Embed Size (px)
Citation preview
Cardiopulmonary Bypass and InfantVaccination TitersJeffrey Vergales, MD, MS,a Peter Dean, MD,a Jacob Raphael, MD,b Deborah Frank, MD, PhD,c Adishesh Narahari, PhD,a
Tyson Hekking, MD,a Carol Ann Rosenberg, CCP,d Mark Roeser, MD,d James Gangemi, MDd
abstractBACKGROUND: Infants with congenital heart disease remain vulnerable to potentially preventablepathogens. Although immunization can significantly reduce this risk, it is unknown howimmunization status can be affected by cardiac surgery with cardiopulmonary bypass (CPB).The objective was to evaluate the effect of CPB on infant vaccination status after cardiacsurgery.
METHODS:We conducted a prospective observational study of patients between 2 and 14 monthsof age who had received at least their first round of infant vaccinations and who requiredcardiac surgery with CPB. Antibody titers were measured before CPB and again the followingmorning. Demographic and surgical variables were assessed via regression methods for theireffects on the change in titers.
RESULTS: Among the 98 patients followed, there was no demonstrated difference between thepre- and postoperative values in regard to diphtheria, tetanus, polio 1, polio 3, or Haemophilusinfluenzae titers. Bordetella (1.03 vs 0.84, P, .001), and hepatitis B (log 2.10 vs 1.89, P = .001)titers did reduce after CPB but did not fall below the immunized threshold. Changes inantibody titers were not associated with time between immunization and surgery, age orweight at surgery, blood products administered, number of previous doses, time on CPB, orheterotaxy diagnosis for most of the vaccines.
CONCLUSIONS: Infant vaccine antibody titers were minimally affected by CPB and not associatedwith any easily modifiable surgical variables. Although antibody titers are only 1 marker ofimmunity, deviation from the recommended vaccination schedule may be unnecessary forchildren requiring congenital heart surgery.
WHAT’S KNOWN ON THIS SUBJECT: Most majorcongenital heart programs have strict guidelines forimmunizations surrounding planned heart surgery ininfants, although no real data exist as to what happensto vaccination status after surgery withcardiopulmonary bypass.
WHAT THIS STUDY ADDS: This study explores thedirect effect of cardiopulmonary bypass on antibodytiters to common infant vaccinations. Furthermore, itexplores the variables that alter infant’s vaccinationstatus after congenital heart surgery.
To cite: Vergales J, Dean P, Raphael J, et al.Cardiopulmonary Bypass and Infant Vaccination Titers.Pediatrics. 2020;145(1):e20191716
aDivisions of Pediatric Cardiology and cCritical Care, Department of Pediatrics, dDivision of Cardiothoracic Surgery,Department of Surgery, and bDepartment of Anesthesiology, University of Virginia, Charlottesville, Virginia
Drs Vergales, Roeser, and Gangemi conceptualized the study, interpreted the results, performeddata analysis, and prepared and reviewed the manuscript; Dr Raphael and Mrs Rosenberg wereessential in sample gathering and analysis as well as gathering and analysis of the operative andbypass data and reviewing the manuscript; Dr Frank conceptualized the study, gathered andinterpreted postoperative results, oversaw gathering the postsurgical samples, and reviewed andrevised the manuscript; Drs Dean, Narahari, and Hekking were essential in conceptualizing thestudy, enrolling patients, analyzing the vaccination data and titers, and reviewing the manuscript;and all authors approved the final manuscript as submitted and agree to be accountable for allaspects of the work.
DOI: https://doi.org/10.1542/peds.2019-1716
Accepted for publication Oct 11, 2019
Address correspondence to Jeffrey Vergales, MD, MS, Department of Pediatrics, University ofVirginia, PO Box 800386, Charlottesville, VA 22903. E-mail: [email protected]
PEDIATRICS Volume 145, number 1, January 2020:e20191716 ARTICLE at Bibliotheque Univ Paris V on December 16, 2019www.aappublications.org/newsDownloaded from

Children undergoing heart surgeryfor congenital and acquiredconditions are particularly vulnerableto infections secondary to theirclinical status, disease burden, andpossible immunocompromised states.These infections may be preventableby routine vaccine administration.Despite ∼10 000 children per year inthe United States undergoing cardiacsurgery before 12 months of age,1
there is little known about the effectsof cardiopulmonary bypass (CPB) onvaccine status.
Cardiac surgery with CPB is known tosignificantly alter circulating levels ofpassively acquired antibodies.2
Furthermore, it can have a profoundeffect on both proinflammatory andanti-inflammatory mediators that canaffect the body’s intrinsic antibodyproduction.3–6 No current availabledata exist regarding how thiscombination of factors alters aninfant’s response to immunizationsand overall immune status againstcommonly vaccinated diseases.Consequently, significant variationexists in how most major cardiacsurgical programs handleimmunization schedules in youngpatients undergoing planned cardiacsurgery requiring CPB.7
The objective of this study was toevaluate the effects CPB on standardchildhood vaccination antibody titersand assess whether modifiable riskfactors affect postoperative immunestatus in infants.
METHODS
We conducted a prospectiveobservational study of patientsbetween 2 and 14 months of age atthe University of Virginia thatrequired cardiac surgery with CPBbetween March 2016 and March2018. The limits on the age rangewere to ensure that screened patientshad begun routine childhoodvaccination. Subjects were recruited ifthey had received at least themajority (.75%) of age-specific
recommended vaccinations asrecommended by the Centers forDisease Control and Prevention8 andthen been verified by documentationin the Virginia ImmunizationInformation System, pediatrician’srecord, or from the electronic healthrecord. Subjects were excluded iftheir surgical procedure wasa planned cardiac transplant.Individuals with potentialimmunodeficiency states, including22q11 chromosomal deletion orheterotaxy syndrome, were enrolledand underwent subanalysis.
Informed consent was obtained for allsubjects. Providers obtained bloodsamples for antibody assays from thearterial line that was placed at thetime of surgery just before going ontoCPB. Providers obtained a repeatblood draw the next morning, fromthe same arterial line, as part ofroutine morning laboratory draws.The timing of the second sample wasvariable but was required to fallbetween 12 and 18 hourspostoperatively for standardizationpurposes so as to not causeunnecessary access to the arterialline. Postoperative blood draws couldnot extend past 18 hours because thelikelihood of receiving exogenousblood products significantlyincreased, theoretically affecting theresults. Titers of antibodies todiphtheria, tetanus, pertussis,Haemophilus influenzae type b (Hib),poliovirus, and hepatitis B wereassayed according to our standardcentral laboratory protocol andreported out as concentrations ortiter ratios on the basis of the assay.Thresholds for being consideredimmunized were reported from eachvaccine’s information data sheet,when available. A history of previousnatural infection was documented, ifpresent.
Demographic and operative variableswere analyzed to assess effect onchanges on antibody titers. Thisincluded, but was not limited to,baseline patient information,
vaccination history, time on CPB, typeof surgery, volume of products usedto prime the bypass circuit, presenceand amount of modifiedultrafiltration at the conclusion of thecase, and requirements for furtherblood products within the first24 hours. All red blood cells used toprime the CPB circuit were washed,leukocyte reduced, and irradiated, asan institutional standard.
Parents or legal guardians had theoption to consent to a third blooddraw, 3 months later. This bloodsample, drawn from a venipuncture,was performed in the clinical settingduring a routine postoperativeevaluation. The same antibody titerswere assessed. Vaccination historywas updated if immunizations wereprovided between the operation andthe third blood sample.
Acute effect of CPB on antibody titerswas analyzed by using appropriatepaired hypothesis testing, looking atcentral tendencies of each antibodytiter to determine statisticallysignificant changes when comparingpre- and post-CPB values.Logarithmic transformation wasperformed, where appropriate,because of large SDs of some of theantibody titers. Polio titers (includingpolio 1 and polio 3 antibodies) arereported as dilutional ratios, and thusa test of symmetry was used todetermine differences between pre-and post-CPB values rather thandiscrete paired hypothesis testing.Threshold lines were plotted alongwith the data to demonstrate whereindividuals are thought to loseprotective immunity.
Multivariate linear regression modelswere then used to ascertain theeffects of the case-specific risk factorsas described above on thepredictability of the results.Confounders that were controlled inthe final analysis or analyzedseparately included timing andamount of previous immunizations,presence of native infection,
2 VERGALES et al at Bibliotheque Univ Paris V on December 16, 2019www.aappublications.org/newsDownloaded from

chromosomal anomalies, heterotaxyor known immunodeficiency,ultrafiltration, and time on CPB. Two-sided P values of ,.05 wereconsidered statistically significant forthe descriptive data as well as beingthe threshold in the univariatemethods to determine if the factorwas appropriate for multivariateregression analysis. Polio titers, asa result of being reported out asdilutional ratios, were excluded fromregression analysis.
The study was approved by andoperated under the guidelines of theInstitutional Review Board of theUniversity of Virginia. Funding wasprovided by Merck Sharp and DohmeCorporation, Merck InvestigatorStudies Program (No. 53360),although they had no influence on theperformance of the study.
RESULTS
Of the 100 subjects who consented toparticipate, 98 had adequate bloodsamples to undergo antibody titeranalysis. The remaining 2 subjectshad early clotting of their samples,preventing any analysis. Baselinedemographics for the population aredepicted in Table 1. There were noidentified patients with 22q deletionsyndrome and 3 patients withheterotaxy syndrome.
The median vaccine titer valuesbefore and after CPB are displayed inFig 1 along with threshold lines forimmunity. There was no differencebetween the median pre- andpostoperative values in regard todiphtheria (0.23 vs 0.24, P = .16),tetanus (0.49 vs 0.55, P = .66), or Hibtiters (log 20.74 vs 20.55, P = .09).Polio titers, as well, did not show anydifference between pre- and post-CPBlevels (polio 1: P = .80; polio 3: P =.23). There was a significantreduction after CPB for Bordetella(1.04 vs 0.83, P , .001) and hepatitisB (log 2.16 vs 2.06, P , .001) titers.
There were no patients after surgerywith CPB whose titers fell below the
immunized threshold with respect todiphtheria, tetanus, polio, orBordetella vaccinations.
There were 39 subjects (40%) whowere nonreactive to Hib during theirprebypass assessment. There were 3subjects whose titers dropped fromimmunized status ($0.15 µg/mL) tounimmunized status (,0.15 µg/mL)after CPB. Likewise, there were 17individuals (17%) who wereconsidered nonreactive to hepatitis Bduring their prebypass assessment.Again, only 4 individuals went fromimmunized ($10 mIU/mL) tounimmunized status (,10 mIU/mL).There was no overlap betweensubjects who lost Hib immunity andthose who lost hepatitis B immunity.
Multivariate linear regressioncontrolling for suspected confoundersdemonstrated minimal effect of anyvariable on the change in pre- andpost-CPB titers (Table 2). Increasingtime on bypass did have an effect onthe tetanus titers (P = .03) and hadclose to a significant effect on thediphtheria (P = .06) and Bordetella(P = .08) titers. Furthermore, thenumber of total doses of the vaccine
the subject received demonstrateda significant change for tetanus (P =.04) and a nearly significant effect onthe change in titers for diphtheria(P = .08), in that the fewer dosesone received, the more profoundthe effect. The volume ofultrafiltration throughout the caseas well as blood productsadministered were not studiedin the multivariate analysis becausethey were not significant in simpleunivariate analysis, suggesting noeffect from those variables.
There were 41 subjects who receivedonly the first dose of the Hib, polio,diphtheria, tetanus, and pertussisvaccines, and of these, 21 had onlyreceived one hepatitis B dose. Amongsubjects receiving one dose ofa vaccination, the mean time betweenhepatitis B delivery and surgery was8.3 weeks (range: 0.9–18.1 weeks)and was 6.5 weeks for all of the otherpathogens (range: 0.9–15.0 weeks).There were 9 individuals who hadtheir only round of immunizations,3 weeks before surgery, and 4 ofthose individuals had them ,2 weeksbefore surgery.
TABLE 1 Baseline Demographics of the Study Population
Attribute of Subjects (n = 98) No. (%) or Mean (Minimum to Maximum)
Male 47 (48)RaceWhite, non-Hispanic 66 (67)African American 26 (27)Asian American or Pacific Islander 1 (1)White Hispanic 3 (3)Other 2 (2)
Cardiac surgeryTetralogy of Fallot repair 26 (27)Bidirectional Glenn 26 (27)Atrioventricular septal defect repair 19 (19)Isolated septal defect (ASD, VSD) repair 19 (19)Pulmonary valvotomy 4 (4)Pulmonary vein repair 2 (2)Anomalous coronary repair 1 (1)Subaortic membrane resection 1 (1)
Gestational age, wk 37.8 (28–41)Birth wt, kg 3.1 (1.1–5.1)Age at surgery, mo 5.5 (2.2–13.0)Wt at surgery, kg 5.9 (3.5–9.2)Time on bypass, min 153.0 (55–410)Heterotaxy 3 (4)22q deletion syndromes 0
ASD, atrial septal defect; VSD, ventricular septal defect.
PEDIATRICS Volume 145, number 1, January 2020 3 at Bibliotheque Univ Paris V on December 16, 2019www.aappublications.org/newsDownloaded from

Of subjects who had only receivedone dose of vaccine, only Hibdemonstrated a difference betweenmean pre- and post-CPB (log 20.90vs 20.65, P = .02) and is shown
in Fig 2. Diphtheria (0.06 vs 0.07, P =.11), tetanus (0.30 vs 0.46, P = .27),Bordetella (log 0.60 vs 0.55, P = .25),and hepatitis B (log 1.78 vs 1.58, P =.07) were unchanged. Polio titers did
not show any difference between pre-and post-CPB levels (polio 1: P = .96;polio 3: P = .22) among patients whohad only received one dose of poliovaccine. There were no patients whohad received their only round ofimmunizations ,3 weeks beforesurgery who lost immunity.
The results of multivariate linearregression for subjects who had justreceived one dose of vaccine are seenin Table 3. Bypass time did have aneffect on the observed change indiphtheria titers (P = .007).Otherwise, there were almost novariables, including time between
FIGURE 1Box plots demonstrating mean (*) and interquartile range (box) for assayed values pre-CPB compared with post-CPB in all patients. Whiskersdemonstrate high and low limits. Dashed lines are the antibody titer level considered to be immunized, representing how changes in antibody titersaffected presumed protective immunity. A, Diphtheria. B, Tetanus. C, Hib. D, Bordetella. E, Hepatitis B.
TABLE 2 Multivariate Linear Regression on All Subjects
Variable Diphtheria Tetanus Bordetella Hib Hepatitis B
Time between last vaccination and surgery .98 .48 .38 .16 .31Age at surgery .95 .25 .25 .62 .45Weight at surgery .19 .98 .39 .10 .19Bypass time .06 .03 .08 .99 .79No. previous doses of vaccine .08 .04 .85 .29 .11Heterotaxy .29 .98 .56 .72 .88
Results of multivariate linear regression on all subjects. Reported values are P values representing strength of thecoefficients in the regression equation and thus importance of that variable in the change between pre-CPB antibodytiters and post-CPB antibody titers.
4 VERGALES et al at Bibliotheque Univ Paris V on December 16, 2019www.aappublications.org/newsDownloaded from
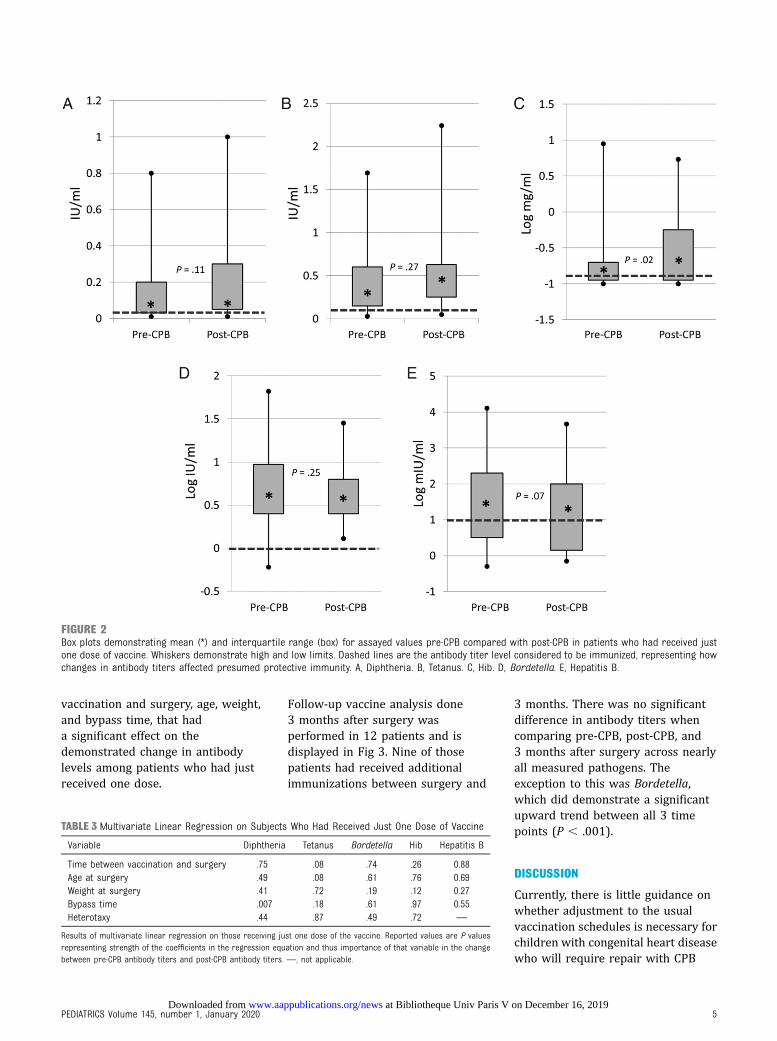
vaccination and surgery, age, weight,and bypass time, that hada significant effect on thedemonstrated change in antibodylevels among patients who had justreceived one dose.
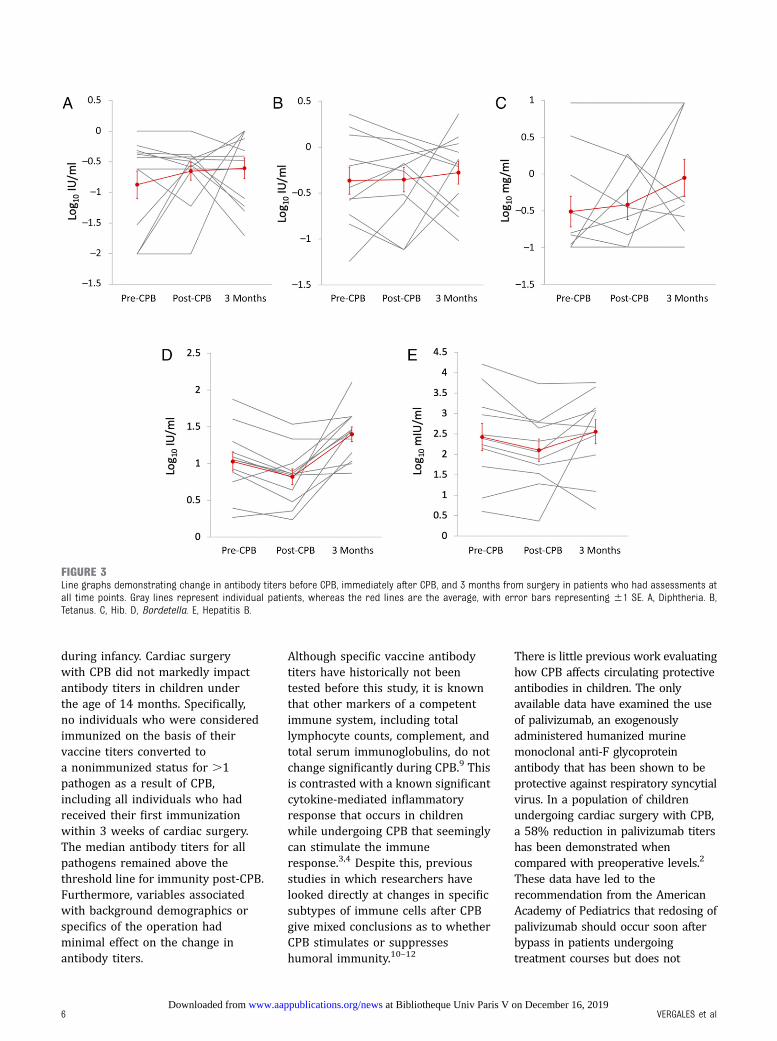
Follow-up vaccine analysis done3 months after surgery wasperformed in 12 patients and isdisplayed in Fig 3. Nine of thosepatients had received additionalimmunizations between surgery and
3 months. There was no significantdifference in antibody titers whencomparing pre-CPB, post-CPB, and3 months after surgery across nearlyall measured pathogens. Theexception to this was Bordetella,which did demonstrate a significantupward trend between all 3 timepoints (P , .001).
DISCUSSION
Currently, there is little guidance onwhether adjustment to the usualvaccination schedules is necessary forchildren with congenital heart diseasewho will require repair with CPB
FIGURE 2Box plots demonstrating mean (*) and interquartile range (box) for assayed values pre-CPB compared with post-CPB in patients who had received justone dose of vaccine. Whiskers demonstrate high and low limits. Dashed lines are the antibody titer level considered to be immunized, representing howchanges in antibody titers affected presumed protective immunity. A, Diphtheria. B, Tetanus. C, Hib. D, Bordetella. E, Hepatitis B.
TABLE 3 Multivariate Linear Regression on Subjects Who Had Received Just One Dose of Vaccine
Variable Diphtheria Tetanus Bordetella Hib Hepatitis B
Time between vaccination and surgery .75 .08 .74 .26 0.88Age at surgery .49 .08 .61 .76 0.69Weight at surgery .41 .72 .19 .12 0.27Bypass time .007 .18 .61 .97 0.55Heterotaxy .44 .87 .49 .72 —
Results of multivariate linear regression on those receiving just one dose of the vaccine. Reported values are P valuesrepresenting strength of the coefficients in the regression equation and thus importance of that variable in the changebetween pre-CPB antibody titers and post-CPB antibody titers. —, not applicable.
PEDIATRICS Volume 145, number 1, January 2020 5 at Bibliotheque Univ Paris V on December 16, 2019www.aappublications.org/newsDownloaded from
during infancy. Cardiac surgerywith CPB did not markedly impactantibody titers in children underthe age of 14 months. Specifically,no individuals who were consideredimmunized on the basis of theirvaccine titers converted toa nonimmunized status for .1pathogen as a result of CPB,including all individuals who hadreceived their first immunizationwithin 3 weeks of cardiac surgery.The median antibody titers for allpathogens remained above thethreshold line for immunity post-CPB.Furthermore, variables associatedwith background demographics orspecifics of the operation hadminimal effect on the change inantibody titers.
Although specific vaccine antibodytiters have historically not beentested before this study, it is knownthat other markers of a competentimmune system, including totallymphocyte counts, complement, andtotal serum immunoglobulins, do notchange significantly during CPB.9 Thisis contrasted with a known significantcytokine-mediated inflammatoryresponse that occurs in childrenwhile undergoing CPB that seeminglycan stimulate the immuneresponse.3,4 Despite this, previousstudies in which researchers havelooked directly at changes in specificsubtypes of immune cells after CPBgive mixed conclusions as to whetherCPB stimulates or suppresseshumoral immunity.10–12
There is little previous work evaluatinghow CPB affects circulating protectiveantibodies in children. The onlyavailable data have examined the useof palivizumab, an exogenouslyadministered humanized murinemonoclonal anti-F glycoproteinantibody that has been shown to beprotective against respiratory syncytialvirus. In a population of childrenundergoing cardiac surgery with CPB,a 58% reduction in palivizumab titershas been demonstrated whencompared with preoperative levels.2
These data have led to therecommendation from the AmericanAcademy of Pediatrics that redosing ofpalivizumab should occur soon afterbypass in patients undergoingtreatment courses but does not
FIGURE 3Line graphs demonstrating change in antibody titers before CPB, immediately after CPB, and 3 months from surgery in patients who had assessments atall time points. Gray lines represent individual patients, whereas the red lines are the average, with error bars representing 61 SE. A, Diphtheria. B,Tetanus. C, Hib. D, Bordetella. E, Hepatitis B.
6 VERGALES et al at Bibliotheque Univ Paris V on December 16, 2019www.aappublications.org/newsDownloaded from

recommend delaying administration ofthe antibody before an operation.13
Palivizumab is a form ofimmunoprophylaxis in which passiveantibody is delivered. This differsfrom vaccinations that purposelystimulate a native immune responsewith the goal of developing memoryand long-term immunity. Thus, it isinteresting that patients who receivedonly 1 round of immunizations, evenat a close interval to surgery, did notdemonstrate an appreciable change.Vaccine antigen, on administration,binds with naive B cells in the lymphnodes or spleen, beginning anextrafollicular reaction that producesa large amount of antibody fromplasma cells nearly immediately afterantigen exposure.14,15 Although theseantibodies are overall low affinity,this mechanism resulting in largeproduction of antibodies couldsuggest why minimal change wasdemonstrated in antibody titersbecause of CPB even in the youngestinfants.
A germinal center reaction follows theextrafollicular reaction and results inthe production of memory B cells. Thisprocess occurs as early as 10 to14 days after antigen exposure,peaking at 4 weeks and resulting inrobust and long-lasting immunity soonafter initial vaccine administration.14,15
Consequently, even if CPB depletescirculating antibodies, as suggested bythe palivizumab studies, enoughplasma cell and memory B-cellresponse can exist early on to repleteantibody levels and potentiallypreserve immunity.
There were individuals who startedout below the immunized threshold
for certain vaccines, specificallyhepatitis B and Hib. Those individualsremained nonimmunized after CPB.This percentage of patients who werenonresponders falls near the reportedrates of individuals who do notmount a response to thosevaccines16,17 but makes individualinterpretation of the CPB effect onthose 2 vaccines somewhatchallenging. This is coupled with thefact that the only patients who lostimmunity as a result of CPB werewith those vaccines specifically.
Survey data have suggested thatupwards of 70% of most majorcardiac surgical programs across thecountry do not have formal policiessurrounding vaccination immediatelybefore or soon after CPB. Owing tothe lack of data or previous work onthis topic, programs that do haveformal policies range anywhere from1 to 6 weeks pre-CPB and 1 to6 weeks post-CPB in limiting vaccineadministration, suggesting significantvariability surrounding a populationthat is known to be at risk for severeinfectious disease.7,18 In our study, wesuggest that alteration of thestandard vaccination schedule forchildren requiring CPB in infancy isunnecessary. More studies in this areawill be helpful in confirming thisconclusion and are essential inprotecting this vulnerable group.
There are several limitations to thisstudy that affect the broaderapplicability. First, antibodies andantibody titers are just 1 marker ofimmunity and were chosen becauseof their ease of measurement and lackof previous data surrounding them inpediatric heart surgery. Still,
reporting antibody thresholds asa function of complete immunity,although standardized, is a simplifiedbinary result, whereas actual immuneresponses are continuous withrespect to antibodies and morecomplex with respect to other aspectsof the immune system. Second,immunodeficiency, especiallysurrounding children with heterotaxyand 22q deletion syndromes, isprevalent in this population. Only 3patients with heterotaxy and nonewith 22q deletion consented to thestudy, making absolute interpretationof the results among those patientschallenging. Targeted studies, lookingspecifically at this population, couldshed light on the immune status afterCPB in these patients. Finally, only 12individuals consented to the thirdblood draw, making completeinterpretation of the long-term effecton immunity challenging to complete.
CONCLUSIONS
Infant vaccine antibody titers areminimally altered by CPB, whetherthe initial or multiple doses of theimmunizations had beenadministered. Titer declines were notassociated with any demographicfactors or modifiable surgicalvariables. This suggests that childrenexpected to undergo congenital heartsurgery with CPB should bevaccinated using the recommendedvaccination schedule.
ABBREVIATIONS
CPB: cardiopulmonary bypassHib: Haemophilus influenzae type b
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2020 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Funded by the Merck Sharp and Dohme Corporation, Merck Investigator Studies Program (No. 53360).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
PEDIATRICS Volume 145, number 1, January 2020 7 at Bibliotheque Univ Paris V on December 16, 2019www.aappublications.org/newsDownloaded from

REFERENCES
1. Husain SA, Pasquali SK, Jacobs JP, et al.Congenital heart operations performedin the first year of life: does geographicvariation exist? Ann Thorac Surg. 2014;98(3):912–918
2. Feltes TF, Cabalka AK, Meissner HC, et al;Cardiac Synagis Study Group.Palivizumab prophylaxis reduceshospitalization due to respiratorysyncytial virus in young children withhemodynamically significant congenitalheart disease. J Pediatr. 2003;143(4):532–540
3. Agirbasli M, Nguyen ML, Win K, et al.Inflammatory and hemostatic responseto cardiopulmonary bypass in pediatricpopulation: feasibility of seriologicaltesting of multiple biomarkers. ArtifOrgans. 2010;34(11):987–995
4. Madhok AB, Ojamaa K, Haridas V,Parnell VA, Pahwa S, Chowdhury D.Cytokine response in childrenundergoing surgery for congenitalheart disease. Pediatr Cardiol. 2006;27(4):408–413
5. Lull ME, Carkaci-Salli N, Freeman WM,et al. Plasma biomarkers in pediatricpatients undergoing cardiopulmonarybypass. Pediatr Res. 2008;63(6):638–644
6. Seghaye M, Duchateau J, Bruniaux J,et al. Interleukin-10 release related tocardiopulmonary bypass in infantsundergoing cardiac operations.
J Thorac Cardiovasc Surg. 1996;111(3):545–553
7. Carrillo S, Woodward C, Taeed R.Immunization of children withcongenital heart disease undergoingcardiopulmonary bypass. CongenitHeart Dis. 2014;9(5):453–495
8. Centers for Disease Control andPrevention. Immunization schedules.2018. Available at: https://www.cdc.gov/vaccines/schedules/index.html.Accessed January 8, 2018
9. Takanashi M, Ogata S, Honda T, et al.Timing of Haemophilus influenzae typeb vaccination after cardiac surgery.Pediatr Int (Roma). 2016;58(8):691–697
10. Tarnok A, Schneider P. Pediatric cardiacsurgery with cardiopulmonary bypass:pathways contributing to transientsystemic immune suppression. Shock.2001;16(suppl 1):24–32
11. Habermehl P, Knuf M, Kampmann C,et al. Changes in lymphocyte subsetsafter cardiac surgery in children. EurJ Pediatr. 2003;162(1):15–21
12. Tajima K, Yamamoto F, Kawazoe K, et al.Cardiopulmonary bypass and cellularimmunity: changes in lymphocytesubsets and natural killer cell activity.Ann Thorac Surg. 1993;55(3):625–630
13. American Academy of PediatricsCommittee on Infectious Diseases;
American Academy of PediatricsBronchiolitis Guidelines Committee.Updated guidance for palivizumabprophylaxis among infants and youngchildren at increased risk ofhospitalization for respiratory syncytialvirus infection [published correctionappears in Pediatrics. 2014;134(6):1221]. Pediatrics. 2014;134(2):415–420
14. Siegrist CA. Vaccine Immunology. In:Plotkin S, ed. Plotkin’s Vaccines, 7th ed.Philadelphia, PA: Elsevier; 2018
15. De Silva NS, Klein U. Dynamics of B cellsin germinal centres. Nat Rev Immunol.2015;15(3):137–148
16. Kubba AK, Taylor P, Graneek B, Strobel S.Non-responders to hepatitis Bvaccination: a review. Commun DisPublic Health. 2003;6(2):106–112
17. Hartkamp A, Mulder AHL, Rijkers GT, vanVelzen-Blad H, Biesma DH. Antibodyresponses to pneumococcal andhaemophilus vaccinations in patientswith B-cell chronic lymphocyticleukaemia. Vaccine. 2001;19(13–14):1671–1677
18. Cabalka AK. Physiologic risk factors forrespiratory viral infections andimmunoprophylaxis for respiratorysyncytial virus in young children withcongenital heart disease. Pediatr InfectDis J. 2004;23(suppl 1):S41–S45
8 VERGALES et al at Bibliotheque Univ Paris V on December 16, 2019www.aappublications.org/newsDownloaded from

originally published online December 4, 2019; Pediatrics Tyson Hekking, Carol Ann Rosenberg, Mark Roeser and James Gangemi
Jeffrey Vergales, Peter Dean, Jacob Raphael, Deborah Frank, Adishesh Narahari,Cardiopulmonary Bypass and Infant Vaccination Titers
ServicesUpdated Information &
019-1716http://pediatrics.aappublications.org/content/early/2019/12/03/peds.2including high resolution figures, can be found at:
References
019-1716#BIBLhttp://pediatrics.aappublications.org/content/early/2019/12/03/peds.2This article cites 16 articles, 1 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/cardiac_surgery_subCardiac Surgeryhttp://www.aappublications.org/cgi/collection/cardiology_subCardiologyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at Bibliotheque Univ Paris V on December 16, 2019www.aappublications.org/newsDownloaded from
originally published online December 4, 2019; Pediatrics Tyson Hekking, Carol Ann Rosenberg, Mark Roeser and James Gangemi
Jeffrey Vergales, Peter Dean, Jacob Raphael, Deborah Frank, Adishesh Narahari,Cardiopulmonary Bypass and Infant Vaccination Titers
http://pediatrics.aappublications.org/content/early/2019/12/03/peds.2019-1716located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2019 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Bibliotheque Univ Paris V on December 16, 2019www.aappublications.org/newsDownloaded from





























