Embed Size (px)
Citation preview

Cardiovascular and Respiratory Systems: Oxygen Transport
Integration of Ventilation, Cardiac, and Circulatory Functions

Cardiorespiratory System
Functions of cardiorespiratory system: transportation of O2 and CO2
transportation of nutrients/waste products distribution of hormones thermoregulation maintenance of blood pressure

Ability of cardiorespiratory system on maintaining arterial PO2 (PaO2)
during graded exercise to exhaustion

Critical elements of O2 Transport Pathway
Lungs Ventilation
– VE = RR VT
O2 diffusion into blood– PO2 gradient determines O2 movement– Hb
Heart and circulation– Q = HR SV– cardiac output = muscle blood flow
O2 diffusion into mitochondria– oxyhemoglobin dissociation relationship– Fick principle [VO2 = Q (CaO2 – CvO2)]
Control of cardiorespiratory system– central control– peripheral inputs– maintenance of blood pH

Ventilation and Diffusion
Getting O2 from air into blood

A. Major pulmonary structure
B. General view showing alveoli
C. Section of lung showing individual alveoli
D. Pulmonary capillaries within alveolar walls
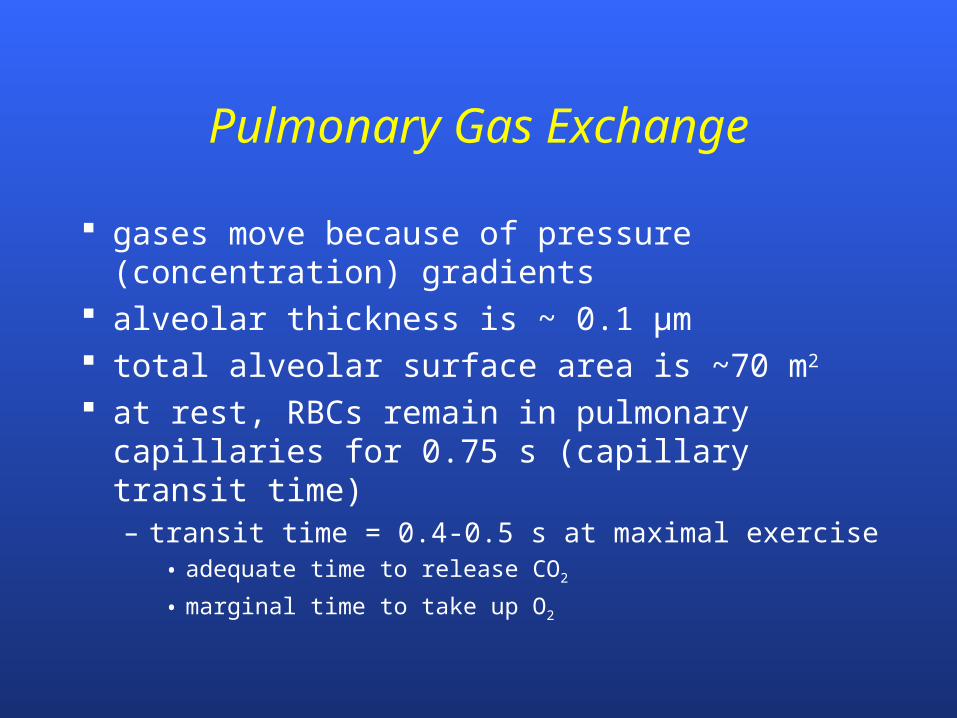
Pulmonary Gas Exchange
gases move because of pressure (concentration) gradients
alveolar thickness is ~ 0.1 µm total alveolar surface area is ~70 m2
at rest, RBCs remain in pulmonary capillaries for 0.75 s (capillary transit time)– transit time = 0.4-0.5 s at maximal exercise
• adequate time to release CO2
• marginal time to take up O2

PO2 and PCO2 gradients in body

Pressure gradients for gas transfer at rest: Time required for gas exchange in lungs (left) and tissue (right)

What would be the effect on the saturation of arterial blood with O2 (SaO2) when pulmonary blood flow is faster than RBC can uptake O2?
a. SaO2 would remain unchanged
b. SaO2 would be decreased
c. SaO2 would be increased

What effect might a decreased SaO2 have on O2 utilization by mitochondria?
a. no effect on mitochondrial VO2
b. will decrease mitochondrial VO2
c. will increase mitochondrial VO2

Pulmonary circulation
Pulmonary circulation varies with cardiac output

RBC
Single alveoli at rest showing individual RBCs
Single alveoli under high flow showing increased RBCs

Gas Exchange and Transport
Oxygen transport ~98% of O2 transported bound to
hemoglobin 1-2% of O2 is dissolved in blood

Hemoglobin
consists of four O2-binding heme (iron containing) molecules
combines reversibly w/ O2 (forms oxy-hemoglobin)

Rate of gas diffusion is dependent upon pressure (concentration) gradient.
Erythrocyte (RBC) ~98% of O2 is bound up with hemoglobin (Hb) and transported from lungs to working muscle.

CO2 + H2O H2CO3 H+ + HCO3-
Transport of O2 and CO2 in blood

Predict the relative O2 pressure differences between alveoli (PAO2) and arterial blood (PaO2)
a. PAO2 > PaO2
b. PAO2 = PaO2
c. PAO2 < PaO2


Role of the Heart
Moving O2 from lungs to working muscle

Cardiac Cycle
systole diastole cardiac output (Q) = stroke volume (SV)
heart rate (HR)
examples– rest: SV = 75 ml; HR = 60 bpm; Q = 4.5 Lmin-1
– exercise: SV = 130 ml; HR = 180 bpm; Q = 23.4 Lmin-1

Control of cardiac function and ventilation
Parallel activations


Reflex control of cardiac output
Primary regulators cardiovascular control center (medulla)
– w/ activation of motor cortex, parallel activation of sympathetic/parasympathetic nerves
• parasympathetic inhibition predominates at HR <~100 bpm• sympathetic stimulation predominates at HR >~100 bpm
skeletal muscle afferents– sense mechanical and metabolic environment
Secondary regulator arterial baroreceptors
– located in carotid bodies and aortic arch– respond to arterial pressure
• Reset during exercise


Cardiac Regulation
Intrinsic control Frank-Starling Principle
Ca2+ influx w/ myocardial stretch
Extrinsic control autonomic nervous system
– sympathetic NS (1 control at HR >100 bpm)– parasympathetic NS (1 control at HR <100 bpm)
peripheral input – chemoreceptors, baroreceptors, muscle afferents
hormonal– EPI, NE (catecholamines)

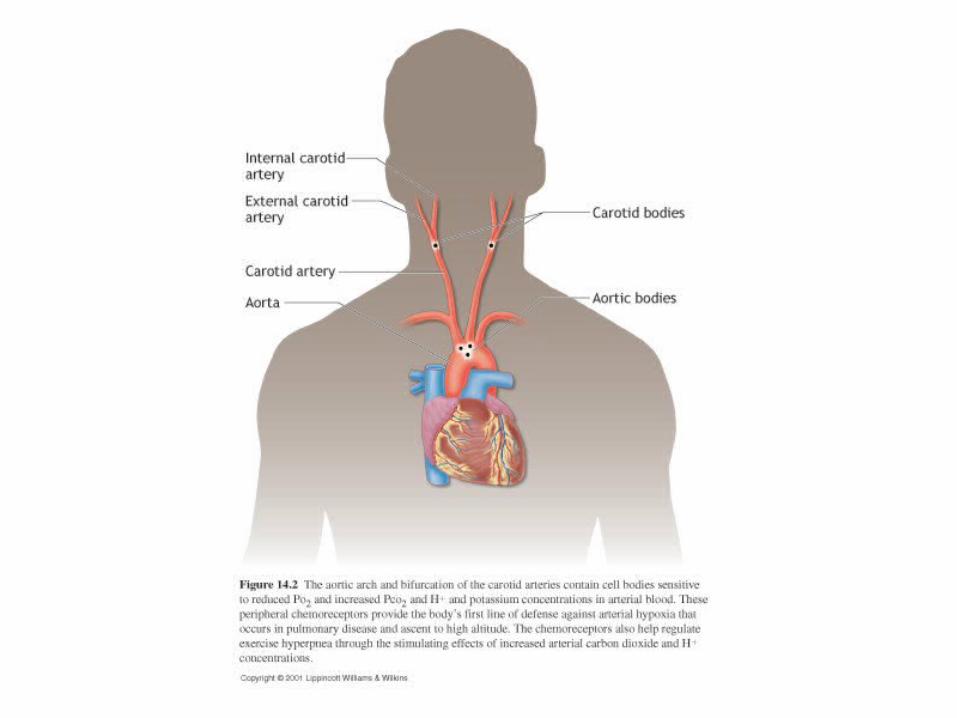

Humoral Chemoreceptors
PaO2
– not normally involved in control
PaCO2
– central PaCO2 chemoreceptors are 1º control factor at rest
H+
– peripheral H+ chemoreceptors are important factor during high-intensity exercise

Control of Ventilation
Central command and muscle afferents are primary control mechanisms
H+ chemoreceptors responsible for “fine-tuning” ventilation



Describe the mechanisms that control cardiac output and ventilation.

Cardiac output affected by:
1. preload – end diastolic pressure (amount of myocardial stretch)
2. afterload – resistance blood encounters as it leaves ventricles
3. contractility – strength of cardiac contraction
4. heart rate

Venus Blood Return to HeartSV dependent on venous return
muscle pump one-way venous valves breathing
Return of blood to heart

Cardiovascular Response to Exercise
Fick equation
VO2 = Q (aO2 – vO2)
VO2 = [HR SV] (aO2 – vO2)
VO2 = [BP TPR] (aO2 – vO2)

VO2 = Q (aO2 – vO2)
How would VO2 be affected if cardiac output/O2 extraction were increased?
a. increased
b. decreased
c. no effect
d. cannot be determined

Matching O2 delivery to muscle O2 needs
Regulation of cardiorespiratory system

Effects of Exercise on Cardiac Output

HR and SV responses to exercise intensity

Exercise effects on heart
HR caused by sympathetic innervation parasympathetic innervation release of catecholamines
SV, caused by sympathetic innervation venous return
cardiac output

Increasing Blood Flow to Working Muscle During Exercise
Blood flow redistribution

Blood Distribution During Rest

Blood vessels are surrounded by sympathetic nerves. A feed
artery was stained to reveal catecholamine-containing nerve
fibers in vascular smooth muscle cell layer. This rich
network extends throughout arterioles but not into capillaries
or venules.

Local blood flow control
general sympathetic response occurs with exercise onset that causes vasoconstriction
exercise hyperemia = increase in blood flow to cardiac and skeletal muscle
blood flow to working muscle increases linearly with muscle VO2
– muscle metabolic rate is key in controlling muscle blood flow
– controlled primarily by local factors


Onset of exercise
(1-adrenergic receptor blocker)
30 s

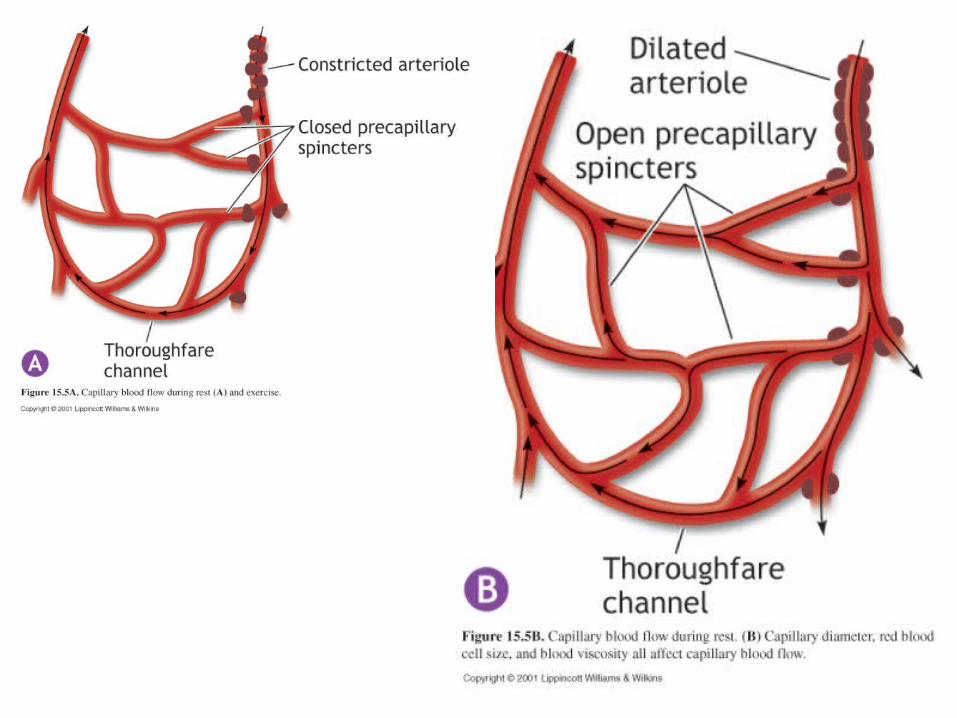
Blood Flow Redistribution During Exercise


Capillaries
flow of blood– aorta arteries arterioles capillaries
venules veins vena cava
arterioles regulate blood flow into muscle– under sympathetic and local control
precapillary sphincters fine tune blood flow within muscle– under only local control
• adenosine, PO2, PCO2, pH, nitric oxide (NO)

What is the primary mechanism to increase blood flow to working muscle?
a. baroreceptors
b. sympathetic innervation
c. local factors
d. epinephrine

At rest, most blood is found in the ______ while at exercise most blood is in _____.
a. venous system; active muscle
b. pulmonary circulation; heart
c. arterioles; capillaries
d. heart; heart
e. liver; active muscle



O2 Extraction
Moving O2 from blood into muscle

Factors affecting Oxygen Extraction
Fick equation
VO2 = Q (aO2 – vO2)

O2 extraction response to
exercise
Represents mixed venous blood

a-v O2 difference
Bohr Effect: effect of local environment on oxy-hemoglobin binding strength
amount of O2 released to muscle depends on local environment– PO2, pH, PCO2, temperature, 2,3 DPG
2,3 diphosphoglycerate (DPG)– produced in RBC during prolonged, heavy
exercise– binds loosely with Hb to reduce its affinity for O2
which increases O2 release

Bohr effect on oxyhemoglobin
dissociation
O2 loading in lungsO2 unloading in muscle
Oxyhemoglobin binding strength
affected by:PO2
PCO2
H+
temperature2,3 DPG

A change in the local metabolic environment has occurred: pH and PO2 have ; temperature and PCO2 have .
What effect will these changes have on the amount of O2 released to the muscle?
a. increase O2 release
b. decrease O2 release
c. no change in O2 release
d. cannot be determined

A change in the local metabolic environment has occurred: pH and PO2 have ; temperature and PCO2 have .
What do these changes in local environmental suggest has occurred?
a. the muscles changed from an exercise to a resting state
b. the muscles began to exercisec. no changed. cannot be determined

Carbon dioxide transport dissolved in plasma (~7%) bound to hemoglobin (~20%) as a bicarbonate ion (~75%)
CO2 + H2O H2CO3 H+ + HCO3-

Ventilatory Control of Blood pH

VO2 vs Power
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
0 100 200 300 400 500
Power (W)
VO
2 (
L/m
in)
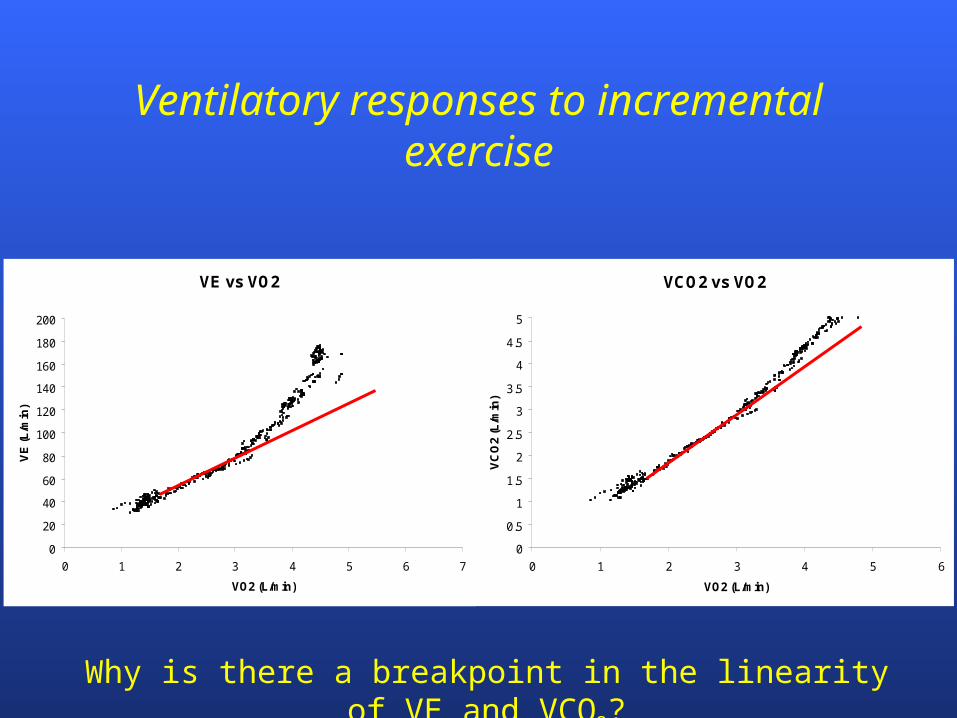
Ventilatory responses to incremental exercise
1. What was the subject doing? What data support your response?
2. What is the relationship of VO2 and exercise intensity?
VE vs VO2
0
20
40
60
80
100
120
140
160
180
200
0 1 2 3 4 5 6 7
VO2 (L/min)
VE
(L/m
in)
VCO2 vs VO2
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
0 1 2 3 4 5 6
VO2 (L/min)
VC
O2
(L/m
in)
Ventilatory responses to incremental exercise
Why is there a breakpoint in the linearity of VE and VCO2?

Ventilatory Regulation of Acid-Base Balance
CO2 + H2O H2CO3 H+ + HCO3-
at low-intensity exercise, source of CO2 is entirely from substrate metabolism
at high-intensity exercise, bicarbonate ions also contribute to CO2 production– source of CO2 is from substrates and bicarbonate
ions (HCO3-),
blood H+ stimulates VE to rid excess CO2 (and H+)
Can RER ever exceed 1.0? When? Explain

Blood pH
7.05
7.10
7.15
7.20
7.25
7.30
7.35
7.40
7.45
4 5 6 7 8 9 10 11 12 13 14 15
Treadmill Speed (mph)
pH

Respiratory Exchange Ratio
0.8
0.9
1.0
1.1
1.2
1.3
4 5 6 7 8 9 10 11 12 13 14 15
Treadmill Speed (mph)
RE
R
RER = VCO2
VO2

Minute Ventilation
0
20
40
60
80
100
120
140
160
180
200
2 3 4 5 6 7 8 9 10 11 12 13 14 15
Treadmill Speed (mph)
Min
ute
Ven
tila
tio
n (
L/m
in)

CO2 Production
0
10
20
30
40
50
60
70
80
90
2 3 4 5 6 7 8 9 10 11 12 13 14 15
Treadmill Speed (mph)
VC
O2
(m
l/k
g/m
in)

Ventilatory threshold: breakpoint in VE linearity— corresponds to lactate threshold
A subject completed a treadmill test in which the end-exercise RER was 0.98. Predict the subject’s RPE.
a. very light
b. moderate
c. hard
d. cannot be determined

What is the cause of hyperventilation during incremental exercise?
a. muscles cannot get enough O2
b. sympathetic innervationc. accumulation of lactate ions in bloodd. accumulation of H+ ions in blood
e. stimulation of PO2 chemoreceptors
VE vs VO2
0
20
40
60
80
100
120
140
160
180
200
0 1 2 3 4 5 6 7
VO2 (L/min)
VE
(L/m
in)
VCO2 vs VO2
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
0 1 2 3 4 5 6
VO2 (L/min)
VC
O2
(L/m
in)

Ventilation Questions
1. Describe how ventilation regulates blood pH.
2. Explain why the ventilatory threshold is related to the lactate threshold
3. Can RER ever exceed 1.0? Under what circumstances? Explain.


Effects of Exercise on Blood Pressure
BP = Q TPR

Regulation of Blood Flow and Pressure
Time
120
Pressure(mm Hg)
80
blood pressure (BP) = cardiac output (Q) total peripheral resistance (TPR)

Regulation of Blood Flow and Pressure
Blood flow and pressure determined by:
arterioles
B. Pressure difference between two ends
A. Vessel resistance (e.g. diameter) to blood flow
A
A BB
cardiac output
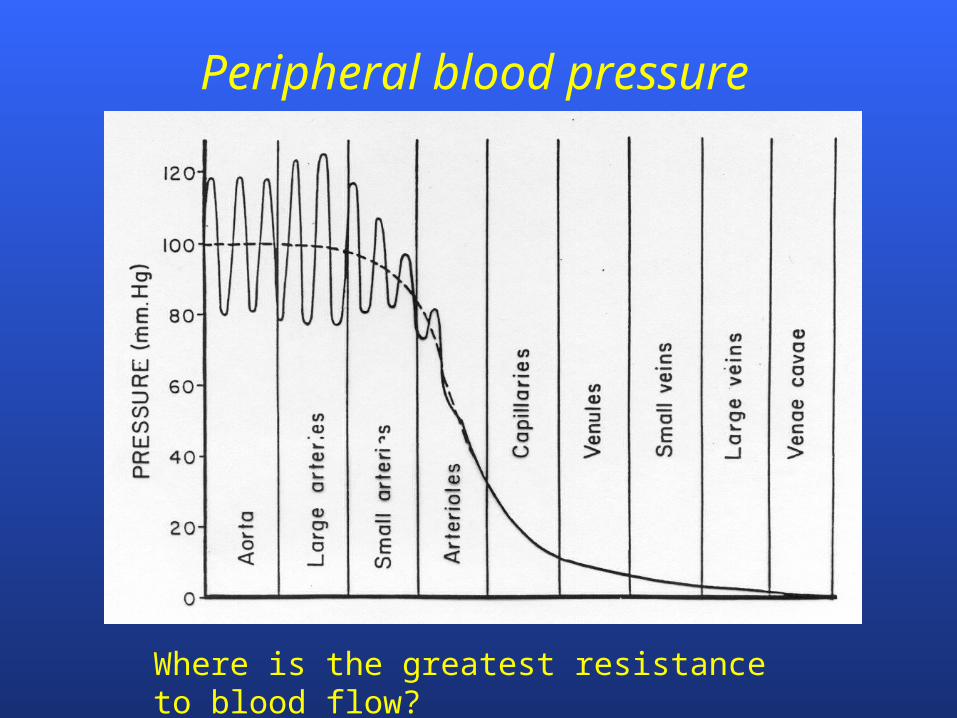
Peripheral blood pressure
Where is the greatest resistance to blood flow?

0
5
10
15
20
25
0 50 100 150 200 250 300 350 400
Treadmill speed (m/min)
TP
R
Effects of exercise intensity on TPR

Effects of incremental exercise on BP
0
25
50
75
100
125
150
175
200
225
250
0 50 100 150 200 250 300
Workload (W)
Blo
od
pre
ssu
re (
mm
Hg
)
Systolic BP
Diastolic BP

Effects of isometric exercise on BP
0
25
50
75
100
125
150
175
200
225
0 30 60 90 120 150
Time (s)
Blo
od
pre
ssu
re (
mm
Hg
)
Systolic BP
Diastolic BP

Comparison of BP Response Between Arm
and Leg Ergometry

Why is the BP response to resistance exercise greater than cycling exercise?
a. greater HR response during cycling
b. greater decrease in TPR during resistance exercise
c. greater decrease in TPR during cycling exercise
d. cardiac output is less during resistance exercise

Cardiorespiratory adaptations to endurance training
How does endurance training affect VO2max?

Maximal oxygen consumption (VO2max)
VO2max
– highest VO2 attainable– maximal rate at which aerobic system
utilizes O2 and synthesizes ATP– single best assessment of CV fitness
intensity
VO2VO2max
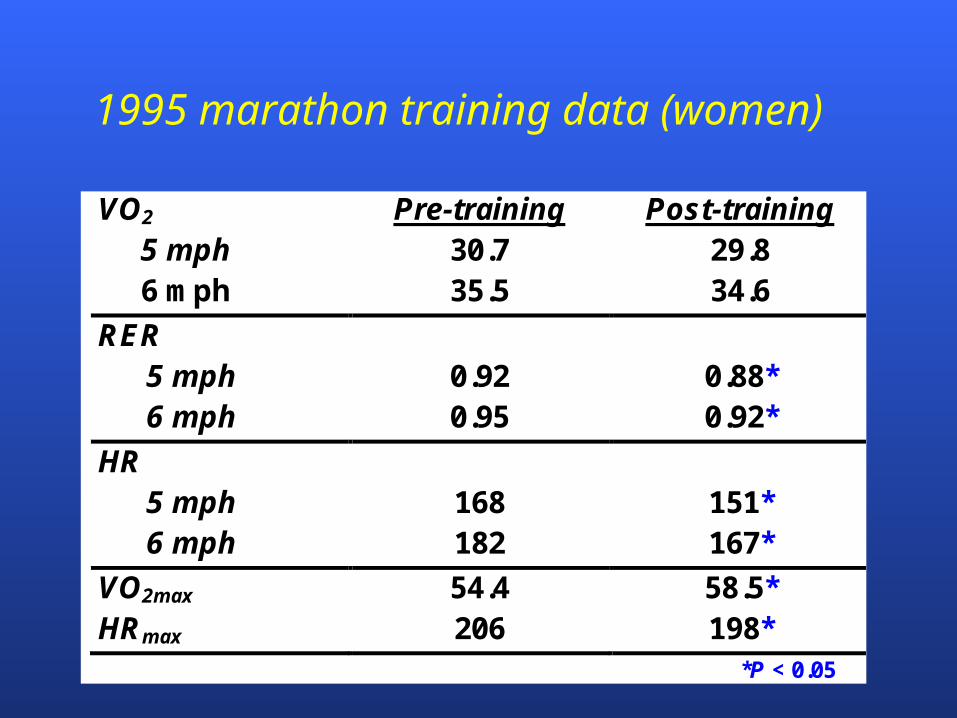
1995 marathon training data (women)
VO2 Pre-training Post-training 5 mph 30.7 29.8 6 mph 35.5 34.6
RER 5 mph 0.92 0.88* 6 mph 0.95 0.92*
HR 5 mph 168 151* 6 mph 182 167*
VO2max 54.4 58.5* HRmax 206 198*
*P < 0.05

Heart adaptations to training

Heart adaptations to training
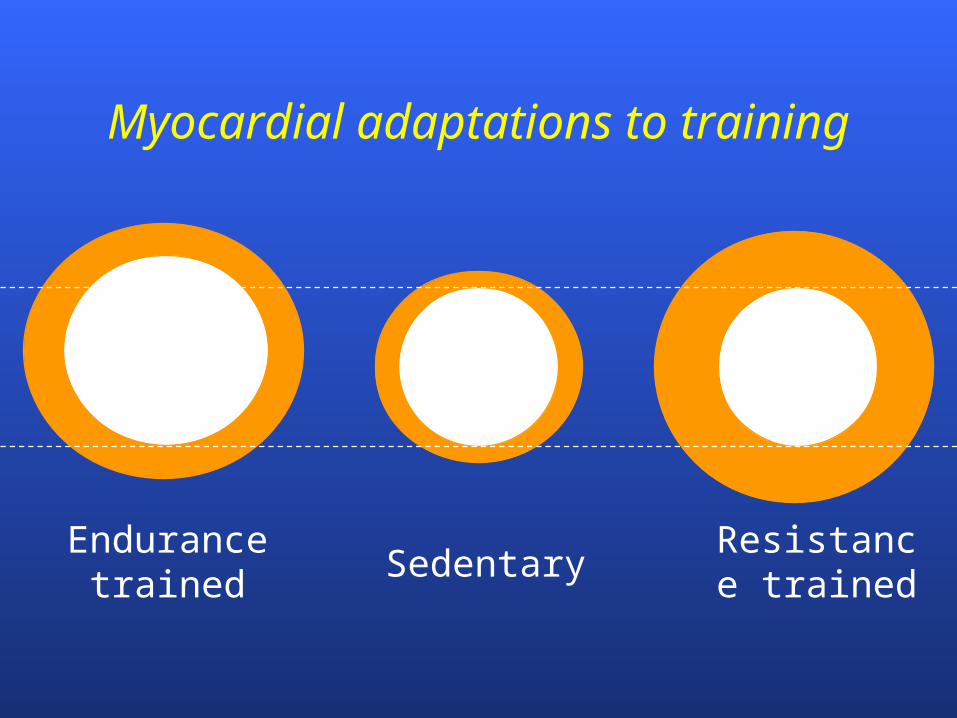
Myocardial adaptations to training
Endurance trained Sedentary
Resistance trained

Cardiorespiratory training adaptations
VO2max ~15% with training
ventilation? – training has no effect on ventilation capacity
O2 delivery?– CO ( ~15%) plasma volume SV
O2 utilization?– mitochondrial volume >100%

VO2max affected by:
– genetics (responders vs. nonresponders)– age– gender– specificity of training

Normalized data for VO2max (mlkg-1min-1)
Category %ile Age 20-29
Age 40-49
Age 60+
Excellent >80 >44 >39 >33
Average 40-60 36-39 31-35 25-28
Poor <20 <31 <28 <22
Excellent >80 >52 >49 >41
Average 40-60 43-47 39-44 33-36
Poor <20 <31 <28 <22
Aerobic Center Longitudinal Study, 1970-2002
Women
Men

As the SDSU women’s cross-country coach, would you be interested in a recruit who has a VO2max of 29.8 ml/kg/min?
a. definitely yes
b. definitely no
c. maybe

Which of the following would likely result in an increase of VO2max?
a. breathing faster and deeper during maximal exercise
b. faster HR at maximal exercise
c. ability to deliver more O2 to muscles during maximal exercise
d. more mitochondria

Which of the following does NOT occur following endurance training?
. blood volume
b. HRmax
c. SVmax
d. COmax
e. mitochondrial volume
f. maximal ventilatory capacity

How would you evaluate a VO2max of 28.9 mL/kg/min for a 22-year-old man?
a. excellent
b. above average
c. average
d. very low
e. dead

Which of the following adaptations likely had the LEAST influence for explaining why VO2max increased 12% after completing a cross country season?
. cardiac output
b. blood volume
c. mitochondrial volume
d. capillary density
e. number of RBC

Which of the following exercises would likely decrease TPR the LEAST?
a. jogging
b. fast walking
c. shoveling snow
d. cycling
e. all the above would decrease TPR similarly

What is the cause of the sudden increase in VE when the lactate threshold is reached during an incremental exercise test?
. muscle afferent activation
b. H+ in blood
c. stimulation of motor cortex
d. PO2 in blood
e. PCO2 in blood
What is the primary mechanism for increasing VE at the onset of exercise?
. PO2 in blood
b. PCO2 in blood
c. blood pH
d. neural factors
e. all of the above are equally responsible