Embed Size (px)
Citation preview

278 Choosing to Live
Literature and Medicine 28, no. 2 (Fall 2009) 278–332© 2010 by the Johns hopkins University Press
Choosing to Live: Cancer Education, Movies, and the Conversion Narrative in America, 1921–1960David Cantor
When, in 1921, the American society for the Control of Cancer (ASCC) released its first cancer education movie, it chose a form that would dominate cancer education movies until the 1950s: the conver-sion narrative. In general, the narratives issuing from this choice dra-matized the ways in which people were persuaded to accept ASCC/ACs1 advice regarding cancer and the penalties for those who failed to convert. Crudely put, those who converted to the ASCC/ACS’s vi-sion of cancer survived their diseases; those who did not tended to die. The former chose to live, as the title of one 1940 film put it; the latter chose a different ending.2
Conversion narratives dominated the ASCC/ACS’s cinematic output from the 1920s to the late 1940s, and in two senses of the term. The vast majority of its films included a conversion story, and conversion provided the central narrative structure of those movies in which it appeared. This hegemony, however, did not survive the 1940s. Both forms of domination came to be challenged late in that decade, as television began to change the context in which these films were viewed, and as the cancer organization began to increase the number of educational films it produced and to broaden the range of subjects covered by its movies beyond its earlier focus on persuading people to seek early detection and treatment. Part of the aim of this paper is to explain the changing role of the conversion narrative within the ASCC/ACS’s cinematic output.
A second aim of this article is to explore the role of movies, and the conversion narratives embedded in them, as tools for managing public responses to cancer. Movies were of particular interest to the

279David Cantor
ASCC/ACS because the organization argued that visual media had a unique power to shape public attitudes and beliefs, a power, as this essay will show, that textual and aural media were said to lack. To the ASCC/ACS, this power made film an unrivalled technology for persuading people to seek early detection and treatment, but it also made the organization quite cautious about movies. In its view, mo-tion pictures could have quite unanticipated consequences. Even the best educational films could create in the public an excessive fear of the disease or its treatments that might undermine public education efforts by dissuading people from going to the doctor. The problem was particularly acute in the case of cancer, for the ASCC/ACS believed that the disease itself inspired a particular phobia—cancerophobia—that froze people into inaction and so damaged the organization’s efforts to promote programs of early detection and treatment. Putting cancer and movies together was thus fraught with difficulty. While movies had the potential to calm the fears that prompted people to delay seeking approved medical help, they also had the potential to exacerbate these fears and to thereby weaken the educational goals they were supposed to promote. It was quite unclear to the ASCC/ACS which way a particular film would work.3
the conversion narrative emerged as one method of managing this problem, but, as I shall argue, a highly problematic one. The ASCC/ACS’s hope was that, by offering a reassuring salvation story about the curability of cancer, the conversion narrative would help to calm the fears generated by the movie, the disease, or the combination of both, and so remove a barrier to people’s willingness to go to their physicians. The problem, however, was that the conversion narrative’s ability to calm these fears often seemed quite limited. The ASCC/ACS worried that its effectiveness as a tool of management was constantly threatened by the very problems the narrative was intended to control. The organization thus found itself constantly struggling to ensure that the conversion narrative did its work: persuading people to seek early detection and treatment. The conversion narrative’s power was con-tingent, and a final aim of this paper is to highlight this contingency and to show how the ASCC/ACS sought to ensure that this one form of narrative served the purpose it intended.
Education and the Movie4
The ASCC/ACS was interested in movies, and the conversion narratives embedded in them, as part of a broader program aimed

280 Choosing to Live
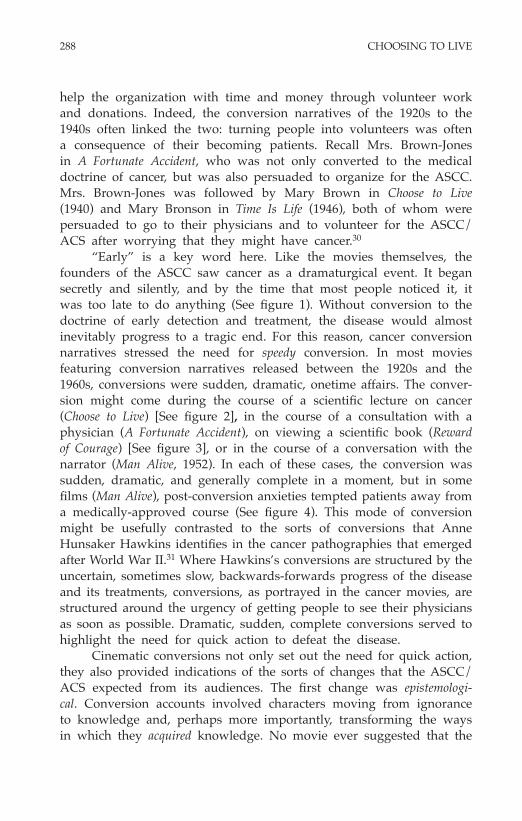
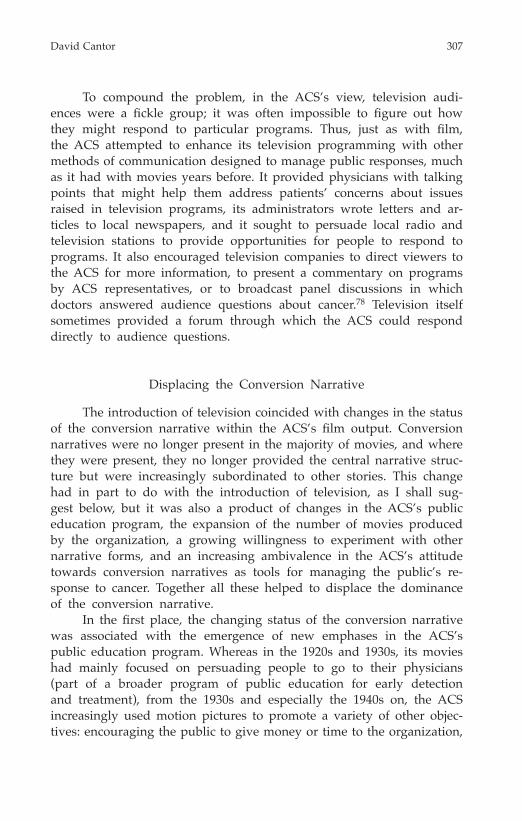
at reforming public attitudes and behaviors toward cancer. From its creation in 1913, the Society argued that for cancer control to suc-ceed, Americans had to be persuaded to abandon past practices and to seek qualified medical assistance at the first sign of what might be cancer, and from the late 1910s, it worked to persuade Americans to go for regular medical checkups, even if they felt well.5 in its view, treatment was most likely to work either before the tumor arose, if a “precancerous” condition could be identified, or in the early stages of the disease itself, while the tumor was still a local, circumscribed entity, before it spread to other parts of the body and the possibility of successful treatment began to fade (See figure 1). this meant that patients had to see competent physicians, ideally, before the onset of the disease proper or very early in its development and to undergo treatment the moment the disease or its possibility was identified. To this end, the Society sought to persuade people to go for regular medical checkups and to train them to identify what the ASCC/ACS called the “danger signals” or “early warning signs” of the disease. As one article in its newsletter put it, “our chief hope of overcoming this enemy of the human race must lie in the fact that people everywhere will learn to recognize the danger signals of the early stages, and seek advice and treatment while there is yet time.”6
The problem, the ASCC/ACS argued, was that patients often arrived in the doctor’s office long after the best opportunities for successful treatment were gone.7 The early signs of cancer could be subtle and easily missed, and pain or debility often occurred too late in the course of the disease to prompt people to see their physicians before the disease spread and became incurable. But even if cancer was suspected, the ASCC/ACS claimed that patients still delayed. Many were frightened by the disease or its treatments (mainly surgery and radiation). Others were unduly pessimistic about the possibility of a cure or ignorant of the warning signs of the disease. Still others were swayed by the advice of quacks, purveyors of patent medicines, or friends and family, all of whom tended to dissuade people from seeking appropriate help. Even regular physicians were a problem. Too often they were ignorant of the disease and its treatment; too often they were pessimistic about the possibility of successful treatment; too often they displayed a disturbing lack of urgency when confronted with cancer. “If your doctor advises delay, see another doctor,”8 an AsCC lanternslide cautioned the public in 1919, implicitly acknowledging that the skills and knowledge of practitioners dealing with cancer could vary considerably. “If your doctor isn’t sure, see another doctor.”

281David Cantor
Figure 1. A sequence of animated frames from Reward of Courage (1921) that trace the growth and development of cancer, and how its “curability” diminishes with time. (Access this issue at http://www.press.jhu.edu/journals/literature_and_medi-cine/ to view full color graphics).
in its efforts to combat the factors that promoted delay, the ASCC/ACS sought to educate people about the early warning signs of the disease and to persuade them to seek advice and treatment while there was time. It also sought to warn the public of the dangers of quackery, of ineffective and hazardous home remedies, of the advice of friends and family, of the media, and of ignorant physicians, all of which could encourage people to delay seeking appropriate help. Yet, as its educational program took off in the 1920s and 1930s, the ASCC
1
3
5
7
2
4
6
8

282 Choosing to Live
became alarmed about suggestions that its own educational efforts were adding to the problem. Critics argued that instead of persuading people to seek early detection and treatment, the ASCC’s educational program was in fact promoting cancerophobia and, consequently, encouraging delay by frightening people into inaction.9 the organization seemed caught between a rock and a hard place. It believed that efforts to promote early detection and treatment would fail without public edu-cation. Yet it was also forced to defend itself against accusations that its own efforts at education exacerbated existing fears of the disease and dissuaded people from seeking care.10
The ASCC sometimes seemed unsure how to respond to such criticism. At times, it sought to shift the burden of responsibility for seeking care onto the patient: what one physician called the layman’s [sic] responsibility in the control of cancer.11 In this view, the ASCC’s responsibility was to get the message of early detection and treat-ment out; the public’s responsibility was to act on this message. But this division of labor was undermined by the ASCC’s admission that certain members of the public seemed particularly vulnerable to fears of cancer: “over-emotional, uncontrolled, or uninformed individuals,” who presented “an unreasoning and illogical phobia.”12 Virtually any educational program was likely to unduly alarm these people. They were overwhelmed by their fears, almost incapable of taking responsi-bility for seeking care. “[A]ction springs from the emotions,” especially fear, asserted Mary R. Lakeman, the supervisor of adult education in the Massachusetts Department of Health, writing in 1933 about cancer education in her state. However, she noted,
If stimulated to a high degree in certain ill-adjusted or hypersensi-tive individuals fear leads—not to action—but to a phobia which leaves its victim not only in a state of inaction but of inability even to face an unpleasant situation. In attempting to reach the general public we must give due consideration to those wide differences in temperament which make the sudden realization of an unwelcome fact a “knock-out blow” to a highly sensitive person, while the same fact leaves a less impressionable being untouched.13
The problem, as one physician put it, was to “seek to transmit accurate information without unduly alarming the public.”14 But sometimes the ASCC acknowledged that any information—no matter how accurate—alarmed the public and, consequently, undermined people’s willingness to seek appropriate care.

283David Cantor
Despite such admissions, the ASCC generally tended not to emphasize concerns that its educational efforts might induce cancero-phobia. instead, it responded to criticisms of the effectiveness of its educational efforts by telling optimistic stories (ironically, conversion narratives of sorts) in which better public education rids the world of ignorance and fear and persuades people to seek early detection and treatment. Such stories were sometimes backed up with evidence that showed greater public discussion of cancer, more people seeking early detection and treatment, and improved chances of survival for those who did seek early treatment. “Each such step in public education,” the AsCC noted in the 1930s,
. . . buries deeper the rapidly disappearing spectre of cancer pho-bia and serves as a guarantee that the efforts to encourage a more enlightened public attitude towards cancer control are bearing fruit. Knowledge of the success which has attended these pioneer advances should spur others to the utilization of the motion picture, the press, magazines and the stage as vehicles for expression. the period of free speech on cancer control has only just begun.15
In these discussions, there was little if any mention of those who might be harmed by such free speech. By implication, the public good that resulted from better education outweighed any harm done to those sensitive individuals who were excessively vulnerable to can-cerophobia. Instead, as the quotation above suggests, the ASCC saw the success of public education as a stimulus to adopt a variety of means of communication: newspapers, magazines, posters, circulars, pamphlets, exhibits, lantern slides, lectures, and movies. Movies thus came to cancer as part of a complex array of different methods of public education that ranged from private, face-to-face talks (as between doctor and patient) to technologies of mass communication (such as newspapers, posters, and magazines, and newer ones such as radio).16 The ASCC’s first radio broadcast was in 1921, the same year it also released its first motion picture, both part of the first national cancer week—an intense effort at fund-raising and education.17
The Work of the Movie
In turning to motion pictures, the ASCC hoped to build on a growing interest in the movie as a technology of social and personal

284 Choosing to Live
transformation. In 1910, Thomas A. Edison forecast that film would “. . . wipe out narrow-minded prejudices which are founded on ig-norance . . . create a feeling of sympathy and a desire to help the down-trodden people of the earth, and . . . give new ideals to be fol-lowed.”18 Edison’s comments must be seen in the context of efforts by filmmakers to fend off public criticism that movies and movie theaters had become recruiting stations for vice by emphasizing the educative possibilities of the medium.19 His enthusiasm for movies was widely shared. Film was often portrayed as a medium that would revolution-ize society, and from the 1910s, public health advocates and physicians added their voices to the chorus. Impressed by cinema’s hold over mass audiences, they released numerous films on the health hazards of alcoholism, water and food contamination, tuberculosis, venereal disease, and other topics.20 The ASCC’s interest in movies echoed this enthusiasm. As the organization noted of its first film, Reward of Courage (1921), “The value of this kind of visual instruction can not be over estimated.”21
The phrase “visual instruction” is notable. In the early twentieth century, “visual instruction” and “visual education” movements sought to introduce visual material—including illustrations, photographs, post-ers, exhibits, stereographs, lanternslides, and especially movies—into schools and other sites of education. Although many advocates of visual instruction feared what they perceived as the anaesthetizing and corrupt-ing effects of movies, they also saw visual technologies, appropriately used, as valuable ways of inspiring and informing students through a combination of visual pleasure and learning. More memorable and engaging than words, moving images could communicate information, vast amounts of information, more speedily and effectively than print and would help to modernize the masses to meet the challenges of a visually-oriented world.22
Many physicians jumped on the bandwagon, turning this idea to their own purposes. “We are living in an age of visualization,” de-clared the president of the newly formed society for Cinematographic Instruction in Medicine and Surgery, James Edlin, in 1922. “The oral age is giving way more and more to a period in which a vast number of things must be visualized to become mental possessions. The com-plexity of modern medicine demands the extension of our avenues of learning into the infinite possibilities of visualization.”23 Visual media, to Edlin and many other advocates of movies, had a unique power to instruct, something that the written and spoken word seemed to lack. The focus of Edlin’s article was the instruction of physicians,

285David Cantor
but as the quotation about Reward of Courage above suggests, similar sentiments were also applied to public education. In the ASCC’s view, public attitudes and behaviors concerning cancer could be transformed by enabling people to visualize the disease, its treatments, and the outcomes of both.
the Conversion narrative
If the ASCC saw movies as transforming attitudes and behaviors by means of their visual impact, it also saw film as transformative in another way: through telling stories. The cancer organization wanted its public education films to tell tales that showed the routes by which people facing the possibility of cancer got to the doctor, the obstacles that hindered them from reaching this goal, and the events that helped them take the right path as defined by the ASCC/ACS.
Its first film, Reward of Courage, illustrates the sorts of narratives that the ASCC’s films employed. A two-reel movie, the story revolves around the efforts of nefarious quack Maurice Maxwell (played as an untrustworthy dandy by an unidentified actor), who offers a worth-less treatment for cancer to Anna Flint, wife of factory owner Mar-shall Flint. Anna has recently discovered a lump on her breast, and Maxwell exploits her anxiety to persuade her to hand over $200 for his treatment. To compound his villainy, he has already tried to cap-ture the affections of Anna’s daughter, who is engaged to Marshall’s efficient factory superintendent, Eugene (Gene) Barnes, and he also tries to persuade Anna’s husband to hand over the names of work-ers who have been diagnosed with cancer in a clinic that Marshall has established in his factory. Marshall is taken in by Maxwell, but then receives a telegram which reveals Maxwell’s shady background. In a dramatic scene, Marshall races from his office to his home by automobile and bursts in on the quack, who has Anna’s $200 check in his hand. Marshall confronts Maxwell, has him arrested, and in the process, saves his wife’s life and his daughter’s happiness. The movie ends six years after the rescue scene, when Mrs. Flint has recovered from cancer after an operation, her daughter has married Gene, and they are all celebrating the birth of a new baby, Anna and Marshall’s grandchild.24 Reward of Courage set the tone for other movies. From the 1920s to the 1950s, the typical cancer movie was a melodrama in which the identification of cancer, or what may be cancer, leads to a crisis, which is typically resolved by one of the central characters

286 Choosing to Live
choosing to follow the advice of the cancer organization and to seek help from a qualified physician after facing a number of opportunities to deviate from this path.
Take, for example, a 1925 ASCC movie, A Fortunate Accident.25 in this film, Mrs. Brown-Jones, a woman of wealth and social position in an unnamed small town, is involved in an automobile collision with a coal truck outside the offices of Dr. Strong, a young, well-trained physician who has recently arrived in town with his mother, hoping to establish himself in practice, only to find that establishing a practice is not an easy thing to do. strong examines Brown-Jones and finds that she is not seriously injured, but while she is briefly unconscious, he discovers what he thinks may be an early breast cancer. Mrs. Brown-Jones is indignant, believing that this implies a hereditary taint. she dismisses strong and seeks a second opinion of the lump in her breast from an eminent surgeon. He confirms Strong’s diagnosis, recommends an immediate operation, and refers Brown-Jones to what he calls a capable physician in her hometown. this physi-cian turns out to be Dr. Strong. Mrs. Brown-Jones accepts the referral and reengages strong, who arranges for the operation that saves her life. The automobile accident is thus fortunate for Mrs. Brown-Jones, whose cancer is detected early enough to be treated successfully; for Dr. Strong, who is now able to establish himself in practice; and for the crusade against cancer, which gains an influential supporter in the person of Mrs. Brown-Jones. An ASCC synopsis of the movie concludes: “Mrs. Brown-Jones is thus converted to the modern doctrine of cancer control, and becomes a center of intelligent and useful information in regard to cancer within her large sphere of social and philanthropic influence.”26 The key word here is “converted.” As the term suggests, this movie is a conversion narrative, telling the tale of how an ignorant woman is persuaded to seek early treatment and eventually becomes a missionary for the cancer crusade. It is the story of a transition from darkness to light, from ignorance to knowledge, from tradition to modernity, from impending death to life. And it is a story of how male medical authority trumps class and women’s knowledge (in the guise of a society lady)—all through the intervention of circumstance and a knowledgeable physician.
similar conversions are evident in many other movies of the 1920s through the 1950s. In the ASCC/ACS’s view, their purpose was to reassure the public about the value of early detection and treat-ment by showing the results of following the organization’s recom-mendations. Their language echoed that of religious conversion, with

287David Cantor
individuals being “saved,” “choosing to live,” and coming to accept the “doctrine” of cancer control. But these were not religious conver-sion stories. They may have drawn on the language and structure of the religious conversion narrative, but the organization turned them into something else: medical conversion narratives. The orthodoxy they sought to promote was early detection and treatment. The devils they sought to exorcise were quackery, ignorance, fear, and a lack of deference to medical authority. The gods they sought to install were the doctor’s office, the hospital, and later, the laboratory.
the elements of Conversion
The ASCC/ACS was not the first medical organization to employ the language of conversion. As Nancy Tomes notes, evangelical con-version had long provided a way of talking about how people were persuaded of the truth of the germ theory of disease; of bolstering the emergent authority of a new experimental, laboratory-based medi-cal science; and of promoting health reform based on these ideas and methods.27 Much as religious converts were expected to change not only what they believed but also how they lived, so converts to the germ theory were expected to change not only what they thought about the body and illness, but also what they did to maintain health and to prevent and treat disease. the conversion narrative became a way for aspiring germ theory “church” members to recount the story of their own conversions, to provide model routes to conversion that others could follow, to warn about the problems they might encounter along the way, and to caution about dire consequences for those who failed to convert.28 The conversion narrative thus served double-duty: as a way of reforming the public and of elevating the status of the organizations and individuals who employed it.29
This double-duty was precisely what the ASCC/ACS hoped the conversion narrative would perform in the case of cancer. The cancer organization was a small, financially vulnerable organization when it started, founded by a small group of men (primarily surgeons and gynecologists) who worried that their message about cancer went unheard by most Americans and who hoped that their campaign against the disease would encourage public support for them and their organization. This support, they projected, would be built upon a transformation in public understanding of cancer that would encourage people both to seek timely help from a recognized physician and to
288 Choosing to Live
help the organization with time and money through volunteer work and donations. indeed, the conversion narratives of the 1920s to the 1940s often linked the two: turning people into volunteers was often a consequence of their becoming patients. Recall Mrs. Brown-Jones in A Fortunate Accident, who was not only converted to the medical doctrine of cancer, but was also persuaded to organize for the ASCC. Mrs. Brown-Jones was followed by Mary Brown in Choose to Live (1940) and Mary Bronson in Time Is Life (1946), both of whom were persuaded to go to their physicians and to volunteer for the ASCC/ACs after worrying that they might have cancer.30
“Early” is a key word here. Like the movies themselves, the founders of the ASCC saw cancer as a dramaturgical event. It began secretly and silently, and by the time that most people noticed it, it was too late to do anything (See figure 1). Without conversion to the doctrine of early detection and treatment, the disease would almost inevitably progress to a tragic end. For this reason, cancer conversion narratives stressed the need for speedy conversion. in most movies featuring conversion narratives released between the 1920s and the 1960s, conversions were sudden, dramatic, onetime affairs. The conver-sion might come during the course of a scientific lecture on cancer (Choose to Live) [See figure 2], in the course of a consultation with a physician (A Fortunate Accident), on viewing a scientific book (Reward of Courage) [See figure 3], or in the course of a conversation with the narrator (Man Alive, 1952). In each of these cases, the conversion was sudden, dramatic, and generally complete in a moment, but in some films (Man Alive), post-conversion anxieties tempted patients away from a medically-approved course (See figure 4). This mode of conversion might be usefully contrasted to the sorts of conversions that Anne Hunsaker Hawkins identifies in the cancer pathographies that emerged after World War ii.31 Where Hawkins’s conversions are structured by the uncertain, sometimes slow, backwards-forwards progress of the disease and its treatments, conversions, as portrayed in the cancer movies, are structured around the urgency of getting people to see their physicians as soon as possible. Dramatic, sudden, complete conversions served to highlight the need for quick action to defeat the disease.
Cinematic conversions not only set out the need for quick action, they also provided indications of the sorts of changes that the ASCC/ACS expected from its audiences. The first change was epistemologi-cal. Conversion accounts involved characters moving from ignorance to knowledge and, perhaps more importantly, transforming the ways in which they acquired knowledge. No movie ever suggested that the

289David Cantor
public could acquire sufficient knowledge to determine what constituted cancer. Instead, they encouraged the audience to turn to sources of knowledge sanctioned by the Cancer Society, including physicians and ASCC/ACS educational media such as pamphlets, posters, and mov-ies. At the same time, as i shall show, they set limits on the capacity of lay people to diagnose the disease and discouraged them from seeking information from alternative sources such as quacks, gossips, or purveyors of patent medicines (This Great Peril, 1929; Man Alive). Conversion stories thus aimed to establish medical and, especially from the 1940s, pathological knowledge as the arbiter of what was cancer and to channel the public to physicians and pathologists approved by the ASCC/ACS.32
the second component of cinematic conversion was behavioral. Characters were not only persuaded of the benefits of the medical model of dealing with cancer, they acted in response to the persuasion. Those who survived their cancers chose to monitor their own bodies for signs of the disease and to go to physicians for regular checkups or if they detected anything suspicious. They avoided quacks (Reward of Courage, This Great Peril, Man Alive), they heeded the advice of fam-ily and friends only when it accorded with that of the ASCC/ACS (Man Alive), and sometimes they began working for the ASCC/ACS (A Fortunate Accident, Choose to Live, Time Is Life). those who did not follow such a route tended to die (Time and Two Women, 1957; You Are the Switchman, 1946).
Figure 2. Mary Brown’s conversion moment (Choose to Live, 1940). Mary (left) is persuaded to go to her physician when she attends a lecture by a physician (right) at her women’s club. Note the posters behind the physician, which were used by the ASCC and the Public Health Service as part of cancer education campaigns in the 1940s.

290 Choosing to Live
the third component of cinematic conversion was emotional. in most movies, the identification of what might be cancer generated considerable fear, stress, and anxiety, and one of the consequences of a decision to see a physician was emotional relief. Conversion involved emotion, not only knowledge and behavior. in early cancer movies, the emotional conversion was heightened by the melodramatic tradition derived from the nineteenth-century stage; in later movies, it had more in common with the emergent tradition of the “woman’s movie.”33 But whatever the genre, the narrative trajectory moved from fear or anxiety to relief, a transition that was important to the ASCC/ACS because it regarded fear and anxiety as major causes of delay in seeking appropriate help. In one movie, relief comes at the first consultation with a doctor, before any diagnosis is confirmed (Choose to Live). But in most movies, relief comes much later, either when the doctor announces that a person does not have the disease (Man Alive; Inside Magoo, 1960; Time Is Life) or following a successful operation (Reward of Courage; You, Time, and Cancer, 1948). in most cases, this relief is dramatic, one-time, and sudden, like the epistemological and behavioral elements of conversion. However, as I shall discuss later, from the 1950s onward, a number of movies began to imagine not only a sudden conversion, but one also organized around the need to continually manage fear. In such stories, conversions might be dramatic, but they were always at risk of being undermined as patients met new challenges along what was often a difficult therapeutic pathway.
A Role for Religion?
Two other characteristics of the conversion narrative should be noted, both of which relate to the audiences that the ASCC/ACS hoped to reach. The first characteristic concerns the role of religion in these stories. The ASCC/ACS’s cinematic conversions were, as I’ve hinted before, secular conversions: they focused on saving lives rather than souls, on this world rather than the next, and organized religion had little or no role to play. the absence of organized religion is worth comment because churches were often important in getting the mes-sage of early detection and treatment to the public because cancer movies were routinely shown to church groups and because campaigns against other diseases did not necessarily exclude organized religion from their educational films. On the contrary, in other campaigns, priests and pastors sometimes became keys to conversion.34 Part of

291David Cantor
the reason the clergy did not have this role in the ASCC/ACS’s films, I suggest, had to do with the fact that the organization targeted its movies at white audiences.35
The point I make here about the “racial” composition of the in-tended audience is suggested by comparing ASCC/ACS movies with the five films Edgar G. Ulmer made for the National Tuberculosis As-sociation between 1938 and 1941. The aim of these tuberculosis films was very similar to that of the cancer movies: They urged people to learn the early warning signs of the disease, to go for regular checkups from a recognized physician, to avoid quacks, and to seek early, medically sanctioned treatment the moment the disease was identified—and often they used conversion accounts to teach these lessons. Thus, the conversions portrayed in tuberculosis movies were similar to those found in cancer movies in that they focused on secular salvation. however, they differed from cancer movies in the role they gave to religion in facilitating this form of conversion. Ulmer’s movies can be divided into two groups: one group which, like cancer movies, gave no role to religion and another group which gave to religion a significant role in promoting a medical conversion.
What divides these two groups is the “race” of the intended audience. Ulmer’s films targeted African Americans (Let My People Live, 1938), Mexican Americans (Cloud in the Sky, 1939), white children (Goodbye Mr. Germ, 1940), white adults (They Do Come Back, 1940), and native Americans (Another to Conquer, 1941). Ulmer’s movies aimed at non-white audiences tended to give a different place to organized or traditional religion than those aimed at white adults or children. For example, in Let My People Live, it is a black pastor who persuades Mary to seek help from a recognized physician when she suspects she might have tuberculosis, and in Cloud in the Sky, it is a Catholic padre who persuades Consuelo to seek medical attention after she suspects she might have the disease. in the other movie aimed at non-whites, Another to Conquer, the story is more complicated. The film progresses as a fight between traditional faith and contemporary medicine, which contemporary medicine eventually wins, and is incorporated into a Native American vision of “Indians” as fighters against disease. The key figure here is Slow-Talker, grandfather to Nema and Don, whose parents have died from TB. Slow-Talker is converted to white, scientific ways of seeing tuberculosis when a physician persuades him that his own TB is the cause of Nema and Don’s parents’ deaths. Slow-Talker, a respected figure in the tribe, becomes a convert to science and isolates himself in a sanatorium, providing an example to his people.

292 Choosing to Live
By contrast, in Ulmer’s movies aimed at white adults and chil-dren, organized religion plays little or no part, nor is there much reference to traditional cultures. The proselytizer is not a pastor, padre, or someone like slow-talker, who represents traditional beliefs. instead, he is a scientist or physician. Thus, in Goodbye, Mr. Germ, a scientist seeks to persuade his children of modern scientific understandings of TB by telling them a story about an invention that allows “Tee Bee the germ” to talk with him about tuberculosis and efforts to combat it. in They Do Come Back, Roy Adams and Julie Clarke are converted by physicians and medical educators to the National Tuberculosis Association’s way of seeing TB after both contract the disease.36 Roy is the first to be diagnosed and is sent to a sanatorium for bed rest, as is Julie after being diagnosed with early tuberculosis, though she avoids the pneumothorax that Roy undergoes when bed rest alone does not work for his advanced case of the disease. Roy’s and Julie’s conversions come during their treatment in the sanatorium, where they begin to plan a new future for themselves based on scientific principles that promote rehabilitation and prevent recurrence.
The absence of organized religion in these movies is a puzzle. The tuberculosis campaign, like the campaign against cancer, relied on churches to get its message across to white audiences, showed its movies to church groups, and probably found receptive audi-ences inasmuch as church groups were both concerned about cancer and interested in educational movies as a moral counterweight to sensationalist commercial ones.37 Yet the movies released by the TB organization for white audiences generally did not portray a role for organized religion in the conversion of people to the medical view of the disease, just as the films released by the cancer organization for white audiences gave no role to religion. Perhaps both organizations believed that black and Hispanic audiences would more readily turn to medically sanctioned ideas if the suggestion came from a churchman, albeit a fictional one; pastors and priests were, after all, proselytizers to their communities for many organizations and causes. Perhaps they believed that white audiences would be more persuaded by scientists and physicians alone and did not need the intercession of the church. Or perhaps they feared invoking organized religion because they saw denominational divides as more important to white than to black or Hispanic audiences and feared that a proselytizer from one denomination might work against efforts to persuade members of another denomina-tion of their intent. Whatever the reason, the content of Ulmer’s films aimed at white audiences did not include representatives of churches
293David Cantor
or church groups, nor did the content of the movies produced by the cancer organization. It is not possible to say whether the ASCC/ACS would have given a greater role to the churches had it sought to make films for Hispanic, black, or Native American audiences, since it did not do this until much later than the Tuberculosis Association, after the period covered by this essay.38
Converting Women
The second characteristic of the conversion narrative that should be noted concerns the differences between conversion narratives aimed at women and those aimed at men. A growing historical scholarship has shown that the ASCC/ACS focused most of its educational efforts on women.39 Movies were no exception. The organization argued that more women died of cancer than men and consequently targeted most of its movies at women. As with the broader educational efforts of which it was a part, the ASCC/ACS provided different educational messages to women and men. Many movies, for example, urged women to abandon the false modesty that Leslie Reagan suggests was portrayed as a distinguishing mark of women’s resistance to early detection and treatment and to seek immediate care from a qualified physician. False modesty was never a reason why, in the educational movie, men failed to go to their physicians.40
Most women’s cancer movies were melodramas, which, especially from the 1930s, drew on the conventions of the commercial “woman’s film.”41 In the woman’s educational movie, the story was told from the perspective of the central female character, albeit a perspective often voiced by a male narrator who described the turbulent inner emotional world of the woman afflicted with cancer or a fear of the disease. It invited female audiences to identify with the dilemmas of the central character caught between her fears of cancer and its treat-ment, her hopes of a cure, and her obligations to her family. Like the medical melodrama, the subgenre of the woman’s film identified by Mary Ann Doane, such films tended also to include scenes in which a traumatized or disturbed female character tells her story to a sym-pathetic male doctor, scenes that sometimes generated the moment of conversion. Thus, in Choose to Live, Mary Brown gains emotional relief from telling her physician about the lump on her breast, and Mrs. Brown-Jones in A Fortunate Accident agrees to return to Dr. Strong after seeking a second opinion from another physician.

294 Choosing to Live
Cancer education movies aimed at women tended to conflate male and medical authority.42 As we have seen in A Fortunate Accident, it is the unnamed eminent male surgeon who converts Mrs. Brown-Jones to the modern doctrine of cancer control. And the theme of medical/male authority over women is reiterated in other movies. In This Great Peril, a young physician persuades his former fiancée to save her mother by encouraging the latter to abandon a quack sanitorium and to go to a recognized physician. The figure of the mother in this movie, as in Reward of Courage, represents gullibility, ignorance, tradition, and outmoded belief. In both films, it is the mother who stands in the way of progress, who endangers herself through her credulity and lack of knowledge, and who seeks to interfere with her daughter’s marriage prospects.43 By the 1940s, this older figure of the ignorant mother had disappeared from cancer education movies, but women facing the pos-sibility of cancer still tended to be characterized as uninformed, and they and their families were saved only by putting their trust in men and medicine (Choose to Live).
Time Is Life provides a good example of a women’s cancer movie.44 The film opens in the dead of night with Mary Bronson unable to sleep for fear that she might have cancer. Perhaps she doesn’t have cancer, perhaps she does, and what will happen if she does have it?—all are questions asked either in her own voice or in the voice of the male narrator, Neil O’Brien. Unable to cope and increasingly agitated, Mary resolves to do something about the disease, though she is apparently uncertain what to do. Then, one day while walking on the street, she stops in front of the local office of the Women’s Field Army of the ACS (a volunteer organization established in 1937), where a sign broadcasts the optimistic message that “Many Cancers Are Being Cured Today because they are treated in the early stages.” As she looks through the window, the narrator—perhaps the voice of Mary’s own thoughts, perhaps the voice of the audience, perhaps the voice of the ACS—urges her to “Go on in. Don’t be frightened. Don’t go away.” At first, she walks away. However, her conversion moment comes soon after, when she returns to the ACS office, tells her fears to the female ACS volunteer, and goes to her family physician, Dr. Addison. in this case, there are several proselytizers, and not all are men. But, the result is the same as in other movies aimed at women: a conflation of male and medical authority. Mary is persuaded by the female volunteer to go to her male physician.
As in many women’s educational films, the conversion in Time Is Life is not only about Mary’s decision to see her physician, but also

295David Cantor
about the relief that follows from her decision to seek help. Conver-sion is as much an emotional event as a behavioral and intellectual one. The film traces a transition from fear to relief, first in the reas-suring atmosphere of the ACS office, then in Dr. Addison’s office, and even in the operating room where surgeons perform a biopsy. In the course of Mary’s journey from street to operating table, the audience learns what cancer is not (a hereditary or contagious disease), the early warning signs of the disease, the major forms of treatment used to treat cancer (surgery, x-rays, and radium), the vast research effort against the disease, and the nature of the one-step operation. Mary agrees that if the pathologist finds cancer, the surgeons will operate immediately, without waking her up. We watch Mary as she lies un-conscious on the operating table, partially obscured by white sheets, surrounded by surgeons and nurses waiting for the pathologist’s report. While we wait to learn her fate, O’Brien tells us about how cancer is diagnosed by the pathologist, and we watch the pathologist examine her biopsy. Then the tension is resolved, and Mary’s decision to go for a consultation is vindicated: She does not have cancer. Her fear of the disease has turned out to be phantom. Mary returns to the ACS office and becomes a volunteer, helping other women overcome their fears and seek medical care among other things.
The plotline of this movie, like many women’s cancer education movies, carries the story from the female character’s perspective: it asks the viewer to empathize with her fear of cancer, its treatment, and its consequences for her family; it opens the possibility that she might transgress medically sanctioned codes of behavior; and it explores the consequences of her actions—the emotional relief that follows from her acceptance of medical advice. this story, like many other conversion narratives, allows Mary to reach the bottom of an emotional abyss before she begins to rise, post-conversion, above the valley of the shadow of suffering and death. In its focus on Mary’s decision to volunteer, Time Is Life portrays a world like the Women’s Field Army of the ACs, in which networks of women helped each other to overcome their fears of disease and channeled thousands of other women to their physicians. in this movie, cancer and cancero-phobia are defeated by a combination of women’s mutual self-help and male medical expertise.

296 Choosing to Live
Converting Men
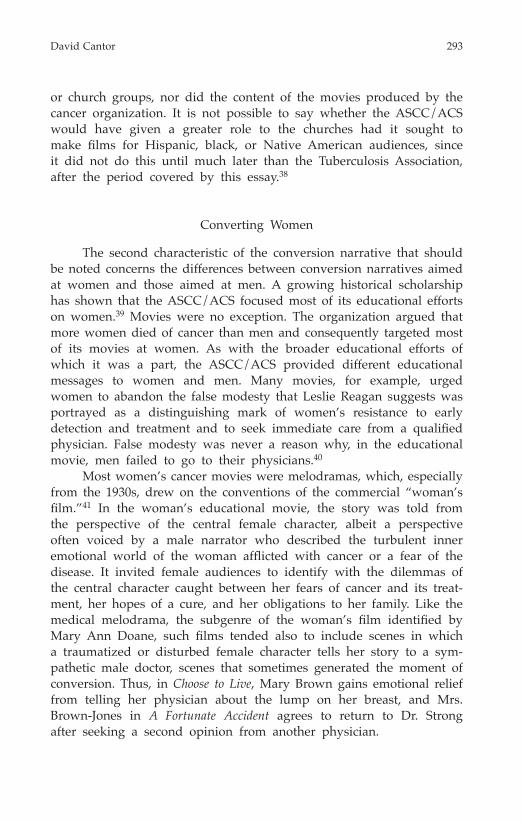
Although most movies were aimed at women, some plot elements of some films were aimed specifically at and showed the conversions of men. Indeed, in the first ASCC movie, Reward of Courage, it is Marshall Flint, husband, father, and employer, who is converted to the medical approach to cancer, and it is he who saves his wife from cancer and his daughter from marrying the quack Maurice Maxwell. Unlike the conversions of women in later films, it is not the personal threat of cancer that prompts his conversion, but the information pro-vided by Dr. Dale (the physician in the clinic Marshall has installed in his factory) [See figure 3], combined with his wife’s subsequent diagnosis of breast cancer and the revelations of Maxwell’s deception. Flint had previously been convinced of the value of the clinic when Gene Barnes, his factory superintendent, showed him statistics which demonstrated that the clinic was reducing time lost on account of sickness and ensuring that the workers in his company did not lose wages. To the ASCC, businessmen like Flint were converted by hopes of profit and industrial efficiency, by the authority of science, by the danger that cancer posed to their families, and by the prospect of being taken in by fraud.
Like most movies of the 1920s and 1930s, Reward of Courage was a melodrama, but it drew on a tradition different from that of the woman’s film discussed above. Its roots lay in earlier theatrical and movie melodramas that played on the audience’s familiarity with stock (medical) heroes and villains (quacks) and stock themes, including the vulnerable endangered, thwarted love, the race to the rescue, and the ultimate triumph of good over evil. The film’s narrative worked to heighten the audience’s sense of agitation from observing the callous, money-grabbing quack exploit a vulnerable woman, and it sought to create further tension with Marshall’s (largely off-screen) race to res-cue his wife from Maxwell. With its echoes of earlier melodramatic traditions that focused on action, incident, and jeopardy, this movie sought to associate medical conversion with the relief that came with Maxwell’s demise and Anna’s rescue.45
But Reward of Courage was an exception. it was the only movie in the 1920s and 1930s that portrayed the conversion of men to the idea of early detection and treatment. All other movies during this period portrayed the conversion of women; men remained cinematographically unconverted until the 1940s, when a small number of movies began to portray male conversion. Some of the later male conversions, such

297David Cantor
as those in You Are the Switchman and You, Time, and Cancer, were embedded in dramas and melodramas that drew on very different dramatic and melodramatic traditions than did Reward of Courage. there was none of the accident, incident, and jeopardy of the 1921 movie, nor were later films focused on the personal fears of cancer or its treatment, as was common in earlier women’s movies. Instead, the male melodramas of the 1940s focused on the threat that cancer posed to the man’s family. Viewed through a sentimental lens, they emphasized his responsibility as a bread-winner and the tragedy of widowed wives and fatherless children.
If the ASCC/ACS continued to target melodramas at men, it was also increasingly ambivalent about the use of this genre for this audience. Given its association with the women’s film, it was not clear to the Society that the conversion narrative would work for men if it was embedded in this genre. so the organization began to search for alternatives. one alternative was to incorporate the conversion narra-tive into a detective/mystery genre. Thus, Enemy X (1942) concerns the mystery of an unknown assailant who is murdering people in New York City (and marking each victim with an X on the forehead) and the efforts of the police and a rich piano-playing sleuth named Keith Prescott, played by William harrigan, to track down the killer. the
Figure 3. Marshall Flint’s conversion (Reward of Courage, 1921). Dr. Dale (right) shows Marshall Flint (left) and Gene Barnes (center) a book describing the nature of cancer, which constitutes one of a series of conversion moments for Marshall. The animated sequence in Figure 1 follows this scene. Note the reverse text next to the sprockets: this image was taken from an original nitrate print.

298 Choosing to Live
police inform Prescott that the mysterious killer is cancer, but then audience members are surprised to learn that the detective story itself is a film (also called Enemy X) within the film they are watching. A voice calls “cut,” and the actors (all men) take a break, step out of role, and chat with the movie’s medical advisor, Dr. Crandall. It is the film within the film and the conversation with the consulting physician that convince the actors of the curability of cancer and of the need for regular checkups. As the actor William Harrigan, playing himself, comments to Dr. Crandall, the film within the film gave him a “jolt,” and he hopes it will do the same for the audience. Harrigan had previously played in a number of other detective/gangster films, including G-Men (1935) and Federal Bullets (1937).46
Another alternative to the melodrama was cartoon animation. Starting in the 1950s, the ACS developed a series of cartoons for male audiences (Traitor Within, 1946; Man Alive; Inside Magoo), some of which employed conversion stories (Man Alive, Inside Magoo). the organiza-tion seems to have seen cartoons, and especially humorous cartoons, as particularly effective ways of reaching men and of addressing the fears that men might have about the disease and its treatment. Indeed, in the 1950s, cartoons and humor were almost exclusively targeted at men. With the exception of some television spots, movies aimed at women did not use cartoon animation until the 1960s, nor did they use humor to dampen fears of the disease.47
The message in all of these films targeting men is much the same as the message aimed at women—early detection and treatment save lives. They encouraged men to learn the early warning signs of the disease, to go for regular checkups, and to avoid quacks, the dubious advice of friends, and home remedies.48 But there are some noticeable differences between these and the cinematic conversions aimed at women. In many of these films, the proselytizer is not a physician or scientist but a wife. As Leslie Reagan notes, urging men to listen to the health advice of their wives underlined the gendered nature of health education and the expectation that women should teach the lessons of public education and ensure public health.49 An ACs advertisement captured the tone: “A Nagging Wife May Save Your Life.”50
An example of the proselytizing wife can be seen in You Are the Switchman, the story of John Dole (father of Bob and Jane and husband to Mary), who has a sore on his lip. In fact, the film is not one story but two. In the first story, John delays seeking help for this sore, dis-missing it until it grows too big to ignore. Eventually, Mary has had enough and persuades her husband to see Dr. Benjamin. Unfortunately,
299David Cantor
John has waited too long, and this story ends with a widowed Mary, a single, working mom, looking after their children alone. in the second story, Mary is also the proselytizer. She has found an ACS leaflet on the early warning signs of cancer in a local drug store and brings it home to John, who acts immediately on the information and goes to Dr. Benjamin. (He also persuades Mary to go for a checkup.) In this story, John survives, Mary does not have to go to work, and the fam-ily stays together, the children “warm, snug, secure, and happy about the whole thing,” as the narrator puts it.51
The point about listening to wives is driven home by the car-toon Man Alive.52 In this film Ed Parmalee has a stomach pain and delays seeking medical attention out of fear that the problem might be cancer. His wife, Marion, repeatedly suggests that he go to see his physician, but he refuses to listen to her and eventually explodes in anger before repenting and agreeing to go. But Ed’s repentance and conversion have as much to do with the male narrator of the film as with Marion. This narrator—perhaps Ed’s conscience, perhaps the voice of the audience, perhaps the voice of the ACS—functions similarly to Neil O’Brien, the narrator in Time Is Life, in that he urges Ed to seek help, much as O’Brien had urged Mary Bronson to seek help. The difference in Man Alive is that ed answers back. the narrator tells ed that his anger toward his wife is unreasonable, and when Ed shame-facedly agrees, the narrator persuades him to go to the doctor. The message of the film is thus quite confused in regard to Marion: On the one hand, it suggests that Ed should have listened to his wife; on the other, it suggests that only a man-to-man talk can persuade a man to listen to his wife.
Man Alive is unique among movies of the 1950s in the attention it gives to the psychology of delay (and to the psychology of not listening to wives). The narrator divides Ed’s responses to Marion’s suggestions into four categories—denial, sarcasm, icy disdain, and un-reasoning anger—which he describes as the consequences of excessive fear of the disease. Part of the aim of this movie is to help ed, and viewers recognize these responses in themselves and thereby combat their inclination to delay by cultivating a healthy, self-controlled fear of the disease that balances fear and reassurance: As the narrator tells Ed: “It is foolish to worry day and night about cancer, but it’s just as foolish not to worry about it at all. Be on guard. Don’t let fear make a mess of your life again. But, use your good common sense.” This self-controlled fear is the key to conversion. in the 1930s, the AsCC had worried about the impact of its message on “over emotional and

300 Choosing to Live
uncontrolled” individuals; in Man Alive, the ACS sought to provide such individuals with a means of maintaining emotional equilibrium by psychologizing their fear in something of the same way fear among servicemen had been psychologized during World War II. Mary Lakeman had argued in 1933 that action sprang from fear; Man Alive suggested that it also sprang from self-knowledge and self-control.
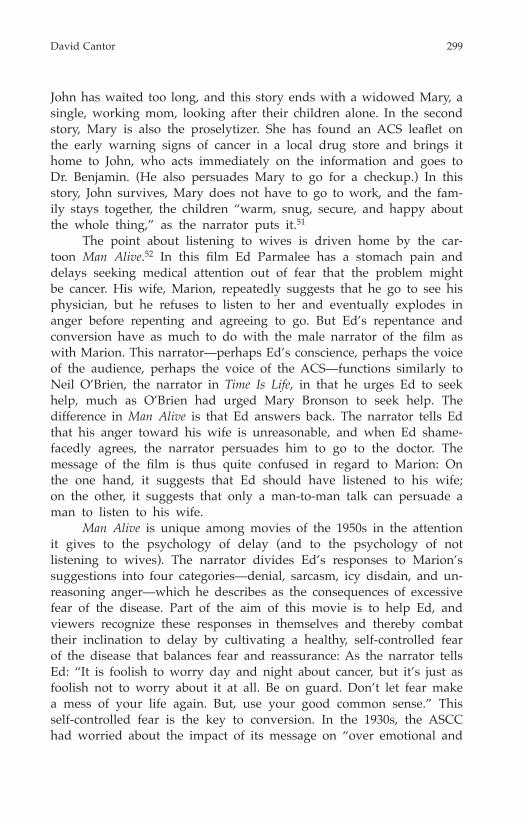
Man Alive is also notable for the importance it gave to a me-chanical analogy to the process of conversion,53 an analogy that was rarely if ever used in movies for women. In the movie, the narrator tries to persuade Ed to see a physician by drawing an analogy be-tween his body and a car engine: just as a car engine gives warning signs of impending problems, he claims, so does the body in regard to cancer. indeed, the narrator reminds ed that he had earlier ignored the warning signs that his car engine needed attention just as he is now ignoring the warning signs of what might be cancer; the risk is that he may suffer the same fate as his car. Ed had compounded his car problems by going to a dodgy car mechanic, hoping to save money, only to find that the mechanic ruined the engine and cost him more than if he had gone to a recognized car mechanic in the first place. Ed seems doomed to repeat these mistakes in the case of cancer. After agreeing to see a physician, his resolve fails [See figure 4], and he turns to a quack, who looks suspiciously like the dodgy car mechanic who had ruined his car engine.
In this movie, cancer and car trouble, quacks and dodgy car mechanics are threats to Ed’s life, his wallet, and his enjoyment of postwar, suburban consumer car culture, all beautifully evoked. These threats are only averted by Ed’s decision to see a doctor. The story ends with him and Marion enjoying a movie at a drive-in theater.
The Problems of the Movie
So far I’ve argued that the ASCC/ACS used movies both to trans-form public attitudes and behaviors concerning cancer and to transform its own status. But this alacrity introduced a problem: Movies, and the conversion accounts embedded in them, could be blunt instruments for getting the ASCC/ACS’s message across. Able to tell the same story repeatedly to audiences across the country but often unable to respond to the needs of different audiences, they were monological. Time and again they told their conversion stories, unchanged except for scratches and broken sprockets, repeating the same involved tale

301David Cantor
to whomever would watch. No small wonder, then, that the movies often had a relatively short life span. Audiences might find them persuasive the first time they watched, but they could soon tire of the show, and boredom or inattention could set in with subsequent viewings, which could weaken the films’ capacity to persuade people to see a physician. For this reason, the ASCC/ACS felt compelled to introduce new movies on a regular basis and to retire old ones, so that the senses were not dulled.54
Paradoxically, if movies could undermine the power of the con-version narrative to do its work by inducing boredom and inattention,
Figure 4. Man Alive (1952). After agreeing to go to his physician, Ed Parmalee be-gins to doubt his decision, and he physically shrinks as he becomes more fearful of what the doctor might find. Here he has shriveled to a size smaller than a white picket fence; dwarfed by the telegraph poles and tall buildings that lean over him. Man Alive was one of the first cancer education movies to highlight post-conversion anxieties. In this image Ed is on his way to see his physician, but as his fears grow, he is about to be tempted to see a quack: His route to the doctor is ap-parently blocked by the structure in front of him. Note the urban backdrop: Ed is passing into a seedy part of town where the quack has set up shop. By contrast, Ed’s regular physician has a manicured, middle-class suburban office.

302 Choosing to Live
they could also undermine it by exciting too much, or the wrong sort of, emotion. In the view of the ASCC/ACS, film had such a powerful emotional impact that it could easily intensify existing public fears about cancer and its treatments, and thereby counteract the work the ASCC/ACS intended it to do, prompting people to delay rather than to seek immediate and appropriate help. In some cases, as I’ve men-tioned, the Society sought to counteract such fears by introducing an element of reassurance into its films—the promise of a cure or the relief from fear and anxiety. But reassurance was also a problem because it could easily turn into complacency, and complacency into delay. It was quite impossible to predict which way an audience would turn, so the ASCC/ACS sometimes felt uncertain which way to proceed.
The problem was exacerbated by the visual component of the movies. The ASCC/ACS was enthusiastic about visual media as a way of transforming social attitudes and behaviors. Yet, if it saw visual images as a powerful means of educating the public to identify the possibility of cancer, it also worried that some images might have the opposite effect. In its view, some visual images were too evocative or too sensitive to show because they might distract or dissuade people from seeking help by exaggerating the cancerophobia that physicians already detected in the public. For this reason, it rarely showed the disease itself, 55 nor did it show details of therapy (surgery, radiotherapy), their post-operative consequences, or even the “danger signals” that it argued should prompt a person to go to his or her physician. Thus, if the ASCC/ACS rhapsodized about the possibility of visual instruction, it also sought to limit the role of images in its campaigns.
The point can be illustrated by the place of the “danger signal” in its poster campaigns.56 Given its enthusiasm for visual instruc-tion, one might have expected the organization to illustrate the early warning signs of cancer, so as to provide the public with visual clues that might send them to the doctor. in fact, it tended to avoid this strategy. Instead of using visual images of the early warning signs, posters tended to describe them in words.57 this is not to say that graphic images of the early warning signs were entirely absent from publicity aimed at the public. Occasionally, especially from the 1940s, images of some of the warning signs of cancer found their way into ASCC/ACS posters, pamphlets, and exhibits.58 But in general, the organization was wary of using such images, tending instead to rely on vivid phrases such as “Danger Signals,” “irregular bleeding,” or “a wart that does not heal” to conjure up mental images whose visual representation might be too disturbing.59 The ASCC/ACS seems to have believed that such phrases and the mental images they evoked

303David Cantor
were less likely to scare potential patients than visual images of the warning signs themselves.
In movies, a similar reticence about explicit images can be dis-cerned. very few of the movies from the 1920s and 1930s that have survived show the early warning signs. These signs were generally either spoken by the narrator or listed as captions or as text within the film.60 This began to change in the 1940s and 1950s, when, for example, movies began to show early surface cancers.61 nevertheless, some warning signs, such as bodily discharges, were never shown in public education films, except as animation which was sometimes used, like words, to avoid the emotional impact of live-action im-ages. Animation could show aspects of cancer and its treatment that would have been difficult to show in live action using the bodies of real patients.62
If visual images could serve to inflate fears about cancer and its treatment, they were also problematic in another way: They could encourage people to overestimate their knowledge of the disease. Thus while the ASCC/ACS argued that people should learn the early warning signs of the disease, they also worried that people might not recognize the limits of their own knowledge and engage in their own diagnoses. So they sought to set limits on lay knowledge, in film, for example, by showing visually—often by means of animation, or of cine-microphotography—what ordinary people could not see: the inside of the body as revealed by surgery or the world of the cell as revealed by the microscope. In the context of efforts to define cancer as a surgeon’s and pathologist’s disease, these visual images of the inside of the body and of the cell stressed the impossibility of iden-tifying cancer based on the visual signs that might drive a person to see a physician.63 The message was that people might be taught to identify the early warning signs of cancer, but that these clues did not necessarily signify cancer. Only a physician or pathologist could determine the diagnosis. Consequently, if the ASCC/ACS came to see movies as a means of transforming public attitudes and behaviors and if it sought to limit the sorts of visual images employed to promote that transformation, it also used visual images to impose boundaries around the public’s understanding of the disease.
Addressing the Problems
Some of the problems of managing audiences were addressed at the production stage. When the ASCC/ACS commissioned a movie,

304 Choosing to Live
it routinely negotiated with film companies about cinematic content. From the start, it agreed that public education messages should be wrapped in a dramatic narrative, which, until the 1950s, was generally a conversion narrative embedded in a melodrama or, later, in cartoon or detective stories. It also routinely sought to cut scenes that seemed to risk undermining the message of the movie. From the 1920s to the 1940s, it cut hospital, surgical, post-operative, and rehabilitation scenes, and there was no portrayal of the scars or pain that an op-eration could leave nor, as I’ve mentioned, any visual representations of the “danger signals.”64 In the organization’s view, all these could undermine efforts to encourage people to seek medical care as soon as possible. it was only in the 1940s that this began to change, when the ASCC/ACS introduced hospital and surgical scenes and shots of cancers into its movies, joined in the late 1950s by scenes depicting post-operative rehabilitation, scars, and pain.65 these changes were in part the result of pressure from critics who thought the ASCC/ACS undermined its own message by ignoring issues that people were fully aware of, from outside organizations which began to promote cancer education in areas such as rehabilitation,66 and from the organization’s increasing tendency to test its films on audiences prior to release. To its surprise, audiences sometimes responded positively to scenes which the ACS thought would turn them off.67
The conversion narrative must be seen within this context: It provided an important method by which the ASCC/ACS sought to manage viewers’ responses. The conversion narrative provided a reassuring ending to the story that calmed potential fears generated by the subject, its visual representation, or the film’s melodramatic excesses. Whether it succeeded in such an aim is unknown. Indeed, the ASCC/ACS worried that the effectiveness of conversion narratives might be undermined by the visual elements they were supposed to counteract. Nevertheless, this sense of reassurance—a balance to the fear that might be generated by a movie—seems to have been very important to the ASCC/ACS, and helped to counter criticisms that its education programs intensified cancerophobia.
But modifications at the production stage of the movie could only go so far. They did little to address the inability of individual movies to tailor their messages to different audiences. For this reason, the ASCC/ACS also sought to control the conditions under which movies were exhibited. The organization typically required an expert to be present at each screening who might present a lecture, answer questions from the audience, and address any unwanted reactions to

305David Cantor
the film.68 In addition, it hoped that the family physician would help to address any issue raised by the film: in its imagination, family physicians were trusted advisors, albeit often ignorant of the latest advances in cancer and ill-equipped to deal with patients’ anxieties about the disease and its treatment. Thus, the organization prepared “talking-points” for family physicians that addressed likely concerns that patients might raise after a screening and a blizzard of instructional leaflets, newspaper and magazine articles, and radio and, later, television reports that might accompany the show. the movie might have been monologic, unresponsive to such individual concerns, but it was part of a broad array of methods of communication that ASCC/ACS hoped would allow it to manage audience responses to its message.69
This is not to say that the efforts of the ASCC/ACS to control the conditions under which movies were exhibited replaced efforts to modify their production. On the contrary, they often went hand in hand. The point can be illustrated by the problems that the ASCC/ACS had in getting experts to attend its film shows. Too often, experts either were not available or were not very adept at public speaking, and in the 1950s, the ACS began to make movies that could be shown either without an expert or with an expert who could not communicate ef-fectively. An example of the first type of film was A Question in Time (1949), which, according to its publicity, was intended to be shown in situations where a medical expert could not be present. The film itself would answer questions that a film audience might commonly ask a medical speaker. An example of the second type of film was The Doctor Speaks His Mind (1948). Released the year before A Question in Time, this movie was designed to pave the way for a medical speaker, but its publicity claimed that it was intended to be particularly effective where the doctor was not an accomplished public speaker.70
The introduction of television in the late 1940s and 1950s chal-lenged all these efforts to manage audience responses. Whereas film screenings were public events, television was often (though by no means exclusively) viewed in the home, and the mechanisms that sought to control audience responses in the public setting were not always possible in the home. To add to these difficulties, the organi-zation increasingly felt itself losing control of visual media to other organizations. From the 1920s to the 1930s, the AsCC had been more or less the sole provider of educational movies, but it was joined in the 1940s by the United States Public Health Service.71 In the 1950s, this near monopoly was undermined by the emergence of commer-cial television and by other agencies producing educational movies,

306 Choosing to Live
including movies on cancer. In some ways the business leaders, led by Mary Lasker, who took over the ASCC in 1944 and renamed it the American Cancer society, welcomed the proliferation of organiza-tions creating educational movies. In these films, they saw evidence of the ASCC’s success in breaking the taboos around cancer that had discouraged public discussion of the subject in earlier years.72 But the films also magnified the problem of managing the public responses to the disease.
Like the movies, the organization regarded television as a new and powerful medium that could transform people’s behaviors. But it also worried that television could undermine the message of can-cer control by exacerbating fears of the disease, providing erroneous information, and dissuading people from seeking early detection and treatment. While television companies were generally responsive to ACs concerns, the society no longer had complete control over the production of visual educational messages about cancer, nor was it able to control the conditions under which they were viewed. On the production side, the ACS responded by trying to influence how individual television programs portrayed cancer and its treatment. It offered lists of ACS-approved scientific advisors to television companies, and it sought to persuade them to broadcast ACS movies73 and to cooperate with the ACS in producing a variety of cancer programs.74 Beginning about 1949, the ACS produced a series of television spots, short thirty-second to two-minute films designed to fit easily into tight television schedules. Many were designed to accompany programs such as music, weather, sports, or news shows.75 Many also served double-duty by raising funds and encouraging people to see their doctors. As the slogan in one series of spots from the 1950s put it, “Fight cancer with a check-up and a check.”
As television audiences grew, the ACS devoted increasing ef-forts to promoting its messages via the new medium, much as it had with radio in the 1920s and 1930s. In 1956, for example, the ACS reported that its divisions encouraged more that 16,000 cancer radio programs five minutes or more in length and 1,599 television programs.76 Despite such efforts, the ACS felt it was a difficult thing to persuade the television companies to show its film programs. Some were too long for television or dealt with subjects that made televi-sion programmers uneasy, and the organization also had to compete with many other “good causes.”77 the organization came to worry that television companies might stray from its message about cancer or not present it at all.
307David Cantor
To compound the problem, in the ACS’s view, television audi-ences were a fickle group; it was often impossible to figure out how they might respond to particular programs. Thus, just as with film, the ACs attempted to enhance its television programming with other methods of communication designed to manage public responses, much as it had with movies years before. it provided physicians with talking points that might help them address patients’ concerns about issues raised in television programs, its administrators wrote letters and ar-ticles to local newspapers, and it sought to persuade local radio and television stations to provide opportunities for people to respond to programs. It also encouraged television companies to direct viewers to the ACs for more information, to present a commentary on programs by ACS representatives, or to broadcast panel discussions in which doctors answered audience questions about cancer.78 television itself sometimes provided a forum through which the ACS could respond directly to audience questions.
Displacing the Conversion narrative
The introduction of television coincided with changes in the status of the conversion narrative within the ACS’s film output. Conversion narratives were no longer present in the majority of movies, and where they were present, they no longer provided the central narrative struc-ture but were increasingly subordinated to other stories. This change had in part to do with the introduction of television, as I shall sug-gest below, but it was also a product of changes in the ACS’s public education program, the expansion of the number of movies produced by the organization, a growing willingness to experiment with other narrative forms, and an increasing ambivalence in the ACS’s attitude towards conversion narratives as tools for managing the public’s re-sponse to cancer. together all these helped to displace the dominance of the conversion narrative.
In the first place, the changing status of the conversion narrative was associated with the emergence of new emphases in the ACS’s public education program. Whereas in the 1920s and 1930s, its movies had mainly focused on persuading people to go to their physicians (part of a broader program of public education for early detection and treatment), from the 1930s and especially the 1940s on, the ACs increasingly used motion pictures to promote a variety of other objec-tives: encouraging the public to give money or time to the organization,

308 Choosing to Live
promoting public support for research, educating people in techniques of self-surveillance, and training patients to manage the post-operative effects of cancer. All these films aimed to convert the public to the ACS’s vision of combating cancer, but many of them abandoned the device of dramatizing conversions that viewers might emulate.
The changing status of conversion is most clear in the research movies, the first of which were released in the late 1930s.79 none of these films employed dramatized conversions as part of the storyline. Research movies aimed either to persuade the general public to sup-port clinical, laboratory, and epidemiological research into cancer or to encourage young people to take up a career in cancer research. Yet, instead of using cinematic conversions to encourage support for re-search, these movies, predominantly newsreels or documentaries, tended instead to document the range of research being done, the questions that interested researchers, the results of their work, and what these results boded for the future in terms of better scientific understandings of cancer and better interventions against the disease.
The changing status of the conversion narrative is also evident in other cancer movies that addressed subjects other than early detection and treatment. First, it is evident in movies that aimed to encourage the public to give time or money to the ACS. Prior to the 1950s, most movies that portrayed people—normally women—volunteering time or money to the ACS represented these acts as a consequence of the women’s earlier conversion to programs of early detection and treatment. During the late 1940s and 1950s, this sort of narrative was rarely used in cancer education movies: portrayals of the conversion of people into patients were increasingly dissociated from portrayals of the conversion of people into volunteers and donors, and often films that targeted volunteers and donors abandoned the device of the con-version narrative. Some simply asked for the money or time by using a catchy phrase, such as “Fight cancer with a check-up and a check.” Others asked for money and time through the use of poster children or patients or by showing how the ACS used its money.80 other movies sought to show, practically, how volunteers might charm money and time out of others. For example, Man on the Other Side of the Desk (1957) taught volunteers the techniques that they might employ and the resources they might offer to the manager of a television or radio station to promote the ACs. Eight out of Ten (1957) traced the history of a successful fund-raising drive in Arizona. There are conversions, or attempts at conversion, in both movies, but conversion does not hold the central place in either that it had in the pre-1950s movies.81

309David Cantor
The changing status of the conversion narrative is also evident in a new form of movie in the 1950s that focused on techniques people might themselves employ to detect and recover from cancer. Conver-sions were not central to the narrative trajectory of these movies. on the detection side, the most important were movies that emerged in the late 1940s and 1950s which taught women how to examine their breasts for warning signs of cancer. Their focus was on teaching women medically-approved techniques for examining their breasts and on promoting the idea that breast examination was crucial to emotional self-management by reassuring women who might be paralyzed into inaction in the intervals between examinations that they did not have cancer. As the narrator in the 1950 Breast Self-Examination movie puts it, “Here truly is a habit for health with an immediate reward: peace of mind.” The point was echoed by Emerson Day, Chairman of the Department of Preventive Medicine at New York City’s Memorial Hospital for Cancer and Allied Diseases, in the 1958 movie Breast Self-Examination: An Urgent Message to All Women from the American Cancer Society: “For the vast majority [of women] who have not and will not find cancer, breast self-examination has brought peace of mind,” he claimed. if these movies told a story of conversion at all, they told one in which conversion was not a one-time transformation but something that had to be maintained and worked upon.82
In other movies, the focus was not on techniques for cancer detection but on techniques for recovery after an operation. The re-habilitation movie After Mastectomy (1958), for example, told the tale of the slow healing of Kay elliot after the removal of her breast and of how she came to terms with the physical and emotional issues raised by the operation. Her conversion to a more optimistic outlook occurred very slowly and is remarkable because it occurred in spite of the loss of her breast, a loss that was never mentioned in early detection and treatment movies. As in the tuberculosis movie, They Do Come Back, the moment of conversion in After Mastectomy comes after the discovery of the disease during post-operative recovery and rehabilitation.
the displacement of the conversion narrative, however, was not unique to movies that addressed new subjects. Even in those films of the 1940s and 1950s that focused on the older theme of early detection and treatment, the centrality of the dramatized conversion began to fade. In an increasing number of these motion pictures, the conversion was at best implicit: no moment of conversion is depicted, just warn-ings of what might happen if the viewer failed to seek early treatment,

310 Choosing to Live
accounts of how early detection saved an individual, and stories about the huge numbers of lives that would be saved if only people sought timely care (The Doctor Speaks His Mind; Eight out of Ten; The Other City, 1957).83 if there was a moment of conversion, it happened off screen, suggested perhaps, but it was not explicitly dramatized.
instead of conversion stories, early detection and treatment movies began to use an assortment of alternative narrative devices to get the warning message across. one alternative was to provide a series of vignettes that traced what happened to a variety of people, some of whom sought early detection and treatment and others who did not. For example, The Doctor Speaks His Mind tells the story of a family physician who has just given some bad news to an old friend and patient, Joe Todd and his wife Ellen: Joe had delayed seeking help, and he is now dying. Saddened by this fact and frustrated at his in-ability to do anything about it, the doctor begins to reminisce about other patients, some who delayed and others who sought timely medi-cal help. The former all died, including Ed Irwin, a baseball player who ignored a mole on his leg; Ann Philips, a former librarian who avoided her doctor’s appointment when she went on vacation; Mario, the owner of a gas station who ignored a persistent cough; an un-named woman who went to a quack; and the disembodied voices of former patients that tell of fear or fatalism. By contrast, those who followed the doctor’s advice lived, including Officer Kahn, a traffic cop, whose skin cancer was identified during a routine examination required by the police department; Mrs. Allen, a mother whose cancer of the cervix was identified after she went to her physician about some unusual bleeding; and Mr. William Barrett, a cigar-smoking businessman whose cancer of the mouth was identified during a routine bi-annual physical examination. None of these examples features a conversion story, except perhaps the tale of Mrs. Allen, whose sister, a volunteer for the ACs, prompts her to go see her physician after reading some ACS literature. But if this is a conversion narrative, it is little more than the suggestion of one.84
The displacement of the conversion narrative was thus not simply a consequence of new emphases in the ACS’s public education pro-grams. the organization may have chosen alternatives to the conversion narrative for its new educational ventures such as research or giving time or money, but it also chose alternative narratives for its continu-ing efforts to persuade people to seek early detection and treatment. this is not to say that it abandoned the conversion narrative. on the contrary, it continued to use such stories (You are the Switchman, Man

311David Cantor
Alive, Inside MaGoo) to persuade people to seek early detection and treatment, but mixed these with other types of stories. The result was that the ACS’s repertoire of films in the 1940s and 1950s provided an assortment of narrative forms, targeted at a variety of audiences, and that addressed a diverse range of subjects, old and new. Conversion narratives were part of the mix.
The proliferation of narrative forms in the 1940s and 1950s re-flected two contradictory attitudes towards the conversion narrative. The first was a continuing enthusiasm for these narratives as technologies of social transformation. in the view of the ACs, cinematic conversion stories had proved important means of persuading people to seek early detection and treatment for this group of diseases, and there was no reason to abandon this form of story. Equally, there was no reason not to try other narratives. Indeed, the expansion of the ACS’s income in the 1940s and 1950s, and a consequent increase in its cinematic output,85 provided the organization with an opportunity to introduce new narrative forms without abandoning the older, tried-and-tested, conversion narrative.
Paradoxically, the second reason for the proliferation of narra-tive styles reflected not enthusiasm about the conversion narrative, but growing doubts about its power to transform public attitudes and behaviors. For all its faith in the conversion narrative as a tool of management and reform, the ASCC/ACS also saw limits to its effec-tiveness. In the organization’s view, it did not seem appropriate to all subjects, and even where it had been used with some success there was always the risk that using the same type of story time and time again might dull audiences to the organization’s message. Consequently, as its cinematic output expanded in the 1940s and 1950s, it took the opportunity to experiment with new narrative forms not only out of faith in the value of new forms, but out of fear that the older conver-sion narrative might not work. The profusion of narrative forms and the displacement of the conversion narrative thus reflected two quite opposed rationales: one was a wish to build upon an effective narrative form, the conversion story; the other was a desire to find substitutes that might address the limitations of this same form.
It was in this context of ACS indecision about the value of the conversion narrative that television entered the picture, and the or-ganization seems to have been as undecided about the value of the conversion narrative to television as it was about its value to traditional motion pictures. In its view, the conversion narrative was both an effec-tive narrative that could be adapted to television and one which was

312 Choosing to Live
quite limited in its effectiveness and which needed to be replaced by other narrative forms. In part, this indecision reflected concerns about the previously mentioned fickleness of audiences: sometimes television audiences seemed to respond well to traditional conversion narratives, while at other times, they seemed indifferent. But, it also probably reflected the fact that the conditions of exhibition had changed. Instead of making movies to show in the public setting of a film show, the ACS now had to make programs to fit the television schedules, and the traditional conversion narrative did not always fit such schedules. The short spots designed to slot into a thirty second gap in the schedule, for example, were quite unable to tell the complex conversion stories that had been a staple of educational films in previous decades.86 Most did not use a conversion narrative, and where they did, it was quite different from the older conversion narrative. Compare, for example, the dramatized conversion in the mid-1950s of a cartoon ostrich in a thirty-second spot (it stopped hiding its head in the sand when the narrator suggested it was best not to do so) with the relatively complex conversions of Mrs. Brown-Jones, Mary Brown, Mary Bronson, or Ed Parmalee in twenty- or thirty-minute films.87
this is not to say that the older style of conversion narrative disappeared from the television screens.88 For example, in 1956, NBC put on The Charlatan, the story of a quack, played by George Sanders, who successfully sues a physician who condemns his treatments. The moment of conversion comes when he discovers that he has a cancer-ous growth, and his own treatment fails to cure it. Mortally afraid of the disease, Sanders’s character turns for help to the physician he had previously sued for questioning the effectiveness of his treatment. And, to avoid the temptation that he might go back to his quackish ways if the diagnosis turns out not to be cancer, he confesses his conversion to a newspaper reporter and asks her to publish it. But generally, these sorts of stories were only a small part of the vast output of television programming.
Thus, the conversion narrative lost the dominance that it had once enjoyed. The introduction of new emphases in public education, the vast expansion of movie output, the willingness to experiment with new narrative forms, changing attitudes toward movies as a tool of public reform, and the growth of television combined to weaken its hold over cinematic and other visual media. This paper has sought to trace and to explain the changing fortunes of the conversion narrative and to show how the ASCC/ACS hoped to use it to transform people’s attitudes and behaviors towards cancer. What is less clear from this

313David Cantor
paper is how people responded to these narratives. The ASCC/ACS might have adopted an increasing mix of hope and caution about the value of these narratives in persuading people to seek early detection and treatment, but the stories it deemed appropriate to this purpose were not always appropriate to people trying to make sense of their lives after the onset of cancer. The sudden, dramatic, one-time con-versions that dominated ASCC/ACS cinematic output for much of the period covered by this essay are very different from the sorts of narratives that people who lived day-by-day with the disease have come to tell of their illnesses.89 While this phenomenon is beyond the scope of this paper, it may provide a final reason for the decline of the conversion narrative in cancer films and other media representa-tions of the disease, for patient narratives have often sought to engage with the stories put out by the cancer agencies, and sometimes to question their value.
Filmography
Key to Abbreviations:
Where copies of films survive they are noted under “Copies”NLM: National Library of Medicine, Bethesda, MarylandLoC: Library of Congress, Washington D.C.ACS: American Cancer Society, Atlanta, GeorgiaNARA: National Archives and Records Administration, College Park, MarylandInternet Movie Archive: http://www.archive.org/details/moviesNFB: National Film Board of Canada, Montreal, Quebec
Cancer Films
The list of cancer films here is not a complete list of movies released during this period; it is simply a list of those that are discussed in this paper. For other cancer education films released during this period, see Cantor, “Uncertain Enthusiasm,” 57–59. An asterisk (*) refers either to movies identified since the publication of “Uncertain Enthusiasm” or to movies where further research has lead to a revision of filmographic details provided in the 2008 article.

314 Choosing to Live
1921 Reward of Courage Produced by the Eastern Film Corporation for the American
society for the Control of Cancer. Copies: NLM, Library of Congress
1925 A Fortunate Accident Produced for the American Society for the Control of Cancer.
Production company unknown.
1929 This Great Peril Produced by Visugraphic Pictures for the American Society for
the Control of Cancer. Cast: Alden Chase (Dr. Gordon Crane), Warren Cooke (Dr. Charles Crane, his father), Amy Dennis (Margaret Salter), Jane Jennings (Mrs. Salter, her mother), Harold Clarendon (“Dr. Wythe”) Joseph Bannon (His Assistant), Andrew Andruss (Dr. George Gwyn).
Copies: ACS (partial copy, first reel)
1937 Cancer: Its Cure and Prevention originally Conquering Cancer, part of the March of Time series.
(vol. 3, episode 6) January 22, 1937. Produced by Time, Inc., publisher of Time, Life, and Fortune magazines, all of which produced articles on cancer associated with this production.
Copies: ACS, NARA
1940 Choose to Live Produced by the United States Department of Agriculture
Extension Service for the United States Public Health Service and the American Society for the Control of Cancer. Director: W. Allen Luey. Medical Director: C.V. Akin. Script: Clifton R. Read. Production Manager: Ernest R. Bryan. Photographer: Carl F. Turvey. Cast includes: Thomas Parran, Clarence C. Little.
Copies: NLM, NARA
1942 Enemy X Produced by Eagle Pictures for the American Society for the
Control of Cancer and the United States Public Health Service. Writer-Director: Owen Murphy. Director of Photography: George Webber. Art Director: Oscar Yerg. Film Editor: Shirley Stone. Sound: Harold Vivian. Cast: William Harrigan (Keith Prescott), Edmond Dorsay (Rollins Darwin), Frederic Tozere (Dr. Crandall),
315David Cantor
Royal Beal (Inspector Thorndyke), Robert Allen (Tom Dudley). Also appearing: Lyman Bryson (Columbia Broadcasting System), Clarence C. Little, Marjorie B. Illig, Samuel Binkley.
Copies: NLM; NARA
1946 The Traitor Within Produced by John Sutherland Productions for the American
Cancer Society. Director: George Gordon. Story: Norm Wright. Music: Paul Smith. Art direction: Bernice Polifka. Animation: Pete Burness, Irven Spence, Elmer Swanson.
Copies: NLM
1948* The Doctor Speaks His Mind Produced by Caravel Films (New York), supervised by Film
Counselors (New York) for the American Cancer Society. Copies: ACS
1946 Time Is Life Produced by the International Film Foundation for the Ameri-
can Cancer Society. Director: Francis Thomson. Supervisor of Photography: Peter Glushanok. Camera: Albert Mozell. Film Editor: Charles R. Senf. Supervisor of Music: Gene Forrell. Unit Manager: Paul Petroff. Narration: Neil O’Brien.
Copies: ACS, Internet Movie Archive: http://www.archive.org/details/time_is_life (accessed May 6 2010).
1946 You Are the Switchman Unknown producer for the American Cancer Society. Copies: Internet Movie Archive: http://www.archive.org/details/
YouAreth1951 (accessed May 6, 2010).
1947* The Battle against Cancer Adapted from the film Kampf dem Krebs, Produced by the Swiss
society for Combating Cancer. Copies: ACS
1948 You, Time, and Cancer Produced by Byron, Inc. for the American Cancer Society Copies: ACS

316 Choosing to Live
1948 Life Saving Fingers Produced by for the Idaho Division of the American Cancer
Society, Alfred M. Popma, MD, Executive Chairman. Copies: ACS, Library of Congress
1949* A Question in Time Produced by Transfilm for the American Cancer Society.
1949 To Save These Lives Produced by Tempo Productions, New York. Made by De Luxe
Labs for the American Cancer society.
1950 From One Cell Produced by Sturgis-Grant Productions for the American Cancer
Society. Director: Warren Sturgis. Technical Director: Douglas A. Sunderland. Animation: Dwinell Grant.
1950 Challenge. Science Against Cancer Produced by National Film Board of Canada (in cooperation
with the Medical Film Institute of the Association of American Medical Colleges) for the Department of National Health and Welfare, Canada, and the National Cancer Institute of the Public Health Service, Federal Security Agency. Director: Morten Parker. Narrator: Raymond Massey. Producer: Guy Glover. Script and Text: Maurice Constant. Images: Grant McLean. Editor: Douglas Tunstell. Animation: Colin Low, Evelyn Lambart. Music: Louis Applebaum. Sound: Clarke Daprato. Production Executive Ralph Foster. Production Consultants: David Ruhe, MD; Bernard V Dryer. Scientific Consultant: V.F. Bazilauskas (for animation scenes). Special Effects Camera: Gordon Petty, Arnold Schieman.
Copies: NCI, NFB
1950 Breast Self-Examination Produced by Audio Productions Inc. (New York) for the Ameri-
can Cancer Society and the National Cancer Institute of the U.S. Public Health Service, Federal Security Agency. Director: Alexan-der Gansell. Script: Earl Peirce. Photography: Peter Glushanok. Editor: Murray Margolin. Cast: Unidentified.
Copies: ACS
1951 The Fight against Cancer theatrical version of Challenge above. Copies: NLM, NFB

317David Cantor
1951 The Outlaw Within A ten-minute version of Challenge above. Copies: NFB
1952 Man Alive Produced by UPA (United Productions of America) for the
American Cancer Society. Story: Bill Scott, William Roberts. Design: Art Heinemann, Sterling Sturtevant. Music: Benjamin Lees. Voices: Vic Perrin, Dorothy Scott, Bill Scott.
Animation: Cecil Surry, Phil Monroe, Rudy Larriva. Color: Robert McIntosh, Boris Gorelick, Michi Kataoka, Jules Engel. Production manager: Herbert Klynn. Executive producer: Stephen Bosustow. Director: William T. Hurtz. Color by Technicolor.
Copies: NLM
1953* Cancer: A Research Story. Produced by Teleprograms, New York, for the American Cancer
Society. Narrator: Charles S. Cameron. Photography: Joe Dephoure. Sound: Ed Gilman. Executive Producer: Bill Hodapp. Associate Producer: Bob Wald. Director: Larry Schwab Jr. Writer: John Latham. Production Manager: Larry Lockwood. Scene Designer: Joe Kirby. Cast: Clarence C. Little, Charles Huggins, Lewis F. Fieser, C. P. Rhoads, John Bittner.
Copies: ACS
1953 The Warning Shadow Produced by Herbert Kerkow Inc. (New York) for the American
Cancer Society and the National Cancer Institute of the U.S. Public Health Service, Federal Security Agency. Director and Photography: Julian Roffman. Script: Howard Breslin. Animation: Sturgis-Grant Productions. Musical score: Gene Forrell. Editor: stanley Cypher.
Copies: ACS
1955 The House-to-House Campaign
1955 Alexander Ten Spot Made for ARCO films by a production group in Paris. Narrator:
tom ewell.
1957 Much Ado about Something

318 Choosing to Live
1957 The Man on the Other Side of the Desk Produced by the American Cancer Society. Narrator: Dean Land-
fear, program manager of WMT radio, Cedar Rapids, Iowa. Copies: ACS
1957 Eight out of Ten Presented by the American Cancer society. Copies: ACS.
1957 The Other City Produced by the American Cancer Society. Producer-Director:
John F. Becker. Photography: Kenneth Snelson. Editor: Stefan Bodnariuk. Musical score: Charles Strouse. Script: Allan Sloane. Orchestration: Amerigo Marino. Narrator: Robert Carson. [Pro-duced in-house?]
Copies: ACS.
1957 Time and Two Women Produced by Audio Productions Inc. (New York) for the
American Cancer Society. Cast: Joe V. Meigs M.D. (Consulting Visiting Gynecologist to the Vincent Memorial Hospital at the Massachusetts General Hospital, Boston).
Copies: ACS
1957 Decision for Life Made by Cine-Pic Hawaii for the Hawaii Cancer Society. Credits:
Walter B. Quisenberry.
1958 Never Alone Produced by Camera Eye Productions, Los Angeles, for the
American Cancer society.
1958 After Mastectomy Produced by Churchill-Wexler Film Production for the American
Cancer society. Copies: ACS
1959* Breast Self-Examination: An Urgent Message to All Women from the American Cancer Society
Produced by Audio Productions Inc. (New York) for the Ameri-can Cancer Society. Narrator: Emerson Day.
Copies: ACS
319David Cantor
1960 Inside Magoo Produced by UPA for the American Cancer Society. Narrator:
Marvin Miller. Live action cast includes Jim Backus and Stephen Bosustow as themselves and Jeff Corey (the doctor) and Joi Lansing (the nurse). Live action sequences written and directed by John F. Becker.
Copies: Internet Movie Archive, ACS
Cancer Television Movies and Programs
1951 This is Serious Business ACS Connecticut Division, sponsored by the New Haven Unit:
Director: Aubrey Moore. Script: Morris Koffman. Cast: Julius Kauf-man (father), Sue Ann Young (mother) Susan Achorn (daughter), Patricia Hanlen (daughter). Shown on WHNC, New Haven.
1951 Worry and Doubt
1954 Operation Cancer Kentucky Division of ACS and WHAS-TV. A telecast on a lung cancer operation.
1956 The Charlatan Produced by Revue Productions Inc. in association with MCA
TV Ltd. Director: John Brahm. Story and teleplay: Wells Root. Producer: William Frye. Director of Photography: John MacBur-nie. Art Director: John Meehan. Editorial Supervisor: Richard G. Wray. Film Editor: Daniel A. Nathan. Set Decorator: Ralph Stylos. Sound: William Lynch. Assistant Director: Hilton Green. Music Supervisor: Stanley Wilson. Wardrobe Supervisor: Vincent Dee. Makeup: Jack Barron. Hair Stylist: Florence Bush. Cast: George Sanders, Jeff Morrow, Virginia Gregg, Bart Burns, Fredd Wayne, William Remick, Dan Riss, Jean Willes, Marianne Stewart.
Copies: ACS
1958 Just by Chance Produced by ABC in conjunction with the American Cancer
Society. Photography: George Jacobson. Music: Corelli and Ja-cobs. Special Effects: Arthur Jack. Editor: Tony Gemini. Writer, director, and producer: John F. Becker. Cast: Ruth Hussey.
Copies: ACS

320 Choosing to Live
1959 Tactic Produced by NBC in collaboration with the ACS and the Educa-
tion Television and Radio Center. A series of six programs called Tactic, in which different artists dramatized the subject of cancer in different ways through music, song (Hy Zaret), cartoons (Mr. MaGoo and Pogo), drama (Alfred Hitchcock), dance (Mata and hari), and comedy (Wally Cox).
Other Health Education Movies
1938 Let My People Live Produced by the Motion Picture Service Corporation for the
National Tuberculosis Association. Director: Edgar G. Ulmer. Camera: William Miller. Editor/sound: Nelson Minnerly. Dramatic assistants: S. E. Walker, Edward Lawson. Cast: Rex Ingram, Peggy Howard, Merritt Smith, Erostine Coles, Christine Johnson. Jackson Burnside.
Copies: NLM, Internet Movie Archive: http://www.archive.org/details/let_my_people_live_1938 (accessed January 25, 2010).
1939 Cloud in the Sky Produced for the National Tuberculosis Association. Director:
Edgar G. Ulmer. Director of Photography: J. Burgi Contner. Sound: Dean Cole. Film Editor: Marc S. Asch. Cast: Rosario de la Vega, R. C. Ortega, F.L. Tafolla, Frederick J. Mann, R. Trevino, Jr.
Copies: Internet Movie Archive: http://www.archive.org/details/cloud_in_the_sky_1939 (accessed January 25, 2010); http://www.archive.org/details/cloud_in_the_sky_1939_esp (accessed January 25, 2010).
1940 Goodbye, Mr. Germ Produced at De Frenes Studios, Philadelphia, for the National
Tuberculosis Association. Director: Edgar G. Ulmer. Animation: H.L. Roberts Jr.
Camera: Joseph Noble. Settings: Stanley Levick. Editor: Hans Mandl. Cast: James Kirkwood.
Copies: Internet Movie Archive: http://www.archive.org/details/goodbye_mr_germ_1940 (accessed February 3, 2010).

321David Cantor
1940 They Do Come Back Produced at De Frenes Studios, Philadelphia for the National
Tuberculosis Association. Director: Edgar G. Ulmer. Camera: Jo-seph Noble. Editor: Hans Mandl. Narrator: Alois Havrilla. Cast: Wilma Caspar, Edward Mulhern.
Copies: Internet Movie Archive: http://www.archive.org/details/they_do_come_back_1940 (accessed January 25, 2010). For a dif-ferent version of They Do Come Back, see http://www.archive.org/details/they_do_come_back (accessed February 3, 2010).
1941 Another to Conquer Produced by Springer Pictures for the National Tuberculosis As-
sociation and the U.S. Office of Indian Affairs. Director: Edgar G. Ulmer. Camera: Robert Cline. Sound: Clarence Townsend. Consultant: Ruth Underhill. Editor: H. E. Mandl. Cast: Howard Gorman, Sammy Day, Geraldine H. Birdsbill, Richard Hogner, W. W. Peter, M.D.
Copies: Internet Movie Archive: http://www.archive.org/details/another_to_conquer_1941 (accessed January 25, 2010).
notes
Movies listed in the Filmography above that appear in notes are referenced by title only. Films not included in the Filmograpy include dates as well as titles.
1. in 1944, the AsCC became the American Cancer society (ACs). the ab-breviation ASCC/ACS is used when the discussion crosses the 1944 divide. ASCC is used when the discussion covers topics that concern only the American Society for the Control of Cancer; ACS is used when discussion covers topics that concern only the American Cancer society.
2. Choose to Live.3. Cantor, “Uncertain Enthusiasm.”4. Parts of this section are based on Cantor, “Uncertain Enthusiasm.”5. In 1919, two ASCC lantern slides noted, “In a few more years thorough
physical examinations every year will be taken as a matter of course . . . .” and “This alone will add several happy years to the average life.” Anon., “Lantern Slides on Cancer,” [4].
6. Fisk, “A Deadly Foe Routed,” [2].7. On the history of delay, see Aronowitz, “Do Not Delay,” and Aronowitz,
Unnatural History.8. Anon., “Lantern Slides on Cancer,” [4].9. Anon., “Cancerophobia,” 10. On phobias about cancer, see Little, “How to
Educate Women to Recognize Breast Tumors,” 10, and Clarkson and Baker, “Cancer Control,” esp. 4.
10. For discussions of the effectiveness and status of cancer education in the 1930s that emerged, partly in response to concerns that cancer education exacerbated cancerophobia and delay, see Anon., “Is Cancer Education Effective?”; Salzstein,

322 Choosing to Live
“Cancer Education: A Note”; and Anon., “The Present Status of the Educational Campaign Against Cancer.”
11. Dozier, “The Layman’s Responsibility in the Control of Cancer.”12. Anon., “Intelligence and Cancer Control,” 9.13. Lakeman, “Cancer Education in Massachusetts,” 158.14. Bluestone, “The Importance of Cancer Education,” 6.15. Anon., “The Radio as a Pioneer in Cancer Education,” 10. See also O’Brien,
“The Use of Radio in Cancer Education.”16. For accounts of the range of educational methods used by the ASCC in
its National Cancer Weeks in 1921 and 1922, see Anon., “Consolidated Report of the President and Executive Committee”; and Anon., “Suggested Plans for National Cancer Week.”
17. On the first radio broadcast, see Anon., “Suggested Plans for National Cancer Week,” [3]. According to George Rosen, this might have been the first health talk ever broadcast by radio (Rosen, A History of Public Health, 375). On the role of movies in the first national cancer week, see Cantor, “Uncertain Enthusiasm,” 42–44.
18. Edison quoted in Anon., “The Moving Picture and the National Char-acter,” 317.
19. grieveson, Policing Cinema, chapter 3; and Bowser, The Transformation of Cinema, chapter 3.
20. Nichtenhauser, “A History of Motion Pictures in Medicine,” 106–09. See also Pernick, “Thomas Edison’s Tuberculosis Films”; Pernick, The Black Stork; Lederer and Rogers, “Media”; Cartwright, Screening the Body; and Reagan, Tomes, and treichler, Medicine’s Moving Pictures.
21. Anon., “The Rockefeller Gift” [3].22. On the history of visual education, see Wiatr, “Seeing American” and
Wiatr, “Between Word, Image, and the Machine.”23. Edlin, “Cinematography: Its Uses in Teaching Medicine and Surgery,”
191; Anon., “Society for Cinematographic Instruction in Medicine and Surgery”; and Anon., “Cinematographic Instruction.” See also Edlin, Letter to Simon Flexner.
24. For a description of this movie, see Cantor, “Uncertain Enthusiasm,” 43–44.
25. It has not been possible to trace a copy of this movie, but an ASCC synopsis survives which sets out the sorts of narrative strategies the Society adopted in its movies: Anon., “‘A Fortunate Accident,’ the New Cancer Film.” This section of the essay is derived from Cantor, “Uncertain Enthusiasm.”
26. Anon., “‘A Fortunate Accident,’ the New Cancer Film.”27. tomes, Gospel of Germs, 27–28, 114, and 124. 28. The practice of recounting one’s own conversion narrative was hardly
new. The term “conversion narrative” is often associated with a particular form of autobiographical expression that emerged in the mid-seventeenth century on both sides of the Atlantic. People wishing to join a Puritan church had to appear before its members to recount the story of their religious conversion and provide compelling oral evidence that their souls were saved. On the Puritan conversion narrative, see Caldwell, The Puritan Conversion Narrative; Cohen, God’s Caress; and Dorsey, Sacred Estrangement.
29. historians of stage and screen have also highlighted how conversion narratives have served similar instrumental purposes for theater owners and filmmakers. Thus, in the mid-nineteenth century, theater owners used conversion stories to transform the cultural status of the theater by promoting the educational aspects of theatrical productions and by appealing to women and family audiences as signifiers of respectability. Similarly, from 1908, a cycle of filmed temperance dramas appeared as an important part of the commercial film industry’s attempt to reposition itself through appeals to gendered conceptions of respectability by

323David Cantor
emphasizing the educative function of the cinema. What this meant in effect was the emergence of a variety of social problem films—uplift films, as they were described—that sought to reform a variety of deviant forms of masculinity, espe-cially drunkenness (McConachie, Melodramatic Formations, 163–179, and grieveson, Policing Cinema, 103–114). For later uses of conversion narrative in film, see May, The Big Tomorrow, chapter 4.
30. There is an extensive, if somewhat inaccurate description, of this film in gardner, Early Detection, 134–137.
31. hawkins, Reconstructing Illness, 40.32. On pathological knowledge, see Cantor, “Uncertain Enthusiasm,” 52–3.33. Doane, The Desire to Desire.34. For examples of church support of the cancer organization, see Anon.,
“Utah”; Anon., “Letter Prepared for Federation of Churches, Ministers and General Circulation in Massachusetts CANCER WEEK”; and Anon., “The Church Letter.”
35. This is not to say that the cancer movies were not seen by non-white audiences or that they did not include some non-white cast members. Most likely these films were shown to non-white audiences, and a very small number of movies included non-whites in the cast. One example was Challenge: Science Against Cancer, a Canadian movie made for the US National Cancer Institute in 1950, which in-cluded a South Asian pathologist and a “negro” medical student in the cast. This was primarily a recruitment movie for young scientists rather than one aimed at promoting early detection and treatment, and the inclusion of these characters may have had as much to do with casting policy of the Canadian filmmakers as with the desire of the sponsoring bodies to attract these groups to science.
36. Lisa Cartwright suggests that Roy catches the disease from an asymptomatic Julie. In fact, the film does not mention the possibility of asymptomatic tuberculosis and is ambiguous on the direction of transmission. Indeed, the movie can be read to suggest that Julie caught TB from Roy: Roy’s tuberculosis is an advanced case when it is diagnosed. Julie’s tuberculosis is discovered after his; she has early tu-berculosis, and her treatment is less severe than his (Screening the Body, 150).
37. Parker, Purifying America, 213.38. Keith Wailoo’s current research suggests that the ASCC/ACS did not
target non-whites until much later than the tuberculosis organization. The National Tuberculosis Association began to target non-white audiences in the 1930s and to encourage churches to continue their earlier work of educating the public about this disease, not least through Ulmer’s films (Shryock, National Tuberculosis Association, 232–6). See also Roberts, Infectious Fear.
39. Reagan, “Engendering the Dread Disease.” See also, Gardner, Early Detec-tion; Aronowitz, Unnatural History; and Lerner, The Breast Cancer Wars.
40. Reagan, “Engendering the Dread Disease,”1781.41. On melodrama in film, see Gledhill, “The Melodramatic Field”; and Neale
Genre and Hollywood.42. This paragraph is derived from Cantor, “Uncertain Enthusiasm,” 47.43. For another example of maternal culpability in public health movies, see
Cartwright’s discussion of the anti-tuberculosis movie Let My People Live (1938) in Screening the Body, 149–50.
44. For another example, see the discussion of Choose to Live in Cantor, “Uncertain Enthusiasm,” 51–54.
45. On the relations between stage and screen melodrama, see Vardac, Stage to Screen; Fell, Film and the Narrative Tradition; and Singer Melodrama and Modernity.
46. William Harrigan (1894–1966), the son of playwright/actor Edward Har-rigan, was one-half of the Harrigan and Hart musical comedy team. Harrigan made his film debut in 1917, starring as the duplicitous Dr. Kemp in The Invisible Man (1933); as a retired gangster “Mac” McKay, aka Joseph Lynch, in G-Men (1935); and as the Federal Agency Chief in Federal Bullets (1937).

324 Choosing to Live
47. Another exception is To Save These Lives, a movie that aimed to recruit members of the public to volunteer for the ACS (Anon., “Animated Film to Launch Drive for Recruits”; and Anon., “Recruiting Movie”). For the use of humor in cancer education aimed at men, see Reagan, “Engendering the Dread Disease,” 1784.
48. Thus, You, Time, and Cancer told the tale of a young husband who experi-ences symptoms of persistent indigestion. After trying self-cures without effect, he undergoes surgery and realizes the need for extensive cancer research and more cancer funds (Anon., “New Cancer Film Prepared for Campaign Use”; Anon., “New Film Ready for Use in Drive”; Anon., “Murphy Seeks Check on Film”; Anon., “ACS Drive Film Clicks in Capital”; Anon., “Milwaukee”; and Dewey, “Recent Additions to the Film Library,” 561).
49. Reagan, “Projecting Breast Cancer,” 184. Reagan implies that the BSE program of 1950 made the ACS realize that its educational programs had neglected men. in fact, as Enemy X and You Are the Switchman indicate, educational efforts to target men had started in the 1940s.
50. “A Nagging Wife May Save your Life.” This advertisement was part of a campaign against lung cancer that urged men to see the movie The Warning Shadow.
51. For another example, see Decision for Life, in which a father who has a warning sign of cancer is persuaded by his wife to attend a PTA lecture on cancer and decides to see a physician. Cancer is detected, and an immediate operation saves his life (Cancer Control Program and the National Library of Medicine; Cancer Motion Picture Guide, 22; U. S. Public Health Service, Cancer Control Branch; and Cancer Film Guide, 19).
52. On the gendered messages in this movie, see Reagan, “Engendering the Dread Disease.”
53. Two other movies aimed at men draw on analogies with work: The Traitor Within conjured up anxieties about industrial disruption with portrayals of the body as a series of factories and cancer as workers gone bad, and You Are the Switch-man conjured up the image of the railway switchman to illustrate the consequences of delay and early detection. In the case of the latter movie, the film asks us to imagine John as the switchman, deciding which track his life will take (delay or early detection and treatment), just as the railway switchman decides which track the train will take. in Man Alive, Ed Parmalee’s decision to seek medical advice follows from the narrator explaining the mechanical analogy— it is central to his decision to convert. This is not the case with the industrial analogies in Traitor Within and You Are the Switchman. The mechanical analogy found in Man Alive is also briefly referred to in the story of Mario, the owner of a gas station who ignored a persistent cough, which is told in A Doctor Speaks His Mind.
54. Some movies might remain available in film libraries long after the ASCC/ACS retired them. However, the ASCC/ACS tended not to promote these legacy films in its educational campaigns.
55. Sometimes images of cancer were used as a warning of what could happen if people delayed and sometimes as a stimulus to giving for research. several images of cancer and early cancers were provided by the AsCC for the public in Anon., “Lantern Slides on Cancer.” Before and after photographs were used to show the wonders of new therapies and to urge early treatment (Anon., “U.S. Science Wars Against an Unknown Enemy: Cancer”). See also Anon., “Cancer: The Great Darkness.”
56. I am relying here on those posters discussed in the ASCC/ACS’s news-letters, and in American society for the Control of Cancer, Catalog of Educational Material. For an article enthusing on the value of posters to the ASCC, see Rigney, “Does Medical Publicity Work Really Have a Place?” 7.
57. See the following advertisements: Anon., “Advice for Preventing Unneces-sary Sickness in Texas,” esp. [3]; and Anon., “New Cancer Poster.” Where illustra-

325David Cantor
tions were used, they tended not to illustrate the warning signs themselves, but the consequences of acting or not acting appropriately upon discovering such warning signs, or they tended to show the location of these signs in the body rather than the signs themselves. (Anon., “If Daddy Had Only Known of This!”).
58. Thus, for example, a “By The Way” poster from the c.1940s showed the thickening in the breast in a stylized form, and “Symptoms and Diagnosis,” an exhibit, also from the 1940s, showed warning signs (Both in American society for the Control of Cancer, Catalog of Educational Material).
59. Mitchell, Iconology; Mitchell, Picture Theory.60. For example, in Choose to Live, the signs are described by a physician. in
Man Alive, they are listed in a poster that the characters view, and in Man Alive and The Traitor Within, the location of the warning signs (but not the warning signs themselves) are indicated in the visuals.
61. see, for example, Challenge: Science Against Cancer, The Doctor Speaks His Mind, and You Are the Switchman, all of which displayed skin or lip cancers. At the same time, movies also began to show other body parts previously not show, includ-ing from the late 1940s women’s breasts. Compare the discrete breast examination in Reward of Courage with the medical and self-examinations in Breast Self-Examination. On the breast self-examination movie, see Reagan, “Projecting Breast Cancer.”
62. in Time and Two Women, the discharge from uterine cancer is shown through animation. In Inside Magoo, the nearsighted central figure worries about cancer when he mistakes the paint dripping from his head for blood. in Traitor Within, there is a remarkably clean animated depiction of surgery.
63. Thus, in Reward of Courage, an animated sequence shows the growth and dissemination of cancer subjects. The animated sequence allowed viewers to be shown aspects of cancer that would normally only be seen by the knife and the microscope. the contrivance is that these images are from a book that the live actors are viewing.
64. Cantor, “Uncertain Enthusiasm”; Cantor, “Before Survivorship.”65. For operation scenes, see Time is Life and Choose to Live. For cancers, see
Battle against Cancer and Challenge: Science Against Cancer. For mastectomy scars, see After Mastectomy.
66. Cantor, “Before Survivorship.”67. Anon., “testing of the Film, Time and Two Women.” More generally, on
efforts to evaluate the importance of movies to cancer education programs, see Survey Research Center, The American Public Discuss Cancer, 28, 29 and 87. Also, horn, Kipnis, and Craig, Public Opinion on Cancer. On lay education in the post-war period, see Wilzbach, “Lay Education.”
68. to this end, it also provided materials that might help an expert prepare for a film show and conduct the discussion. See, for example, the folder for film forums Get One Man Up on His Feet issued by the ACS c.1949 (Anon., “New Public Education Material,” 12).
69. For an example of how the ACS sought to organize film showings and embed them in other forms of communication, including program packets, see Anon., “Taking a Fresh Look.” See also the advice given to volunteers in Anon., “How to tell Neighbors.”
70. Anon., “Education vs. Cancer.”71. For some exceptions, see Cantor, “Uncertain Enthusiasm,” 59.72. On Lasker’s take-over of the ASCC, see Patterson, Dread Disease, 172–179;
and gardner, Early Detection, 95–104.73. see, for example, This is Serious Business, a tv play for the ACs Con-
necticut division which appeared on WNHC, New Haven, in 1951 (Anon., “Volunteer actors appear in a TV play . . .”).
74. Two examples illustrate the point: Tactic (1959) and Operation Cancer (1954). on Tactic, see: Anon., “T.V. Guide Will Carry a Color Photo Story on Tactic . . .”;

326 Choosing to Live
Anon., “Crusader Publicity Check List”; Corwin, “Tactic”; Anon., “Cancer Goes to College”; Anon., “The Series of 6 TV Shows . . .”; Anon., “National Notes”; Anon., “Tactic to Reach Early Audience of 12 Million”; Anon., “Variety Lauds Tactic”; and Anon., “The Virginia Experience with Tactic.” On Operation Cancer, see: Anon., “TV Program Cited”; and American Cancer Society, Annual Report [1954], 27.
75. Copies of these are available in the ACS archives in Atlanta. A selection of these is also available in Man on the Other Side of the Desk.
76. American Cancer society, Annual Report [1956], 30.77. For examples of movies that crossed over from public shows to television,
see Alexander Ten Spot, Man Alive, and Traitor Within.78. American Cancer Society Annual Report [1956], 30.79. Cancer: Its Cure and Prevention; The Battle Against Cancer; From One Cell;
Challenge: Science Against Cancer; The Fight against Cancer; The Outlaw Within; and Cancer: A Research Story.
80. For example, the humorous short Alexander Ten Spot was a film in which a cartoon version of Alexander Hamilton jumps off a ten dollar bill and shows how the ACS allocates a $10 gift for various purposes in the fight against cancer. Ham-ilton was apparently already converted to the ACS cause (Anon., “Alexander Tells a Story”; and Anon., “Television Campaign is Set, Features Two Special Films”).
81. Only two movies aimed at volunteers have been viewed: The Man on the Other Side of the Desk and Eight Out of Ten. Published descriptions of other volunteer movies do not put conversion at the heart of the narrative. These other movies included: To Save These Lives, which aimed to recruit volunteers for ACS public-education programs; The House-to-House Campaign, which taught ACS volun-teers and officials how to organize successful door-to-door campaigns; Much Ado about Something, which was an “All Star” round-up that showed how more than a dozen celebrities helped the Society; and Never Alone, which was a celebratory story of the ACs and its work (American Cancer society, Annual Report [1950], 16; Braddock, “Films for Teaching Mass Communication,” 167; American Cancer Society, Annual Report [1957], 32; American Cancer Society, Annual Report [1958], 32; and Anon., “Medical Film Reviews”).
82. Of the three breast self-examination movies released before 1960—Life Sav-ing Fingers, Breast Self Examination, and Breast Self-Examination: An Urgent Message to All Women—only the Breast Self-Examination seems to hint at a conversion. in this film Mrs. Wright attends a talk by Dr. Williams at her Women’s club and appears to be persuaded to see her own physician when she nods (in agreement?) with comments by the physician. But, if this is a conversion story, it is a very truncated one. In early detection films, the story of delay was often used as a way of setting up the eventual conversion. But there is little emphasis on the problem of delay in the movie, and most of this film, like the other BSE films, focuses on teaching women techniques of breast self-examination. On breast examination movies, see Reagan, “Projecting Breast Cancer.”
83. Anon., “The Other City.”84. Another example of this technique is The Warning Shadow. this dramatic
documentary film re-enacts the first successful pneumonectomy undertaken in 1933 by the thoracic surgeon Evarts A. Graham on the obstetrician James L. Gilmore. After this reenactment, we are introduced to the real Evarts and Gilmore (who survived the operation), who both reminisce about the operation and use its success to stress the point that that lung cancer is curable. This is followed by a description of how cancer spreads from a local to a general condition and then by a series of vignettes that tell stories of several patients to promote the idea that every man over forty-five should have a chest x-ray twice a year: the ‘warning shadow’ on their chest x-rays saved all these men. none are conversion narratives, except to the extent that gilmore decides to have the operation. The Warning Shadow was released shortly after Breast Self Examination, and the ACs saw it as an effort to

327David Cantor
reach out to men (Anon., “Army Launches Educational Offensive”; ACS Annual Report, [1953], 14 and 23; and ACS, Annual Report [1954], 21).
85. Cantor, “Uncertain Enthusiasm,” 57–8.86. In earlier years, spots might not have been regarded as “films.” Before
television, the ASCC/ACS had distinguished between full-length films (from twenty to thirty minutes) and shorts (approximately ten minutes), trailers, and spots (Anon., “How to Tell Neighbors, Your Country about Cancer”). But as it tried to adapt its films to television, its movies were shortened to fit television schedules, and the distinction between shorts, spots, trailers, and films sometimes blurred. See, for example, the discussion of Worry and Doubt (c.1951), a movie which aimed to show the futility of worrying and doing nothing about cancer, sometimes described as a “television trailer” and distinguished from ‘television films’ and sometimes described as a “short motion picture” (ACS, Annual Report [1951], 26; Anon., “How to Tell Neighbors, Your Country about Cancer”).
87. The ostrich film is shown in The Man on the Other Side of the Desk.88. Man Alive, with its conversion story centered on ed Parmalee, was also
shown on television.89. On pre-war efforts to tell stories about cancer, see Clow, Negotiating Dis-
ease. For discussions of the post-Second World War rise of cancer narratives, see for example, hawkins, Reconstructing Illness, esp. chapter 2, and Deshazer, Fractured Borders. For lay attitudes toward cancer and quackery, see Cantor, “Cancer, Quackery and the Vernacular Meanings of Hope in 1950s America.”
BIBLIOGRAPHY
Primary Literature
American Cancer society. Annual Report. 1950.American Cancer society. Annual Report. 1951.American Cancer society. Annual Report. 1953.American Cancer society. Annual Report. 1954.American Cancer society. Annual Report. 1956. American Cancer society. Annual Report. 1957.American Cancer society. Annual Report. 1958.American society for the Control of Cancer. Catalog of Educational Material. new
York: American Society for the Control of Cancer, c.1941–4. Anon. “ACS Drive Film Clicks in Capital.” ACS Campaign Bulletin, no. 47 (May
4, 1948): 4.———. “Advice for Preventing Unnecessary Sickness in Texas.” Campaign Notes of the
American Society for the Control of Cancer 1, no. 3 (March 15, 1918): [2–3].———. “‘A Fortunate Accident’ the New Cancer Film.” Campaign Notes of the ASCC
7, no. 2 (1925): [4].———. “Alexander Tells a Story. Film Shows where Funds Go.” ACS Bulletin 4,
no. 14 (March 28, 1955):1.———. “A Nagging Wife May Save your Life.” Cancer News 8, no. 4 (october
1954): inside back cover.———. “Animated Film to Launch Drive for Recruits.” ACS Campaign Bulletin 5,
no. 2 (January 10, 1950): 2.———. “Army Launches Educational Offensive.” ACS Bulletin 4, no. 1 (september
27, 1954): 4–5.———. “Cancer Goes to College,” Signals: Public Education Newsletter 6, no. 2
(Winter 1961): [4].———. “Cancerophobia.” Bulletin of the American Society for the Control of Cancer 16,
no. 2 (February 1934): 10–12.

328 Choosing to Live
———. “Cancer: The Great Darkness.” Fortune 15, no. 3 (March 1937): 112–14, 162, 164, 167–68, 170, 172, 174, 176, and 179.
———. “Cinematographic Instruction.” Boston Medical and Surgical Journal 186 (May 25, 1922): 714.
———. “Consolidated Report of the President and Executive Committee.” Campaign Notes of the American Society for the Control of Cancer 4, no. 3 (March 1922): [3–4].
———. “Crusader Publicity Check List.” PR Crusader 1, no. 4, (April 1959): [4].———. “Education vs. Cancer.” Sight and Sound. National Magazine of Sight and
Sound in Education 5, no. 2 (October 1949): 31.———. “How to Tell Neighbors, Your County About Cancer.” ACS Bulletin 2, no.
1 (September 29, 1952): 4.———. “If Daddy had Only Known of This!” Campaign Notes of the American Society
for the Control of Cancer 3, no. 4 (April 1921): [4]. ———. “Intelligence and Cancer Control.” Bulletin of the American Society for the
Control of Cancer 16, no. 2 (February 1934): 9–11.———. “Is Cancer Education Effective?” Bulletin of the American Society for the Control
of Cancer 16, no. 9 (September 1934): 3.———. “Lantern Slides on Cancer.” Campaign Notes of the American Society for the
Control of Cancer 1, no. 14 (June 1919): [2–4].———. “Letter Prepared for Federation of Churches, Ministers and General Cir-
culation in Massachusetts CANCER WEEK.” Campaign Notes of the American Society for the Control of Cancer 4, no. 4 (April 1922): [3].
———. “Medical Film Reviews.” Journal of the American Medical Association 170, no. 9 (June 27, 1959): 1112.
———. “Milwaukee.” ACS Campaign Bulletin 1948, no. 44 (April 13 1948): 3.———. “Murphy Seeks Check on Film.” ACS Campaign Bulletin 1948, no. 44 (April
13, 1948): 2.———. “National Notes.” Signals: Public Education Newsletter 3, no. 1 (February
1959): [6].———. “New Cancer Film Prepared for Campaign Use.” Cancer News 2, no. 4
(1948): 16.———. “New Film Ready for Use in Drive.” ACS Campaign Bulletin, no. 42 (March
30, 1948): 2.———. “New Cancer Poster.” Campaign Notes of the American Society for the Control
of Cancer 1, no. 16 (August 1919): [4].———. “New Public Education Material.” Cancer News 3, no. 5 (May 1949):
12–13.———. “Recruiting Movie.” Cancer News 4, no. 3 (March 1950): 11.———. “Society for Cinematographic Instruction in Medicine and Surgery.” Medical
Woman’s Journal 28 (1921): 240.———. “Suggested Plans for National Cancer Week. November 12–18, 1922.” Cam-
paign Notes of the American Society for the Control of Cancer 4, no. 8 (August 1922): [1–4].
———. “Tactic to Reach Early Audience of 12 Million.” PR Crusader 1, no. 1 (Janu-ary 1959): [4].
———. “Taking a Fresh Look.” Signals. Public Education Newsletter 4, no. 4 (June 1960): [1–2].
———. “Television Campaign is Set, Features Two Special Films.” ACS Bulletin 4, no. 13 (March 21, 1955): 2.
———. “Testing of the Film, TIME AND TWO WOMEN.” Signals: [ACS] Public Education Newsletter 1, no. 1 (1957): 3–4.
———. “The Church Letter.” Campaign Notes of the American Society for the Control of Cancer 5, no. 10 (October 1923): [3].
———. “The Moving Picture and the National Character.” The American Review of Reviews 42 (1910): 315–320.

329David Cantor
———. “The Other City.” Cancer News 11, no. 2 (Spring 1957): 6–8.———. “The Present Status of the Educational Campaign against Cancer.” Bulletin
of the American Society for the Control of Cancer 17, no. 2 (February 1935): 10–11.
———. “The Radio as a Pioneer in Cancer Education.” Bulletin of the American Society for the Control of Cancer 18, no. 4 (April 1936): 9–10.
———. “The Rockefeller Gift.” Campaign Notes of the American Society for the Control of Cancer 3, no. 5 (May 1921): [2–3].
———. “The Series of 6 TV shows . . .” Signals: Public Education Newsletter 4, no. 1 (September 1959): [4].
———. “The Virginia Experience with Tactic.” PR Crusader 2, no. 1 (October 1959): [3–4].
———. “T.V. Guide Will Carry a Color Photo Story on Tactic . . .” PR Crusader 1, no. 4 (April 1959): [3].
———. “TV Program Cited.” ACS Bulletin 3, no. 14 (April 5, 1954): 3.———. “Utah.” Campaign Notes of the American Society for the Control of Cancer 4,
no. 6 (June 1922): [2–3]. ———. “Variety Lauds Tactic.” PR Crusader 1, no. 2 (February 1959): [3].———. “Volunteer Actors Appear in a TV Play . . .” ACS Bulletin 1, no. 5 (De-
cember 17, 1951): 2.———. “U.S. Science Wars Against an Unknown Enemy: Cancer,” Life Magazine 2,
no. 9 (March 1, 1937), 11–17.Bluestone, E.M. “The Importance of Cancer Education.” Bulletin of the American
Society for the Control of Cancer 15, no. 7 (July 1933): 5–6.Braddock, Richard. “Films for Teaching Mass Communication.” English Journal 44,
no. 3 (March 1955): 156–8, 167.Cancer Control Program and the National Library of Medicine. Cancer Motion
Picture Guide. Washington, DC: US Department of Health, Education, and Welfare, 1961.
Clarkson, Wright and Allen Baker. “Cancer Control.” Bulletin of the American Society for the Control of Cancer 18, no. 7 (July 1936): 3–5.
Corwin, emil. “Tactic.” Cancer News 13, no. 3 (Summer 1959): 9–12.Dewey, William. “Recent Additions to the Film Library.” Bimonthly Bulletin of the Wis-
consin State Board of Health 8, no. 19 (November–December, 1949): 560–1.Dozier, Henry C. “The Layman’s Responsibility in the Control of Cancer.” Bulletin
of the American Society for the Control of Cancer 18, no. 11 (November 1936): 6–7.
Edlin, James S. “Cinematography: Its Uses in Teaching Medicine and Surgery—A Prophecy in Fulfillment.” International Journal of Surgery 35 (1922): 191–4.
———. Letter to Simon Flexner, September 5, 1921. American Philosophical Society, Society for Cinematographic Instruction in Medicine and Surgery, Simon Flexner Papers, BF 365.
Fisk, Eugene Lyman. “A Deadly Foe Routed. Overtake Cancer Early and It Is Easily Prevented.” Campaign Notes of the American Society for the Control of Cancer 1, no. 10 (February 1919): [1–4].
horn, Daniel, David Kipnis, and Leonard Craig. Public Opinion on Cancer and the American Cancer Society. Report of a National Survey. New York: American Cancer Society, April, 1956.
Lakeman, Mary R. “Cancer Education in Massachusetts.” In Cancer and Other Chronic Diseases in Massachusetts, edited by george h Bigelow and herbert L Lombard, 147–59. Boston: Houghton Mifflin, 1933.
Little, C. C. “How to Educate Women to Recognize Breast Tumors.” Bulletin of the American Society for the Control of Cancer 16, no. 8 (August 1934): 9–12.
O’Brien, William A. “The Use of Radio in Cancer Education.” Bulletin of the American Society for the Control of Cancer 18, no. 5 (May 1936): 7–9.

330 Choosing to Live
Rigney, Ella Hoffman. “Does Medical Publicity Work Really Have a Place?” Cam-paign Notes of the American Society for the Control of Cancer 11, no. 8 (August 1929): 7–8.
Salzstein, Harry C. “Cancer Education: A Note.” Bulletin of the American Society for the Control of Cancer 16, no. 9 (September 1934): 10–12.
Survey Research Center. The American Public Discuss Cancer and the American Cancer Society Campaign. A National Survey. Ann Arbor, MI: Survey Research Center, University of Michigan, December 1948.
U. S. Public Health Service, Cancer Control Branch. Cancer Film Guide. Washington, DC: US Department of Health Education and Welfare, 1963.
Wilzbach, Carl A. “Lay Education.” In Proceedings of Inservice Training Course on Cancer Services for Health Directors and Public Health Nurses, January 26, 27, and 28, 1948, 83–8. Ann Arbor: University of Michigan, School of Public health, 1948.
Secondary Literature
Aronowitz, Robert A. “Do Not Delay: Breast Cancer and Time, 1900–1970.” Milbank Quarterly 79 (2001): 355–86.
———. Unnatural History: Breast Cancer and American Society. Cambridge and new York: Cambridge University Press, 2007.
Bowser, eileen. The Transformation of Cinema, 1907–1915. Berkeley: University of California Press, 1994.
Cantor, David. “Before Survivorship: The ‘Moment of Recovery’ in Twentieth Century American Cancer Campaigns.” Paper presented to the NIH History Office work–in–progress seminar program held at the National Institutes of Health, Bethesda, MD, April 6, 2010.
———. “Uncertain Enthusiasm: The American Cancer Society, Public Education, and the Problems of the Movie, 1921–1960.” In Cancer in the Twentieth Century, edited by David Cantor, 39–69. Baltimore: Johns Hopkins University Press, 2008.
———. “Cancer, Quackery and the Vernacular Meanings of Hope in 1950s America.” Journal of the History of Medicine and Allied Sciences 61 (2006): 324–68.
———, ed. Cancer in the Twentieth Century. Baltimore: Johns Hopkins University Press, 2008.
Caldwell, Patricia. The Puritan Conversion Narrative: The Beginnings of American Ex-pression. New York: Cambridge University Press, 1983.
Cartwright, Lisa. Screening the Body: Tracing Medicine’s Visual Culture. Minneapolis: University of Minnesota Press, 1995.
Clow, Barbara. Negotiating Disease: Power and Cancer Care, 1900–1950. Montreal: McGill–Queen’s University Press, 2001.
Cohen, Charles Lloyd. God’s Caress: The Psychology of Puritan Religious Conversion. New York: Oxford University Press, 1986.
Deshazer, Mary K. Fractured Borders: Reading Women’s Cancer Literature. Ann Arbor: University of Michigan Press, 2005.
Dorsey, Peter A. Sacred Estrangement: The Rhetoric of Conversion in Modern American Autobiography. University Park: Pennsylvania State University Press, 1993.
Doane, Mary Ann. The Desire to Desire: The Woman’s Film of the 1940s. Bloomington: indiana University Press, 1987.
Fell, John. Film and the Narrative Tradition. Norman: University of Oklahoma Press, 1974.
gardner, Kirsten e. Early Detection: Women, Cancer, & Awareness Campaigns in the Twentieth-Century United States. Chapel Hill: University of North Carolina Press, 2006.

331David Cantor
Gledhill, Christine. “The Melodramatic Field: An Investigation.” In Home is Where the Heart Is: Studies in Melodrama and the Woman’s Film, edited by Christine Gledhill, 5–39. London: British Film Institute, 1987.
grieveson, Lee. Policing Cinema: Movies and Censorship in Early-Twentieth-Century America. Berkeley: University of California Press, 2004.
Hawkins, Anne Hunsaker. Reconstructing Illness: Studies in Pathography, 2nd ed. West Lafayette, IN: Purdue University Press, 1999.
Lederer, Susan E. and Naomi Rogers. “Media.” In Medicine in the Twentieth Cen-tury, edited by Roger Cooter and John Pickstone, 487–502. Amsterdam, the Netherlands: Harwood Academic Publishers, 2000.
Lerner, Baron. The Breast Cancer Wars: Hope, Fear, and the Pursuit of a Cure in Twentieth-Century America. New York: Oxford University Press, 2003.
May, Larry. The Big Tomorrow: Hollywood and the Politics of the American Way. Chicago: University of Chicago Press, 2002.
McConachie, Bruce. Melodramatic Formations: American Theatre and Society, 1920–1870. Iowa City: University of Iowa Press, 1992.
Mitchell, W. J. T. Iconology: Image, Text, Ideology. Chicago: University of Chicago Press, 1986.
———. Picture Theory: Essays on Verbal and Visual Representation. Chicago: University of Chicago Press, 1994.
neale, steve. Genre and Hollywood. London: Routledge, 2000.Nichtenhauser, Adolf. “A History of Motion Pictures in Medicine.” Unpublished
manuscript, c.1950. Adolf Nichtenhauser History of Motion Pictures in Medicine Collection, MS C 380, Archives and Modern Manuscripts Program, History of Medicine Division, National Library of Medicine.
Parker, Alison M. Purifying America: Women, Cultural Reform, and Pro-Censorship Activism, 1873–1933. Urbana: University of Illinois Press, 1997.
Patterson, James t. The Dread Disease: Cancer and Modern American Culture. Cam-bridge, MA: Harvard University Press, 1987.
Pernick, Martin S. The Black Stork: Eugenics and the Death of “Defective” Babies in American Medicine and Motion Pictures Since 1915. New York: Oxford Univer-sity Press, 1996.
Pernick, Martin S. “Thomas Edison’s Tuberculosis Films: Mass Media and Health Propaganda.” Hastings Center Report 8 (June 1978): 21–7.
Reagan, Leslie J., Nancy Tomes, and Paula A. Treichler. Medicine’s Moving Pictures: Medicine, Health, and Bodies in American Film and Television. Rochester, NY: University of Rochester Press, 2007.
Reagan, Leslie J. “Engendering the Dread Disease: Women, Men, and Cancer,” American Journal of Public Health 87 (1997): 1779–87.
———. “Projecting Breast Cancer. Self-examination Films and the Making of a New Cultural Practice.” In Medicine’s Moving Pictures: Medicine, Health, and Bodies in American Film and Television, edited by Leslie J. Reagan, Nancy Tomes, and Paula A. Treichler, 163–198. Rochester, NY: University of Rochester Press, 2007.
Roberts, Samuel. Infectious Fear: Politics, Disease, and the Health Effects of Segregation. Chapel Hill: University of North Carolina Press, 2009.
Rosen, George. A History of Public Health, expanded ed. Baltimore: Johns Hopkins University Press, 1993.
Shryock, Richard Harrison. National Tuberculosis Association, 1904–1954: A Study of the Voluntary Health Movement in the United States. New York: National Tu-berculosis Association, 1957.
singer, Ben. Melodrama and Modernity: Early Sensational Cinema and Its Contexts. new York: Columbia University Press, 2001.
tomes, nancy. The Gospel of Germs: Men, Women, and the Microbe in American Life. Cambridge, MA: Harvard University Press, 1998.

332 Choosing to Live
vardac, A. nicolas. Stage to Screen: Theatrical Method from Garrick to Griffith. Cam-bridge, MA: Harvard University Press, 1949.
Wiatr, Elizabeth Ann. “Seeing American: Visual Education and the Making of Modern Observers, 1900–1935.” PhD diss., University of California, Irvine, 2003.
———. “Between Word, Image, and the Machine: Visual Education and Films of Industrial Process.” Historical Journal of Film, Radio, and Television 23 (2002): 333–51.



![MATINS OF THE DEAD - haligweorc.files.wordpress.com€¦ · Web view[Remain standing] Cantor: The King to whom all live; / come, let us adore him. Choir: The King to whom all live;](https://img.dokumen.tips/doc/110x75/5f800f126f666434544824df/matins-of-the-dead-web-view-remain-standing-cantor-the-king-to-whom-all-live.jpg)


![From: Alderucci, Dean - Cantor Fitzgerald [mailto:DAlderucci@cantor… · 2019-02-07 · From: Alderucci, Dean - Cantor Fitzgerald [mailto:DAlderucci@cantor.com] Sent: Wednesday,](https://img.dokumen.tips/doc/110x75/5f7ae1df7225817acd095b1d/from-alderucci-dean-cantor-fitzgerald-mailtodalderuccicantor-2019-02-07.jpg)