Embed Size (px)
Citation preview

Capacity Building: Capacity Building: Iran Experience of Family Iran Experience of Family
PsychoeducationPsychoeducation
Yasaman Mottaghipour, Ph.D




Iran’s Mental Health Iran’s Mental Health • Catchment area• Community Services• General hospital• Psychiatric hospital• Centers for chronic patients/rehab centers• Beds : 7000 based on Mental Health Atlas
2011• Beds: 4350 residential facilities• 400,000 severe mental disorder
LiteratureLiterature
• Significant research and guidelines available
• Family intervention programs for families of patients have not been incorporated into routine mental health services
• The gap is greater in developing countries with different cultural values and scarcity of available resources

LiteratureLiterature• In Iran, limited services for psychiatric patients
and their families in the community• The main burden of care lies on families of
patients• Developing a program and selecting
appropriate and feasible services for families of patients becomes a necessity
• No specialized services for patients with first-episode psychosis and their families in Iran

OverviewOverview
• Research Studies• Training & Supervision• Resources • Capacity Building• Our Challenges

Carer’s Experience and Psychological Well-Being of Families of Patients with Severe Mental Disorder in Iran: Family
Education Program Y Mottaghipour, J Shams, N Beyraghi,
M Samimi, F Khodaeifar
Shahid Beheshti University of Medical Science Tehran, Iran

Family Education in Two CentersFamily Education in Two Centers
• 1157 Families of patients• 1745 Family members• One hundred and thirty three, 2-hour
sessions• Two clinicians discussed the content• Lecture and questions and answers

MethodMethod
• Questionnaires: – Experience of Caregiving Inventory (ECI) – General Health Questionnaire (GHQ-28)
• 266 family members
• 206 family members filled the questionnaires

DemographicsDemographics
• Family members:– 32.8% mothers– 42.9% family members of patients with first episode
of psychosis
• Patients:– 172 patients (61% male, 39% female)
– 77% of patients with three main diagnoses (schizophrenia, bipolar, schizoaffective)

ResultsResults• 45.5% of family members had GHQ score of six or
more (psychiatric morbidity)
• Distressed family members scored significantly higher on ECI total negative score (P<0.00)
• Significant difference between negative experiences of families of patients with first episode of psychosis compared to families of patients with a history of psychiatric hospitalization (P<002)

ResultsResults
ECINumber of subscales /
items
Tehran
(Mean /SD)
England*
(Mean /SD)
Italy*
(Mean /SD)
Total negative
scales8 subscales52 items
122.81 + 29.78 59.06 + 32.60 75.27 + 36.49
Total positive scales
2 subscales14 items 32.99 + 9.06 26.41 + 9.71 23.83 + 10.88
* Tarricone I. et al. (2005) European Psychiatry

Randomized Clinical Trial of Family Education in Iran: Families of Patients
with First-Episode Psychosis
Y Mottaghipour, V Sharifi, Z Shahrivar, J Mahmoudi-Gharaei, J Alaghband-Rad,
M Jalali Roudsari, N Salesian, A Seddigh

ObjectivesObjectives
• To evaluate two different models of family education in order to choose an effective, feasible and culturally accepted program
• Assessment of Carer’s experience and Psychological well- being

MethodMethod
• 50 families of first-episode psychosis patients • Randomly assigned to two different groups• Home based family education or multiple
family groups at the hospital• Both models of family education consisted of
four sessions• Two health professionals conducted the
family education sessions

MethodMethod
• Outcome measures:– Experience of Caregiving Inventory (ECI) – General Health Questionnaire (GHQ-28)
• Both measures were administered before the family education program, after 6 months and one year
Results : (Demographic Data)Results : (Demographic Data)• 62 family members participated• 30.6% mothers• Age:– Mean 39.6 years old + 15.3
• Education:– 19.7% illiterate – 57.4% 9 years and less

ResultsResults
• 34 Home based /28 Multiple family group
• Participation rate of family members 66.1% (3 sessions and more)
• Each family participation rate 77.1% (3 sessions and more)
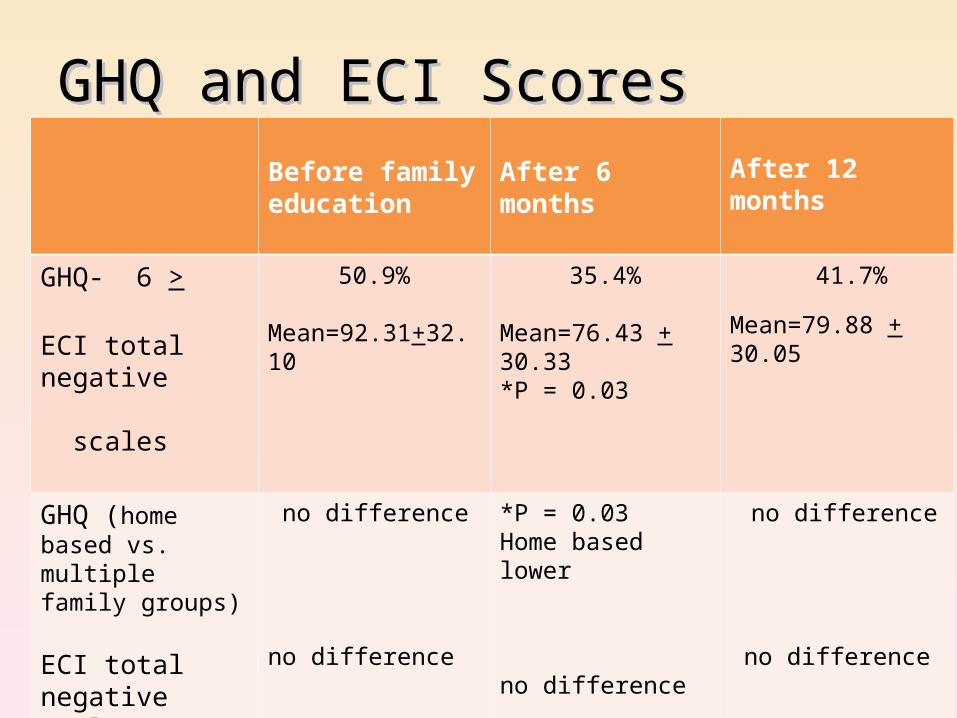
GHQ and ECI ScoresGHQ and ECI ScoresBefore family education
After 6 months After 12 months
GHQ- 6 >
ECI total negative scales
50.9%
Mean=92.31+32.10
35.4%
Mean=76.43 + 30.33*P = 0.03
41.7%
Mean=79.88 + 30.05
GHQ (home based vs. multiple family groups)
ECI total negative scales (home based vs. multiple family groups)
no difference
no difference
*P = 0.03Home based lower
no difference
no difference
no difference

ConclusionConclusion
• Psychological morbidity (GHQ) 12% to 74%• Poor psychological well being with poor rating
on ECI• Home based treatment: regular contact with
families• 6 months lower rate, not stable• Acceptability of family intervention program• Limitations

Main PointsMain Points• Both models were acceptable• Short–term family education part of a
comprehensive treatment program• Patients live with the families, this has an
effect on families as well as the intervention program
• Low level of education an important factor• Contrary to previous assumptions families
accepted participation

Training Health Professionals to Conduct Family Education for Families
of Patients with First-Episode Psychosis: Adherence to Protocol
Y Mottaghipour, N Salesian, A Seddigh, M Jalali Roudsari, S Tahbaz Hosseinzade

LiteratureLiterature
• Implementation difficulties
• Lack of training • Limited resources

Method/TrainingMethod/Training
• 3-day workshop• Supervision:– 12 supervision sessions– 2-hour group supervision– Content :• Audiotapes of family education analyzed• Topics related• Areas of concern

Method /SubjectsMethod /Subjects
• Eight health professionals :– General practitioner (4)– Nurse (2)– Social worker (4)

Method/AnalysisMethod/Analysis
• Transcripts of sessions • Content analysis based on protocol
• Duration of each session
• Number of questions asked

ResultsResults• 44 recorded sessions• 24 analyzed• 72% adherence to protocol• Multiple family group sessions vs. home
based:– 79% vs. 69%– Time: 60 min vs. 30 min– Q : 6 to 2

ConclusionConclusion
• Level of adherence satisfactory
• Difference between the two due to:– Cultural issues– Time limitation– Presence of the patient– More specific content at home

Main PointsMain Points
• The missing parts: “introduction” and “conclusion”
• Patients present at home
• Quality of conducting the sessions did not change over time

Burden of Families of Patients with Severe mental Disorder in Iran:
a One-Year Follow-Up
Y Mottaghipour, V Sharifi, H Amini,A Hajebi

Demographics Demographics
• 118 family members• 55.1% mothers and sisters• 32.2% no literacy or minimum• 49 (41.5%) hospital base/multiple family
group• 69 (58.5%) home based/home visit sessions• 56.8% four sessions and more

Results: Baseline and 12 monthsResults: Baseline and 12 months
• GHQ significant decrease• Total burden significant decrease• Four subscales significant decrease

After Care Services After Care Services
• Expert group program for after care services:– Treatment follow-up • Home care/Telephone follow-up
– Family psychoeducation– Patient social skills training

Other ResearchOther Research
• Professionals vs. family members case management
• Effect on EE• Multi–center home visit• Family psychoeducation (schizophrenia,
bipolar disorder, borderline personality disorder)
• Patient education

Summary of DemographicsSummary of Demographics• Family members:–30% to 40% mothers–More than 55% female– Literacy (30% no or minimum
literacy, to about 50% nine years and less)– Living with family–42.9% family members of patients
with first episode of psychosis

TrainingTraining
• One day workshop:– Thirteen workshops for residents (274 participants)
• Two-day workshop– Five workshops for after care and day center teams (68
participants)
• Three-day workshop– Two workshops for research teams (10 participants)

Supervision Questions Supervision Questions • Language of sessions• Language of information sheets• How much involvement?• Recording of sessions• Patient presence at home• Acceptance of recovery for team members • Family’s other problems

ResourcesResources
• Information sheets• Manuals– Patient education (schizophrenia)– Patient education (bipolar disorder)– Family psychoeducation
• FAQ families• Transcript of sessions

Sustainable Psychoeducation Program:Sustainable Psychoeducation Program:Capacity BuildingCapacity Building
• Leadership• Organizational structures• Workforce development• Strategic resource development• Partnerships: Working with Non-
Government Organizations

Summary of Major PointsSummary of Major Points• Language• Literacy• Female participants• Setting• Supervision• Content of education• Common language/shared language

Our Challenges with Families
FAQFAQ• Dependence on medication• Substance abuse• Nutrition/food and illness• Blaming another person• Family and friends• How to handle patient’s demands• Questions on medication• Questions on diagnosis• Questions on prognosis

Main IssuesMain Issues
• Marriage• Recovery• Stigma • Society attitude re: medication• Doctor shoppers• Dependence/Independence































