Embed Size (px)
Citation preview

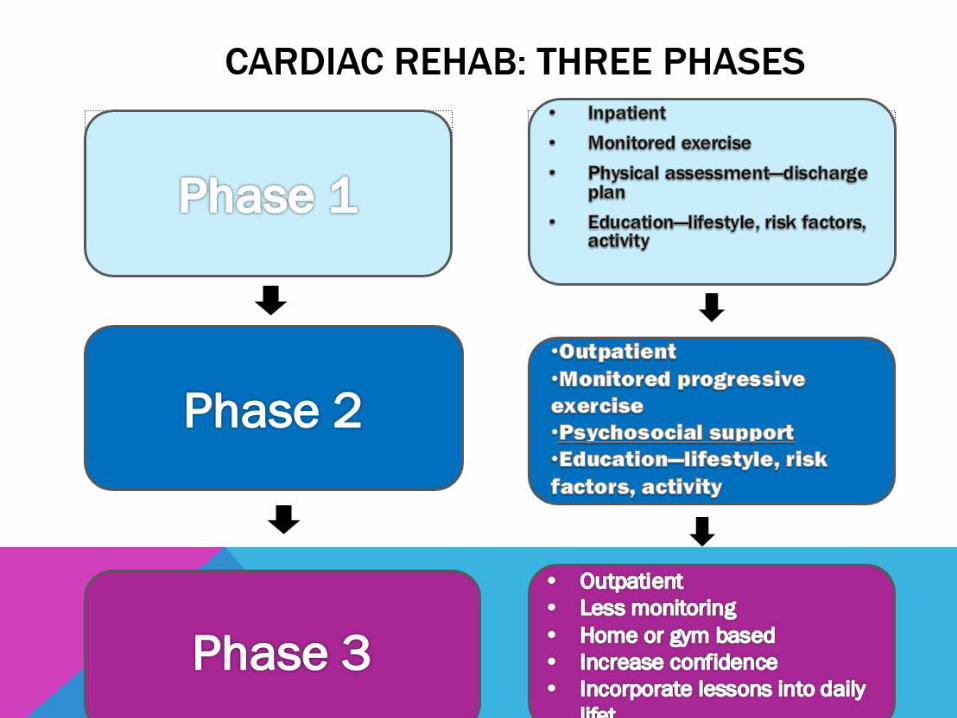
CARDIAC REHABILITATION
J A N E T J O H N S O N D N P, A P R N - B C , C D E , F A A N PC L I N I C A L D I R E C T O R
T H E M A R I E - J O S É E A N D H E N R Y R . K R A V I S C E N T E R
F O R C L I N I C A L C A R D I O V A S C U L A R H E A L T H
2 3 4 E 8 5 T H
N E W Y O R K , N Y
C A R D I O L O G Y N U R S E P R A C T I T I O N E R S Y M P O S I U M
F R I D A Y , N O V E M B E R 1 5 , 2 0 1 9

CARDIAC REHABILITATIONEARLY 20TH CENTURY
Early recommendations following heart attacks: Strict Bed Rest.
Discharge instructions restricted moderately stressful activities for up to a year
The original question 50 years ago was whether exercise was safe for cardiac patients.
“The patient is to be guarded by day and night nursing and helped in every way to avoid voluntary movement or effort.”§ -Thomas Lewis, 1933

CARDIAC REHABILITATIONDEFINED
C O M P R E H E N S I V E , M U L T I - D I S C I P L I N A R Y P R O G R A M O F E X E R C I S E , E D U C A T I O N , A N D B E H A V I O R M O D I F I C A T I O N D E S I G N E D T O R E T U R N P A T I E N T T O F U L L P H Y S I C A L , E M O T I O N A L , P S Y C H O S O C I A L , A N D V O C A T I O N A L F U N C T I O N .

SECONDARY PREVENTION:POST CARDIAC EVENT
S E C O N D A R Y P R E V E N T I O N
F O L L O W U P M E D I C AT I O N S M E D I C A L V I S I T S
E D U C AT I O N / C O U N S E L I N GE X E R C I S ED I E TW E I G H T L O S ST O B A C C O C E S S A T I O NCARDIAC REHAB
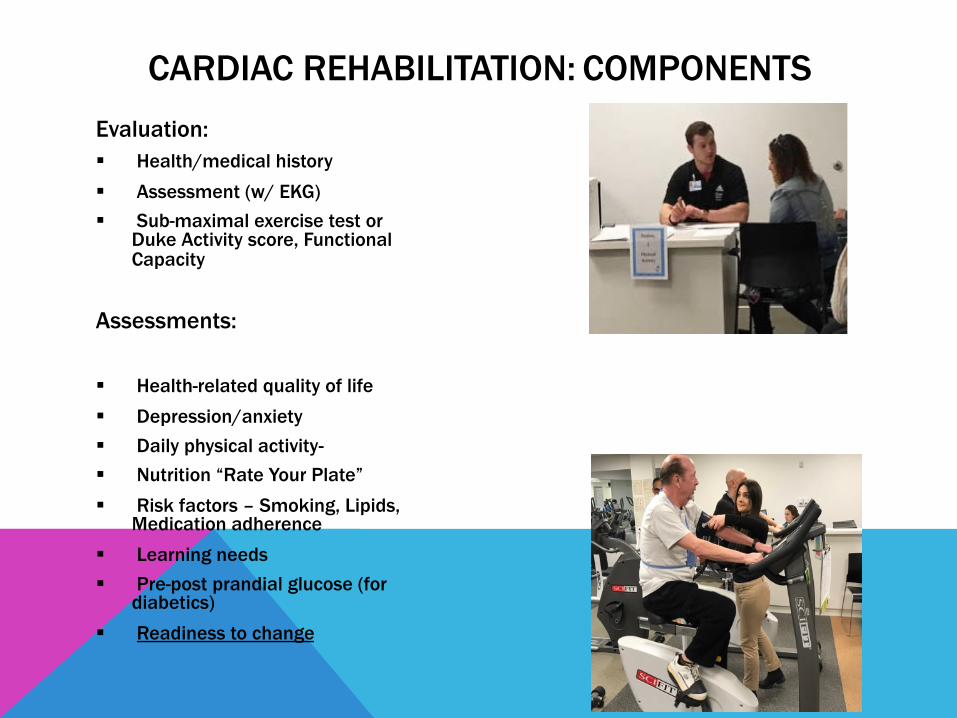
Evaluation:§ Health/medical history§ Assessment (w/ EKG) § Sub-maximal exercise test or
Duke Activity score, Functional Capacity
Assessments:
§ Health-related quality of life§ Depression/anxiety§ Daily physical activity-§ Nutrition “Rate Your Plate”§ Risk factors – Smoking, Lipids,
Medication adherence§ Learning needs§ Pre-post prandial glucose (for
diabetics) § Readiness to change
CARDIAC REHABILITATION: COMPONENTS

Interventions:§ 60 minute group exercise session with telemetry-monitor and progressive exercise, 2 or 3 times/ week24-36 sessions§ Psycho-social support, Monthly Support group
§ Heart Healthy Education – Lectures/ 1:1/Videos* Nutrition* Exercise* Risk factors- Cognitive Behavior Therapy* Tobacco cessation* Diabetes control* Stress management: Mindfulness * Medications
Follow-Up Assessment/Evaluation§ Re-administer assessment tools to measure
outcomes
§ Documentation of any clinical issues with patient during rehabilitation
§ Summary report to patient and referring provider
CARDIAC REHABILITATION: COMPONENTS

INDIVIDUAL TREATMENT PLAN


CARDIAC REHABILITATION
W H O ?
W H Y ? ( A N D W H Y N O T( B A R R I E R S )
W H E R E ?
W H A T A R E T H E F U T U R E P L A N S ?

CARDIAC REHABILITATION :WHO TO REFER

CARDIAC REHABILITATION: INDICATIONS
Class I Recommendation (ACC/AHA/ESC):
§ Myocardial infarction (within 12 months of hospital discharge)
§ Stable angina
§ Percutaneous Coronary Intervention
§ Coronary Artery Bypass
§ Valve repair/replacement
§ Heart/heart-lung transplant
§ Peripheral Artery Disease
§ Heart Failure§ LVEF ≤ 35%; NYHA II-IV, includes LVAD

CARDIAC REHAB--CONTRAINDICATIONS
Unstable angina
Acute MI (within 2 days)
Recent change in the resting ECG suggesting significant ischemia
SBP>200 or DBP>110 at rest
Symptomatic severe aortic stenosis or other valvular disease
Arrhythmia uncontrolled
Decompensated symptomatic heart failure
Heart block without PPM
Active pericarditis/myocarditis
Acute pulmonary embolus or pulmonary infarction
Diabetes mellitus uncontrolled
Acute noncardiac disorder that my affect exercise performance or may be aggravated by exercise (infection, thyrotoxicosis)
Physical disability that would preclude safe and adequate exercise performance
AACVPR. Guidelines for Cardiac Rehabilitation and Secondary Prevention Programs. Fifth Edition, Human Kinetics, 2013.

CARDIAC REHABILITATION :WHY?
EVIDENCE-BASED MEDICINE

CARDIAC REHABILITATION: OUTCOMES
• 20-30% reduction in all-cause mortality rates
• Reduction in the risk of death due to a cardiovascular cause• Decreased mortality at up to 5 years post participation
• Reduced symptoms (angina, dyspnea, fatigue)
• Reduction in nonfatal recurrent myocardial infarction over median follow-up of 12 months
• Improved health factors like lipids, blood pressure, BMI, Insulin sensitivity
• 31% reduction in hospital admission
CARDIAC REHABILITATION: OTHER BENEFITS
§ Improved Quality of Life
§ Reduced depression/anxiety
§ Reduced apprehension regarding physical exertion
§ Increased physical work capacity
§ Obtain skills/knowledge on how to change lifestyle to help manage disease process
§ Improved adherence with preventive medications“ Cardiac Rehab Centers have become disease management and secondary
prevention centers that assist in Healthy Living”

CARDIAC REHABILITATION: PHYSIOLOGIC MECHANISMS
§ Slow/reduce the severity of atherosclerosis§ Improved endothelial function
* Increased nitric oxide * Reduced angiotensin II and endothelin production
§ Improved vasomotor function (enhanced vasodilation)
§ Reduction in inflammatory markers * CRP
§ Reduced ischemia* Reduced RPE at given work rates* Increased myocardial flow
§ Anti-thrombolytic activity* Reduced platelet aggregation* Decreased blood viscosity/increased blood volume

WHY REFER? PERFORMANCE MEASURES MUST BE LINKED TO MEANINGFUL PATIENT OUTCOMES

BARRIERS TO UTILIZATION1,2
Despite these benefits, participation in cardiac rehab remains low,
Ranging from 19% to 34% in a national analysis with
strong state-by-state geographic variations and differences by cardiac diagnosis.(Mayo Clinic Proceedings, 2016),

WHY NOT – BARRIERS TO CARDIAC REHAB
• Lack of referral from the patient’s physician
• Lack of perceived need for rehabilitation/awareness
of CR (physician and patient)
• Limited, or no health care coverage (cost/ co-pays)
• Limited follow-up or facilitation of enrollment after
referral
• Hours of operation conflicting with work/family demands
• Scarcity of programs in rural areas and/or low income communities
• Distance to CR facility from patient’s home
• Access to public transportation or parking issues
• Male gender-dominated programs and little racial staff diversity
• Language problems and cultural beliefs
• Low Reimbursement Rates

PURPOSE: To assist QI Team and CR Programs to put systems and strategies in place that target improved care for more eligible patients. PROVIDES Change Concepts, Change Ideas, and Tools and Resources
Make CR a Health System PriorityEstablish a ChampionUse Referrals as Quality of Care
indicatorEngage Care Team and Ensure
buy-in
Incorporate Referrals into standardized process…order sets, discharge orders, morning discharge rounds
Use Data to drive Improvements to CRDetermine Inpatient and Outpatient
referral metricsDashboard with CR Referrals, Goals
and Performance

Educate Patients about the Benefits of Cardiac Rehab “Liasion”, brochures
Reduce delay from discharge to CR –goal 12 days **
Use data to drive improvementReduce cost- assist with out of
pocket $, philanthropic fundImprove efficiency of enrollment,
flexible modelsUse Clinician Follow-up
* *1 day delay in starting CR, there is ~1% less likelihood of patient enrolling
Identify population at risk for low engagement
Improve patient engagement- use of financial and motivational incentives/gift cards for completion of certain number of sessions
Automatic remindersAmbassador or “sponsor” graduate

CARDIAC REHABILITATION :MOUNT SINAI
WHERE TO REFER?

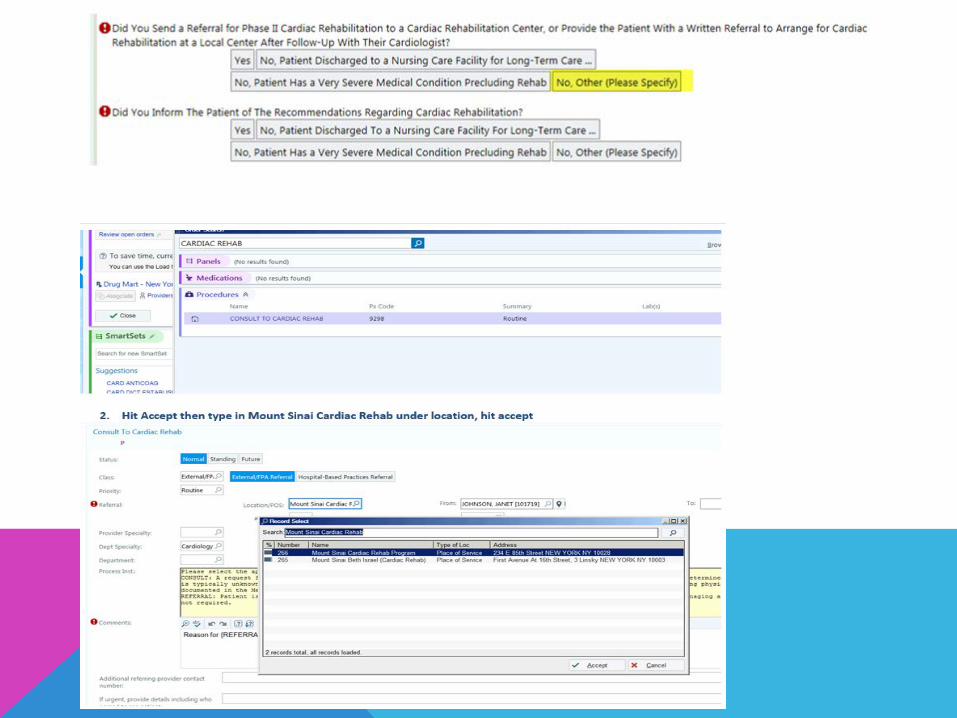

CARDIAC REHABILITATION: MOUNT SINAIReferral Process
OSH Fax Referral Epic Order Inpatient and MSH outpatient provider
Fax directly to cardiac Consult to Cardiac Rehab
rehabilitation dept.
Cardiac Rehab Patient Coordinator- call patient to confirm interest
Cardiac Rehab Clinical manager
Patient is contacted, program is explained to patient, insurance is verfied, and patient is then scheduled to begin
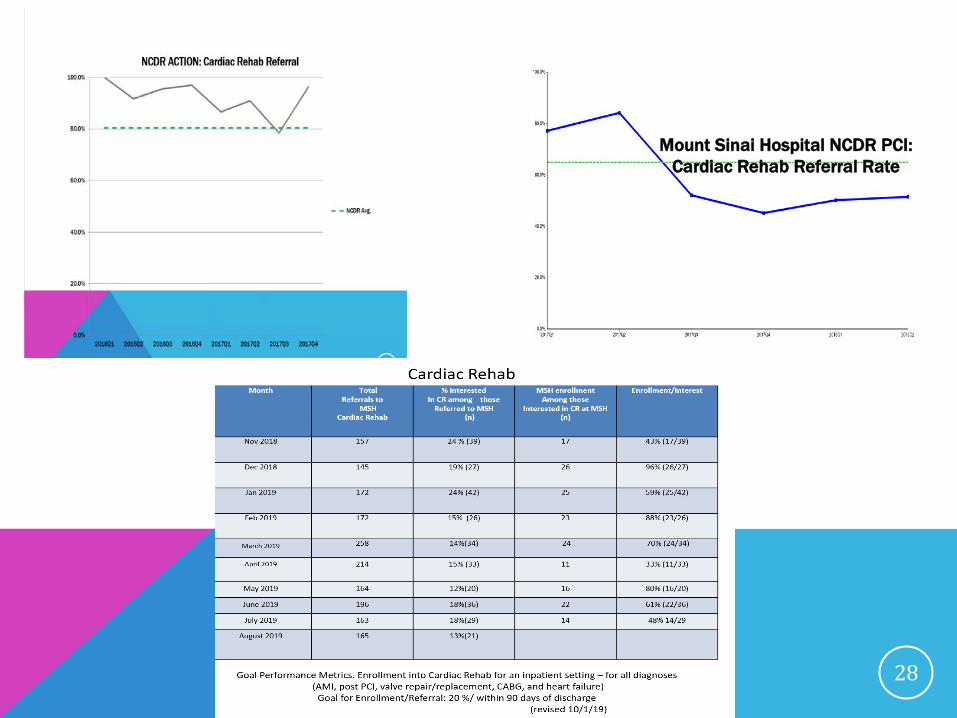
28
NCDR Avg.
Mount Sinai Hospital NCDR PCI: Cardiac Rehab Referral Rate





FUTURE PLANS?


DIRECT PHYSICIAN SUPERVISION FOR CR, PR, & ICRFEDERAL REGISTER, VOL. 76, NO. 230, NOVEMBER 30, 2011, PGS 74580-81:42 CFR 410.27
Therapeutic outpatient hospital or CAH services and supplies incident to a physician’s or nonphysician practitioner’s service: Conditions:
(D) For pulmonary rehabilitation, cardiac rehabilitation, and intensive cardiac rehabilitation services, direct supervision must be furnished by a doctor of medicine or a doctor of osteopathy, as specified in 410.47 and 410.49, respectively;
This remains in effect until January 1, 2024 when the BBA of 2018 mandates that nonphysician practitioners will be allowed to meet the requirement for direct physician supervision for CR, PR, and ICR services.

FUTURE PLANS♥ Inpatient Exercise Physiologist specialist « Liaison « for Outpatient Cardiac
Rehabilitation
♥ Reducing the Delay Between Hospital Discharge and Enrollment in to Outpatient CR
♥ Success Board
♥ Extended hours
♥ Expansion of Space
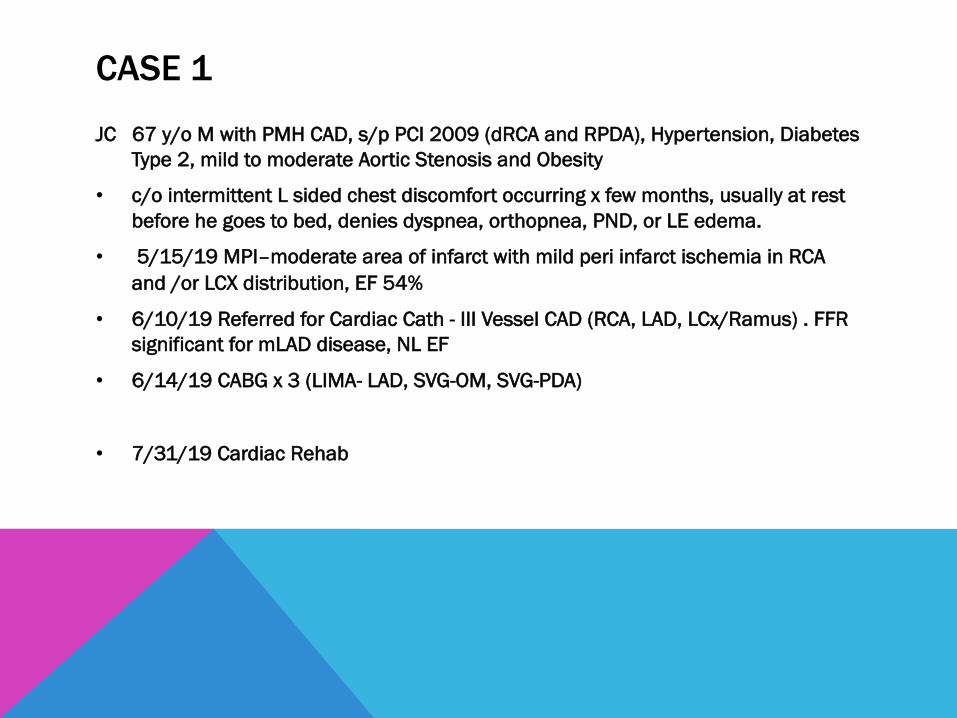
CASE 1
JC 67 y/o M with PMH CAD, s/p PCI 2009 (dRCA and RPDA), Hypertension, Diabetes Type 2, mild to moderate Aortic Stenosis and Obesity
• c/o intermittent L sided chest discomfort occurring x few months, usually at rest before he goes to bed, denies dyspnea, orthopnea, PND, or LE edema.
• 5/15/19 MPI–moderate area of infarct with mild peri infarct ischemia in RCA and /or LCX distribution, EF 54%
• 6/10/19 Referred for Cardiac Cath - III Vessel CAD (RCA, LAD, LCx/Ramus) . FFR significant for mLAD disease, NL EF
• 6/14/19 CABG x 3 (LIMA- LAD, SVG-OM, SVG-PDA)
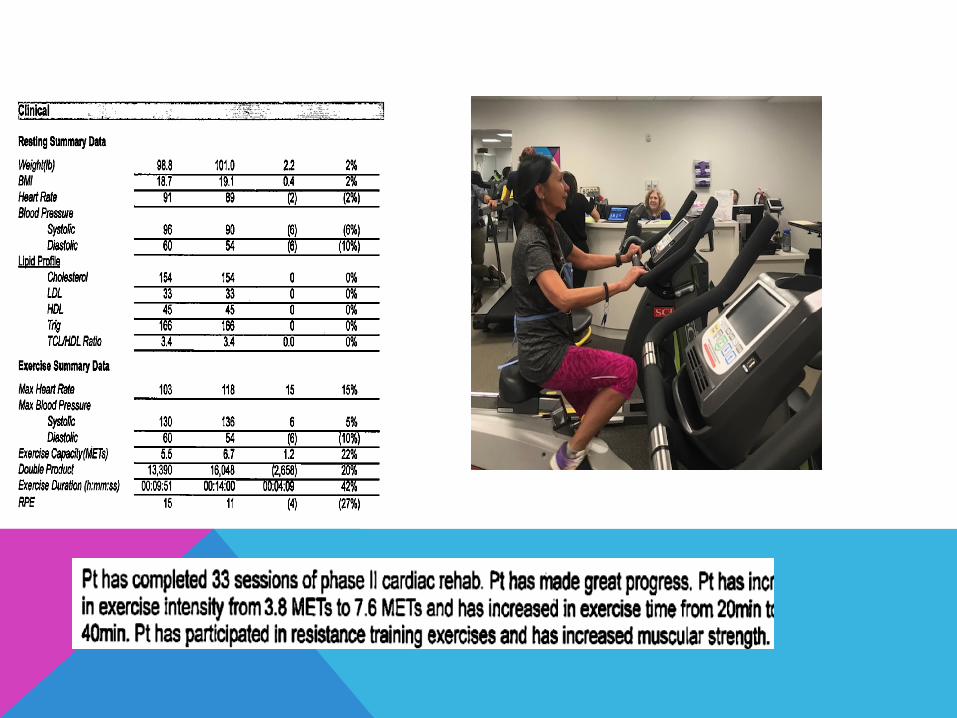
• 7/31/19 Cardiac Rehab

“THIS IS THE BEST I FELT IN 50 YEARS”

CASE 2
SZ 71 y.o. female was in the Philippines x 7 weeks, where she became ill with a dry cough and nasal congestion. On her return went to an urgent care facility, with symptoms of URI, where a new murmur was found.
• Echo was done showing ruptured chordae with 3+ MR, but no vegetations.
• 3/15/19 seen at ED presented with new onset shortness of breath, congestion, weakness and palpitations on minimal exertion and at rest. Repeat TTE showed partial flail of mitral valve P2, moderate to severe MR, EF= 71%. Medical management attempted, but continued with severe symptoms.
• 3/22 Pre-op cardiac Cath Procedure: Small Access Mitral Valve Repair; Patent Foramen Ovale Closure
• 5/10 Cardiac Rehab
CONCLUSIONS
• C A R D I A C R E H A B I L I TAT I O N I S A N I N T E G R A L C O M P O N E N T O F S E C O N D A R Y P R E V E N T I O N
• C A R D I A C R E H A B H A S S I G N I F I C A N T M O R TA L I T Y A N D O T H E R B E N E F I T S
• C A R D I A C R E H A B I S O F T E N U N D E R -U T I L I Z E D
• S T R AT E G I E S T O I N C R E A S E C A R D I A C R E H A B U S E H AV E R E S U LT E D I N I M P R O V E D R E F E R R A L S , E N R O L L M E N T A N D AT T E N D A N C E
THANK YOU TO THE CARDIAC REHAB TEAM





























