-
8/12/2019 Carpal Tunnel Syndrome Anty
1/22
Carpal Tunnel Syndrome
The five Minute Orthopedic Consult, Rohit Robert Dhir BA
Damien Doute MD
A. Jay Khanna MD
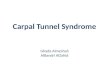
HasmiyantiC 111 06 034
Supervisor
dr. Jainal Arifin, M.Kes, Sp. OT
-
8/12/2019 Carpal Tunnel Syndrome Anty
2/22
Carpal Tunnel Syndrome
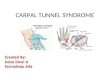
CTS is a neuropathy caused by compression of the mediannerve
within the carpal tunnel.
The floor of the tunnel is formed by the volar radiocarpaland
intercarpal ligaments.
The transverse carpal ligament forms the roof of the tunnel.
9 long flexors of the wrist and fingers and 1 nerve (median)run
within this spatially limited and relatively rigid tunnel.
Thus, any increase in pressure within the tunnelcompresses the
injury-prone median nerve.
A decrease in thenar muscle strength occurs, along with
anumbness or a decrease in the sensibility of the palmarsurface of
the radial 3 1/2 digits, especially the middle andindex
fingers.
-
8/12/2019 Carpal Tunnel Syndrome Anty
3/22
-
8/12/2019 Carpal Tunnel Syndrome Anty
4/22
Incidens
50% of cases are reported to occur in patients
40-60 years old; average age at carpal tunnel
release is 54 years.
CTS occurs predominantly in females (70%),
although the number of males with CTS may
be underestimated.
-
8/12/2019 Carpal Tunnel Syndrome Anty
5/22
Prevalence
The prevalence of CTS has been reported to
vary between 0.6% and 61% in different
occupational groups.
It is the most commonly diagnosed site of
nerve compression in the upper extremity.
-
8/12/2019 Carpal Tunnel Syndrome Anty
6/22
Risk Factors
Repetitive hand work Endocrine imbalance
History of neuropathy
Associated conditions
Rheumatoid arthritis
Pregnancy
Thyroid myxedema Acromegaly
Amyloidosis
Multiple myeloma
Diabetes
Trauma
Alcoholism
Gout
-
8/12/2019 Carpal Tunnel Syndrome Anty
7/22
Pathophysiology
Internal fibrosis of the median nerve
Epineural scarring and constriction
Reduced nerve conduction velocity
-
8/12/2019 Carpal Tunnel Syndrome Anty
8/22
Diagnosis
CTS can be diagnosed accurately by carefulhistory and physical
examination, inspection forthenar atrophy, and detection of
sensory
disturbance via light touch or a pinwheel. Provocative tests,
such as the Phalen test (which
consists of placing the affected wrist inhyperflexion in an
attempt to reproduce the
numbness in the hand) or tapping over thecourse of the nerve in
the tunnel to elicit a Tinelsign, also serve to confirm the
diagnosis.
-
8/12/2019 Carpal Tunnel Syndrome Anty
9/22
-
8/12/2019 Carpal Tunnel Syndrome Anty
10/22
-
8/12/2019 Carpal Tunnel Syndrome Anty
11/22
Signs and Symptoms
These symptoms can be aggravated with use of theaffected
hand:
Paresthesia in the median nerve distribution in the hand
Weakness or clumsiness in the hand
Pain in the hand, wrist, or distal forearm
Awakening from sleep with pain or numbness in the hand
Tinel sign: Tapping the median nerve over the carpaltunnel with
resultant paresthesias in the radial 3 fingers
Phalen sign: Paresthesias in the median nerve distributionwith
full flexion for at least 1 minute
-
8/12/2019 Carpal Tunnel Syndrome Anty
12/22
Physical Exam
The hand should be examined to detect
thenar muscle atrophy.
2-point discrimination should be checked at
the tips of the fingers on the radial and ulnar
borders (should be
-
8/12/2019 Carpal Tunnel Syndrome Anty
13/22
Tests
The following basic tests should be ordered to
rule out systemic causes of CTS:
Sedimentation rate
Serum glucose concentration
Serum uric acid level
Thyroid function test
Electromyography/nerve conduction velocity can
confirm diagnosis and help determine severity.
-
8/12/2019 Carpal Tunnel Syndrome Anty
14/22
Imaging
Radiography
Plain radiographs of the wrist in patients with
previous trauma or in patients with a long history
of inflammatory disease should be performed.
Electromyographic studies can help rule out
proximal injury to the median nerve or
identify peripheral neuropathy.
-
8/12/2019 Carpal Tunnel Syndrome Anty
15/22
Differential Diagnosis
Compression of the lower cervical roots by
cervical degenerative disc disease or tumors
-
8/12/2019 Carpal Tunnel Syndrome Anty
16/22
Treatment General Measures
Nonoperative intervention: Modalities: Cockup wrist splinting,
NSAIDs (not proven
effective), diuretics, and cortisone injections (which must
beperformed by an experienced physician to avoid direct injury
tothe median nerve)
The patient should wear a wrist splint during sleep.
Activity modification in work-related CTS is recommended.
Surgical release of the transverse carpal ligament is
performed when nonoperative measures have failed or inpatients
with constant numbness, motor weakness, orincreased distal median
nerve motor latency noted onelectromyography.
-
8/12/2019 Carpal Tunnel Syndrome Anty
17/22
Special Therapy
Physical Therapy
Occupational or physical therapy should be
consulted for activity modification teaching or
for nerve gliding exercises that might decrease
symptoms of nerve compression.
Postoperative therapy is aimed at minimizing
the development of painful scars and
increasing ROM and strength.
-
8/12/2019 Carpal Tunnel Syndrome Anty
18/22
Medication (Drugs)
No effective medication specifically to treatCTS has been
described.
Corticosteroid injection into the carpal tunnel
is indicated when the median nervecompression is predicted to be
temporary, as
in pregnancy or when the patient's activity
can be modified.
Injections must be done with great care to avoid
injury to the median nerve.
-
8/12/2019 Carpal Tunnel Syndrome Anty
19/22
Prognosis
Most patients with CTS associated with therepetitive trauma
commonly seen in theworkplace respond to a combination of
splinting,cortisone injection into the carpal tunnel, and
activity modification. If job modification is not in the
patient's
nonoperative treatment program, splinting andcortisone
injections may provide only temporary
relief. The maximum return of strength after carpal
tunnel release can take 6 months or longer.
-
8/12/2019 Carpal Tunnel Syndrome Anty
20/22
Complications
Iatrogenic injuries to the median nerve or its
branches may occur with open or endoscopic
release.
Painful surgical scars may ruin the results of a
successful decompression procedure.
Flexion tendon bowstringing may occur in a
few patients.
-
8/12/2019 Carpal Tunnel Syndrome Anty
21/22
Patient Monitoring
To obtain maximal beneficial results, the splintshould be worn
full-time for at least 3-4months, after which time use of the
splint can
be discontinued gradually. If symptoms return with removal of
the splint,
the patient becomes a surgical candidate.
The patient usually experiences immediate painrelief after
carpal tunnel release, whereasnumbness gradually improves over the
nextseveral months.
-
8/12/2019 Carpal Tunnel Syndrome Anty
22/22
THANK YOU