok for unstable angina
• Quality good
•

Acute services
• Incidence: 100/100 000 inhab. annually– Does not specify age – PCI or trombolysis
• PCI acute– At RH 25 to 270 from 1999-2002
• Time critical– Ambulance personnel (prehospital trombolysis)– RH: within one hour– Decentralized service (Arendal)- transport

Summary in report
• Prevention should be improved as collaboration between GP and specialist
• Capacity for elective invasive examination ok, but need improved organization
• A decentralized center should be established for treating acute infarction
• Prehospital trombolysis should be improved
• Larger postoperative capacity at RH

Lessons• Use earlier number of patients to describe need
– Difficult as availability to new technology increases the use
– Must have age-specific data to make scenarios
• Important to know – efficiency of treatment– time for reaching the treatment facility– availability of health personnel– see the total chain of treatment (GP, prehospital
emergency, specialist emergency and elective care)

Questions to discuss
• Who should define need– Need and demand
• The validity of need assessment
• Value and use of need assessment in developing the supply of services
• Need and prioritizing
• Technology and future need

How should need be defined?
• Medical definition– Linked to diagnosis (CHD)– Linked to medical challenges– Linked to guidelines for examination and treatment/care– Often expressed as the optimal, no resource limitations
• Lay people/patient defined– Linked to suffering (Pallation)– Linked to human/patient’s right
• Management defined– Linked to resources and “the contract”
• Politically defined– Linked to patients’ rights– Linked to resources– Linked to priority





























