Embed Size (px)
Citation preview

Cardiac DysrhythmiasNuro 438February 2015

Learning ObjectivesAt the completion of this presentation, the nursing student will be able to successfully Describe cardiac anatomy and physiology
Describe the function of the heart, including circulation and automaticity
Describe and define the major cardiac waves in an EKG
Define normal sinus rhythm
Differentiate between rate, conduction, atrial, and ventricular arrhythmias
Recognize life-threatening dysrhythmias
Identify nursing considerations related to various cardiac dysrhythmias
Differentiate types of medications to treat arrhythmias
Identify risks for cardiac arrhythmias
Identify adverse effects associated with cardiac dysrhythmias
Analyze EKG Rhythm strips
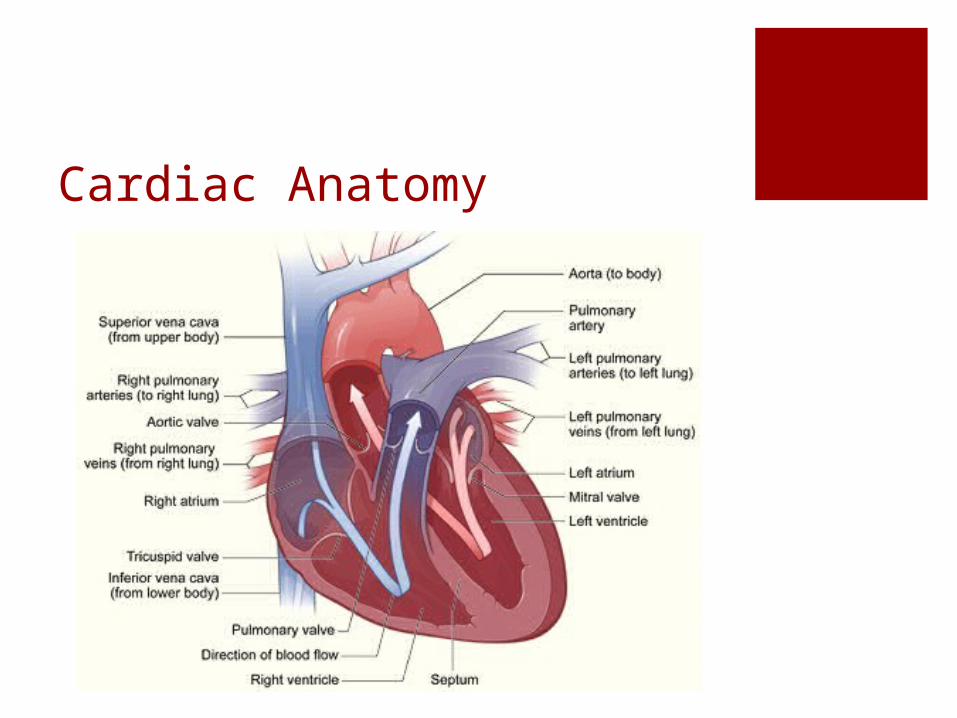
Cardiac Anatomy

Cardiac Anatomy4 Chambers, 2 Atria, 2 Ventricles
4 Valves
Acts as a PUMP
Receives deoxygenated blood from body, pumps to lungs
Receives oxygenated blood from lungs, pumps to body

Cardiac Circulation

Cardiac Function
Heart functions a pump to deliver blood to the body
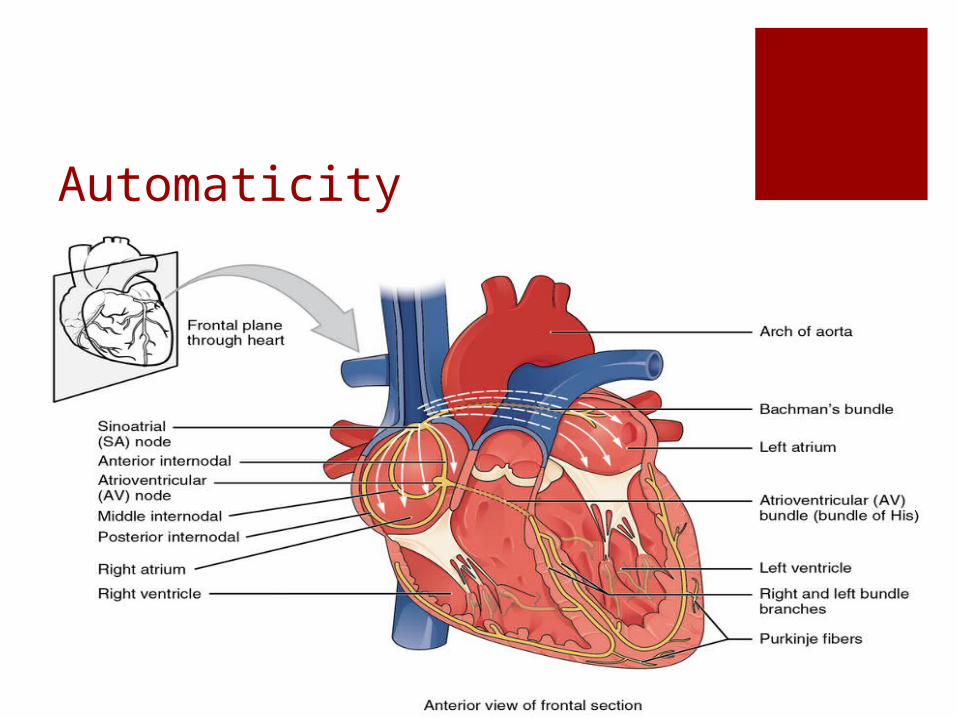
Automaticity
Impulse GenerationUnder Usual circumstances
Impulse generated from pacemaker cells in SA node
Impulse then travels to AV node
Impulse then travels to Bundle of His
Impulse then travels to Right and Left Bundle Branches
Impulse travels to Perkinje Cells that innervate ventricles

Components of an EKG

EKG Graph
X Axis = time Y Axis = amplitude
Displays electrical activity of heart
Electrical impulse precedes contraction
Depolarization and repolarization are depicted as waves Atrial Depolarization = P wave Atrial repolarization occurs during ventricular depolarization Ventricular depolarization = QRS complex Ventricular repolarization = T wave

EKG BasicsBipolar lead: positive and negative electrode.
Measures electrical potential between the electrodes
AKA ‘Standard Limb Leads’
Leads I,II,III
Used to monitor only for dysrhythmias
Lead II most commonly used

Telemetry PlacementRed = Brake (right), Green =
Gas (left)
Smoke (black) over Fire (red), Snow (white) on the Trees (green)
Stars and Stripes

Lead II

12 Lead EKG3 Standard (bipolar) Limb Leads
3 Augmented (unipolar) Leads (aVR, aVL, aVF) Triaxial reference- measures the difference in
electrical potential between one of three extremity electrodes and the central terminal
6 Precordial (unipolar) Leads (V1, V2, V3, V4, V5, V6)

aVR, aVL, aVF
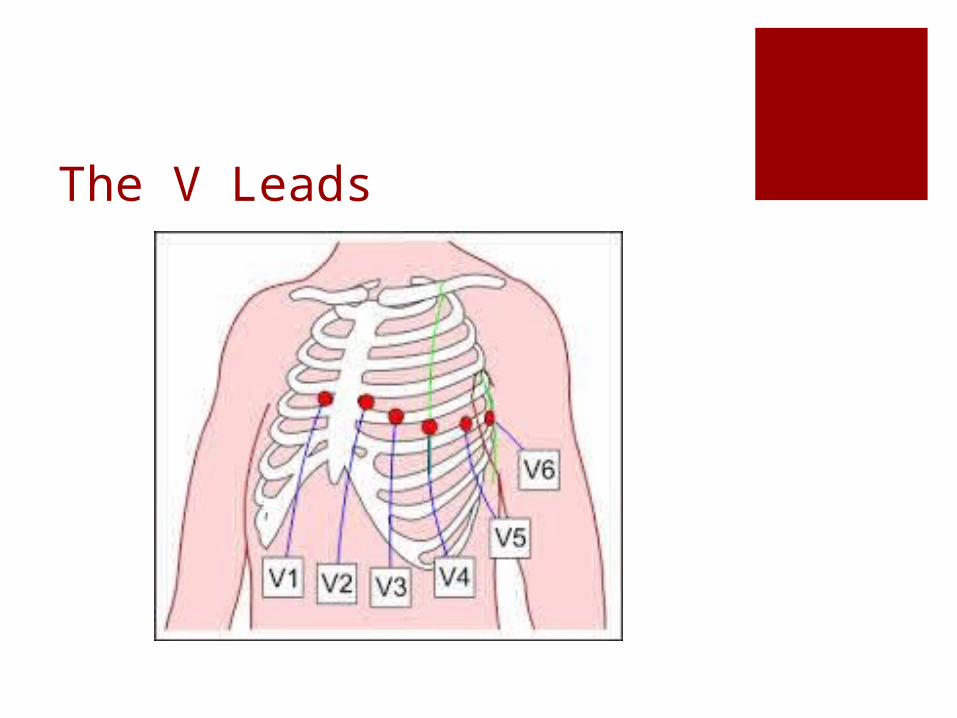
The V Leads

Cardiac Waves

The P wavePacemaker is SA node,
rate 60 - 100
Correlates with atrial depolarization (begins in SA node moves R-> L and down)
PR interval 0.12-0.2
Determine atrial rate
Compare atrial rate to ventricular rate

The QRS ComplexRepresents normal
depolarization of the ventricles
Normal duration 0.06- 0.12
Measured from Q wave (first deviation from isoelectric line) to S wave (the return to isoelectric line)
Abnormal QRS is abnormal depolarization BBB Ventricular pre-excitation Cardiac pacemaker

The T WaveRepresents Ventricular
repolarization
Occurs during end of ventricular systole
Typically in same direction as QRS complex
Lasts 0.10 – 0.25

U WaveFinal stage of
repolarization, thought to be repolarization of Perkinje Fibers
Not usually seen
May indicate Hypokalemia Cardiomyopathy LVH Dig toxicity

EKG Paper
At the 25 mm speed, Each mark at top is 3 secondsThere are three large boxes between each markEach large box is 1 second or 25 mmEach large box has 5 medium boxes in itEach medium box is 0.2 seconds or 5 mmEach medium box is made up of 5 small boxes (or dots)Each small box (dot) = 0.04 seconds or 1 mm

EKG Paper

Steps to Interpreting Cardiac RhythmsDetermine the Heart Rate
Determine the Regularity
Identify and analyze P waves or flutter
Determine PR interval and AV conduction
Identify and analyze QRS complex
Determine site of origin of dysrhythmia
Identify dysrhythmia
Evaluate significance of dysrhythmia

Determine the Heart RateThe Six-second Method
Most common/least accurate Simplest, quickest
Heart Rate Calculator
The Rule of 300 Must be regular
R-R Interval Method Rhythm must be regular Distance between peaks of 2 R
waves and /60

Describe the Rate & RhythmNormal = 60-100
Tacchycardia >100
Bradycardia <60
Regular
Irregular
Regularly-irregular

Sinus ArrhythmiasST = HR >100
SB = HR ,60

Steps to Interpreting Cardiac RhythmsDetermine the Heart Rate
Determine the Regularity
Identify and analyze P waves or flutter
Determine PR interval and AV conduction
Identify and analyze QRS complex
Determine site of origin of dysrhythmia
Identify dysrhythmia
Evaluate significance of dysrhythmia

Measuring the Waves

PR IntervalRepresents progression of electrical
impulse from the SA node or an ectopic pacemaker (in atria or AV junction) through entire conduction system of the heart to the ventricular myocardium
Normal duration 0.12 – 0.20
PR >0.20 represents delayed conduction of impulse

Irregular P WaveRemember P wave represents
atrial depolarization
Irregular P represents altered, damaged, or abnormal atria Increased Right Atrial Pressure
or hypertrophy as seen in COPD and CHF = tall peaked P wave
Increased left atrial pressure or hypertrophy = wide notched P wave

Ectopic P WaveElectrical impulse for ectopic P wave originated
outside SA node or in AV junction
Occur in PAC’s Atrial tacchycardia SVT

PAC’s Premature Atrial Contraction
P wave followed by normal QRS
Generally followed by noncompensatory pause
P waves vary, PR intervals normal
AV Ratio 1:1 Conduction

Causes of PAC’s Increased sympathetic tone
Infection
Emotional Stress
Stimulants
Medications; epinephrine
Hypoxia
Digitalis toxicity
ACS or CHF

QRS ComplexRepresents normal
depolarization of the ventricles
Onset is point where first wave (Q) deviates from isoelectric line
End is where last wave (S) returns to isoelectric line
Duration 0.06 – 0.12

Irregular QRSRepresents
abnormal depolarization of ventricles
Irregular QRS present in Bundle Branch Block Ventricular
preexcitation Cardiac pacemaker

QT IntervalRepresents time it takes for
ventricles to depolarize and repolarize
Prolonged QT associated with pericarditis, myocarditis, MI, LVH, hypothermia, CVA, increased IC trauma or hemorrhage, medication SE, electrolyte imbalances (K, Ca), or liquid protein diets

ST SegmentRepresents early part of
repolarization of right and left ventricles
Duration < 0.20
Normally ST segment is flat
Elevation can be evidence of myocardial ischemia or infarction, coronary vasospasm, pericarditis, LBBB, LVH, raised ICP

Steps to Interpreting Cardiac RhythmsDetermine the Heart Rate
Determine the Regularity
Identify and analyze P waves or flutter
Determine PR interval and AV conduction
Identify and analyze QRS complex
Determine site of origin of dysrhythmia
Identify dysrhythmia
Evaluate significance of dysrhythmia
Arrhythmias Rate Arrhythmias
Tachycardia Bradycardia
Atrial Arrhythmias Afib/Aflutter WPW SVT
Conduction Arrhythmias Bundle Branch Blocks AV Conduction Block (1st, 2nd, 3rd Degree)
Life Threatening Arrhythmias V Fib Complete Heart Block Asystole

Living Arrhythmiashttps://www.youtube.com/watch?
v=TJR2AfxVHsM

Atrial ArrhythmiasAtrial Tacchycardia
Atrial fibrilation
Atrial flutter
Supra Ventricular Tacchycardia
Wolf-Parkinson-White
8 Steps ID P or F waves Conduction ratio, is every P followed by QRS
Atrial TachycardiaRate is usually 160-240 beats
Type of SVT, where generation for impulse is outside SA node
A Fib and Aflutter are most common forms
P waves are uniform
PR intervals are normal
AV conduction is 1:1

Atrial TachycardiaClinical significance
Dependent on presence and extent of heart disease
Palpitations, nervousness, anxiety Perfusion Syncope Workload of heart
Nursing Assessment

Atrial Tachycardia

A FlutterCauses
Cardiomyopathy Atrial dilation Valve Disease Thyrotoxicities Hypoxia CHF ETOH Abuse

A Flutter Risks; Incomplete emptying of ventricles
Thrombi formation Loss of atrial kick Syncope, hypotension CHF
Treatments Beta Blockers CCB Digoxin Warfarin Cardioversion if uncontrolled Ablation

Atrial Flutter Impulse generated by ectopic pacemaker or reentry
pathway
F waves have a saw-tooth appearance
Rate; Atrial 240-360, Ventricular half the atrial rate
Rate is regular
Normal P waves absent
Unable to measure PR intervals
Expressed as ratio 4: 1 Flutter

Atrial FibrillationAtrial Rate 350-600
Ventricular rate < 100 = controlled, >100 = uncontrolled
Irregularly irregular rate
P waves absent, F waves absent
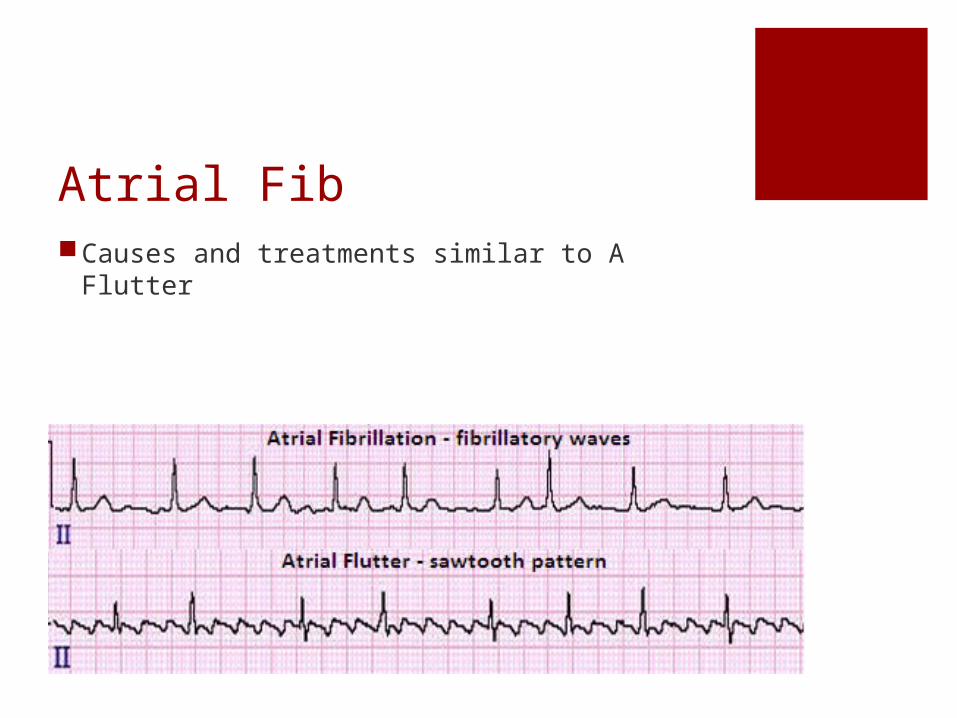
Atrial FibCauses and treatments similar to A Flutter

SVTRapid rhythm (>100) that generated outside
the ventricles
AKA Paroxysmal Atrial Tach (PAT)
Symptoms Palpitations Lightheadedness Dizziness Maybe symptomless, self limiting
Treatments
Beta Blockers, CCB,antiarrhythmics

SVT

WPWVentricular pre-excitation; early activation of
ventricles by impulse that bypasses the AV node
Impulse can be generated in accessory pathway or bypass tract that abnormally
Most frequent AV bypass tract in WPW is Bundle of Kent
Presence of Delta wave

Wandering Atrial Pacemaker
Dysrhythmia originating in multiple pacemaker sites that shift between SA node and AV junction
Rate 60 – 100
Irregular
P waves vary in size and shape
PR intervals are normal to very short
AV Conduction ratio 1:1

Wandering Atrial Pacemaker

Conduction Arrhythmias
Conduction Block/ AV Block
Bundle Branch Block

AV BlocksFirst Degree AV Block
Second Degree Type I AV Block
Second Degree Type II AV Block
Third Degree AV Block

First Degree AV BlockDelay in conduction of electrical impulse,
usually through the AV node
Most common Heart Block
Prolonged PR (> 0.20)
Rate and Rhythm Regular
AV Conduction 1:1
Causes 1* AV Block Acute Inferior Wall MI Ischemic Heart Disease Digitalis Toxicity Medications (B Blockers, CCB) Hyperkalemia

First Degree AV Block

Second Degree Type I AV BlockAKA Wenckebach
Usually temporary condition, and asymptomatic
Prolonging PR form one QRS to the next until one QRS is not conducted or “dropped” then pattern starts over again
P to P intervals are regular
R to R intervals are irregular
More P waves than QRS complexes
Causes; Acute inerior wall MI, Ischemic heart disease, Dig Toxicity, BB, CCB, Hyperkalemia

Second Degree AVB, Type I

Second Degree Type II AV BlockDysrhythmia with constant P-R interval with
missing QRS complexes
Complete block of conduction in one bundle branch and an intermittent block in the other bundle branch
Can present as pattern, ie 2:1 block or 3: 1 block OR without pattern of QRS/ unstable QRS
Causes; Damage to Bundle Branches p MI,
Very high potential to convert to Third Degree (Complete) Heart Block
Excessively slows HRMay require pacemaker, Atropine not effective
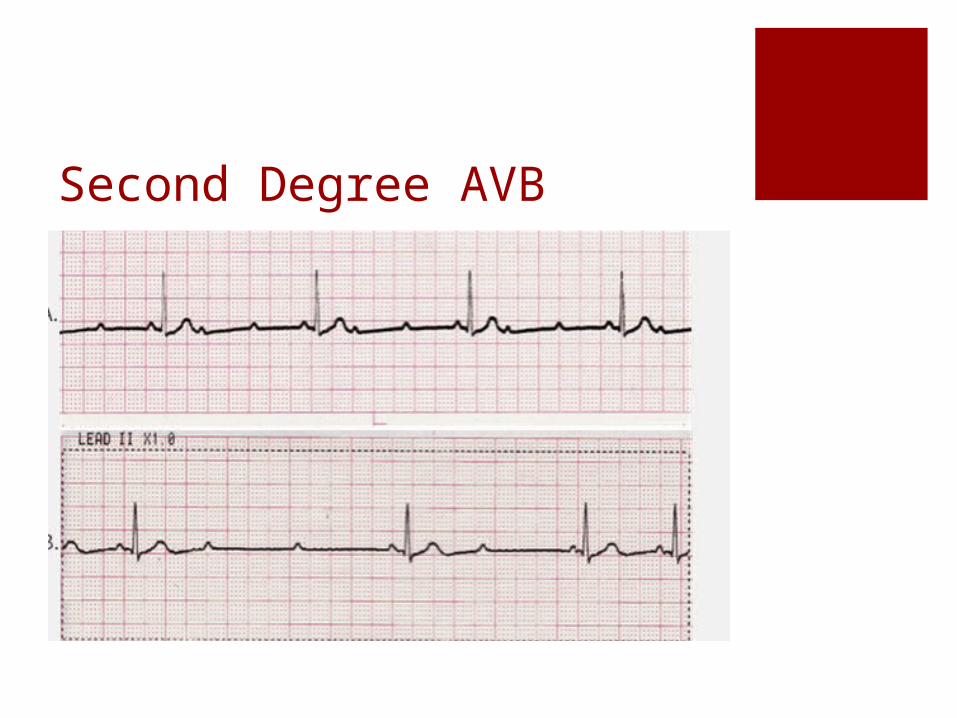
Second Degree AVB

Third Degree COMPLETE HBComplete absence of conduction of electrical
impulse through AV node, Bundle of His, and BB
Atria rhythm independent from Ventricular rhythm; Regular P-P and regular R-R
LIFETHREATENING Rhythm, will lead to asystole
Requires Pacing
Causes; Inferior wall MI, Ischemic Heart Disease, Medications (Dig, BB, CCB), hyperkalemia

Complete Heart Block

Treatment of CHBCardioversion or Defibrillation
Transcutaneous pacing for symptomatic bradycardia
Medications Atropine Vasopressors CCB BB
Nursing Assessment

Bundle Branch Block Irregular conduction or block of electrical
pathway through bundle branches
Ventricles do not contract simultaneously
QRS > 0.12, appears “notched”

Ventricular Arrhythmias
PVC’s
Ventricular Tachycardia
Ventricular Fibrillation
Premature Ventricular Contraction, PVC’SAbnormally wide, bizarre QRS complex, not
associated with P wave
Electrical impulse generated in ventricle, Bundle Branch, or Perkinje Fibers
Does not lead to contraction of ventricles, therefor not “perfused”
Usually followed by compensatory pause
Can be observed with or without a pattern

Causes of PVCs Increased Catecholamine and increased sympathetic
tone
Stimulants
Amphetamine and cocaine
Myocardial ischemia or infarction
CHF
Hypoxemia
Acidosis
Dig Toxicity
Hypokalemia
Hypomagnesemia

Significance of PVCs Isolated PVC without hx heart disease are
usually insignificant, and require no treatment
May indicate presence of ventricular abnormality
Can lead to V tach or V fib

Single PVC

Ventricular Bigeminy
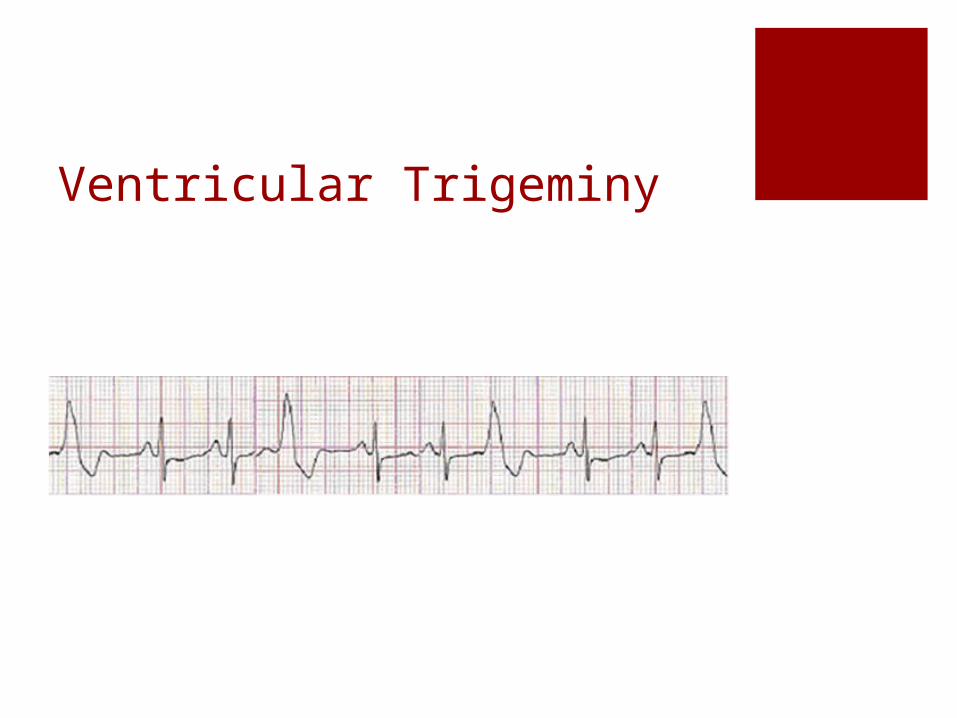
Ventricular Trigeminy

Couplet

Run PVC
Ventricular TachycardiaAKA V Tach
Dysrhythmia originating in an ectopic pacemaker in the bundle branches, perkinje fibers, or ventricular myocardium
Rate 100 – 250 bpm
P wave absent
QRS abnormally wide and bizarre

V Tach

Causes of V TachSignificant Cardiac Disease
CAD ACS Cardiomyopathy LVH
Dig Toxicity
QT interval Prolongation
Electrolyte disturbances
Liquid protein diets
Clinical Significance of V TachDetermine inset and termination
More than 3 PVCs is sustained V Tach
Can be short, nonsustained and asymptomatic
Increased frequency can lead to Ventricular Fibrillation which is LIFETHREATENING
PULSELESS V TACH IS TREATED THE SAME AS V FIB!

Ventricular FibrillationNo coordinated ventricular beats are present
No P wave or QRS complexes noted
Electrical Chaos in Heart
Ventricles ‘contract’ at rate of 300 – 500 bpm
EMERGENCY
Cardiac output CEASES
Nursing Considerations

V FIB

AsystoleTotal Absence of electrical activity in heart
Pt is clinically dead
Absence of P wave and QRS complex
Flat line
Remember, if your patient is speaking to you then they are NOT in a systole

TreatmentsCardioversion and Defibrillation
Medical Management Atropine Vasopressors Calcium Channel Blockers Beta Blockers
Nursing Considerations Oxygen, Pain management

AtropineBlocks parasympathetic nervous system
influence on the heart
Accelerates SA node firing rate
Increases HR
Increases conduction velocity
Administered by IV bolus
Used in Symptomatic Bradycardia Second Degree Type I AVB Second Degree 2:1 AVB Third Degree AVB with narrow QRS complexes

Atropine Ineffective in Second Degree Type II AVB
Advanced AVB with wide QRS complexes Third Degree AVB with wide QRS Complexes
Use with Caution Acute MI Worsening myocardial ischemia Heart Transplant patient

VasopressorsCause vasoconstriction on arterioles and
venous circulation
Improves blood pressure
Increases HR and Strength of Contraction Epinephrine Vasopressin (DOC in asystole) Dopamine Norepinephrine Dobutamine Isopreterenol

AntidysrhythmicsAdenosine; depress AV node and Sinus node
activity SVT, Tachycardia Will not terminate Afib/flutter but will slow rate
Amiodarone; Affects NA, K, and Ca channels SVT VT Vfib
Lidocaine; Widely used, ? Effectiveness in VT SE; altered consciousness, seizures, bradycardia
Procainamide; supresses atrial and ventricular dysrhythmias by slowing conduction VT, control of rate in AF/AF, PVST
Calcium Channel BlockersDiltiazem and Verapamil
Slow conduction and increase conduction time through AV node
Used in Afib and A flutter with rapid ventricular response
Contraindicated in 2nd and 3rd Degree AVB With Beta Blocker Therapy Use with caution on CHF and hypotension

Beta BlockersDecrease HR and BP
Used in SVT To control rate in Afib Aflutter

Time for a GameEKG Jeopardy!
jeopardylabs.com/play/ekg-jeopardy#.VOLPYmdso-w.gmail
Fifteen Question EKG Rhythm Strip Analysis
http://www.12leadecg.com/arrhythmias/index.cfm

Wave Matching1. Ventricular
Depolarization
2. Irregular Ventricular Beat
3. Atrial Depolarization
4. 0.12-0.20
5. Ventricular Repolarization
6. Backup pacemaker Rate 40-60
7. Early atrial beat
8. Pacemaker site
9. 0.06-0.12
10. Sets Normal Heart Rate
A. AV Node
B. T wave
C. PAC
D. SA Node
E. PVC
F. P wave
G. QRS Complex

Take Home PointsEKG is measurement of ELECTRICAL activity
Look at the patient
Irregular activity can progress from asymptomatic to life threatening
Causes are similar (electrolytes, hypoxia, ischemia…)
Treatments also very similar (BB, CCB, antiarrhythmic)

Referenceshttp://lifeinthefastlane.com/ecg-library/
http://ekg.academy/learn-ekg.aspx?seq=11&courseid=315
http://my.clevelandclinic.org/services/heart/patient-education





























