Embed Size (px)
Citation preview

Cancer in Pregnancy Pregnancy interruption vs. Active treatment
MATERNITA E TUMORI Milan, May 16th – 18th, 2013
Hatem A. Azim Jr., MD, MSc.
Department of Medicine, BrEAST Data Centre
Institut Jules Bordet
Brussels, BE

Berry DL et al; JCO 1999
EPIDEMIOLOGY
1/1.000 pregnancies

Rising Trend of Delaying Childbearing
Mathews T & Hamilton B; NCHC 2009

Pregnancy Interruption .. Why not ?
Customs &Traditions
Precious Child
Religion Too late
Main Themes
Regret
A Woman who interrupted her pregnancy
“It does make me feel, you know, quite bad some days. It does not go”

A Woman who already completed her family and opted to continue her pregnancy
Main Themes
Anxiety & Decision Conflict
“If they said the best option is to have a termination, I think I would have had one . But I knew it would have been really hard but I’ve got other kids, I can’t sort of risk my life”
Pregnancy Interruption .. Why ?
This could improve prognosis of these patients ..
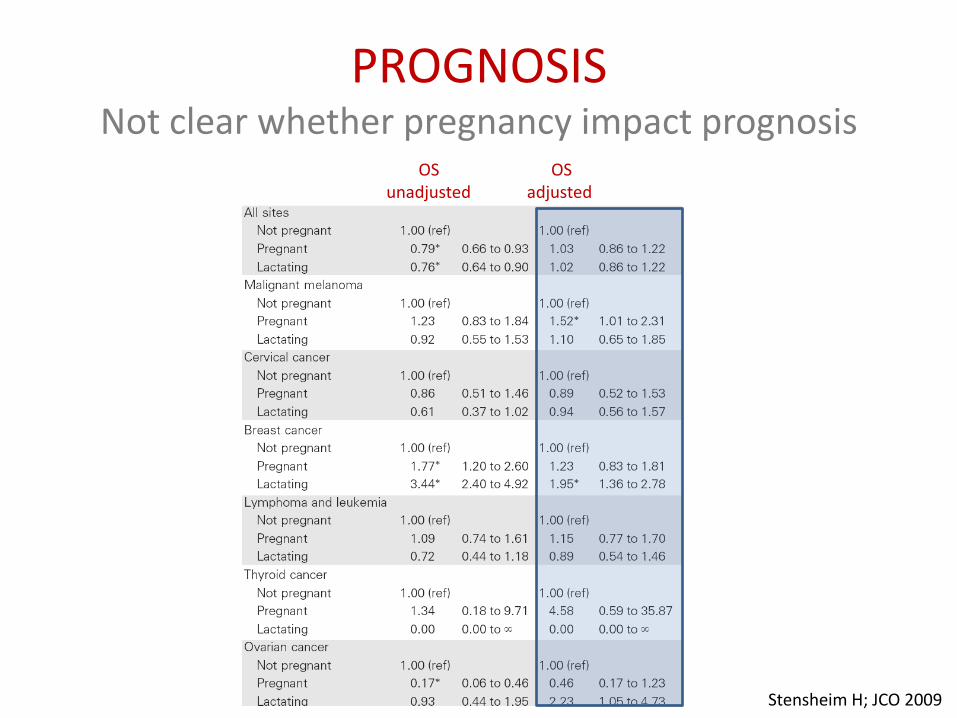
PROGNOSIS Not clear whether pregnancy impact prognosis
Stensheim H; JCO 2009
OS unadjusted
OS adjusted
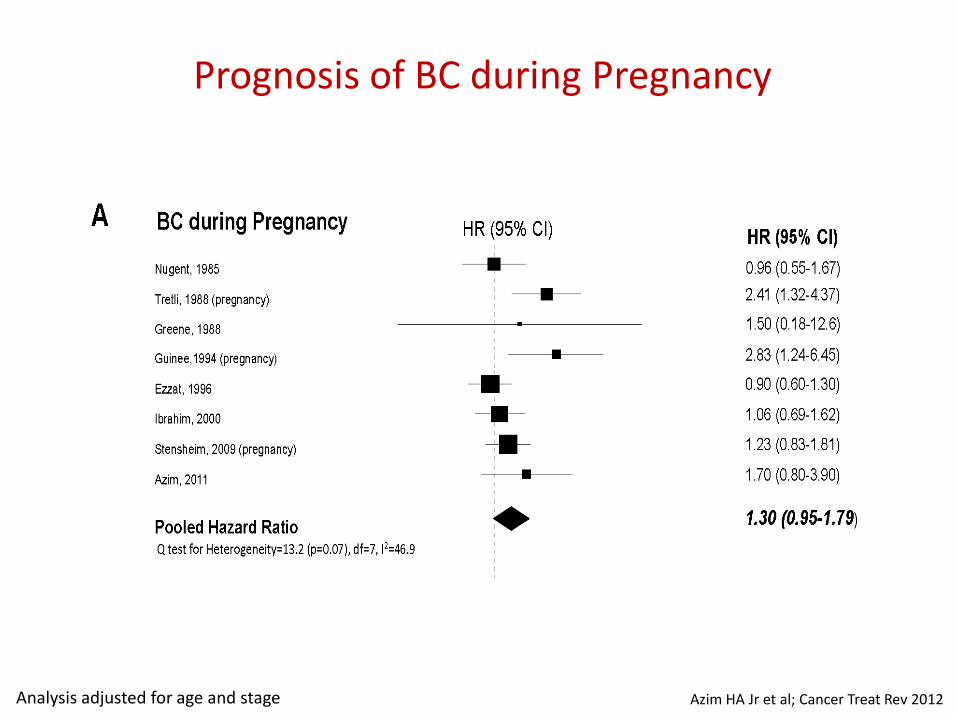
Prognosis of BC during Pregnancy
Analysis adjusted for age and stage Azim HA Jr et al; Cancer Treat Rev 2012
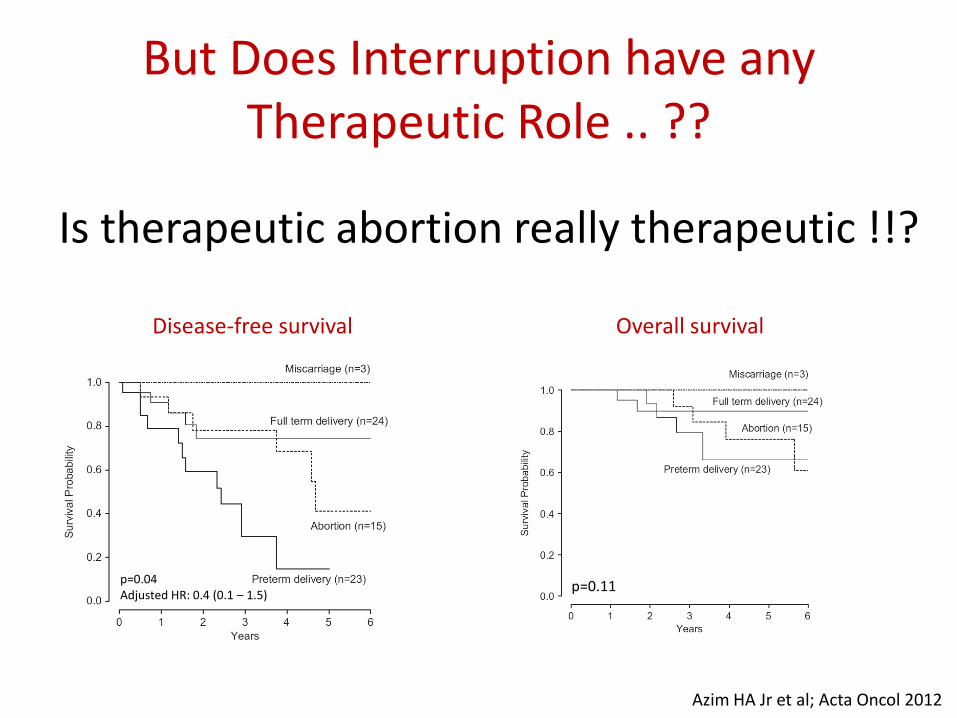
But Does Interruption have any Therapeutic Role .. ??
Is therapeutic abortion really therapeutic !!?
Disease-free survival Overall survival
Azim HA Jr et al; Acta Oncol 2012
p=0.11 p=0.04 Adjusted HR: 0.4 (0.1 – 1.5)

Pregnancy Interruption .. Why ?
This will allow the treating physician to adequately treat the patient
This could improve prognosis of these patients ?

When a drug is administered to the mother, placental transfer of the drug could be hazardous to the fetus
Cardonick E et al; Lancet Oncol 2004
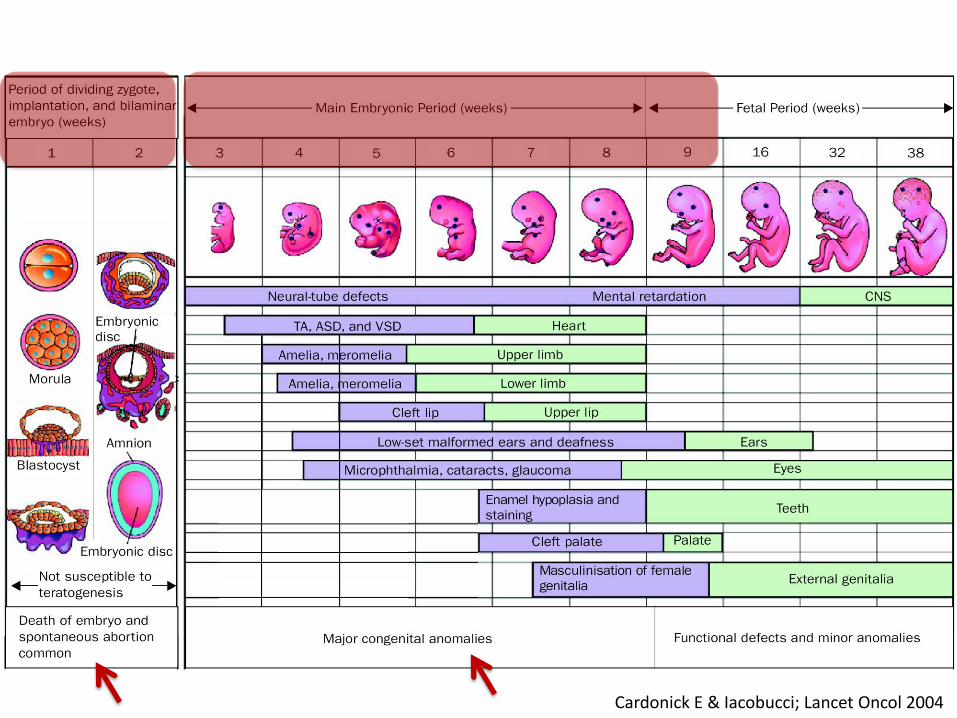
Cardonick E & Iacobucci; Lancet Oncol 2004
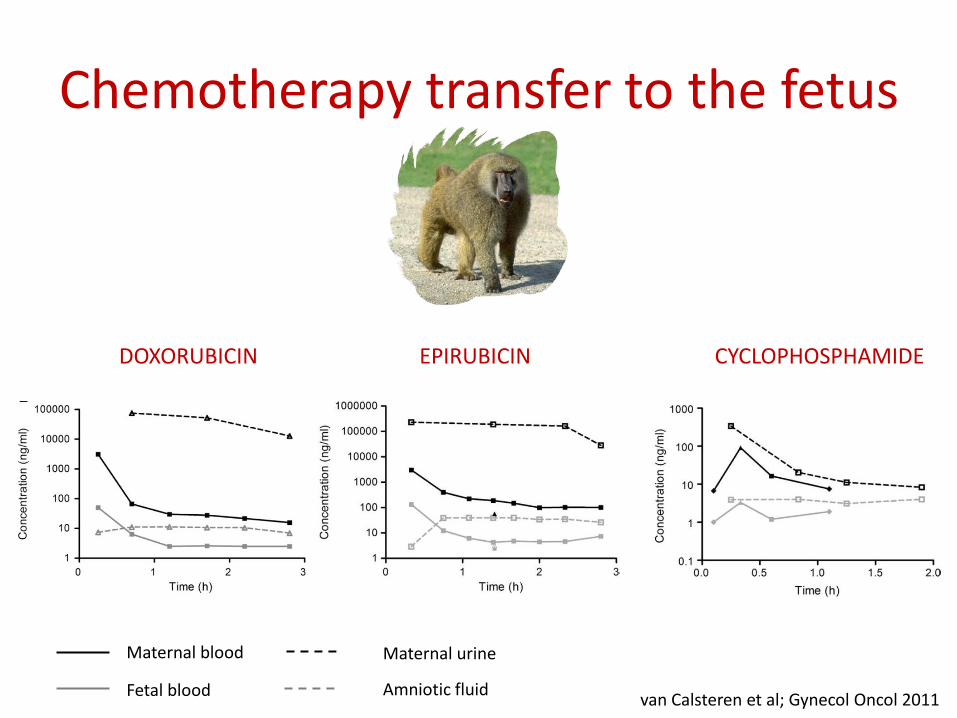
Chemotherapy transfer to the fetus
van Calsteren et al; Gynecol Oncol 2011
Maternal blood Maternal urine
Fetal blood Amniotic fluid
DOXORUBICIN EPIRUBICIN CYCLOPHOSPHAMIDE

van Calsteren et al; Int J Gynecol Oncol 2010 van Calsteren et al; Gynecol Oncol 2011
Number Drug detected in fetus (n) % drug detected in fetus
Doxorubicin 15 6 7.5 ± 3.2
Epirubicin 11 8 4.0 ± 1.6
Paclitaxel 11 7 1.4 ± 0.8
Docetaxel 9 0 0
Cyclophosphamide 4 3 25.1 ± 6.3
Carboplatin 7 7 57.5 ± 14.2
DOXORUBICIN EPIRUBICIN
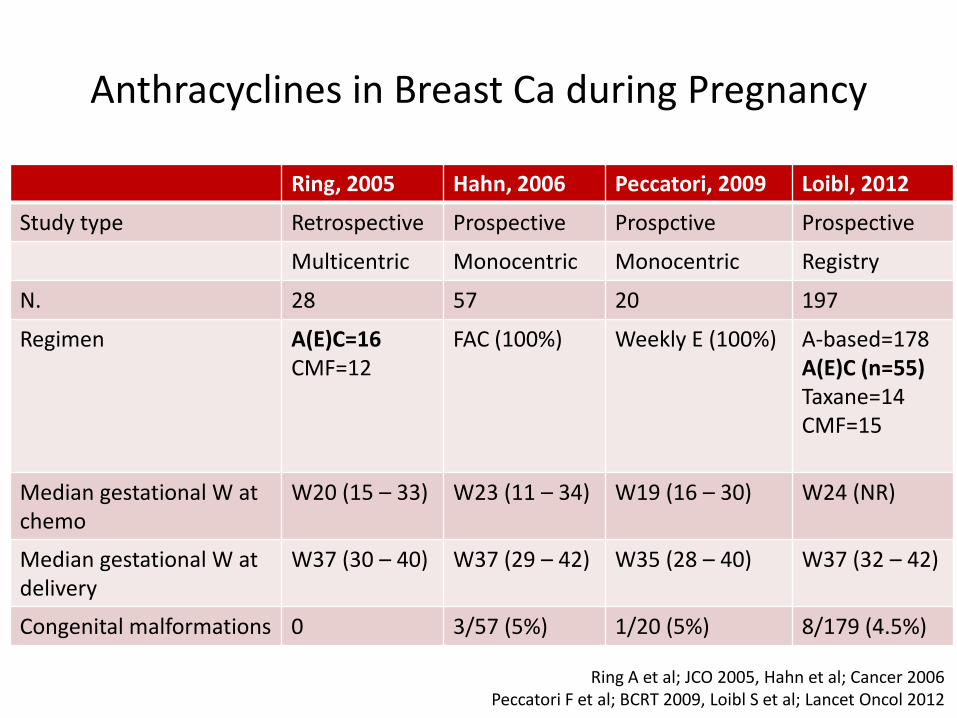
Ring, 2005 Hahn, 2006 Peccatori, 2009 Loibl, 2012
Study type Retrospective Prospective Prospctive Prospective
Multicentric Monocentric Monocentric Registry
N. 28 57 20 197
Regimen A(E)C=16 CMF=12
FAC (100%) Weekly E (100%) A-based=178 A(E)C (n=55) Taxane=14 CMF=15
Median gestational W at chemo
W20 (15 – 33) W23 (11 – 34) W19 (16 – 30) W24 (NR)
Median gestational W at delivery
W37 (30 – 40) W37 (29 – 42) W35 (28 – 40) W37 (32 – 42)
Congenital malformations 0 3/57 (5%) 1/20 (5%) 8/179 (4.5%)
Anthracyclines in Breast Ca during Pregnancy
Ring A et al; JCO 2005, Hahn et al; Cancer 2006 Peccatori F et al; BCRT 2009, Loibl S et al; Lancet Oncol 2012
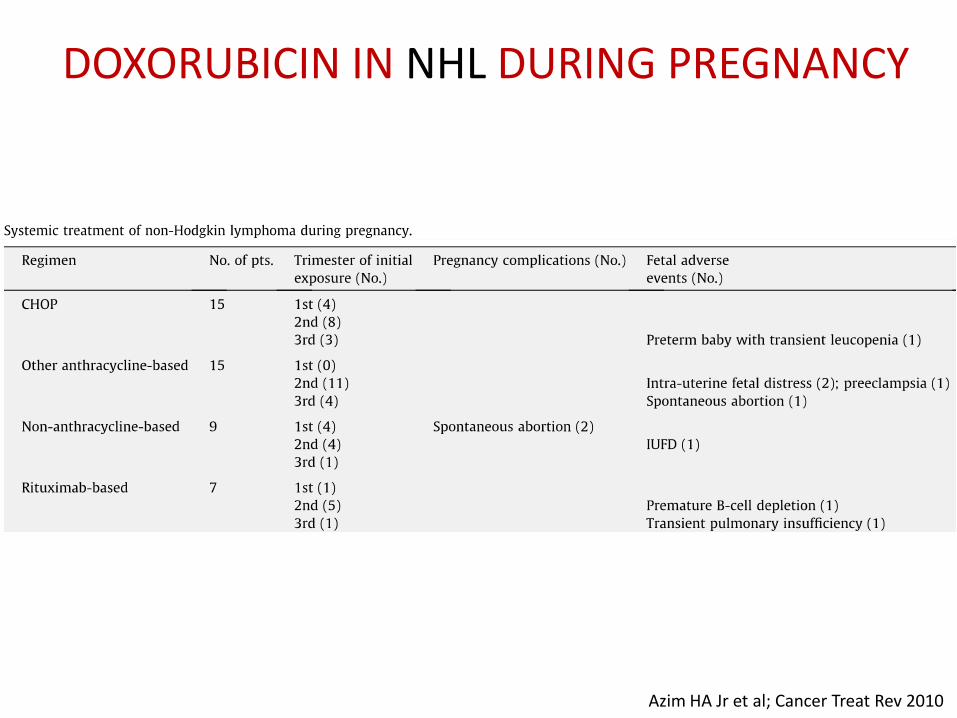
Azim HA Jr et al; Cancer Treat Rev 2010
DOXORUBICIN IN NHL DURING PREGNANCY
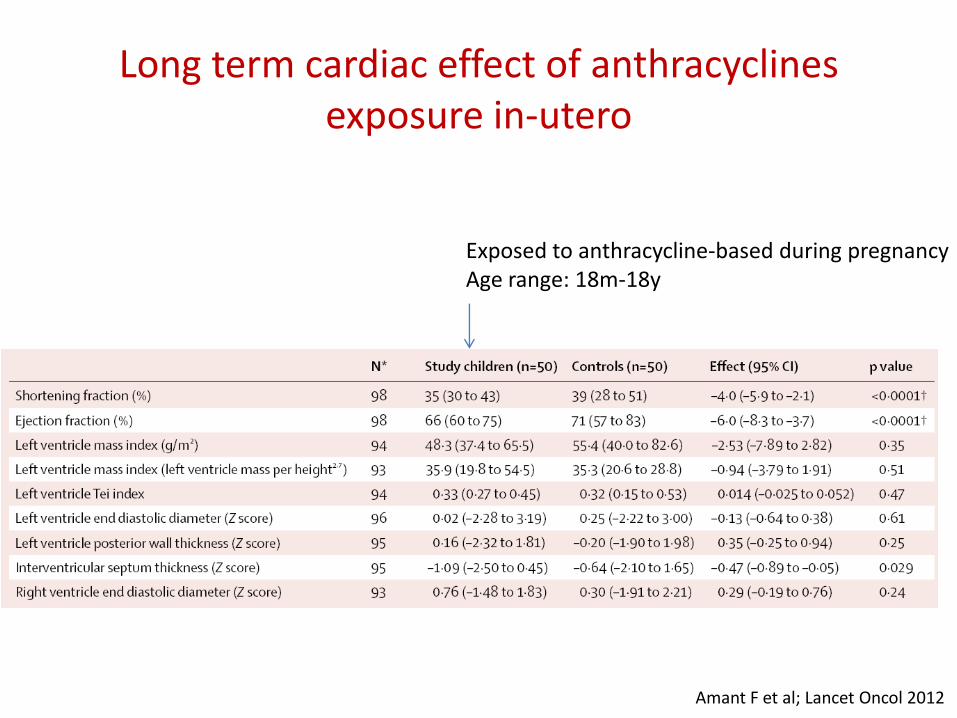
Long term cardiac effect of anthracyclines exposure in-utero
Exposed to anthracycline-based during pregnancy Age range: 18m-18y
Amant F et al; Lancet Oncol 2012
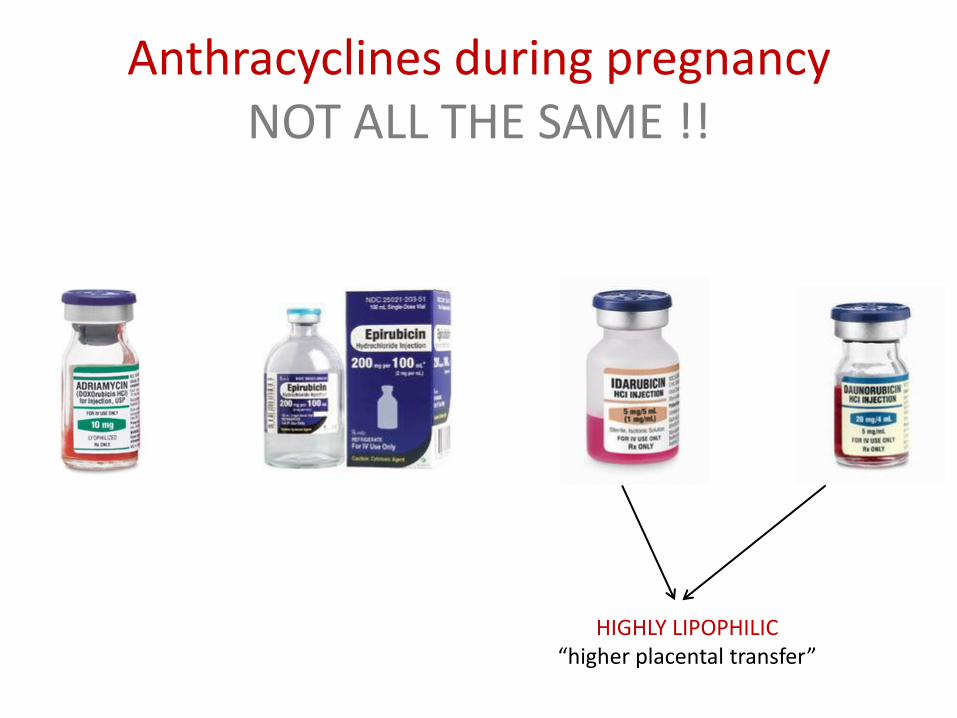
Anthracyclines during pregnancy NOT ALL THE SAME !!
HIGHLY LIPOPHILIC “higher placental transfer”

DAUNORUBICIN
IDARUBICIN
Azim HA Jr et al; Cancer Treat Rev 2010
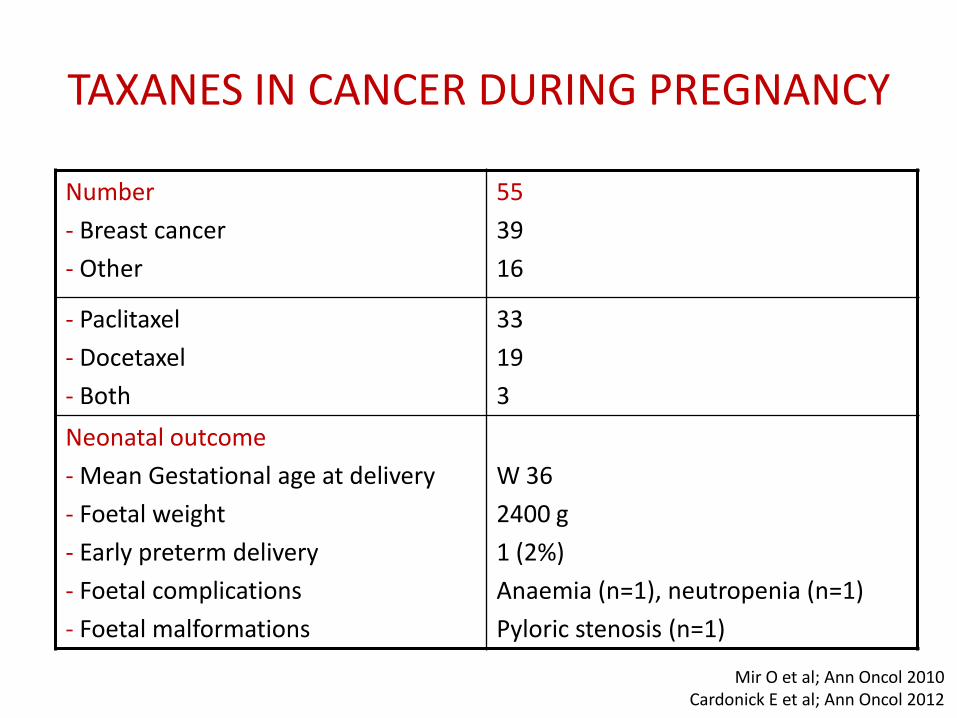
Number
- Breast cancer
- Other
55
39
16
- Paclitaxel
- Docetaxel
- Both
33
19
3
Neonatal outcome
- Mean Gestational age at delivery
- Foetal weight
- Early preterm delivery
- Foetal complications
- Foetal malformations
W 36
2400 g
1 (2%)
Anaemia (n=1), neutropenia (n=1)
Pyloric stenosis (n=1)
TAXANES IN CANCER DURING PREGNANCY
Mir O et al; Ann Oncol 2010 Cardonick E et al; Ann Oncol 2012

Number
- Cisplatin
- Carboplatin
48
47
1
Regimen - Single agent (61.7%)
- Combination with bleomycin, or taxanes (38.3%)
Neonatal outcome
- Mean Gestational age at delivery
- Foetal weight
- Foetal complications
- Foetal malformations
W 33
2200 g
++ creatinin (n=1), intraventricular hge (n=1), hypoglycemia (n=1), hypotension (n=1),hearing loss (n=1)
None
PLATINUM SALTS IN CERVICAL CANCER DURING PREGNANCY
Zagouri F et al; Obstet Gynecol 2013
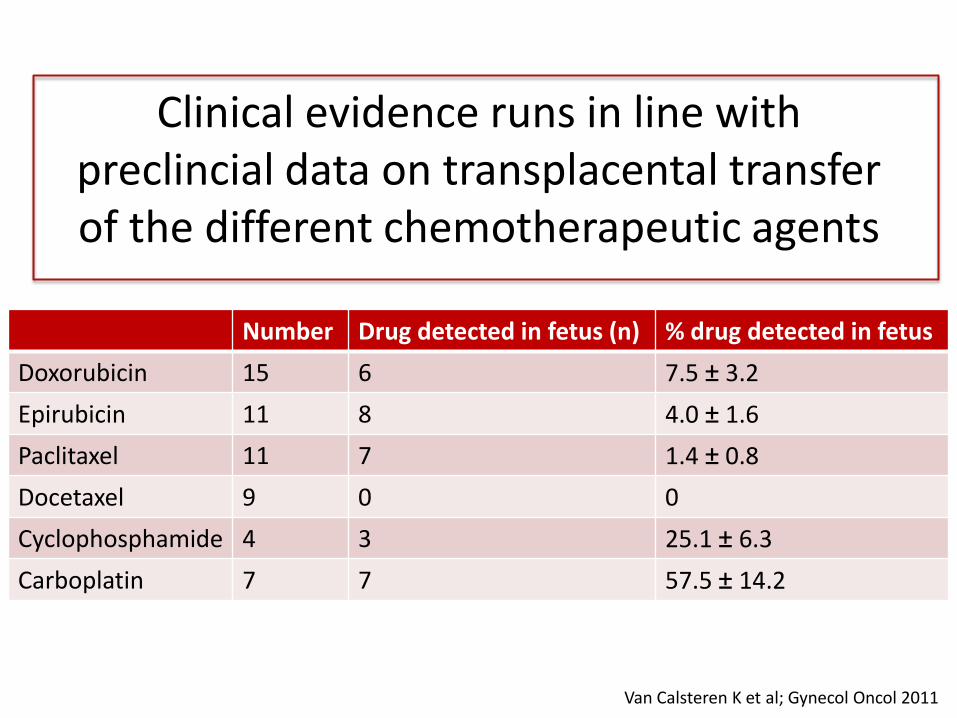
Number Drug detected in fetus (n) % drug detected in fetus
Doxorubicin 15 6 7.5 ± 3.2
Epirubicin 11 8 4.0 ± 1.6
Paclitaxel 11 7 1.4 ± 0.8
Docetaxel 9 0 0
Cyclophosphamide 4 3 25.1 ± 6.3
Carboplatin 7 7 57.5 ± 14.2
Clinical evidence runs in line with preclincial data on transplacental transfer of the different chemotherapeutic agents
Van Calsteren K et al; Gynecol Oncol 2011
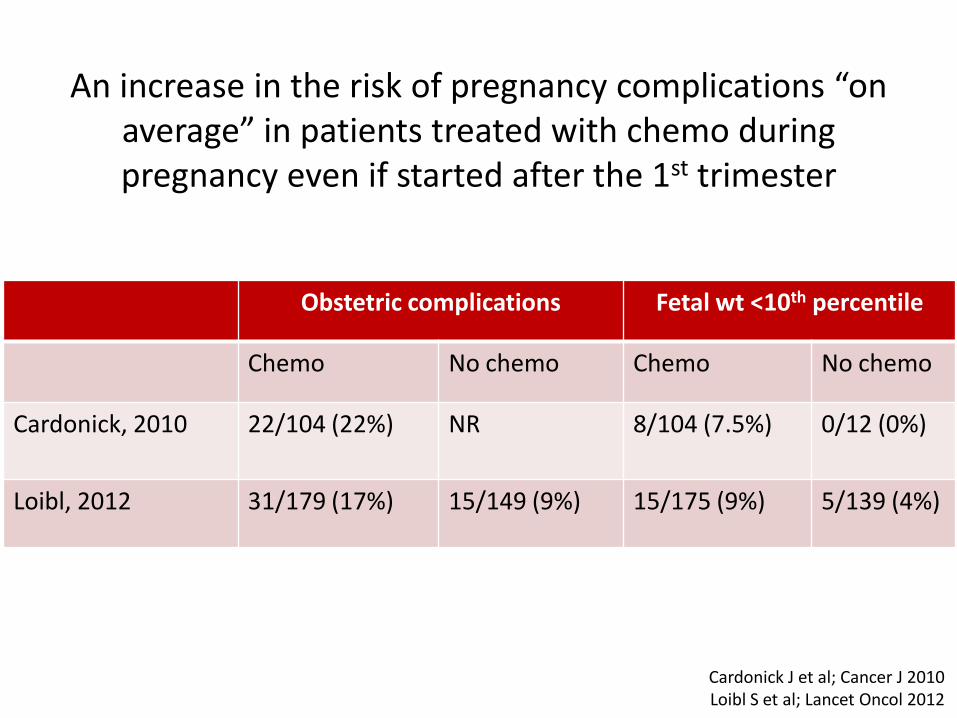
Cardonick J et al; Cancer J 2010 Loibl S et al; Lancet Oncol 2012
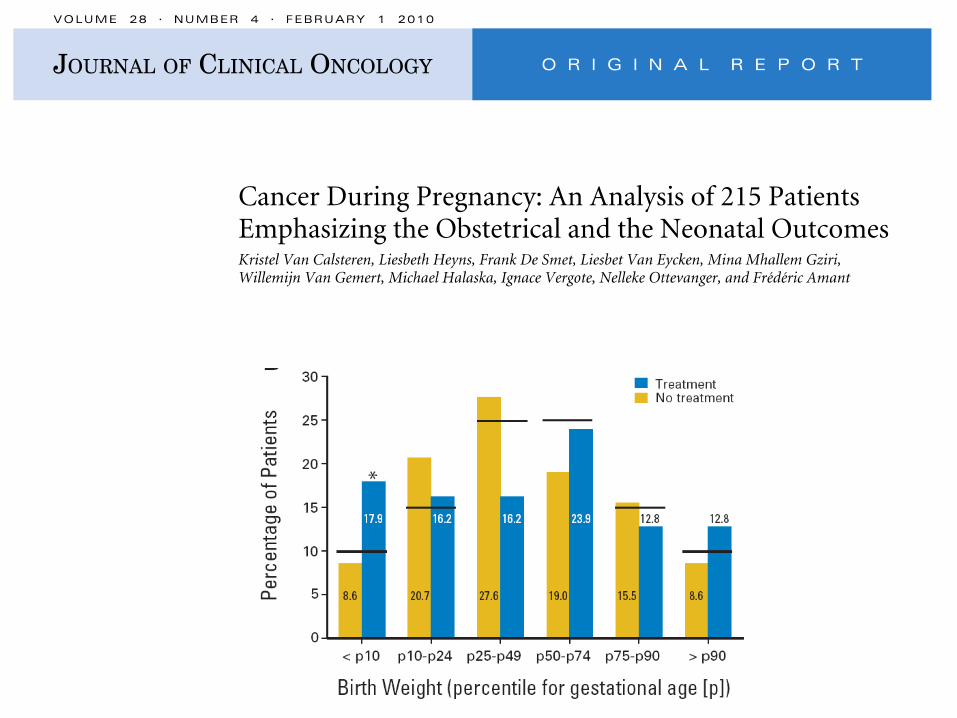
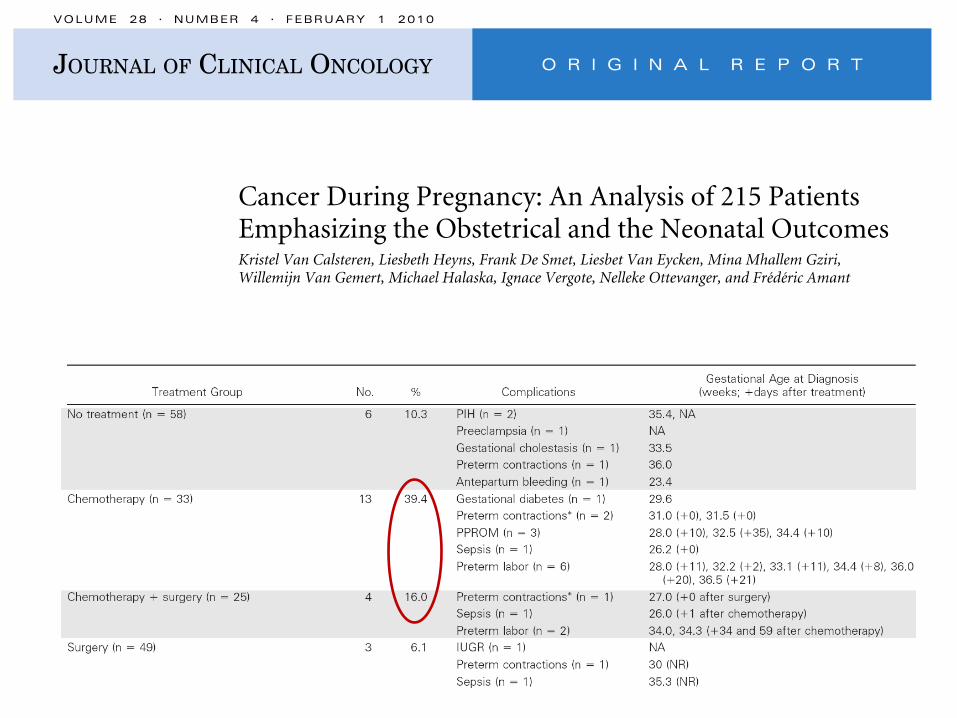
Obstetric complications Fetal wt <10th percentile
Chemo No chemo Chemo No chemo
Cardonick, 2010 22/104 (22%) NR 8/104 (7.5%) 0/12 (0%)
Loibl, 2012 31/179 (17%) 15/149 (9%) 15/175 (9%) 5/139 (4%)
An increase in the risk of pregnancy complications “on average” in patients treated with chemo during pregnancy even if started after the 1st trimester

WEEKLY APPLICATION OF CHEMOTHERAPY Allow close monitoring of pregnancy Low peak plasma concentration resulting in
- Lower toxicity (more safe)
- Possible lower placental transfer & foetal exposure
Easy interruption in case of toxicity

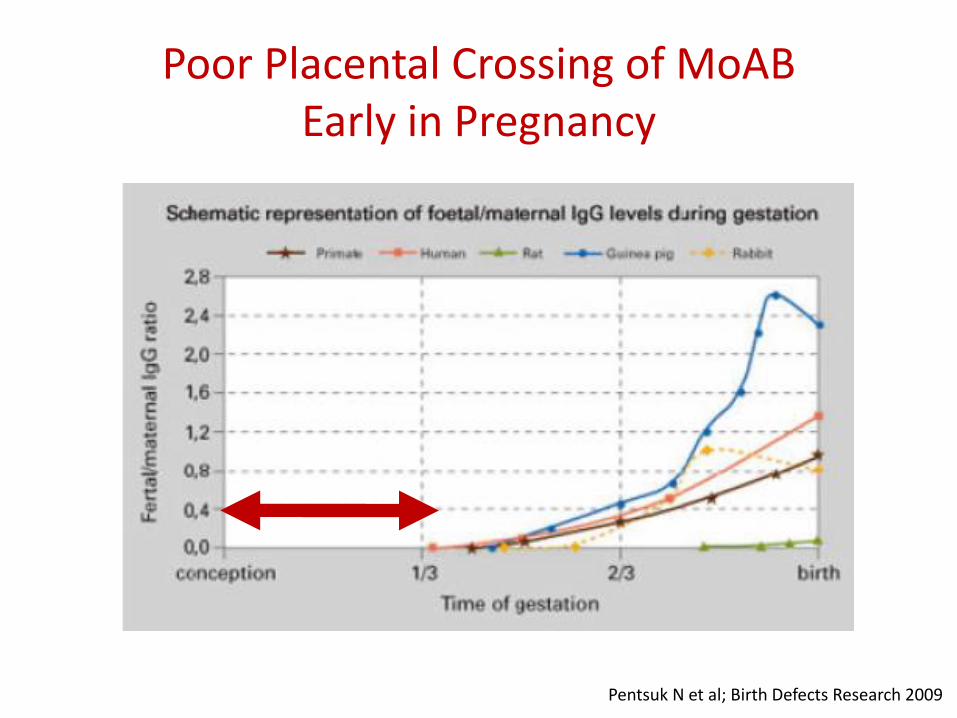
Poor Placental Crossing of MoAB Early in Pregnancy
Pentsuk N et al; Birth Defects Research 2009
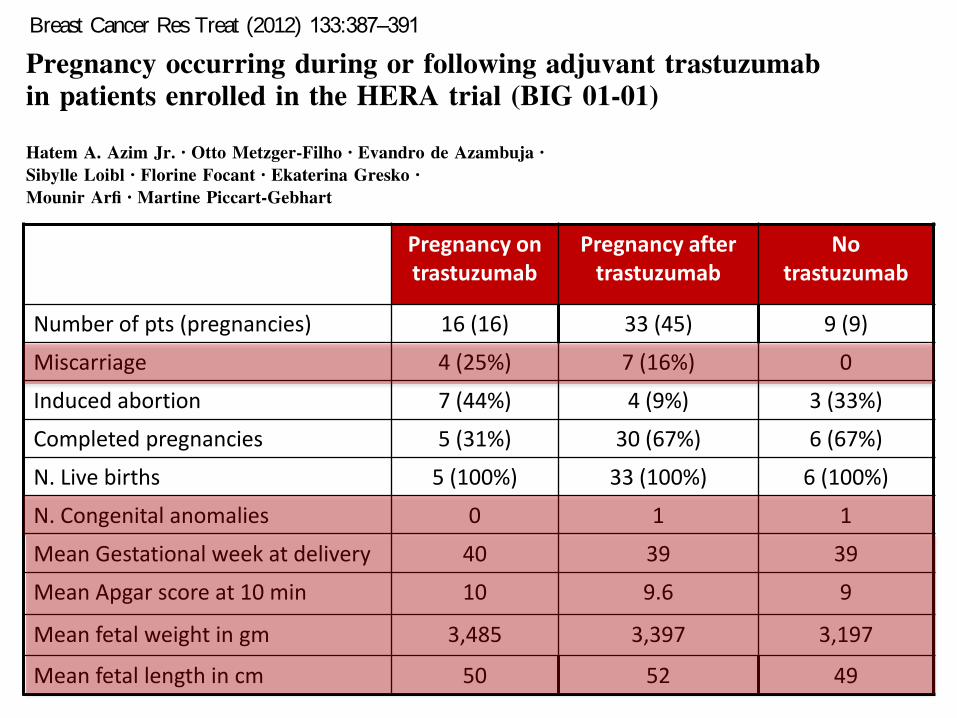
Pregnancy on trastuzumab
Pregnancy after trastuzumab
No trastuzumab
Number of pts (pregnancies) 16 (16) 33 (45) 9 (9)
Miscarriage 4 (25%) 7 (16%) 0
Induced abortion 7 (44%) 4 (9%) 3 (33%)
Completed pregnancies 5 (31%) 30 (67%) 6 (67%)
N. Live births 5 (100%) 33 (100%) 6 (100%)
N. Congenital anomalies 0 1 1
Mean Gestational week at delivery 40 39 39
Mean Apgar score at 10 min 10 9.6 9
Mean fetal weight in gm 3,485 3,397 3,197
Mean fetal length in cm 50 52 49
BRIEF REPORT
Pregnancy occurring during or following adjuvant trastuzumabin patients enrolled in the HERA trial (BIG 01-01)
Hatem A. Azim Jr. • Otto Metzger -Filho • Evandro de Azambuja •
Sibylle Loibl • Florine Focant • Ekaterina Gresko •
Mounir Arfi • Martine Piccart-Gebhart
Received: 9 February 2012/ Accepted: 11 February 2012/ Published online: 26 February 2012
Ó Springer Science+Business Media, LLC. 2012
Abstract Only few case reports describe the pregnancy
course and outcome of breast cancer patients, who were
under treatment with trastuzumab at the timeof conception
or who have completed trastuzumab therapy before
becoming pregnant. The HERA trial is a large phase III
randomized clinical trial in which patients with early
HER2-positive breast cancer were randomized to receive 1
or 2 years of trastuzumab or observation following com-
pletion of primary chemotherapy. To examine the effect of
trastuzumab on pregnancy outcome, we report all preg-
nancy events that occurred until March 2010 in patients
enrolled in the study. For the sake of this analysis, patients
were assigned to three groups: (1) pregnancy occurring
during and up to 3 months after trastuzumab exposure
(group 1); (2) pregnancy occurring [ 3 months of last
trastuzumab dose(group 2); and (3) pregnancy occurring in
patients without prior exposure to trastuzumab (group 3).
Sixteen, 45 and 9 pregnancies took place in groups 1, 2,
and 3, respectively. 25 and 16% of patients in groups1 and
2 experienced spontaneous abortion, the former being
higher than figures reported in the general population.
However, short-term fetal outcomeappeared normal across
the three groups. Only 2 congenital anomalies were
reported, one in group 2 and one in group 3. No congenital
anomalies were reported in those exposed to trastuzumab
in utero. This is the first report from a large randomized
trial assessing the effect of trastuzumab on pregnancy
course and outcome. Based on our results, trastuzumab
does not appear to affect fetal outcome in patients who
manage to complete their pregnancy. We are currently
initiating a collaboration to collect similar data from the
other large adjuvant trastuzumab trials to confirm these
findings.
Keywords Breast cancer Pregnancy Trastuzumab
Counseling Fetal outcome
Introduction
One year of adjuvant trastuzumab is the standard of care
for patients with early HER2-positive breast cancer [1–3].
As trastuzumab is not known to cause amenorrhea [4], and
given the rising trend of delaying pregnancy to later in life
[5], patients with child-bearing potential could become
pregnant during or following trastuzumab exposure.
Unlike chemotherapy, the safety profile of trastuzumab
during pregnancy is not well described and limited to few
published case reports [6–10]. The most striking observa-
tion hasbeen theapparent risk of oligo- and anhydramnios,
which resulted in premature delivery, fetal morbidity, and
This study was conducted on behalf of the HERA study team.
This study was presented as a poster presentation at the 2011 San
Antonio Breast Cancer Symposium.
H. A. Azim Jr. (& ) O. Metzger-Filho E. de Azambuja
F. Focant M. Piccart-Gebhart
Department of Medical Oncology, Institut Jules Bordet and
l’Universite Libre de Bruxelles (ULB), Boulevard de Waterloo
121, 1000 Brussels, Belgium
e-mail: [email protected]
S. Loibl
Department of Medicine and Research, Klinikum Offenbach,
Offenbach, Germany
E. Gresko
F. Hoffmann-La Roche, Basel, Switzerland
M. Arfi
Frontier Science, Kincraig, Kingussie, Scotland, UK
123
Breast Cancer Res Treat (2012) 133:387–391
DOI 10.1007/s10549-012-1996-6
Author's personal copy

Regimen Oligohydramnios Congenital anomalies GW at delivery Fetal complications/death
Waterston 2006 T No No Term No
Berveiller 2008 T No No Elective abortion (ectopic)
…
Azim Jr 2009 T No No W39 No
Goodyer 2009 T No No W39 No
Trastuzumab stopped once pregnancy is discovered
Regimen Oligohydramnios Congenital anomalies GW at delivery Fetal complications/death
Watson 2005 T Yes No W37 No
Shrim 2007 T No No W37 Renal Failure
Witzel 2008 T Yes No W27 (pre-term) Res F. / death
Pant 2008 T Yes No W32 (pre-term) Transient complications
Weber 2008 T Yes No W27 (pre-term) Res F. / death
Warraich 2009 T +tam /LHRH
Yes No W37 Res F. / death
Beale 2009 T + tam Yes No W31 (pre-term) Renal & Respiratory failure / death
Mandrawa 2011 T Yes No W37 No
Trastuzumab continued to 2nd or 3rd trimester along with pregnancy

Trastuzumab & the amniotic fluid
Anhydramnios
o Trastuzumab blocks Her-2 expressed in fetal kidney
o It interferes with VEGF signaling responsible for amniotic fluid production and reabsorption
Sekar R et al: OBY GYN, 2007 Pant S et al: JCO, 2008

Setting Regimen Time Mother Pregnancy Baby
Watson 2005 A T Pre, 1st, 2nd NS Anhydramnios NAD
Fanale 2005 M T+ vinorelbine 3rd NS NS NAD
Bader 2007 M T + paclitaxel 2nd NS Anhydramnios, IUGR Transient Resp F,RF
Shrim 2007 M T Pre, 1st, 2nd -- EF NS Transient RF
Sekar 2007 M T + docetaxel 2nd, 3rd NS Anhydramnios NAD
Witzel 2008 M T Pre, 1st, 2nd, 3rd NS Anhydramnios, vag blee Resp F, died
Pant 2008 M T Pre, 1st, 2nd, 3rd NS Anhydramnios NAD
Weber 2008 M T Pre, 1st, 2nd NS Anhydramnios Resp F, died
Warraich 2009 A T + tam + LHRH Pre, 1st, 2nd , 3rd NS Anhydramnios Res. F, fetal death after 40 minutes
Beale 2009 A T + tam Pre, 1st, 2nd NS Anhydramnios, PROM Twins:
1) RF, Resp F, Death
2) Transient Resp. F
Goodyer 2009 M T 2nd None None Premature
Gottschalk 2011 M T + Carbo + Doc 2nd None Anhydramnios Fetal growth restriction
Azim HA Jr et al; Exp Rev Immunol 2010
High risk of anhydramnios and fetal morbidity/mortality secondary to trastuzumab administration during pregnancy
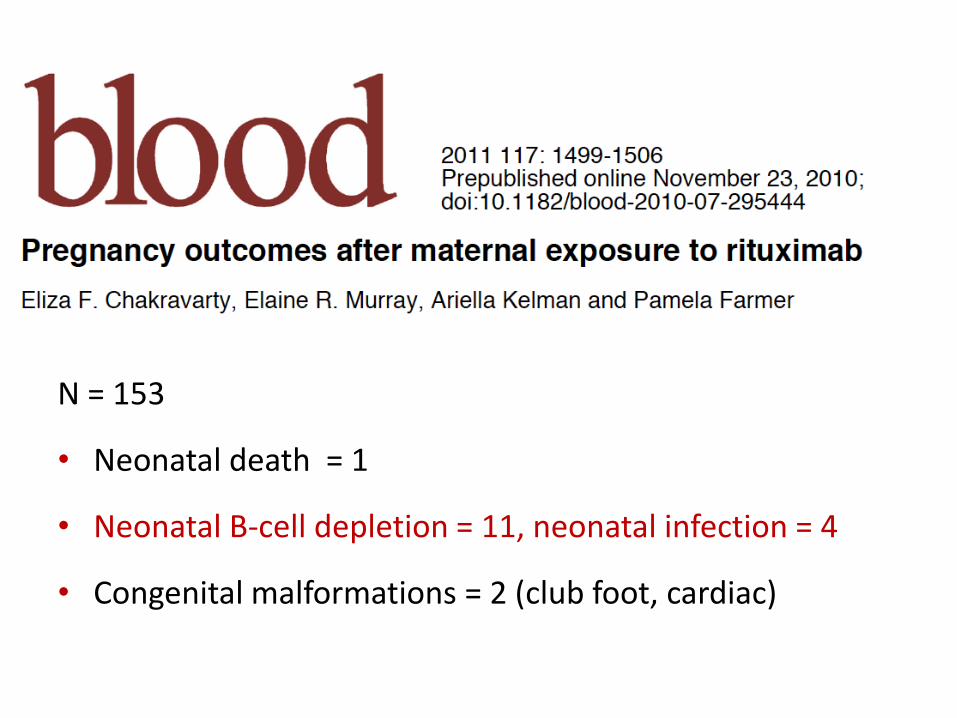
N = 153
• Neonatal death = 1
• Neonatal B-cell depletion = 11, neonatal infection = 4
• Congenital malformations = 2 (club foot, cardiac)

Agent Use during pregnancy
Imatinib Avoid during the first trimester. Possible
starting the second trimester
Lapatinib Only one case report. Avoid during the
whole pregnancy period
Bevacizumab and other VEGF
targeting agents
No clinical data but worrying preclinical
evidence. Avoid during pregnancy
Zoledronic acid Induce anomalies in preclinical models,
could affect uterine contraction secondary
to hypocalcemia. Should be avoided
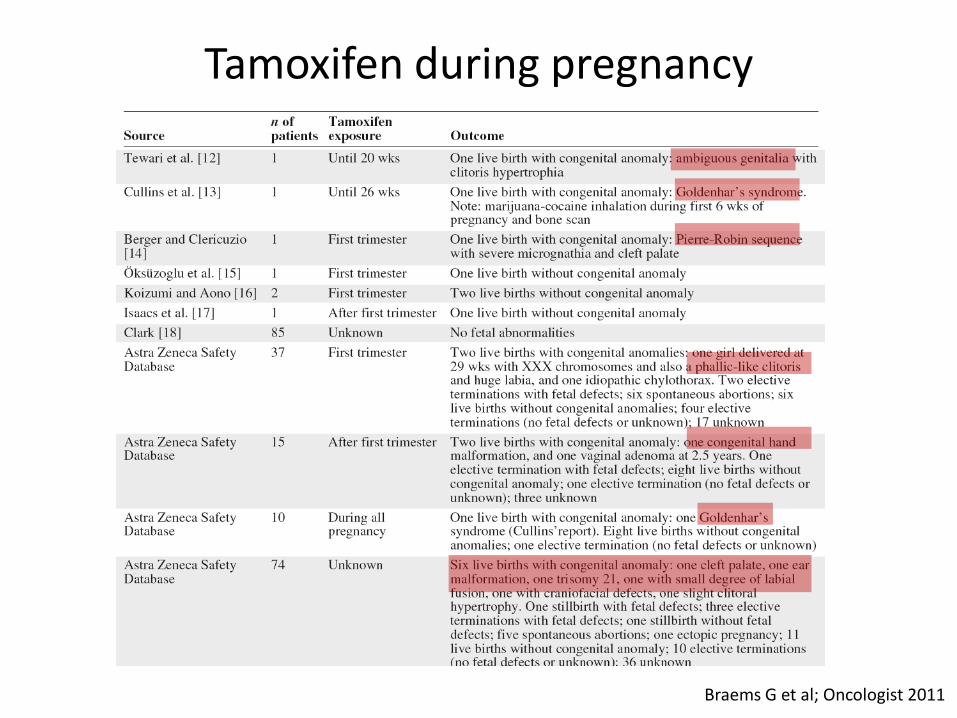
Tamoxifen during pregnancy
Braems G et al; Oncologist 2011
When to consider pregnancy termination ? “Is when you can not balance maternal benefits and fetal risks”
• Delaying standard therapy could seriously affect maternal prognosis (e.g. diagnosis of acute leukemia during 1st trimester)
• Patient is seriously concerned on delaying standard therapy that can not be delivered during pregnancy (e.g. Ca cervix)
MAYBE PRETERM DELIVERY COULD BE THE OPTIMAL SOLUTION ..??

0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
Cerebral palsy Mental retardation
Psycho disorder Disability affecting
working capacity
Full term
W34-W36
W31-W33
Norwegian National Registry ≈1 Million infant
Moster D et al; NEJM 2008
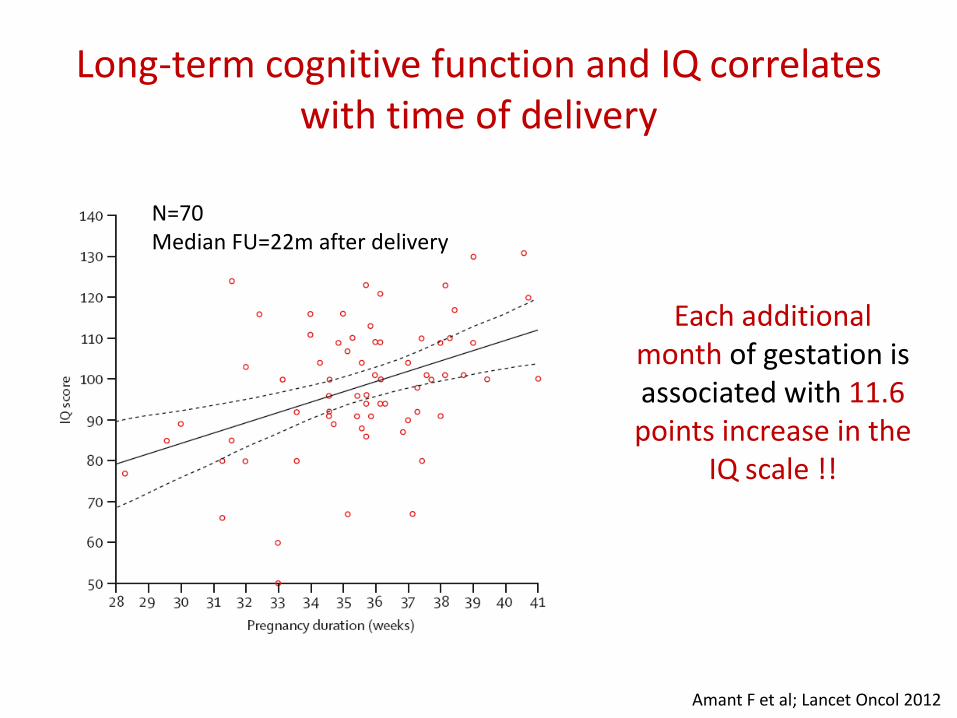
Amant F et al; Lancet Oncol 2012
Long-term cognitive function and IQ correlates with time of delivery
N=70 Median FU=22m after delivery
Each additional month of gestation is associated with 11.6 points increase in the
IQ scale !!

Conclusions
1. Offering active treatment during pregnancy is feasible and could provide adequate disease control with comparable outcomes to the non-pregnant settings

Conclusions
2. Offering standard treatments is sometimes not possible, and hence adapting tailored strategies could be needed. Hence a need to engage centres with expertise in this field
Conclusions
3. Pregnancy terminations offers
– no therapeutic advantages
– Psychological detrimental effect on the patient that can be long-lasting
Should not be routinely offered to patients except in exceptional cases

NEONATOLOGY
PSYCHOLOGY
ONCOLOGY
OBSTETRICS
PAEDIATRICS
Managing BC during pregnancy The need for a multidisciplinary approach

ACKNOWLEDGMENTS
Funding Support
Les Amis de l'Institut Bordet
C. Sotiriou M. Piccart S. Loi V. Jose S. Majjaj S. Michiels C. Desmedt D. Fumagalli M. Ignatiadis E. de Azambuja
F. Peccatori N. Rotmensz G. Pruneri E. Botteri G. Renne G. Viale A. Goldhirsch
N. Pavlidis G. Pentheroudakis





























