Embed Size (px)
Citation preview

1
Cardiac Catheterization is Cardiac Catheterization is Unnecessary in the Evaluation of Unnecessary in the Evaluation of
Patients with Pulmonary Patients with Pulmonary Hypertension:Hypertension:
CONCON
Dunbar Ivy, MDDunbar Ivy, MDThe ChildrenThe Children’’s Hospital Heart Institutes Hospital Heart Institute
2
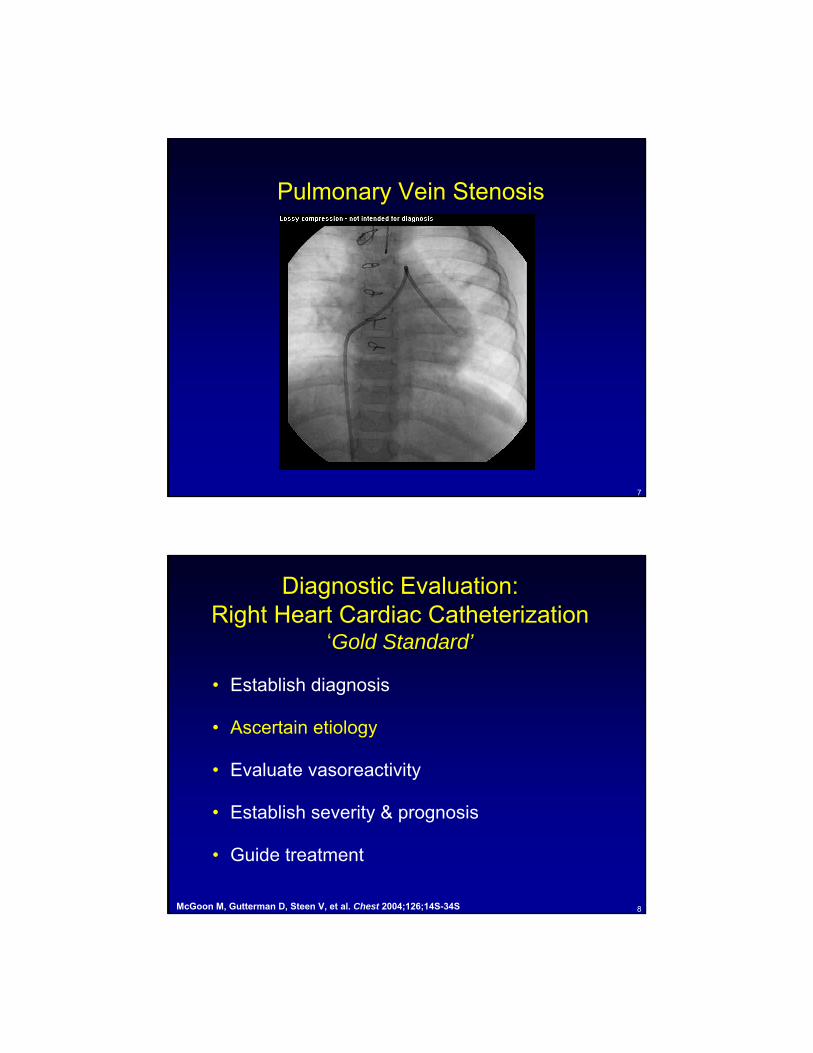
Diagnostic Evaluation:Right Heart Cardiac Catheterization
‘Gold Standard’
• Establish diagnosis
• Ascertain etiology
• Evaluate vasoreactivity
• Establish severity & prognosis
• Guide treatment
McGoon M, Gutterman D, Steen V, et al. Chest 2004;126;14S-34S

3
Pulmonary Arterial HypertensionPulmonary Arterial Hypertension
•• Sustained elevation of mean pulmonary Sustained elevation of mean pulmonary arterial pressure to > 25 mm Hg, with a arterial pressure to > 25 mm Hg, with a mean pulmonary capillary and left atrial mean pulmonary capillary and left atrial pressure < 15 mm Hg at rest pressure < 15 mm Hg at rest
–– Pulmonary Vascular resistance > 3 Units Pulmonary Vascular resistance > 3 Units X mX m22
Simonneau G, et al. J Am Coll Cardiol 2009;54:S43-S54
Echo Doppler Estimate of PA pressure

Limitations of Doppler Estimate of PA Systolic Pressure
• Requires a good acoustic window
• Requires a good and properly aligned Doppler signal
• Tricuspid regurgitation has to be present
• Can be affected by incorrect assumption of right atrial pressure
6
Pulmonary Vein Stenosis IN BPD
7
Pulmonary Vein Stenosis
8
Diagnostic Evaluation:Right Heart Cardiac Catheterization
‘Gold Standard’
• Establish diagnosis
• Ascertain etiology
• Evaluate vasoreactivity
• Establish severity & prognosis
• Guide treatment
McGoon M, Gutterman D, Steen V, et al. Chest 2004;126;14S-34S

9
What Is the Cause of Pulmonary Hypertension?
2
VCVC RARA RVRV PAPA PVPVPCPC
LALA LVLV AoAo
PostPost--Capillary PH Capillary PH (PCWP>15 (PCWP>15 mmHgmmHg; PVR ; PVR nlnl))
Systemic HTNSystemic HTNAoVAoV DiseaseDisease
Myocardial DiseaseMyocardial DiseaseDilated CMPDilated CMP--ischemic/nonischemic/non--iscisc..
HypertrophicHypertrophic CMPCMPRestrictive/infiltrative CMPRestrictive/infiltrative CMP
Obesity and othersObesity and others
AtrialAtrial MyxomaMyxomaCorCor TriatriatumTriatriatum
PV PV compression compression
PVODPVOD
PAHPAHRespiratoryRespiratory
DiseasesDiseasesPEPE
PulmonaryPulmonary Hypertension:Hypertension: TypesTypes
MV DiseaseMV Disease
↑↑LVEDPLVEDP
PrePre--capillary PH (PAH)capillary PH (PAH)PCWPPCWP<<15 15 mmHgmmHgPVR PVR >> 3 Wu3 Wu
10
BPD and PAH
Mourani, Ivy, Rosenberg, Fagan, Abman. J Peds 2008;152:291-293

11
Diagnostic Evaluation:Right Heart Cardiac Catheterization
‘Gold Standard’
• Establish diagnosis
• Ascertain etiology
• Evaluate vasoreactivity
• Establish severity & prognosis
• Guide treatment
McGoon M, Gutterman D, Steen V, et al. Chest 2004;126;14S-34S
Treatment Overview
Barst R, et al. J Am Coll Cardiol 2009;54:S78-S84

Incomplete response
Yes No
Incomplete response
Incomplete response
Incomplete response
Incomplete response
Yes
No
Calcium Channel Blocker
Conventional treatment
Acute vasodilator response
Responder Non Responder
Right heart failure
Bosentan oralSildenafil oralTadalafil oral
Iloprost inhaledTreprostinil sc
Treprostinil inhaled
Combination of drugs
IV prostanoids (Epoprostenol, Treprostinil)
Atrial septostomy
Transplantation
Tissot, Ivy, Beghetti
14
Pulmonary Vascular Pulmonary Vascular Reactivity TestingReactivity Testing
•• Acute response Acute response -- ClassicClassic-- Decrease in mPAP of at least 20% Decrease in mPAP of at least 20% -- with the PVR decreasing with the PVR decreasing 20%20%-- with no change or an increase inwith no change or an increase incardiac outputcardiac output
••Acute response Acute response --RevisedRevised-- Decrease in mPAP of at least 10 mmHg Decrease in mPAP of at least 10 mmHg -- with the mPAP decreasing with the mPAP decreasing ≤≤ 40 mmHg 40 mmHg -- with a normal or high cardiac outputwith a normal or high cardiac output

15
Diagnostic Evaluation:Right Heart Cardiac Catheterization
‘Gold Standard’
• Establish diagnosis
• Ascertain etiology
• Evaluate vasoreactivity
• Establish severity & prognosis
• Guide treatment
McGoon M, Gutterman D, Steen V, et al. Chest 2004;126;14S-34S
HemodynamicsHemodynamics——NIH RegistryNIH Registry
4
Freq
uenc
y
Right Atrial Pressure (mm Hg)
30
20
10
08 12 16 20 24 28
Normal Range
1
Freq
uenc
y
Cardiac Index (L/Min/M2)
50
30
100
40
20
2 3 4 5 6 7 8
Normal Range
20 60 80
50
Freq
uenc
y
Mean Pulmonary Artery Pressure(mm Hg)
4030
20
10
040 100 120
Normal Range
10 40 50
30
Freq
uenc
y
Pulmonary Vascular Resistance Index(L/Min/M2)
25201510
030 70 80
5
20 60 90
Normal Range
Rich S et al. Ann Intern Med. 1987;107:216-223.

Hemodynamic Predictors of Survival in Patients With PPH: A National
Prospective Registry
D’Alonzo GE, et al. Ann Intern Med. 1991;115:343-349.
Variable Odds Ratio (95% CIs)Right atrial pressure (mean) 1.99 (1.47 – 2.69)
Pulmonary arterial pressure (mean) 1.16 (1.05 – 1.28)
Cardiac index 0.62 (0.46 – 0.82)
PAH Determinants of Risk
McLaughlin VV and McGoon MD. Circulation, In press.
Determinants of RiskDeterminants of Risk Lower RiskLower Risk Higher RiskHigher Risk
Clinical evidence ofRV failure No Yes
Progression Gradual Rapid
WHO class II, III IV
6MW distance Longer (>400 m) Shorter (<300 m)
BNP Minimally elevated Very elevated
Echocardiographic findings Minimal RV dysfunction
Pericardial effusion,significant RV dysfunction
Hemodynamics Normal/near normalRAP and CI High RAP, low RAP

Sitbon O et al. J Am Coll Cardiol. 2002;40:780-788.
Predictors of Outcome on EpoprostenolVariables
Hazard Ratio (95% CI) p value
Age >44 yrs 1.17 (0.71-1.94) 0.535
Gender (female/male) 0.95 (0.53-1.71) 0.877
Anorexigenic (yes/no) 0.95 (0.55-1.65) 0.853
Raynaud’s phenomenon(presence/absence) 1.38 (0.72-2.65) 0.334
History of syncope (yes/no) 0.75 (0.44-1.25) 0.226
History of right-sided heart failure (yes/no) 2.19 (1.31-3.64) 0.003
NYHA FC IV vs III 2.24 (1.34-3.73) 0.002
Six-minute walk distance ≤250 m 2.20 (1.31-3.69) 0.003
Baseline hemodynamicsmRAP ≥12 mm HgmPAP <65 mm HgPAOP ≥10 mm HgCI ≤1.80 L/min/m2
TPR ≥35.4 U/m2
mSAP ≤93 mm HgHeart rate ≤88 beats/minSystolic index ≤21.4 mL/m2
Svo2 ≤54.5%
2.74 (1.58-4.75)1.72 (1.04-2.86)0.87 (0.51-1.50)0.96 (0.58-1.59)0.65 (0.39-1.09)1.24 (0.71-2.18)0.76 (0.43-1.34)1.46 (0.83-2.58)1.54 (0.93-2.56)
0.00030.0360.6230.8790.1020.4490.3490.1730.096
VariablesHazard Ratio
(95% CI) p value
NYHA FC III/IV vs I/II 8.75 (4.58-16.7) <0.0001
Six-minute walk distance <380 m 2.62 (1.45-4.74) 0.001
Increaase in distance walked <112 m from baseline 1.09 (0.61-1.96) 0.759
Dose of epoprostenol achieved <14 ng/kg/min 0.60 (0.33-1.08) 0.086
mRAP >10 mm Hg 3.57 (1.65-7.71) 0.001
mPAP <59 mm Hg 1.94 (1.06-3.55) 0.032
Decrease in mPAP ≥10% relative to baseline 1.25 (0.69-2.27) 0.462
CI ≤2.4 L/min/m2 1.45 (0.79-2.66) 0.231
Increase in CI <0.5 L/min/m2 relative to baseline
2.35 (1.23-4.52) 0.010
TPR ≥25 U/m2 1.53 (0.82-2.85) 0.185
Decrease in TPR <30% relative to baseline 1.90 (1.02-3.54) 0.041
Svo2 <62% 2.64 (1.41-4.95) 0.002
20
Diagnostic Evaluation:Right Heart Cardiac Catheterization
‘Gold Standard’
• Establish diagnosis
• Ascertain etiology
• Evaluate vasoreactivity
• Establish severity & prognosis
• Guide treatment
McGoon M, Gutterman D, Steen V, et al. Chest 2004;126;14S-34S

21
Guide Treatment:
• Epoprostenol dosing
• Timing of listing for lung transplantation
• Timing for addition or change of therapy
• Performance of atrial septostomy