Embed Size (px)
Citation preview

Case #1 Community Acquired Pneumonia
October 15, 2010
2- 4:30 PM

CLINICAL HISTORY-1
• A 45-year-old man was found wandering in downtown Orange with alcohol on his breath and coughing up thin, rusty sputum. He was brought to the emergency room where, although a poor historian, he said he had been fine the day before but that morning he had begun to shake uncontrollably and felt alternately cold then hot and sweaty. He said his chest hurt when he breathed and he felt nauseated..

CLINICAL HISTORY-2
• Information from the old hospital chart indicated that significant past history included a hospital admission for tuberculosis 10 years previously. Physical examination revealed a thin white male who was anxious and mildly cyanotic. Other abnormal physical findings included tachypnea and chest splinting, accompanied by fine rales and decreased breath sounds by auscultation over the right lower lobe. His temperature was 100.2o F, but his pulse was normal.

CLINICAL HISTORY-3
• WBC count was 16 × 103/μL (ref. range 4.1-10.9 x 103/μL) with 70% polys, 18% bands, and 12% lymphocytes. Blood gases demonstrated hypoxia and respiratory alkalosis. A chest x-ray is shown in Image 1 (next slide).
• Sputum was collected for smear and culture, and blood was drawn over the next hour for two sets of blood cultures. A Gram stain of the sputum showed lancet-shaped, Gram-positive diplococci.

• 1 - Chest, lobar pneumonia - Radiograph Note that the usual angle between the right heart border and the right diaphragm has been lost, and a diffuse infiltrate extends to the fissure between the right middle and right lower lobes. This is a lobar
pneumonic infiltrate.

CLINICAL HISTORY-4
• The patient was admitted and promptly begun on antibiotics and oxygen therapy. However, he became progressively more hypoxic, was placed in the intensive care unit on increasing concentrations of oxygen, and expired 24 hours after admission. During this time, both of the blood cultures were positive for Streptococcus pneumoniae. An autopsy was done; the pulmonary findings are shown in Images 2 and 3.

• 2 - Lungs, lobar pneumonia, gray and red hepatization - Gross, cut surfaces Lobar pneumonia differs from bronchopneumonia in that bronchopneumonia is patchy and lobar pneumonia is diffuse. These demonstrate the contrast between the stages of red hepatization (right) and gray hepatization (left). The lower lobe is expanded in both photographs; in the stage of red hepatization, the gross appearance reflects the microscopic features of congestion and hemorrhage along with a fibrinosuppurative exudate in the alveoli. The pneumonia takes on the appearance of gray hepatization when the congestion becomes less prominent and red blood cells have exited into the alveoli lyse, leaving behind the fibrinosuppurative exudate.

• 3 - Lung, lobar pneumonia - High power The alveolar spaces are filled with neutrophils (PMNs) and a fibrinous exudate. The alveolar septa are easily demarcated because of congestion with red cells. Because of the alveolar exudate, the lung becomes airless (solid). This is called consolidation. Interstitial pneumonitis, the typical inflammatory response to viruses and mycoplasma, is very different from acute bacterial pneumonia. The clinical presentation of interstitial pneumonitis is that of nonproductive cough, fever, and malaise. Pathologically, there is a lymphoplasmacytic infiltrate in the alveolar septa, shown in the second feature above. Note the absence of inflammatory cells in the alveolar spaces.

QUESTION #1
• Q: What would bronchopneumonia look like radiographically?

QUESTION #2
• Q: What is the most common pathogen causing lobar pneumonia?
•

QUESTION #3
• Q: What predisposed this patient to get pneumonia?

QUESTION #4
• Q: What are the components of the inflammatory reaction to bacteria?

QUESTION #5
• Q: While viral pneumonitis is usually self-limited, some patients develop pulmonary complications secondary to viral pneumonitis. What are these?

QUESTION #6
• Q: What accounts for the rusty sputum in this case?
•

• 4 - Lung, bronchopneumonia - Gross, cut surface This photograph of part of the lower lobe of a lung shows extensive involvement of the anterior aspect of the lung by bronchopneumonia. Bronchopneumonia is different from lobar pneumonia in that, in bronchopneumonia, the consolidation in the lung is patchy and follows the distribution of the bronchi and bronchioles. The light tan peribronchiolar areas represent acute inflammatory cells and fibrin. In addition, an abscess has formed in the basal section of the lung

QUESTION #7
• Q: What organisms are particularly associated with abscess formation?

• 5 - Lung, bronchopneumonia - Low power This image highlights the focal distribution of the inflammatory process in bronchopneumonia. The inflammation is in a bronchiolar distribution, that is, there is abundant inflammation within and surrounding the bronchioles. Some normal areas can also be seen.

QUESTION #8
• What are the complications of pneumonia?

• 6 - Lung, fungal pneumonia (immunosuppressed patient) - Gross, cut surface There is diffuse consolidation and vascular thrombosis with infarction of surrounding parenchyma of the right middle lobe of the lung, secondary to fungal infection. The picture on the left is before fixation in formalin, and the picture on the right is a closer view after fixation.

QUESTION #9
• Q: What are the mechanisms of pulmonary damage in immunocompromised patients with fungal infection?

• 7 - Lung, fungal pneumonia (immunosuppressed patient) - High power This fungus is causing pulmonary damage by occluding a major arterial branch, resulting in a surrounding infarct. Aspergillus and fungi of the Mucorales group are the most likely to produce this type of damage. In this case, the fungus was a dematiaceous fungus acquired through a sinus infection. The PAS stain highlights the fungi, which are seen occluding and penetrating through the wall of a large pulmonary vessel.

QUESTION #10
• Q: Aside from the lungs, what are the other two sites in the body frequently infected by Mucor?
Case 2: Neonatal Respiratory Distress Syndrome

CLINICAL HISTORY- 1
• A newborn girl was delivered at 28 weeks’ gestation (calculated by mother's last menstrual period) to a 25-year-old woman with a history of pregnancy-induced hypertension and continued heavy tobacco use. The mother came to the clinic complaining of cramping. She had a fever of 39°C. The fetal heartbeat was irregular, indicative of fetal distress. Because of concerns about fetal well-being, the delivery was induced.

CLINICAL HISTORY- 2
• The infant was delivered 4 hours later and weighed 600 gm; the Apgar scores were 4 at 1 minute and 7 at 5 minutes. The infant appeared long and thin with a relatively enlarged head size. By measurements, the body weight and crown-heel length were consistent with 25 weeks’ gestational age, and the head circumference was consistent with 28 weeks’ gestation. The gestation was estimated by clinical maturity studies to be 28 weeks.

CLINICAL HISTORY -3
• Sternal retractions were noted, indicating respiratory difficulties, and artificial surfactant was given. The respiratory status did not improve, and the infant was placed on a ventilator. Blood for cultures was drawn, and the infant was begun on antibiotics. Over the course of the next day, increasing ventilatory support was required. The chest radiograph is shown in Image 1.

• 1 - Chest, hyaline membrane disease - Radiograph This chest radiograph of a newborn premature infant shows hazy lung fields indicating fluid or an infiltrate in the airspaces. This is often called ground-glass opacification, and is characteristic of hyaline membrane disease. Similar changes are seen with group B streptococcal pneumonia.

CLINICAL HISTORY -4
• Blood cultures were positive for group B Streptococcus. On the second day of life, seizures developed. A head ultrasound examination diagnosed a severe intraventricular hemorrhage. After a discussion with the parents, it was decided that heroic measures would not be instituted, and the infant died at 32 hours of age. An autopsy was done.

QUESTION #1
• What other pathologic processes may produce a similar picture?
•

• 2 - Lungs, hyaline membrane disease - Gross This image compares the external appearance of a portion of the liver (lower specimen) with the lungs. The lungs appear solid, red, and airless. These are the characteristic findings in hyaline membrane disease. The lungs have an appearance similar to liver
because of extensive collapse and consolidation.

QUESTION #2
• Q: What are the risk factors for hyaline membrane disease?

QUESTION #3
• Q: Would this infant be considered appropriate for gestational age?

• 3 - Lung, hyaline membrane disease - Low power Photomicrograph of hyaline membrane disease of the lung with pneumonia. Note the pink acellular membranes in some airspaces. Neutrophils are also present in the airspaces.

QUESTION #4
• Q: What is the pathogenesis of these changes?

QUESTION #5
• Q: Are neutrophils prevalent in all cases of hyaline membrane disease?

• 4 - Lung, hyaline membrane disease - High power Higher power view of hyaline membrane disease and pneumonia in lung. The hyaline membrane is composed of fibrin and cellular debris.

QUESTION #6
• Q: How do hyaline membranes form?

• 5 - Placenta, chorioamnionitis - Gross A placenta with chorioamnionitis. The fetal membranes, which have flipped over to cover half of the maternal surface, are thickened and gray-tan instead of thin and translucent.

QUESTION #7
• Q: In this case, what pathogenetic sequence of events resulted in fetal infection?

• Placenta, fetal membranes, chorioamnionitis - Medium power Chorioamnionitis microscopically is characterized by a dense infiltrate of maternal neutrophils into the fetal membranes. Note the thin cuboidal cell layer of amnion along one edge of the membranes

QUESTION #8
• Q: Where does the inflammatory infiltrate originate?

• 7 - Brain, intraventricular hemorrhage - Gross, ventral surface This brain from a premature infant shows absence of the normal gyral pattern seen later in life. Normal gyration is present by 40 weeks’ gestation. This brain shows external evidence of intraventricular hemorrhage. There is subarachnoid extension of blood from the ventricles through the foramina of Luschka and Magendie.

• 8 - Brain, intraventricular hemorrhage - Gross, coronal section This image shows subependymal (germinal matrix) hemorrhage with rupture and extension into ventricles.

QUESTION #9
• Q: What are the predisposing factors for intraventricular hemorrhage?
QUESTION #10
• Q: What clinical symptoms may result from this?
•

• 9 - Chest, bronchopulmonary dysplasia (BPD) - Radiograph This chest radiograph shows areas of haziness and lucency in the lung fields. The haziness results from zones of interstitial fibrosis. The lucency reflects areas of hyperinflation.

QUESTION #11
• Q: What is the pathogenesis of BPD?

QUESTION #12
• Q: How have the histologic findings in BPD changed in recent years?

• 10 - Lung, bronchopulmonary dysplasia - Gross This is a lateral view of the external surface of the right lung from a patient who died with bronchopulmonary dysplasia typical of the severe glucocorticoid therapy and surfactant therapy. Note the cobblestone exterior surface of the lung owing to scarring and alternating hyperinflation and collapse of the underlying parenchyma. Compare this with the radiographic appearance of bronchopulmonary dysplasia in the previous image.

QUESTION #13
• Q: What are the clinical sequelae of this disorder?

• 11 - Lung, bronchopulmonary dysplasia - Medium power This microscopic view of bronchopulmonary dysplasia shows resolving hyaline membranes, hyperplasia of alveolar type II cells, and developing interstitial fibrosis, the typical features of severe bronchopulmonary dysplasia as it was seen before to the surfactant therapy era. Most cases now show diminished alveolar development, but lack the prominent alveolar epithelial hyperplasia and fibrosis depicted.

Case 3: Adult ARDS

CLINICAL HISTORY #1
• A 30-year-old white woman presented to the emergency department with fever, chills, and shortness of breath for 24 hours. She was well until 4 days earlier, when she noted pain on urination, followed shortly thereafter by pain in her left flank. She had diabetes treated with insulin.

CLINICAL HISTORY #2
• On arrival, the patient's blood pressure was 70/40 mm Hg, pulse was 120 beats/min, respiratory rate was 24/breaths, and temperature was 39 °C. On examination, wet rales were present in both lungs, and there was tenderness in the left flank. Chest x-ray revealed bilateral diffuse pulmonary infiltrates.

CLINICAL HISTORY #3
• Laboratory results were as follows: WBC 14,000, 82% PMNs, 7% bands; hematocrit 26% with fragmented red blood cells on peripheral blood smear; platelets 25,000; prothrombin time 18 sec (reference range 9.8-11.9 sec), partial thromboplastin time 80 sec (reference range 23-32.5 sec); arterial blood gases pH 7.25, PCO2 36 mm Hg, PO2 28 mm Hg; creatinine 4.8 mg/dL, glucose 600 mg/dL; urine cloudy with protein and PMNs.

CLINICAL HISTORY #4
• The patient was intubated and placed on dopamine, 100% O2, and intravenous antibiotics. She experienced progressive hypotension, an upper gastrointestinal hemorrhage, and intractable acidosis; blood cultures grew gram-negative rods. She died on the second hospital day. At autopsy, her lungs were heavy, firm, red, and boggy.

• 1 - Lungs, acute respiratory distress syndrome (ARDS) - Chest radiograph Radiograph shows extensive, diffuse, bilateral pulmonary infiltrates.

QUESTION #1
• Q: What is the morphologic basis for these radiographic findings?

• 2 - Shock lung - Gross, cut surface If the patient dies during the acute stage of ARDS (as in this case), the lungs are heavy (owing to accumulation of fluid), firm, red, and boggy. The cut surface bulges and oozes fluid.

QUESTION #2• Q: List some of the major causes of ARDS.

QUESTION #3
• Q: How did the patient develop ARDS?

• 3 - Lung, ARDS, exudative stage - Medium power Within the first 5 days, alveolar septa show interstitial inflammation with mononuclear infiltrates and develop hyaline membranes that line alveolar ducts. Alveoli tend to collapse. These findings are present in this image

QUESTION #4
• Q: What is the pathogenesis of hyaline membrane formation?

QUESTION #5
• Q: How does the pathogenesis differ in hyaline membrane disease in newborns?

• 4 - Lung, ARDS, proliferative stage - Medium power About 5 days after the onset of ARDS, the fibroblasts in the interstitium begin to proliferate and lay down collagen. Hyaline membranes begin to organize. Greatly thickened alveolar septa suggest that in this lung, the process may have developed over a few weeks. Lymphocytes and a few PMNs are in the interstitium. Residual hyaline membranes lie in patches in alveolar ducts and alveoli.

QUESTION #6
• Q: With continued proliferation, what type of lung disease develops in these patients?

• 5 - Lung, ARDS secondary to measles infection - High power Several acute infectious agents may result in ARDS. The measles virus propagates in epithelial cells of the respiratory tract and causes diffuse alveolar damage. Type II alveolar cells may fuse to form the characteristic multinucleated giant cells containing viral inclusion bodies. A marked interstitial infiltrate is present, accompanied by extravasation of red blood cells.

QUESTION #7
• Q: What other pulmonary diseases are associated with giant cells?

• 6 - Lung, massive pulmonary hemorrhage and infarct - Gross The lower lobe of this lung has a dark, wedge-shaped discoloration. This is most likely due to hemorrhage in an area of infarction.

QUESTION #8
• Q: What are the usual causes of pulmonary infarction?

• 7 - Lung, hemorrhagic infarct - Gross, cut surface Pulmonary hemorrhage, with or without infarction, may follow embolism. The lower lobes are more frequently involved. Triangular subpleural lesions are characteristic.

QUESTION #9
• Q: Why do only a few emboli result in infarction?

QUESTION #10
• Q: What are the likely outcomes of pulmonary thromboembolism?

QUESTION #11
• Q: What are the typical symptoms and signs in a patient who has nonlethal pulmonary infarction?

• 8 - Lung, hemorrhage and infarct - Low power There is a line of demarcation between normal-appearing lung (right) and an area of hemorrhagice infarction (left). In the hemorrhagic region, faint outlines of alveolar septa can be seen. These have undergone coagulative necrosis.

QUESTION #12
• Q: As this infarct heals, what morphologic evidence remains?

• 9 - Lung, fat embolism Not all pulmonary emboli are thromboembolic in origin. This fat embolus contains cellular marrow elements; a more accurate term would be bone marrow embolus.

QUESTION #13
• Q: How did the fat embolus arise, and from where?

QUESTION #14
• Q: What other types of emboli may reach the lungs?

• 10 - Lung, acute passive congestion - Gross, cut surfaces Acute pulmonary edema and congestion. Typically, it follows left ventricular failure.

QUESTION #15
• Q: What is the appearance of the lung and its cut surface?
•

QUESTION #15
• Q: Name some other causes of acute pulmonary congestion.

• 11 - Lung, pulmonary edema and congestion - High power Pulmonary edema and congestion, characterized by heavy, wet lungs, usually result from hemodynamic causes (cardiogenic edema) or from increased capillary permeability owing to microvascular injuries. In cardiogenic edema (see image), the capillaries are engorged and prominent, and there is an intra-alveolar granular pink transudate.

QUESTION #16
• Q: What would the histologic finding be in edema secondary to microvascular injury?

QUESTION #17
• Q: What parts of the lung are likely to be more severely involved by congestion and edema?

QUESTION #18
• Q: What is the most common cause of cardiogenic edema?
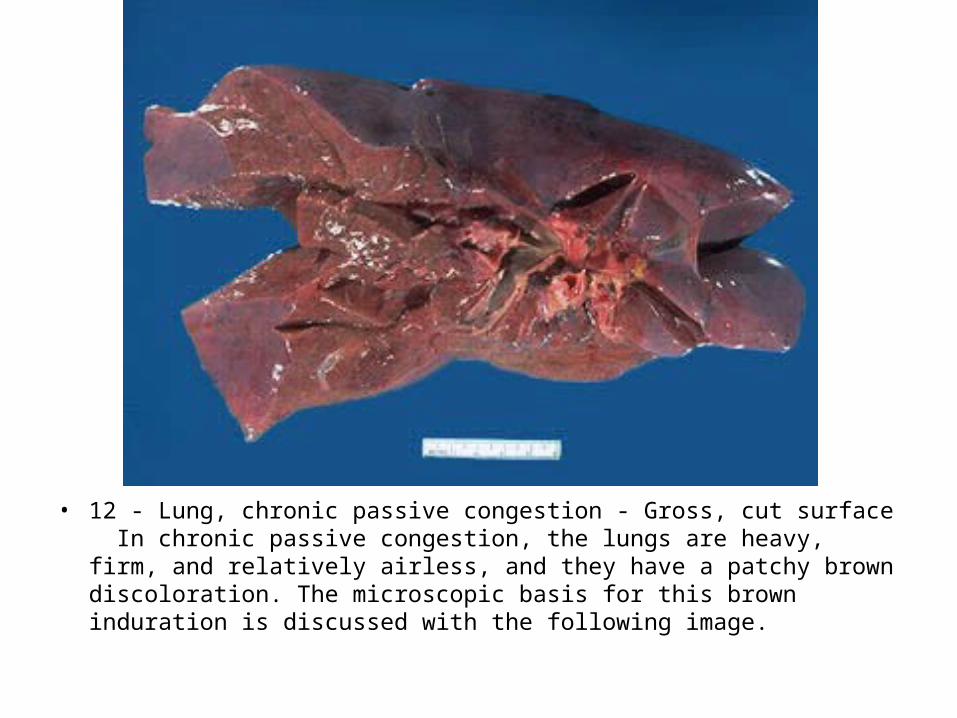
• 12 - Lung, chronic passive congestion - Gross, cut surface In chronic passive congestion, the lungs are heavy, firm, and relatively airless, and they have a patchy brown discoloration. The microscopic basis for this brown induration is discussed with the following image.

QUESTION #19
• Q: What is the nature of this pigment?

• 13 - Lung, chronic passive congestion - Medium power In long-standing pulmonary congestion, the engorged capillaries may rupture, causing intra-alveolar hemorrhages. Phagocytosis and breakdown of the extravasated red blood cells leads to the appearance of pigmented macrophages ("heart failure cells"). Chronically edematous alveolar septa may undergo fibrosis. This feature, combined with the presence of brown pigment, results in a gross finding termed brown induration.

QUESTION #20
• Q: Name some other conditions in which abundant iron pigment is present in the lungs.

• 14 - Lung, pigmented macrophages in chronic passive congestion - Low power In more advanced cases of passive congestion, large focal aggregates of pigmented macrophages are present. The pigment has been stained blue in a cytochemical reaction for detection of iron (Prussian Blue Stain).





























