Embed Size (px)
Citation preview

Can we prevent Alzheimer’s disease and other memory disorders?
Tiia Ngandu, MD, PhD
Diabetes Prevention Unit, National Institute for Health and Welfare and
Alzheimer’s Disease Research Center,Karolinska Institutet, Sweden

� Memory disorders
� Risk Factors
� Interventions
Prevention of cognitive impairment and Alzheimer’s disease

Dementia / Memory disorders
• Dementia: impaired memory and other cognitivefunctions, disability
• Causes:
– Alzheimer’s disease 60-70 %
– Vascular cognitive impairment 15 %
– Lewy Body Disease 15 %
– Others 5 %
• Memory disorders

Occurrence of dementia
• Prevalence increases with age
65-69 years 1.5%
>85 years 35%
>95 years up to 60%
• 35.6 million people with dementia in 2010
�115.4 million in 2050
�2/3 in low and middle income countries
(World Alzheimer Report 2009)

Burden of dementia
• Patient
• Informal care (family)
• Medical care
• Social care (residential or nursing homes)
• Estimated total costs of 604 billion USD in 2010
(1% of world’s gross domestic product)(World Alzheimer Report 2010)

Prevention of AD: postponing the onset of the disease
US
pre
va
len
ce
of
AD
(m
illio
ns)
US
pre
va
len
ce
of
AD
(m
illio
ns)
DelayDelay(years)(years)
00
.5.5
11
22
55
1997199720072007
2017201720272027
2037203720472047
YearYear
88
66
44
22
00
Brookmeyer et al., 1998, Jorm 2005

40 50 60 70 80
Asymptomatic Preclinical Clinical
phase phase phase
Onset of MCI* Clinical diagnosis of AD
0
25
50
75
100
% o
f end-s
tage
AD
Age (years)
Estimated start of neuropathological changes
Modified from PJ Visser, 2000*MCI - mild cognitive impairment
Managing Alzheimer’s Disease –A Lifelong Commitment

FINRISK
� The FINRISK Study, North Karelia Project
� Aim: Integrate memory disorders into the existing framework

Risk and protective factors for dementia/AD
• Cerebrovascular disorders
• Hypertension
• Hypercholesterolemia
• Obesity
• Diabetes mellitus
• Homocysteine
• Smoking
• Depression
• Head trauma
• High education
• Physical activity
• Active lifestyle
• Moderate alcohol intake
• Antioxidants
• Fish oils
• Coffee
• Antihypertensives
• Statins
• NSAIDs?
• Estrogen?
Risk factors Protective factors

FACTOR DISEASE
Risk relationship
Reverse causality
What goes around comes around
i.e. Cholesterol, Blood pressure, BMI…
CAIDE, Solomon A et al. Neurology 2007, Neurobiol Aging 2009
Honolulu Asia Aging Study, Stewart R et al. Arch Neurol 2007
Kungsholmen Project, Qiu C et al. Stroke 2004
Gothenburg Study, Skoog I et al. Lancet 1996, Gustafson D et al. Neurology 2009
Life-course perspective is needed when assessing the risk factors for AD

0 1 2 3 4 5 6 7 8
IV
III
II
I
IV
III
II
I
I
II
III
IV
I
II
III
IV
Active
Sedentary
Active
Sedentary
Non-drinkers
Infrequent
Frequent
Non-drinkers
Infrequent
Frequent
Non-smokers
Smokers
Non-smokers
Smokers
ORs for
dementia
Physical activity
PUFA intake-quartiles
SFA intake - quartiles
Alcoholdrinking
Smoking
5.5 **
4 *
5 *
7.1 **
7.1 *
3.8 *
3.2 *
APOE ε4 non-carriers
APOE ε4 carriers
Kivipelto et al., JCMM 2008
ApoE4 Magnifies Lifestyle Risk for Dementia

Midlife leisure time physicalactivity and dementia/AD
Dementia AD
OR
(95% CI)
0.47
(0.25-0.90)
0.35
(0.16-0.80)
Total brainvolume
Grey mattervolume
White mattervolume
β-
coefficient
0.21 (p<0.001)
β 0.29 (p<0.001)
β 0.15 (p<0.001)
Rovio, et al., Lancet Neurology 2005
Rovio, et al. Neurobiol Aging 2009
Brain derived neurotrophicfactor (BDNF): a marker of cognitive functioning? Komulainen,et al., 2008
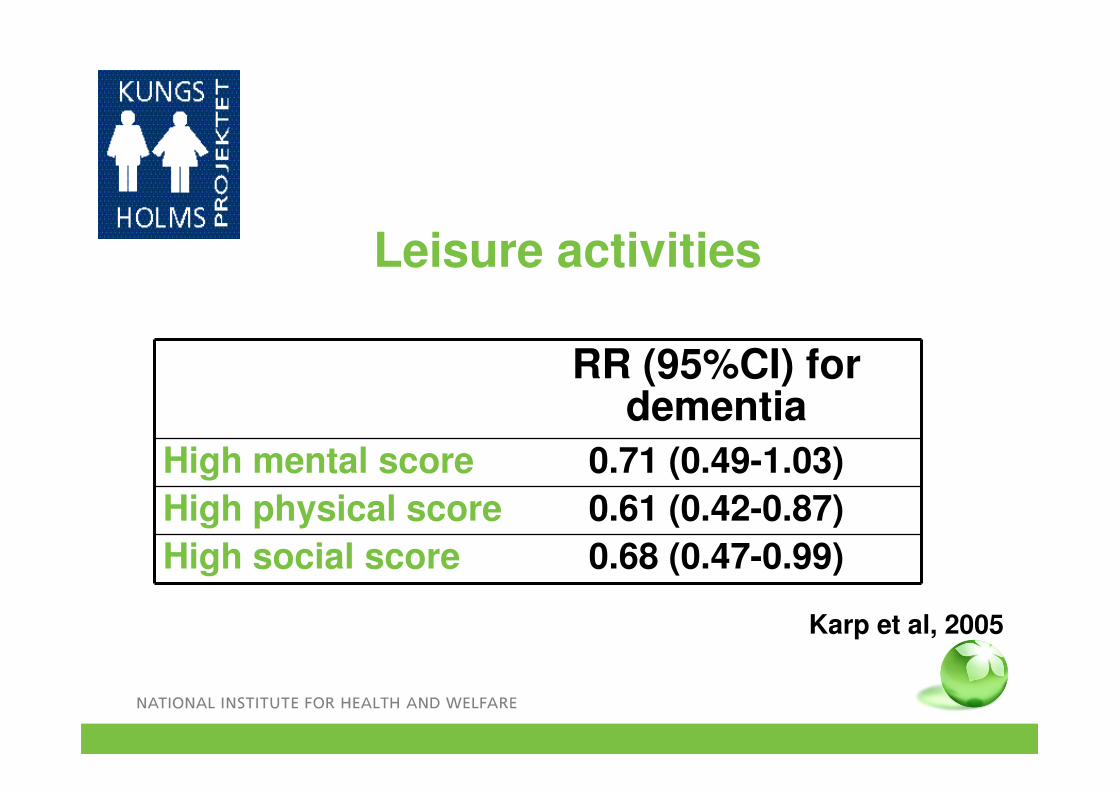
Leisure activities
RR (95%CI) for dementia
High mental score 0.71 (0.49-1.03)
High physical score 0.61 (0.42-0.87)
High social score 0.68 (0.47-0.99)
Karp et al, 2005

0
1
2
3
4
5
6
Ref MCI AD Dementia
The risks of unmarried life…
OR (95% CI) for MCI, AD and dementia in persons without partner at midlife
Controlled for age, sex, education, APOE ε4, BP,
cholesterol, BMI, occupation, occupational physical activity
Håkanson K et al., BMJ 2009

Dementia Risk ScoreAge < 47 years
47-53 years> 53 years
034
Formal education ≥10 years7-9 years0-6 years
023
Sex WomenMen
01
Systolic BP < 140 mm Hg> 140 mm Hg
02
BMI < 30 kg/m2> 30 kg/m2
02
Total cholesterol ≤ 6.5 mmol/l> 6.5 mmol/l
02
Physical activity ActiveInactive
01
Kivipelto, Ngandu et al., Lancet Neurol 2006
Cardiovascular Risk Factors, Aging and Incidence of Dementia

Probability of dementia according to the risk score category
SCORE Risk
0-5 1.0 %1.0 %
6-7 1.9 %1.9 %
8-9 4.2 %4.2 %
10-11 7.4 %7.4 %
12-15 16.4 %16.4 %
Kivipelto, Ngandu et al. Lancet Neurology 2006

Kivipelto, Ngandu et al., Lancet Neurology 2006
Midlife risk profile, 20 years prediction
0
2
4
6
8
10
12
14
16
18
0-5 6-7 8-9 10-11 12-15
SCORE
CAIDE Dementia Risk ScoreCAIDE Dementia Risk Score
Age, years < 4747-53>53
034
Education, years
≥107-90-6
023
Sex WomenMen
01
Systolic BP, mmHg
<140> 140
02
BMI, kg/m2 < 30> 30
02
Cholesterol, mmol/l
≤ 6.5> 6.5
02
Physical activity
ActiveInactive
01
16 %

Randomized controlled trials

SUMMARY OF EARLIER RCT’S
NsCochrane review 2008Cholinesterase inhibitorsMemantine
INTERVENTION STUDIES FINDINGS
Antihypertensives SCOPE, SHEP, Syst-Eur, PROGRESS
Ns, except protective in 1 follow-up study, and 1 study with history of vascular disease
Statins Heart Protection Study, PROSPER
Ns
Estrogen, Estrogen+ProgestinRaloxifeneDHEA
Schumaker JAMA 2003, 2004Cohcrane review 2002
Increased risk/ Ns
NsNs

SUMMARY OF EARLIER RCT’S
Social engagementDiet
Increased riskNs
ADAPT 2009Price 2008
NSAID’sAspirin
Small positive effect
Lautenschlager 2008Dr’s Extra
Physical activity
NsNsNsNsNsNsNs
DeKosky JAMA 2008MAVIS 2007Petersen NEJM 2005Kang 2008McMahon 2006
Ginkgo bilobaMultivitaminsVitamin EVitamin B and folateVitamin CBeta caroteneOmega-3 fatty acids
INTERVENTION STUDY FINDINGS
Cognitive training ACTIVE Positive effect on targeted function

� Timing; starting earlier may lead to better effects
� Target group; a healthy, ’too young’ population will require very long follow-up times and large sample sizes
� Outcome measures; cognitive impairment may be a better measure than conversion to dementia
� Ethical issues; placebo-controlled trials regarding pharmacological treatment of cardiovascular disease risk factors are not possible
‘Recipe’ for prevention trials?

22
Alcoholmisuse
AD is a multi-factorial disease:target several risk factors simultaneously
for an optimal preventive effect
Neuronal damage
Brain reserve
APOE,Other genes
DEMENTIA
Physicalactivity
RISK FACTORS
?
0 20 60 75
Adult life Mid-life Late-life
Unhealthydiet
Transition
Cognitive andsocial activity
Education
PROTECTIVE FACTORS
Smoking
Hypertension
DyslipidemiaObesity
Vascular insultsDiabetes

� Objective: To reduce cognitive impairment in an at risk population through a 2-year multi-domain life-style intervention
� Target population: 60-77 year old persons (n= 1200) from previous population-based non-intervention studies (FINRISK, D2D)
� Time schedule: Screening began in September 2009 and was completed in 2011. The intervention will be completed in the beginning of 2014
Finnish Geriatric Intervention Study to PreventCognitive Impairment and Disability

24
� Study design: A multi-center (6 sites) single-blind RCT enrolling 1200 persons randomized into 2 groups (multi-domain intervention or regular health advice) for a 2-year period. Extended follow-up to 7 years.
� Multidomain intervention:
i) nutritional guidance
ii) increased physical activity
iii) cognitive training and
iv) intensive monitoring and management of vascular risk factors
� Primary outcome: Cognitive impairment

INCLUSION CRITERIA: persons at risk of dementia/ cognitive decline
Dementia Risk score > 6
Based on risk factors assessed in earlier population surveys: Age, Education, Sex, SBP, Cholesterol, BMI, Physical Activity (Kivipelto et al., Lancet Neurology 2006)
AND
Cognitive performance at the mean level or slightly lower than expected for age
CERAD:
1) Word List Immediate Memory task (10 words x3) < 19 words AND/OR
2) Word List Delayed Recall < 75% AND/OR
3) MMSE < 26
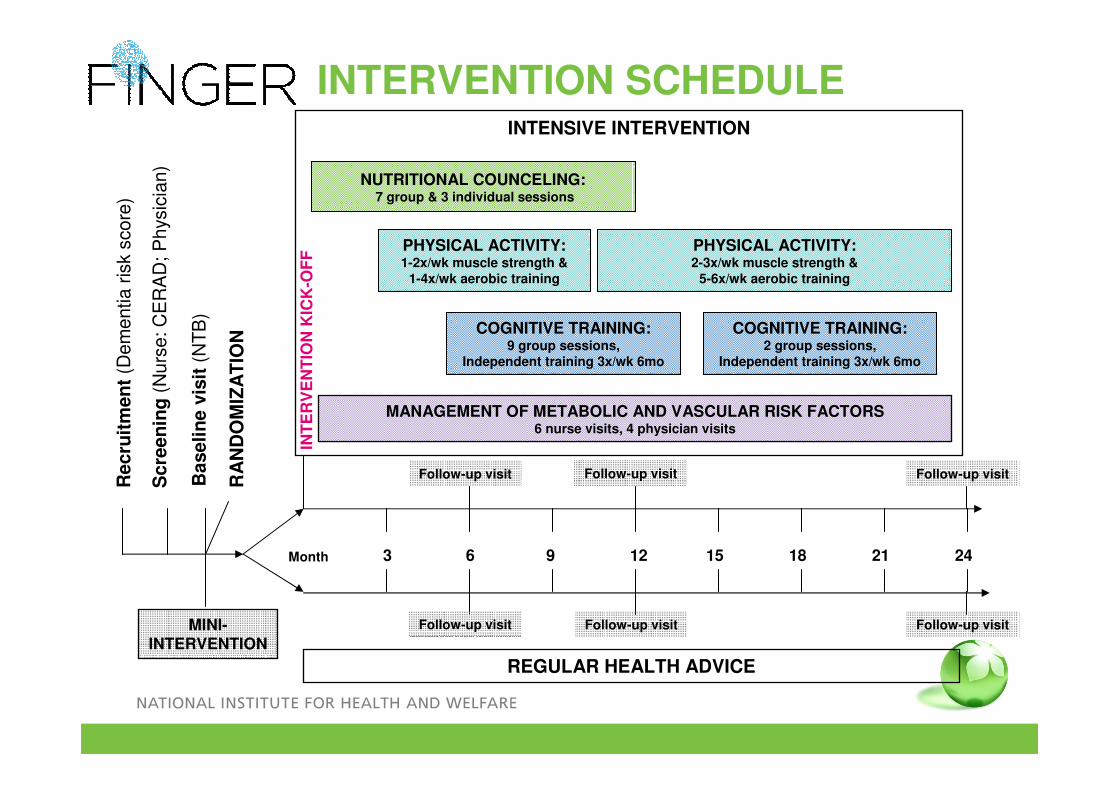
Recru
itm
en
t(D
em
entia r
isk
score
)
Scre
en
ing
(Nurs
e: C
ER
AD
; P
hysic
ian)
Baselin
e v
isit
(N
TB
)
RA
ND
OM
IZA
TIO
N
INTENSIVE INTERVENTION
REGULAR HEALTH ADVICE
INT
ER
VE
NT
ION
KIC
K-O
FF
MINI-INTERVENTION
3 6 9 12 15 18 21 24
Follow-up visit
NUTRITIONAL COUNCELING:7 group & 3 individual sessions
COGNITIVE TRAINING:9 group sessions,
Independent training 3x/wk 6mo
PHYSICAL ACTIVITY:1-2x/wk muscle strength &
1-4x/wk aerobic training
PHYSICAL ACTIVITY:2-3x/wk muscle strength &
5-6x/wk aerobic training
MANAGEMENT OF METABOLIC AND VASCULAR RISK FACTORS6 nurse visits, 4 physician visits
Month
COGNITIVE TRAINING:2 group sessions,
Independent training 3x/wk 6mo
Follow-up visit Follow-up visit Follow-up visit
Follow-up visit Follow-up visit
INTERVENTION SCHEDULE

�Primary:
�Cognitive impairment (Neuropsychological Test Battery, Trail Making & Stroop tests)
�Secondary:
�Dementia (after 7 years)
�Depressive symptoms (Zung scale)
�Vascular risk factors, morbidity and mortality
�Disability (questionnaire, ADL + IADL)
�Quality of life (RAND-36, 15D)
�Utilization of health resources
�Blood markers (i.e. inflammation, redox status, lipid and glucose metabolism, NMR metabonomics)
�Brain MRI measures (n=100) and PET (n=90)
OUTCOMES
RELEVANCE OF A MULTI-DOMAIN INTERVENTION
� Will test to what extent a multi-domain intervention may delay cognitive impairment and dementia onset in people at an increased risk
� Is an innovative approach to delay cognitive impairment while simultaneously intervening upon several risk factors of other major diseases
� Will provide data urgently needed for health education and community planning

European Dementia Prevention Initiative
• FINGER Finnish Geriatric Intervention Study to Prevent
Cognitive Impairment and Disability
• preDIVA Prevention of Dementia by Intensive Vascular Care
• MAPT Multidomain Alzheimer Preventive Trial
EDPI

0
A 10–25% reduction in all seven risk factors could potentially prevent 1.1–3.0 million AD cases worldwide.
July 2011

CONCLUSIONS
Can we prevent/delay memory disorders?
Vascular Vascular
factors: factors: HypertensionHypertension
DiabetesDiabetes
ObesityObesity
• Starting from middle age• Special focus on ApoE
e4 carriers
•Social integration•Physical activities•Mental activities
Be active Be active
and maintainand maintain
an active lifean active life

32
Miia KivipeltoTiina LaatikainenMarkku PeltonenAntti JulaJaana LindströmSatu PajalaSatu AhtiluotoJenni LehtisaloLiisa SaarikoskiPirjo SaastamoinenMarko GrönholmEsko LevälahtiPäivi Valve
Hilkka SoininenTuula Pirttilä †Rainer RauramaaRaimo SulkavaAlina SolomonTuomo HänninenTeemu Paajanen
Timo StrandbergRiitta Antikainen
AcknowledgementsGrant support: Academy of Finland, La Carita Foundation, American Alzheimer Association, Novo Nordisk Fonden, Alzheimer’s Research and Prevention Foundation, The Social InsuranceInstitution of Finland, Juho Vainio Foundation
Jaakko Tuomilehto
Lars Bäckman
Anna Stigsdotter Neely
Turku PET Centre Juha Rinne





























