Embed Size (px)
Citation preview

Cancer Services Overviewfor Northeast Georgia Medical Center
The Cancer Center at Northeast Georgia Medical Centercontinues to grow as it provides state-of-the-art treatment andcompassionate care close to home. As technologic advancesand new cancer therapies become available, the CancerCenter has become a leader in delivering cancer care in north-east Georgia.
This year, the American College of Surgeons awarded a three-year accreditation with commendation to the Cancer Center.This designation recognizes that our cancer program exceedednational standards in delivering cancer care. For patients,that means they can expect to receive the best cancer carepossible here.
This year, the Cancer Center implemented digitalmammography, and by the end of the year, will be providingbreast MRI. Additional upgrades to MRI capabilities willenhance diagnostic imaging for GI and GU malignanciesincluding hepatocellular, rectal and prostate cancers. Withthe rapid growth of the Cancer Center, Radiation Oncologywill require physical expansion, to accomodate plans for theradiosurgery program and Image Guided Radiation Therapy.
The clinical trials program at the Cancer Center continues tobe strong, again exceeding the previous years’ number ofpatient accruals. This year, more than eight percent ofpatients participate in clinical trials, a proportion quadruplenational averages.
The strength and reputation of the Cancer Center is due tothe dedicated physicians, nurses and healthcare professionalscommitted to a multi-disciplinary team approach to cancercare. We strive to provide compassionate and cutting edgecare to the community we serve.
Richard LoCicero, MD, Medical Oncologist2006 Chairman, Cancer Committee
2*2006 Annual Report reflects data from 2005

2006 CancerCommittee Members
Carson Agee, MD SurgeonBradley Auffarth, MD SurgeonPierpont Brown, MD SurgeonAllen Butts, MD SurgeonDavid Carroll, MD RadiologistJoe Conway, MD PathologistKen Dixon, MD SurgeonCasey Graybeal, MD SurgeonJack Griffeth, MD Radiation OncologistAndre Kallab, MD Medical OncologistAnup Lahiry, MD Medical OncologistFrank Lake, MD Radiation OncologistRon Lewis, MD SurgeonRichard LoCicero, MD – Chairman Medical OncologistChris Malone, MD SurgeonCharles Nash, MD Medical OncologistRichard Olson, MD – Co-Chairman SurgeonAntonio Rios, MD InternistNancy Stead, MD Medical OncologistPriscilla Strom, MD SurgeonRandall Thomas, MD Medical OncologistGeoff Weidner, MD Radiation OncologistDan Winston, MD SurgeonDavid Woo, MD UrologistNatalie Allison Outpatient Case ManagementTom Enright Oncology AdministrationKimberly Kamppi Performance ImprovementDianne Kosmala Cancer RegistrarBeth Meers Chief Radiation TherapistRandall Miller Chief Radiation PhysicistVicki Miller Regional Network MarketingJolinda Martin AdministrationPaula Pitts Inpatient/OP ManagerPatti Rotunda Registry/Research ManagerJeff Thompson ClergyDonna Topping PharmacyTeresa Warren Hospice
3
The number of cases entered into theNGMC cancer registry continues toincrease (Figure 1). Twelve hundred caseswere identified during 2005.
The most frequent cancers continue tobe breast, prostate and lung with primar-ies in the colon being almost fifty percentless frequent (Figure 2). These primariescomprise 61 percent of analytic cases.Non-Hodgkin lymphoma, melanoma,hematologic malignancy, bladder and thy-roid primaries each represent four per-cent of cases. With the exception of lungcancer, the rank order of malignancies atNGMC parallels that of the country as awhole.
Soft tissue sarcomas are a mixed group ofmalignancies which have in commontheir origin in the non-bone muscu-loskeletal tissues; fat, muscle, fibrous tis-sue and blood vessel are included. Thefrequency of gastrointestinal stromaltumor is increasing because immunohis-tochemical staining for c-kit proteinenables its differentiation from other softtissue sarcomas. NGMC doctors haveentered enough patients in the AmericanCollege of Surgeons adjuvant chemother-apy trial for this disease that awareness ofthis hospital’s cancer program is occur-ring outside of Georgia.
The frequency of cancers in women againparallels that of men when the sixthdecade is reached; however, in the fourthand fifth decades there are more cases inwomen than in men (Figure 3). Eightypercent of malignancies in the fourthdecade and more than 50 percent of
2005 Registry OverviewNancy Stead, MD, Medical Oncologist
Figure 1
Figure 2
4
1980 – 2005 Annual Analytic Case Load Total
Northeast Georgia Medical CenterTop Five Sites

RabunTowns
UnionFannin
Gilmer
Lumpkin
White Habersham
Stephens
HallDawson
Forsyth
Pickens
Gwinnett
Jackson
Hart
Barrow
North Carolina (15)
25-150 1-24>400
Florida (2)
Franklin
Cobb
DeKalb
South Carolina (1)
Clarke
Fulton
Hancock
Oglethorpe
Walker
Virginia(1)
Banks
2005 NGHS AnalyticCases by County
those in the fifth decade occure in females. Ninety to100 percent of the excess frequency of cancer resultsfrom breast adenocarcinomas.
Cancer screening is effective. Only nine patients hadinvasive cervical carcinoma. The percentage ofprostate and breast malignancies identified at stages 0– 2 is 88 and 79.6 respectively. Only 52 percent ofcolon malignancies present at stages 0 – 2 diseaseprobably because people are more willing to undergo
screening by mammography or measurement of PSAlevel than by colonoscopy. There is no proven screen-ing test for lung cancer. Stage 0 – 2 disease occursonly 26 percent of the time (Figure 4).
The Cancer Center at NGMC is a regional resource.Fifty-four percent of patients reside outside Hall County.Thirty percent reside in counties served by the ToccoaCancer Center (Figure 4).
Figure 3
Figure 4
5
2005 NGMC Analytic CasesStage at Diagnosis
Male vs Female By Age at DiagnosisGender & Age 2005
Figure 5
The thyroid gland lies low in the neck in front of thewindpipe, guarding it like a shield, after the Greek wordfor shield, “thyreos.” Its function is to produce thyroidhormone, an iodine containing protein which is secretedinto the bloodstream. This hormone then acts as a gov-ernor on the degree of activity of the other organs in thebody.
Most cancers of the thyroid are within the well-differ-entiated family of cancers called papillary or follicularcancers. These comprise95 percent of the total30,000 cancers of the thy-roid that occur annuallywithin the U.S. Most thy-roid cancers are diagnosedby the presence of an oth-erwise asymptomatic masswithin the thyroid. Whilemost of these nodules arebenign, one of the issueswith management of thesepatients is the relativeinability to tell which thy-roid nodules are cancerousand which are benign.
Aspiration of some thy-roid cells with a small needle can often give guidanceabout whether the nodule is benign or suspicious forcancer. However, while less than 10% of all solitary nod-ules are cancerous, because of uncertainty as to the diag-nosis, surgeons not infrequently end up operating andremoving the thyroid, or part of it, in many patients inwhom the ultimate diagnosis turns out to be benign (seeFigure 1). Fortunately, surgeons across the world andhere in Gainesville are able to do this surgery with a verylow complication rate. And, best of all, the success ratein curing thyroid cancers is excellent with a long termcure rate of well over 90 percent.
In the patient who ends up having the thyroid, orpart of it, removed because of a thyroid cancer, some-
times the only other treatment is replacement of the thy-roid hormone that the patient is no longer able to make.However, many patients also receive additional treatmentin the form of a tablet of radioactive iodine. This iodineis preferentially taken up by any remaining thyroid cells,thus wiping out potential residual malignancy.
Thirty-five patients had thyroid cancer treated here atNortheast Georgia Medical Center in 2005. Of these,31 were of the less aggressive papillary and follicular
types. One was a medullarycarcinoma, one an oxyphiliccarcinoma, one lymphoma,and one anaplasticcarcinoma.
Twenty patients under-went a total thyroidectomy,three a subtotal thyroidecto-my, and 12 a thyroid lobecto-my only. As is the case acrossthe rest of the U.S. andworld, this non-uniformity ofdegree of surgical resectionreflects the fact that mostpatients do well with thesecancers, even if differenttreatment regimens are uti-
lized. Thirteen patients then were additionally treatedwith radioactive Iodine 131.
On a programmatic note, over the last two years, twoendocrinologists, Drs. Matthey Harris and Carla Suarez-Welch, have joined the medical staff at NGMC. Theybring welcome additional expertise in the managementof the thyroid patient. Also, Dr. David Carroll hasassumed the leadership of the nuclear medicine depart-ment, which is central to the delivery of radioiodine tothese patients. These positive additions at NGMC willallow further expertise in the delivery of radioactiveiodine to thethyroid patient that needs it, as well as clarification ofwhich patients should be viewed as candidates for
6
Site Overview: ThyroidKen Dixon, MD, FACS, surgical oncologist
Northeast Georgia Medical CenterThyroid Initial Therapy 2005
Figure 1
7
radioactive iodine and which should be observed only.This writer holds the hope that, with the evolution of
our local medical community and hospital system to thesophisticated level of tertiary healthcare provision whichour region deserves, we will work diligently together to fur-ther standardize and optimize our treatment agendas forthis and other malignancies. In this way, we canultimately fulfill the motto of NGMC – to improve thehealth of this community in all that we do.
Thyroid Cancer Overview• 95% of the total 30,000 cancers of the thyroid
that occur annually within the U. S. are withinthe family of cancers called papillary or follicularcancers.
• Thirty-five patients had thyroid cancer treatedat Northeast Georgia Medical Center in 2005.Of these, 31 were of the less aggressive papillaryand follicular types.
• Aspiration of some thyroid cells with a smallneedle can often give guidance about whetherthe nodule is benign or suspicious for cancer.
• While less than 10 percent of all solitary nodulesare cancerous, because of uncertainty as to thediagnosis, surgeons often remove the thyroid, orpart of it, in many patients in whom the ultimatediagnosis turns out to be benign.
8
37536363
21620178
873
27392
2225415
239972
1025720254112
2396049
33426353
19919167
793
24382
2023715
222760
66381513359
2164729
4110010
171118030102
170
17212
36195
1263
231320
27514352
13315124
492
20241
1215211
141641
713816172284000
10022011
83554
3817151
10102
498331
311948
194
2356049
000000080105020000000000
N\A
N\A
N\A
N\A
20
38300
5201100
37251
14070110
556
49110
N\A
N\A
N\A
N\A
141
801503
2101000
45522
18181006
122
10110
N\A
N\A
N\A
N\A
31
54501
6002012
37211
19230202
734
69110
N\A
N\A
N\A
N\A
53
22713
13011221
51630
2104021
10843
81000
N\A
N\A
N\A
N\A
409510
7111020
174312002302808330
N\A
N\A
N\A
N\A
74
12902
000000040120000000505100
66381513001300
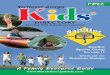
Oral Cavity***LipBase of TongueOther parts of tongueOther parts of mouthTonsilPyriform Sinus
Digestive CavityEsophagusStomachSmall IntestineColonRectosigmoid JCTRectumAnus and Anal CanalLiver – Intrahep Bile DuctsGallbladderPancreas
RespiratoryLarynxBronchus/LungHeartHeartBones/Jnts/Art Cart OT
Blood/Bone MarrowHematopoietic/Reticuloen
Multi MyelomaLeukemia
SkinConn, Subq & Oth SoftBreastFemale Genital
VulvaCervix Uteri
Total Cases Class of Case Male Female Analytic OnlyAnalytic Non-Analytic all cases 0 1 2 3 4 99* 88**
AJCC TNM Stage
2005 Primary Site Tablefor the Cancer Center at Northeast Georgia Medical Center

Totals 1362 1193 169 728 634 78 270 299 177 188 73 101
9
2520
226219
688393
428
1537215
4738
2113
194187
674332
357
1135214
3837
47
32320
1461714200191
00
226219
667272
35275112
2721
2520000
21121768
32103
2017
01000
2602
2100100000
93404
32230801
28001
130
31
167167
0610500000080
21
16132430100200140
136604400002002
110
43000220000200020
2111000000
1002000
37
Corpus UteriOvary
Male Genital***Prostate GlandTestis
UrinaryKidneyRenal PelvisBladder
MeningesBrainThyroid GlandAdrenal GlandOther Endocrine GlandsHodgkin DiseaseNon-Hodgkin Lym.Unknown Primary Site
* Stage unknown** Stage not applicable***Total includes cases not listed by site
10
Kidney/Renal Pelvis CancerBy David Woo, MD, urologist
Kidney cancers include malignancies that affect theconcentrating portion of the kidney — renal cell carcino-ma — and the collectingportion of the kidney —transitional cell carcinomaof the renal pelvis.Kidney and renal pelviscancers account for aboutthree percent of all cancercases in the U.S.
Kidney cancer inci-dence has been rising at arate of about two percenta year for the last 65 yearswith men having abouttwice the incidence aswomen. This rising trendis thought to be, at least partly, due to theincreased number of tumors found incidentally fromabdominal imaging such as computerized tomography(CT) before the cancer is symptomatic. (Figure 1)
Mortality from kidney cancer has increased slightlyover the past two decades, though not as rapidly as theincidence. In 2006, an esti-mated 38,890 new cases ofrenal cancer are expectedto be diagnosed andabout 12,840 are expectedto die.
Locally, the incidenceof kidney cancers in north-east Georgia has been onthe rise as well. In 2005,there were 42 new cases ofrenal cancers, up from 19in 2000. The five year sur-vival by stage of patients atNGMC diagnosed withkidney cancers comparesfavorably with the nationalaverages (see Figures 2 and 3).
The overall five year survival rate for all stages is about 50percent both locally and nationally.
The traditional treatmentfor renal cancers has beencomplete surgical removal ofthe involved organ throughan extensive open incision(radical nephrectomy).Selected patients withmalignant tumors, particu-larly those in whom theremoval of large amounts ofrenal tissue would result inthe significant loss of renalfunction, are appropriatelytreated with removal ofonly the involved portion
of the kidney (partial nephrectomy).In this era of minimally invasive surgery, many of
these same procedures can be performed laparoscopical-ly through smaller and less morbid incisions. Novelapproaches, such as radiofrequency ablation of renaltumors, have shown promise in treating these cancers
effectively with minimalblood loss or change in renalfunction.
Currently, these ablativetechniques are reserved forpatients who cannot toleratethe traditional surgical treat-ments. All of these thera-pies are in use at NGMCand the specific procedurechosen is based on multiplefactors: size and location oftumor, number of tumors,renal function, and co-mor-bid conditions.
Patients with metastaticdisease benefit from a multi-disciplinary approach where
Five Year Surv. Rates for Kidney and Renal PelvisCancer Cases Diagnosed in 1998
All States / Data Reported from 1251 HospitalsHospitals of Type: All
Northeast Georgia Medical CenterKidney/Renal Pelvis Survival 2000Fig. 2
Northeast Georgia Medical CenterGender and Stage at Diagnosis • Kidney Cases 2005
Fig. 1

11
input from medical oncologists, radiation oncologists,surgeons, pathologists,radiologists and ancillary services are shared.Combination therapy involving immunotherapy,chemotherapy, radiation and surgical debulking often
is required in treating and palliating the spread of kid-ney cancer. Newer and more promising therapeuticapproaches for advanced kidney and renal pelvis can-cers have been developed as our understanding of thebody’s natural immune response to malignancy grows.
At the recent annual meeting of the American Societyof Clinical Oncology held in Atlanta in June 2006, excit-ing new results of clinical trials were reported in front of astanding-room only crowd of thou-sands of physicians and researchers.Noted authorities labeled that presen-tation session a “banner day for kid-ney cancer.”
Two new agents, sunitinib(marketed as Sutent) and sorafinib(Nexavar), known in the medicaloncology world as “targeted therapy,”were shown to have eclipsed previoustherapies by impressive margins. The“target” appears to be the vascular endothelial growth fac-tor and its related biochemical pathways. The mechanismof action seems to be their ability to control certain aspectsof the growth and development and blood supply of can-cers. These drugs were FDA approved in January 2006 andDecember 2005, respectively.
Sunitinib bested interferon therapy in terms of progres-sion-free survival durations, 11 months vs. five months,and rate of response by 31 percent vs. 6 percent in patients
with good to intermediate risk features.Sorafinib significantly improved overallsurvival duration by 39 percent com-pared to placebo and doubled progres-sion-free survival duration to 24 weeks.These improved results also came withless toxicity than previous therapies.Both agents are oral medications aswell. A third drug, temsirolimus, alsoimproved overall and progression-freesurvival by 49 percent and 95 percent,
respectively in poor risk patients.These results also form the basis for new clinical trials
that use the agents in combination with other therapies.Improved results also are expected when patient “crossover” from one drug to the next. It seems clear that a newreference standard for kidney cancer therapy has beenachieved, and the future appears quite promising indeed.
New Breakthroughs in Kidney Cancer TherapyCharles H. Nash, III, MD, medical oncologist
Figure 3
12
When your patient is fighting cancer,he or she needs all the weapons possible.The physician specialists who practice atthe Cancer Center at NortheastGeorgia Medical Center want to workwith you in providing the top-qualitycancer care your patients need. Advanceddiagnostic and treatment options avail-able at the Cancer Center include:
Advanced Diagnostics• PET/CT scans• Endoscopic ultrasound staging for
gastrointestinal and lung cancers• Full range of other diagnostic
technologies including breast MRI,digital mammography, interventionalradiology and nuclear medicine
Medical Oncology• Chemotherapy, hormone and
biologic therapies
Radiation Oncology• Intensity Modulated Radiation
Therapy (IMRT)• External beam conformal therapy
and simulation• Low Dose Rate (LDR) brachytherapy
including prostate seed implants• High Dose Rate (HDR) brachytherapy
Surgical Oncology• Radiofrequency liver ablation (RFA)• Sentinel lymph node mapping for
breast cancer and melanoma• Stereotactic breast biopsy
Research (Clinical Trials)• Innovative, progressive therapies
endorsed by the National CancerInstitute
• Multiple treatment options availablethrough national research cooperativegroup and pharmaceutical companies
No longer do your patients have totravel to Atlanta – they can receivehigh-quality cancer care close tohome through the physician specialistswho practice at the Cancer Center.
To refer a patient or consult with aspecialist at the Cancer Center,call 800-404-6400.
The
Cancer Centerat Northeast Georgia Medical Center
Advanced care to help your patientsin their fight against cancer.
Clinical Trials at the Cancer CenterAndre Kallab, MD, medical oncologist
As the Oncology Research Committee Chair forNortheast Georgia Health System (NGHS), I would like toexpress appreciation to the numerous physicians dedicated tooffering their patients every option possible in regard to can-cer treatment by referral to a clinical trial.
Through your diligence, 2005 was a record year for accrualto oncology clinical trials at NGHS with an enrollment of 8.5percent of local analytical cases into clinical trials, comparedto the national average of approximately four percent.
NGHS currently offers oncology clinical trials for all majorcancer sites and, at any given time, approximately 50 to 60 tri-als are available for patient accrual. Many patients have hadthe opportunity to be treated withcutting edge therapies that would have otherwise beenunavailable to them. The trials offered involve componentssuch as chemotherapy, radiation therapy, surgery, hormonetherapy, and more, performed in both adjuvant and neo-adju-vant settings.
In 2005, the Oncology Research department wasapproved to participate in two large-scale national clinical tri-als. The first is a Phase III trial for recurrent metastaticprostate cancer from Novacea, a pharmaceutical company.
This trial is one of the largest prostate trials ever conductedand involves U.S. as well as Canadian research sites.Anticipated patient enrollment is 900 males, and the studyinvolves collaboration of both the patient’s urologist and amedical oncologist.
The second is the TAILORx trial, also know as TrialAssigning Individualized Options for Treatment (Rx).TAILORx examines whether genes that are frequently associ-ated with risk of recurrence for women with early-stage breastcancer can be used to assign patients to the most appropriateand effective treatment.
The study will enroll more than 10,000 women at 900 sitesin the U. S. and Canada. Women recently diagnosed withestrogen-receptor and/or progesterone-receptor positive,Her2/neu-negative breast cancer that has not yet spread to thelymph nodes are eligible for the study.TAILORx is sponsored by the National Cancer Institute(NCI), part of the National Institutes of Health (NIH), and iscoordinated by the Eastern Cooperative Oncology Group.
For more information about these trials, or any other trialswe are currently conducting, contact the NGHS OncologyResearch department at 770-533-8820.

The Cancer Center Community Outreach Programs reached a wide variety of people with cancer messages andscreenings in 2006. Tobacco use prevention programs were provided to more than 450 4th and 5th gradestudents in the region. Prostate screenings served just over 110 men in three screenings. Messages of skincancer prevention and cervical cancer awareness were promoted during the Tour de Georgia's Healthy Expo,and community events, like the Harvest of Hope and Relay for Life, provided opportunities to reach out tocancer survivors. Below is a sampling of some of the activities for the 2006 calendar year:
13
2006 Community Health Activities
SITES REVIEWED IN 2005 CANCER
CONFERENCES
Total 213
Bladder 5Breast 67Colon 21Lung 23Prostate 9Head & Neck 7Blood & Bone Marrow 1Skin 6Kidney 9Thyroid 1Liver/Pancreas 10Sarcoma 5GI Stromal 1Other 29
Tumor conferences provide physicians a venue fordiscussion that is invaluable to quality patientcare. Cases are selected for presentation becauseimmediate treatment decisions are needed, thecase has unique and/or educational value, orfollow-up information is being provided on apreviously presented case. Tumor board confer-ences benefit physicians and patients by providingaccess to the latest information on treatmentoptions and related issues.
In addition, continuing medical education (CME)seminars allow our expert cancer physicians toeducate other members of our medical and clini-cal staff regarding new technology, advanced treat-ment options or other topics of interest.
An average of more than 20 physicians and 15staff members attended 40 tumor boardconferences or continuing education seminars.In the course of the year, 213 cancer cases werepresented.
2005 Tumor BoardEducation Conferences
14
15
2006: A Year ofAccomplishments
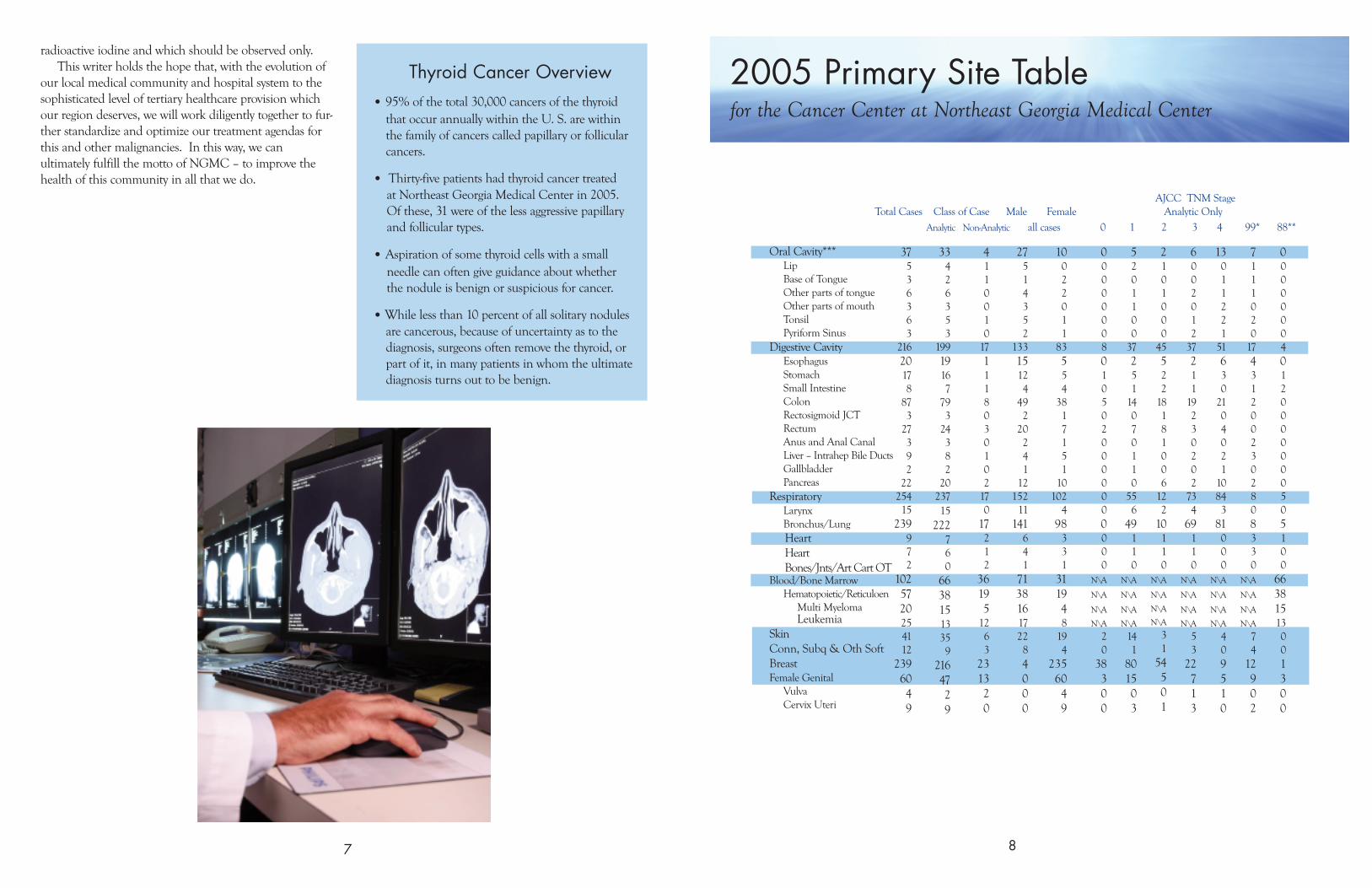
In 2006, the Cancer Center at Northeast Georgia Medical Center (NGMC) made significantprogress. Our leadership developed a process for increased physician involvement through thedevelopment of a Physician Advisory Group and finalized Radiation Therapy’s plans for a new lin-ear accelerator (linac). The addition of a new linac at NGMC’s Main Campus in Gainesville willallow us to provide stereotactic radiosurgery and imaged guided radiation therapy. Image guidedradiation therapy also will be added at the satellite facility in Toccoa.
In addition, breast cancer diagnosis advanced significantly with the installation of digital mammog-raphy and breast MRI, improving our capability to diagnose breast cancers earlier which, in turn,improves our patient’s chances for a positive outcome.
Our staff continues to log countless volunteer hours through expanded community outreach and,in 2006, served more than 1,500 individuals throughout northeast Georgia through cancer screen-ings and education. Through these various screenings, we have identified many cancers and assist-ed with coordinating follow-up treatment for those individuals.
Our research department staff also continues to maintain accruals at twice the national level.Our remarkable accrual rates are a credit to not only our study selection process but also the staff’scommitment to making the process as easy as possible for the patient and physician. I also creditour medical staff who are willing to exert the extra effort to identify potential patients. We expectour clinical trials component to continue to grow and anticipate streamlining the process as muchas possible through computerization.
Hospice of NGMC also had a record year. In addition to celebrating their 20th anniversary inNovember 2006, the Hospice program experienced phenomenal growth in patient days and wassuccessful with increasing non-cancer patients to 52 percent of the total patient base, a direct resultof educating physicians and case managers on appropriate Hospice referrals. Also, the oncologyinpatient unit staff (5 East) was awarded an Oncology Nurse Society (ONS) grant for education onend-of-life care. Two nurses received advanced education on end-of-life issues and, following theirtraining, held a well-received and attended course to educate nurses throughout NGMC.
On a whole, 2006 was a year of advancement and growth for the Cancer Center at NGMC. Asour patient volumes increase, so will our expertise and ability to offer the most advanced carepossible. We expect continued challenges in 2007, but with our commitment to the patient, Iknow we will accomplish our goals in 2007.
Thomas J. Enright, RN, MSN, MBAOncology Service Line Director
16
The boards of Northeast Georgia MedicalCenter and Northeast Georgia HealthSystem congratulate the physicians andstaff of The Cancer Center at NortheastGeorgia Medical Center for their accom-plishment in being granted three-yearaccreditation with commendation fromthe Commission on Cancer (COC) of theAmerican College of Surgeons.
Approval by the COC is given only to thosefacilities that have voluntarily committed toproviding the highest level of cancer careand that undergo a rigorous evaluation andreview of their performance and processes.
Three-year accreditation with commendationis awarded when the program complies
with all COC standards and receives acommendation rating for at least one ormore of the eligible categories of standards.Currently, the COC has eight categories ofstandards, and the Cancer Center atNGMC received commendation in all eightcategories.
We want to express our gratitude to theexperienced physician specialists andhighly trained clinical staff whose hardwork and dedication helped achieve thisrecognition of our comprehensive, multidis-ciplinary cancer care. We’re proud to be apart of an organization that is committed tooffering excellence in cancer care and thelatest in cancer treatment, close to home.
recognized for excellence in cancer care