Embed Size (px)
Citation preview


Can neurobiological treatments replace psychotherapy in the near future? Evalua8ng the efficacy and the benefits of Decoded-Neurofeedback as opposed
to Cogn8ve Behavioural Therapy in treatment of specific phobias.
Neurobiology and psychotherapy: an emerging dialogue
With the emergence and rapid advancement of neuroscience psychologists have come to know that all human feelings and behaviours have their origins in the brain. Nowadays, it appears that neurobiology is star8ng to influence the field of psychology, and especially, the exis8ng ideas about the treatment of mental disorders. With the newly found evidence from neuroscien8fic research, psychotherapy can appear outdated and no longer useful. Are we living in the 8me when neuroscience will overtake the field of psychology as we know it and will eradicate the psychotherapeu8c treatment? The answer to this ques8on remains dubious. This paper is concerned with finding valid evidence that would help to find a resolu8on of the debate. Due to the 8me restric8ons, the project will focus on one disorder and will evaluate a psychotherapeu8c approach and a neurological technique which are both used in treatment of this disorder. Specific phobias have been thoroughly researched and have a number of well-established trea8ng techniques such as Cogn8ve Behavioural Therapy. As for the neuroscien8fic treatment, this paper will discuss Decoded- Neurofeedback as it is one of the rela8vely well researched tools which is also currently being u8lised in treatment of mild disorders.
PHOBIAS
The term phobia in the context of mental illness refers to fear of an object, place, situa8on, feeling, ac8vity or animal. ‘All phobias are anxiety disorders so share symptoms with post-trauma8c stress 1
disorder, panic disorder and others. All anxiety disorders are, fundamentally, based on fear.’ All 2
these disorders share some symptoms with phobic disorders and oPen occur in pa8ents alongside their phobia, before or aPer they started dealing with it. Anxiety linked to phobias can not only be triggered by a physical presence of an object or situa8on but also by a recurring thought of the object or situa8on. The distress that an individual with a phobic disorder experiences, oPen forces him/her to deliberately avoid the object or the situa8on that causes fear. Such behaviour can interfere with the individual’s everyday life, affec8ng social image and personal mental wellbeing. Adults tend to acknowledge the irra8onality of the fear, yet are powerless to resist it.
There are different types of specific phobias:
- Animal phobias: Fear of dogs, snakes, insects, mice etc. Animal phobias is the most common type
- Situa8onal phobias: Fear of specific situa8ons e.g. flying, riding in a car, driving, going over bridges, being in a closed-in place, e.g. an elevator.
‘Phobias’, NHS choices, 2016, hXp://www.nhs.uk/condi8ons/phobias/pages/introduc8on.aspx [accessed 29 1
November 2016].
Lea Winerman, ‘Figuring out phobia. Researchers are using neuroimaging techniques to delve into the 2
neurobiological underpinnings of phobias, with a view to improving treatments.’, American Psychological Associa:on, 2005, Vol 36, No. 7, Print version p.96, available from hXp://www.apa.org/monitor/julaug05/figuring.aspx, [accessed 18 November 2016].

- Natural environment phobias: Fear of storms, heights, water etc
- Blood-injec8on-injury phobias: Fear of being injured, seeing blood, invasive medical procedures.
- Other phobias: fear of falling, a fear of loud sound, fear of characters e.g. clowns.
A person can have more than one specific phobia.
Physical symptoms:
- Trembling
- Difficulty breathing
- A choking sensa8on
- Nausea
- Headache
- Ringing in the ears
- Dizziness
- Confusion or disorienta8on 3
Psychological symptoms:
- Fear of losing control
- Need to avoid the object of fear
- Anxiety or panic aXack
- Feeling the fear aPer the thought of having to be exposed to the object of fear 4
In industrial na8ons, phobias are the most common kind of anxiety disorder. They can affect people of any age, sex, and socioeconomic status. 5
THREATMENT
Cogni3ve behavioural therapy CBT is a type of counselling that can help manage psychological issues by altering the way a person thinks and behaves. It is used to provide prac8cal ways of dealing with the phobia. The na8onal 6
service framework contend that CBT is the number one treatment for depression, panic disorder,
Phobias’, NHS choices, 2016, hXp://www.nhs.uk/condi8ons/phobias/pages/introduc8on.aspx [accessed 29 3
November 2016].
‘Specific phobias’ WebMD < hXps://www.webmd.com/anxiety-panic/specific-phobias#1> [accessed 21 4
February 2017].
Chris8an Nordqvist, ‘Everything you need to know about phobias’, Reviewed by Timothy J. Legg, PhD, CRNP, 5
Medicalnewstoday, 2017 hXps://www.medicalnewstoday.com/ar8cles/249347.php, [accessed 18 November 2016].
Phobias’, NHS choices, 2016, hXp://www.nhs.uk/condi8ons/phobias/pages/introduc8on.aspx [accessed 29 6
November 2016].

obsessive compulsive disorder etc. The same evidence is shown by the Department of Health’s 7
guidelines which cites CBT as the first for depressive disorders, panic disorder, anxiety disorder, agoraphobia etc. 8The aim is to help pa8ents to find different views in which they perceive the object of fear. The clinician’s aim is also to explain the possible beneficial impact that the development of a different view will have on the pa8ent’s life. 9A CBT therapist aXempts to centre therapy on anxiety management techniques. During exposure, he teaches pa8ents breathing exercises along with focusing on restructuring pa8ents’ thinking frameworks that drive the phobia. In the end, the pa8ents always receive homework task that would force them to face the object of fear again e.g. look at the photos of spiders online if they have arachnophobia. Psychoeduca8on is the key element of CBT. It provides a pleasant atmosphere for the pa8ent as he is being treated with care and responsibility, which all pa8ents appreciate. 10
However, in prac8ce CBT is oPen applied with elements of other therapies such as desensi8sa8on or exposure therapy (pa8ents are gradually exposed to the object of fear in different forms e.g a sound then an image then a physical object) because of its reportedly excellent response rate of 80-90% (Adler, 2010) Moreover, it is possible that in some individual cases it is ineffec8ve to aXempt to 11
eliminate an irra8onal fear by offering a ra8onal, logic- based argument against it. According to Professor Bitensky (the director of the clinic of neuroses in Ukraine) such mixture in the procedure 12
allows clinician to stay flexible and adjust to the needs of each pa8ent during every session. However, it can also be argued that then, the evalua8on of CBT alone becomes fu8le as the therapy is never used alone so other techniques can be compensa8ng for its limita8ons. This of course, is a valid point if it is accepted that the informa8on from the primary source is valid, which can be ques8oned.
ADVANTAGES OF CBT
1. It has theore8c evidence.
Psychologists cannot yet determine an exact combina8on of causes that lead to phobia development. The triggers that CBT and exposure therapy rely on are psychological (mainly
J. Holmes, ‘All you need is cogni8ve therapy?’, 2002, Na8onal Centre for Biotechnology Informa8on Search 7
database 324(7332): 288–294, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC1122202/ [assessed 29 November 2016].
Chris8an Nordqvist, ‘Everything you need to know about phobias’, Reviewed by Timothy J. Legg, PhD, CRNP, 8
Medicalnewstoday, 2017 hXps://www.medicalnewstoday.com/ar8cles/249347.php, [accessed 18 November 2016].
C. Nordqvist, ‘ Everything you need to know about phobias’, Reviewed by Timothy J. Legg, PhD, CRNP, 9
Medicalnewstoday, 2017 hXps://www.medicalnewstoday.com/ar8cles/249347.php, [accessed 18 November 2016].
M. Smith, R. Segal, J. Segal, ‘Therapy for Anxiety Disorders. Cogni8ve Behavioral Therapy, Exposure Therapy, 10
and Other Op8ons’, December 2017, HELPGUIDE.ORG Trusted guide to mental & emo:onal health, hXps://www.helpguide.org/ar8cles/anxiety/therapy-for-anxiety-disorders.htm [accessed 28 November 2016]
Annabelle Moore, ‘The Many Treatment Methodologies for Phobias: Finding the Best Fit’ ,NYU STEINHARDT, 11
hXp://steinhardt.nyu.edu/appsych/opus/issues/2012/fall/many, [accessed 11 November 2016].
V.S. Bitensky Doctor of Medical Sciences, Professor, Member of the Na8onal Medical Academy of Sciences of 12
Ukraine, from personal communica8on [16 July 2017].

behavioural) and sociological explana8ons of phobias; therefore, ul8mately support validity of CBT. Psychologists suggest that most phobias tend to form during childhood (4-8 years old )or 13
adolescence. Most phobias are associated with a trauma8c experience or a learned reac8on. For 14
example, a distressing experience that was somehow related to a snake can then be festered into ophidiophobia (fear of snakes). Similarly, if the parents manifestly display disgust or fear towards a certain object or a situa8on, the child can learn this response through social learning theory so may develop a phobia. Therefore, the treatment should be focused on altering the fear response that was implanted by condi8oning. David Barlow, Ph.D, one of the world’s leading experts on anxiety disorders, supports the argument above. The examples of childhood trauma8c experiences could be separa8on or loss of primary caregivers, physical, emo8onal or sexual abuse etc. It is the lack of control over such situa8ons and later over the symptoms that seems to be the dis8nguishing feature of anxiety disorders. Such explana8on supports the procedures of CBT as it helps pa8ents to 15
change their percep8on of the experienced distressing event. These explana8ons are used to support the psychological treatment of phobias, however, even though they are well-established, they should be challenged and ques8oned. For instance, behaviourists believed that a fearful response manifests due to the reflex that has been learned though condi8oning. The unarguable strength of the classical condi8oning theory is its reliance on scien8fic methods. However, it does not adduce an explana8on why the condi8oned response remains as a phobia oPen for the whole life and why humans are more prone to develop phobias for specific objects. There is some evidence 16
that avoidance of the distressing object hinders the chances of confu8ng the unhealthy belief. 17
Therefore, this also provides theore8cal support for cogni8ve therapies as aim to prevent the pa8ent’s avoidance by reinforcing exposure to the object of their fear.
2.Clinician-pa8ent rela8onship
It can be argued that the main purpose of the therapy lies not in the linguis8c skills of the therapist but in accomplishing reciprocity, mutual emo8onal resonance and a pleasant ambiance . However, 18
the paper which proposes this view was wriXen in 1994, meaning, it might be lacking temporal validity, hence, no longer useful in clinical setngs nowadays. Also, this statement is highly holis8c and humanis8c – which may be appreciated by pa8ents but at the same 8me, such idiographic approach to mental health may lead to confusion in diagnosis. Some8mes it might seem that two pa8ents have different symptoms only because they are manifested in different ways, however, they could s8ll be the signs of one disorder. Therefore, it seems as it is important to consider the
C. Nordqvist, ‘ Everything you need to know about phobias’, Reviewed by Timothy J. Legg, PhD, CRNP, 13
Medicalnewstoday, 2017 hXps://www.medicalnewstoday.com/ar8cles/249347.php, [accessed 18 November 2016]
‘Specific Phobias’, WebMed, hXp://www.webmd.com/anxiety-panic/specific-phobias#114
M. D. Jacofsky et al, ‘Psychological Explana8ons of Anxiety Disorders’, Rhode Island RISAS Student Assistance 15
Services, hXp://www.risas.org/poc/view_doc.php?type=doc&id=38474&cn=1, [accessed 22 October 2016]
S. Baldwin, ‘The classical condi8oning explana8on of phobias, and the treatment of such condi8ons.’, 16
hXps://www.academia.edu/7180734/The_classical_condi8oning_explana8on_of_phobias [accessed 17 November 2016].
S. Baldwin, ‘The classical condi8oning explana8on of phobias, and the treatment of such condi8ons.’, 17
hXps://www.academia.edu/7180734/The_classical_condi8oning_explana8on_of_phobias [accessed 17 November 2016].
Jesse H. Wright, Denise Davis,’ The Therapeu8c Rela8onship in Cogni8ve-Behavioral Therapy: Pa8ent 18
Percep8ons and Therapist Responses’ 1994, COGNITIVE AND BEHAVIORAL PRACTICE 1, pp. 26-27, Available from hXp://citeseerx.ist.psu.edu, [accessed 10 December 2017].

individual differences of every pa8ent as it may help to develop a suitable approach in treatment. However, a solely idiographic approach to every case may result in failure of detec8ng a phobia or an anxiety disorder so, arguably, it has to be diagnosed according to DSM. Another ar8cle may be sugges8ng that it could be difficult to establish a personal rela8onship with the pa8ent. The paper highlights ‘Dimensions of pa8ent expecta8ons for therapists’ behaviours’ which are based on 19
personal differences or contextual varia8ons. Hence, for some pa8ents it could even be impossible to create a closer rela8onship as they or their situa8on would instantly reject it. In addi8on, it can seem to be an unpragma8c and unprac8cal technique that will simply weary out the therapists in the process of finding the appropriate approach to every pa8ent and prolong the 8me of recovery. Some prac88oners might as well speculate about the importance of finding the right treatment as soon as possible but not construc8ng a rela8onship in every case.
3. Cultural specificity Another advantage of CBT is that it is cross-cultural which makes it more reliable as it can be used 20
with people from different countries, thus, different backgrounds and experiences. However, it is not yet proved as there might s8ll be some cultural differences which may affect the pa8ent’s percep8on of the therapy and his state during one.
4. Empirical evidence
There is also evidence from studies that support the efficacy of CBT. One study meta analysed 33 studies which examined 1193 adults with specific phobias to assess psychological approaches in the treatment of specific phobias. The meta analyses comprised studies conducted between 1977 and 2007. The researchers found that CBT had a beXer effect comparing to other groups, including CBT without exposure element. Exposure that involved physical contact with the s8mulus was found to be more effec8ve. However, placebo was also significantly more effec8ve than no treatment. 21
Another study compared internet-based self-help with one-session exposure in the treatment of spider phobia in a randomised controlled trial. The study focused on two groups of 30 par8cipants on the whole right aPer CBT and 12 months aPer it. The control groups had to use self-help with almost none interac8on with the therapist available. The study found that both treatments were effec8ve. The 12-month follow up group’s results displayed almost no significant difference to other ones. London CBT trial on depression did not find a beneficial effect which could be because of the 22
low compliance of difficult but clinically typical, as the ar8cles states, group of pa8ents. In one 23
study 8 of 11 couples that were invited to par8cipate did not aXend therapy sessions. This is a serious problem not just for the research as it makes it unreliable and lacking popula8onal validity
Jesse H. Wright, Denise Davis,’ The Therapeu8c Rela8onship in Cogni8ve-Behavioral Therapy: Pa8ent 19
Percep8ons and Therapist Responses’ 1994, COGNITIVE AND BEHAVIORAL PRACTICE 1, pp. 34, Available from hXp://citeseerx.ist.psu.edu, [accessed 10 December 2017].
‘Why Cogni8ve-Behavioral Therapy (CBT)? Advantages and Research Suppor’t, Na:onal Associa:on of 20
Cogni:ve-Behavioral Therapists,hXp://www.nacbt.org/whycbt-htm/, [accessed 20 December 2016].
hXps://www.psychology.org.au/Assets/Files/Evidence-Based-Psychological-Interven8ons.pdf. p.48; Wolizky-21
Taylor, K. B., Horowitz, J.D., Powers, M. B., & Telch, M. J. (2008). Clinical Psychology Review, 28, 1021-1037, [accessed 18 November 2016].
hXps://www.psychology.org.au/Assets/Files/Evidence-Based-Psychological-Interven8ons.pdf. p.49; 22
Andersson, G., Waara, J., Jonsson, U., Malmaeus, F., Calrbing, P., & Ost, L. (2009). Cogni8ve Behavior Therapy, 38, 114-120, [accessed 18 November 2016].
J. Holmes, ‘All you need is cogni8ve therapy?’, 2002, Na8onal Centre for Biotechnology Informa8on Search 23
database 324(7332): 288–294, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC1122202/ [assessed 29 November 2016].

but also for general prac8ce. Many people might feel uncomfortable speaking about the in8mate, distressing maXer with a stranger or simply feel reluctant to spend a long 8me on achieving recovery which is not even guaranteed. The reason for this could be found in the therapy’s procedure. For 24
example, the use of decisional balance sheets. They are u8lised to appraise the degree of risk or reward that the pa8ent’s choices or mentality during the therapy brings. Although they can be helpful there is also one major obstacle. When the pa8ent is already aware of the ra8onal thinking they should adopt a new way of thinking about the fear but they simply cannot bring themselves to do it. Such problem again affects the pa8ent’s self-percep8on as they might persuade themselves that they are failures who do not have the ability to make the simplest choices. Generally, CBT has 25
been widely cri8cised for deficiency of quan8tate research to support it. In some cases, randomised studies are not feasible to conduct so some evidence is drawn from non-randomised controlled trials. Thus, there is a substan8al lack of scien8fic basis of CBT that the scien8st of our age 26
endeavour to find.
5. Biological evidence that supports CBT
Many imaging studies have displayed that CBT alters the pa8ent’s response to a fearful s8mulus by changing the process of the brain ac8va8on at the moment of exposure. The changes were said to occur in emo8on-genera8ng and modulatory regions. The measurable indexes that the study relied on were the calibrated value of res8ng state cerebral blood flow (CBF) before and aPer CBT. Hence, 27
this suggests that CBT alters not only the psychological state but also manipulates the brain structures. If the result is achieved from both psychotherapeu8c and biological perspec8ves, perhaps, it is not important which one holds more significance and dominance. In another study the pa8ents that underwent CBT had experienced a diminu8on of their arachnophobia. Thus, it 28
reaffirms the theory. This evidence poses a ques8on whether the more modern techniques should be designed and used if the old ones keep demonstra8ng efficiency and could poten8ally meet the requirement of the scien8fic approach and are more understood and valid aPer having been put under a trial?
6.More study evidenceThe strategies used in therapy are underpinned by basic animal research. ‘What we know about the neurocircuitry and the brain basis of fear originally comes from animal research’ – psychiatrist ScoX Rauch, MD, Harvard Medical School. One of the first studies that used animals to study fear 29
N. Bolsover,2002, ‘Commentary: The “evidence” is weaker than claimed’ 288–294; hXps://24
www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC1122202/ [assessed 29 November 2016].
N. A. Roes, ‘Understand the limits of CBT’ 2011, Addic:on Professional, hXps://www.addic8onpro.com/25
ar8cle/understand-limits-cbt, [accessed 17 November 2016].
‘Evidence-Based Psychological Interven8ons’, Australian Psychological Society, hXps://26
www.psychology.org.au/Assets/Files/Evidence-Based-Psychological-Interven8ons.pdf. [Accessed 28 November 2016].
Soravia, Orosz, Schwab, Nakataki, Wiest, Federspiel, ‘ CBT reduces CBF: cogni8ve-behavioural therapy 27
reduces cerebral blood flow in fear-relevant brain regions in spider phobia’, 2016, PubMed.gov, NCBI, hXps://www.ncbi.nlm.nih.gov/pubmed/27688940, [accessed 15 January 2017].
Ibid.28
Lea Winerman, ‘Figuring out phobia. Researchers are using neuroimaging techniques to delve into the 29
neurobiological underpinnings of phobias, with a view to improving treatments.’, American Psychological Associa:on, 2005, Vol 36, No. 7, Print version p.96, available from hXp://www.apa.org/monitor/julaug05/figuring.aspx, [accessed 18 November 2016].

through classical condi8oning was Watson and Rayner (1920). In a more recent study the 30
researchers forced mice to develop a fear response to a s8mulus, like a loud sound, by combining its delivery with an aversive element such as an electric impulse. To erase the learned fear scien8sts would expose the mice to the s8mulus repeatedly without administering electric impulses un8l the mice’ response to it would go back to normal (calm). The same structure is u8lised in exposure 31
therapy with humans. This is one of the preponderant issues in psychological research. One ar8cle states that It is a great flaw of the research that the scien8sts have to adopt the findings of animal studies to humans with anxiety disorders as humans cannot be equated with animals. 32
LIMITATIONS OF CBT
1. Sessions are 8me consuming
To result in the desired outcome, it must be longitudinally repeated. This could poten8ally be one 33
of the fundamental drawbacks of the therapy as oPen it is problema8c to devote enough 8me or it is simply exaspera8ng for both the pa8ent and the clinician to be spending a long 8me on trea8ng a disorder when results are slow to manifest. Moreover, due to this, CBT might not alleviate the symptoms all at once but will keep exposing the pa8ent to their object of fear, reinforcing anxiety. It may feel more like a ‘punishment’ for some pa8ents. Nevertheless, there is evidence that the 8me 34
cannot be changed as longer therapies give beXer outcome. 35
One ar8cle contradicts that CBT is a 8me-taking procedure, sta8ng that on average 16 sessions is enough to reach an improvement. Even though there is data displayed, it s8ll can be ques8oned. It 36
is possible that for some pa8ents 16 sessions is the limit for their mental endurance.
2.Issues with diagnosis
Another issue is that psychiatric symptoms are usually interpreted based on social and psychological frameworks of doctors, pa8ents and society which may exacerbate the exis8ng symptoms. Hence, the diagnosis is highly subjec8ve in psychological prac8ces, in contrast to general medicine where all
S. Baldwin, ‘The classical condi8oning explana8on of phobias, and the treatment of such condi8ons.’, 30
hXps://www.academia.edu/7180734/The_classical_condi8oning_explana8on_of_phobias [accessed 17 November 2016].
Lea Winerman, ‘Figuring out phobia. Researchers are using neuroimaging techniques to delve into the 31
neurobiological underpinnings of phobias, with a view to improving treatments.’, American Psychological Associa:on, 2005, Vol 36, No. 7, Print version p.96, available from hXp://www.apa.org/monitor/julaug05/figuring.aspx, [accessed 18 November 2016].
Ibid.32
‘Specific Phobias. Treatment’, Perelman School of Medicine of the University of Pennsylvania, 33
Department of Psychiatry PENN BEHAVIORAL HEALTH, hXp://www.med.upenn.edu/ctsa/phobias_treatment.html, [accessed 10 November 2016].
N. A. Roes, ‘Understand the limits of CBT’ 2011, Addic:on Professional, hXps://www.addic8onpro.com/34
ar8cle/understand-limits-cbt, [accessed 17 November 2016].
J. Holmes, ‘All you need is cogni8ve therapy?’, 2002, Na8onal Centre for Biotechnology Informa8on Search 35
database 324(7332): 288–294, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC1122202/ [assessed 29 November 2016].
‘Why Cogni8ve-Behavioral Therapy (CBT)? Advantages and Research Support’ , ‘Na:onal Associa:on of 36
Cogni:ve-Behavioral Therapists’, hXp://www.nacbt.org/whycbt-htm, [accessed 10 November 2016].

judgments are based on fundamental laws and anatomical evidence. This may be explained by the 37
fact that you do not have to be a doctor to do CBT . No need to have a medical accredita8on may be 38
one of the reasons why underqualified therapists are able to con8nue their prac8ce prosperously. On the other hand, it is also possible that a CBT therapist indeed does not need to have a medical degree, whereas, a person who works with the neurological side of phobias would have to have one. In contrast, there is also a view that ‘in the wrong hands CBT can do great harm’ .This then may be a 39
problem for the psychoneurological industry as the difficulty of acquiring all the qualifica8ons to be permiXed to prac8ce, might result in a shortage of specialists due to their reluctance to undertake such intricate educa8onal path.
3.Limited applica8on
One ar8cle views the CBT therapy from a wider, different perspec8ve that may seem slightly extremist. They depict an example where, theore8cally, the therapy would have to be provided for an American president that has launched a war. They challenge the appliance of CBT and 40
emphasise its limits in terms of severity of cases. In phobic disorders, even though such cases would be extremely rare, there could be a pa8ent who because of his severe vermiphobia (fear of bacteria and infec8ons) has developed OCD and/or an anxiety disorder and physically is unable to leave the room without mul8ple layers of ‘protec8on’. What if this pa8ent is a single mother of three children and she blames herself for being unable to take care of them and the Childcare services already knocking on her door? Would CBT be useful then?
4.The technique is outdated
The Na8onal Ins8tute of Mental Health study of depression (the largest of its kind in the world) is now 20 years old and its findings are s8ll applied to support CBT. This suggests that the exis8ng CBT studies lack temporal validity so the field requires new research. Another ar8cle supports this by 41
displaying the results of the meta-analysis of 70 studies on CBT conducted between 1977 and 2014. The researches Tom Johnsen and Oddgeir Friborg found that CBT is approximately half as effec8ve in the treatment of depression as it used to be. They support the idea that it might be possible that 42
CBT is endangered due to the incompetency of the newly educated or perhaps not properly educated specialists.
J. Holmes, ‘All you need is cogni8ve therapy?’, 2002, Na8onal Centre for Biotechnology Informa8on Search 37
database 324(7332): 288–294, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC1122202/ [assessed 29 November 2016].
Ibid.38
R. D. Lewis, ‘Cogni8ve Behavioral Therapy: The Good, The Bad, The Limita8ons’,2013, ‘Mad in America’, 39
hXps://www.madinamerica.com/2013/05/cogni8ve-behavioral-therapy-the-good-the-bad-the-limita8ons/, [accessed 25 January 2017].
ibid.40
J. Holmes, ‘All you need is cogni8ve therapy?’, 2002, Na8onal Centre for Biotechnology Informa8on Search 41
database 324(7332): 288–294, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC1122202/ [assessed 29 November 2016].
O. Burkeman, ‘Why CBT is falling out of favour. ‘Researchers have found that CBT is roughly half as effec8ve 42
in trea8ng depression as it used to be’’, 2015, Theguardian, hXps://www.theguardian.com/lifeandstyle/2015/jul/03/why-cbt-is-falling-out-of-favour-oliver-burkeman, [accessed 25 January 2017].

Decoded Neurofeedback as an alterna3ve to CBT.
How does it work?
Neurofeedback is a field in biofeedback. Biofeedback is an approach which goal is to help the individuals to learn to control their brain ac8vity and subsequently the psychological manifesta8ons of that ac8vity. Biofeedback monitors and measures heart rate, blood pressure, brain electrical ac8vity, brain blood supply etc. 43
“Neurofeedback is a type of biofeedback and based on the theory that accurate informa8on about states of the body allows a person to learn to control those physical states.” 44
“Decoded Neurofeedback” is focused on the collec8on and recording of data received on the basis of neural ac8va8on of one individual as a response to a s8mulus e.g a video game. Then the second individual is exposed to the same s8mulus and during training learns to match his neural ac8vity with the ac8vity of the first individual. During the session, the person is subconsciously manipula8ng his 45
brain ac8vity usually in a virtual context e.g. a video game in which the desirable or the undesirable outcomes serve as indicators of the quality of his brain performance. When his brain ac8vity matches the one desirable by the inves8gator, the person receives a reward in the game. If the ac8vity is undesirable, the person loses points in the game. Such technique of posi8ve reinforcement and posi8ve punishment can result in change in the brain ac8vity. 46
Real 8me fMRI is essen8al in real 8me decoded neurofeedback as it allows to create a blueprint-like map of an individual’s cor8cal ac8va8on. Moreover, it also u8lised during training with the second individual. 47
How brain ac8vity is detected? Electroencephalography (EEG) and func8onal magne8c resonance imaging (fMRI) are the two non-invasive tools that are usually employed to either detect the frequency or loca8on of brain ac8vity,
D. Moss, L. Kirk, ‘Evidence-Based Prac8ce in Biofeedback and Neurofeedback’, ‘applied psychophysiology and 43
biofeedback’,hXps://www.aapb.org/files/public/Yucha-Gilbert_EvidenceBased2004.pdf; p.2 ,[accessed 27 February 2017].
‘How Neurofeedback Works’, ‘Brainwave Training. Makng good brains beXer.’, hXp://44
measurebrainwaves.com/index.php/how-neurofeedback-works, [accessed 21 February 2017].
‘Decoded Neurofeedback (DecNef): Method, Research & Poten8al Benefits’, ‘Mental Health Daily. Mental 45
Health Blog’, hXp://mentalhealthdaily.com/2015/07/16/decoded-neurofeedback-decnef-method-research-poten8al-benefits/, [accessed 21 February 2017].
T. Asher figures: B. Wierbowski , ‘Brain training: The future of psychiatric treatment?’, 2017, ‘SITN Science In 46
The News. Harvard University: The Graduate School of Arts and Sciences’, hXp://sitn.hms.harvard.edu/flash/2017/brain-training-future-psychiatric-treatment/ [accessed 30 January 2017].
‘Decoded Neurofeedback (DecNef): Method, Research & Poten8al Benefits’, ‘Mental Health Daily. Mental 47
Health Blog’, hXp://mentalhealthdaily.com/2015/07/16/decoded-neurofeedback-decnef-method-research-poten8al-benefits/, [accessed 21 February 2017].

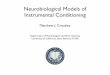
respec8vely. (Figure 1). 48
Figure 1. (EEG, leP) detects neuronal electrical impulses in the cortex of the brain. Func8onal Magne8c Resonance Imaging (fMRI, right) shows the level of blood supply of each brain region. 49
1)EEG- When the person performs a behavioural or a cogni8ve task, the neurones in the cortex are ac8vated and emit electrical energy that is detected by electrodes on the scalp. This ac8vity is scien8fically referred to as oscilla8ons, or waves. 50
2)In fMRI areas, the higher level of blood flow stated to be more ac8ve. During different tasks, more blood is administered to the region involved in the performance of the task, therefore, fMRI allows to detect which regions correspond to each task. 51
ADVANTAGES
1.It is supported by psychological theories of learning and by the biological ac8vi8es that underpin them. In the brain, the fact of learning is evident in the enhanced ac8va8on of sensory networks, ac8vity in memory and learning regions, increased grey maXer volume and changes in white maXer. These
T. Asher figures: B. Wierbowski , ‘Brain training: The future of psychiatric treatment?’, 2017, ‘SITN Science In 48
The News. Harvard University: The Graduate School of Arts and Sciences’, hXp://sitn.hms.harvard.edu/flash/2017/brain-training-future-psychiatric-treatment/ [accessed 30 January 2017].
Ibid.49
Ibid.,2.50
T. Asher figures: B. Wierbowski , ‘Brain training: The future of psychiatric treatment?’, 2017, ‘SITN Science In 51
The News. Harvard University: The Graduate School of Arts and Sciences’, hXp://sitn.hms.harvard.edu/flash/2017/brain-training-future-psychiatric-treatment/ [accessed 30 January 2017].

subjects are objec8ve so can be targeted with r|MRI. In contrast according to psychological 52
theories (e.g. behaviourism), learning occurs when a specific experience influences behaviour or cogni8on. In the case of r|MRI such experience is the task, feedback about the ac8va8on of the brain areas, numerous paXerns of brain ac8vity, cogni8ve processes that appear etc. Learning with 53
r|MRI is based on several suggested mechanisms but the dominant one resembles the basic behaviourist condi8oning models. It is called “a reward-based skill learning via cor8cal-basal ganglia brain networks.” Condi8oning occurs as a result of a feedback that is received from a brain region. S8mula8on of this region may act as a reinforcing reward. Because of the increased ac8vity in this region and the tangen8al regions that relate to the feeling of reward, plas8city occurs in that area. 54
Overall, both CBT and Decoded Neurofeedback are based on condi8oning theories only worth the second one being more empirical as a research tool and more pleasant as a treatment. One of the main advantages is that it is delivered by experts with at least 10 years of experience in the field. 55
Considering the fact that CBT therapy can be delivered by a person without a medical degree, hence, without experience with mental health, neurofeedback appears more credible.
2. Used as a treatment. Many different psychiatric disorders are characterized by specific paNerns of brain ac3vity which led researchers and clinicians to inves8gate whether EEG and fMRI-based Neurofeedback training that u8lises EEG and fMRI can change the malfunc8ons of the brain. The example provided below 56
illustrates the mechanism of neurofeedback in the case of ADHD treatment. 57
Children with for aXen8on-deficit hyperac8vity disorder (ADHD) tend to display lower levels of high frequency beta waves and higher levels of low frequency theta waves (the bar chart on the right) while children without this diagnosis show the opposite paXern (the bar chart on the leP). This observa8on suggests that beta waves are associated with the enhanced ability to focus as they are the waves which are underac8ve in ADHD children. The purpose of neurofeedback training is to bring the pa8ent to balance the level of the waves in their brain. During training, the pa8ent receives feedback about their own brain ac8vity, some8mes in the form of a videogame. When children 58
succeed in altering their brain ac8vi8es during training, they are rewarded e.g points in the video game. Similarly, they are deprived of the reward when their brains generate higher level of theta waves. This process allows the children’s brains to subconsciously learn how to generate the wave of each frequency at a level found in healthy individuals. Even though, the example is not about 59
L.E. Stoeckel et al., ‘Op8mizing real 8me fMRI neurofeedback for therapeu8c discovery and development.’, 52
2014, ‘US Na:onal Library of Medicine Na:onal Ins:tutes of Health’, NCBI, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC4141981/, [accessed 21 February 2017].
Ibid.53
Ibid.,2.54
‘How Neurofeedback Works’, ‘Brainwave Training. Makng good brains beXer.’, hXp://55
measurebrainwaves.com/index.php/how-neurofeedback-works, [accessed 21 February 2017].
T. Asher figures: B. Wierbowski , ‘Brain training: The future of psychiatric treatment?’, 2017, ‘SITN Science In 56
The News. Harvard University: The Graduate School of Arts and Sciences’, hXp://sitn.hms.harvard.edu/flash/2017/brain-training-future-psychiatric-treatment/ [accessed 30 January 2017].
Ibid.57
Ibid.,2.58
T. Asher figures: B. Wierbowski , ‘Brain training: The future of psychiatric treatment?’, 2017, ‘SITN Science In 59
The News. Harvard University: The Graduate School of Arts and Sciences’, hXp://sitn.hms.harvard.edu/flash/2017/brain-training-future-psychiatric-treatment/ [accessed 30 January 2017].

phobias, it is useful for demonstra8ng the applicability of the approach in a clinical setng. In spite of usefulness of this informa8on, one disadvantage of it is that it is based on one source. The evidence of the use of Decoded-Neurofeedback in treatment of mental illness is extremely limited. This already gives an insight into the likely limita8ons of the technique.
Figure 2. 60
3. During the sessions par8cipants feel empowered to change their state. Par8cipants can carry out an unlimited number of cogni8ve manipula8ons to control brain ac8vity and neurofeedback whilst the condi8ons and the environment remain under control of the researchers, providing internal validity of the procedure. In some studies, the researchers do not inform the person when feedback will be presented but in the frame of another paradigm. Having 61
power is important for pa8ents as it prevents the feeling of being trapped in their illness. Moreover, it solves the general problem in scien8fic approaches which are focused solely on the brain. Decoded-Neurofeedback appears more holis8c and less determinis8c as even though behaviours are s8ll predetermined by the brain, the pa8ents are welcomed to believe they have free-will to overcome it.
4.It is supported by research.
Dr. Ben Seymour’s comment on the study on recondi8oning the brain to overcome fear supports the usefulness of Decoded- Neurofeedback on the biological level as he says they “could no longer see the typical fear skin-swea8ng response nor iden8fy enhanced ac8vity in the amygdala - the brain's fear centre". She then concludes that the benefice of the approach is indeed in the fact that the par8cipants do not consciously experience fear during Decoded-Neurofeedback. 62
DeCharms and colleagues found that aPer being trained to regulate the ac8vity in the dorsal anterior
T. Asher figures: B. Wierbowski , ‘Brain training: The future of psychiatric treatment?’, 2017, ‘SITN Science In 60
The News. Harvard University: The Graduate School of Arts and Sciences’, hXp://sitn.hms.harvard.edu/flash/2017/brain-training-future-psychiatric-treatment/ [accessed 30 January 2017].
‘Decoded Neurofeedback (DecNef): Method, Research & Poten8al Benefits’, ‘Mental Health Daily. Mental 61
Health Blog’, hXp://mentalhealthdaily.com/2015/07/16/decoded-neurofeedback-decnef-method-research-poten8al-benefits/, [accessed 21 February 2017].
hXps://www.eurekalert.org/pub_releases/2016-11/uoc-rtb111816.php62

cortex (brain region related to the percep8on and modera8on of pain) the par8cipants experienced change in their percep8on of pain. Another study found that Dec-Nef successfully reduced 63
amygdalar fear responses during the cunter-condi8oning of visual-cor8cal-based fear,without the par8cipants’ awareness of the purpose of the procedure. Other studies have also reported 64
decreased mood symptoms in people with depression (Linden et al., 2012) and lowered contamina8on anxiety in subjects diagnosed with sub-clinical anxiety (Scheinost et al., 2013).
5. It is painless. Some scien8fic evidence supports the theory that the approach is indeed pain free. If consider 65
psychological distress as pain, neurofeedback appears in an advantage comparing to CBT therapy. To illustrate the difference in the individual’s level of stress it might be worth looking at the example of a real 8me in vivo exposure therapy such as the one in the video. However, a conclusion cannot be 66
drawn from a single example of an in vivo session. Nevertheless, it could be argued that the point itself has high face validity as knowing the procedure of the therapy it becomes clear that many pa8ents could be distressed and uncomfortable during the therapy.
LIMITAIONS
1. One limita8on is that there is a shortage of the scien8fic clinical studies.Despite all the evidence, it should be underlined that the studies were not conducted with clinical samples whilst the technique has aspira8ons to be implemented into mental health where it would target real pa8ents. Without the relevant and valid evidence for the efficacy of Decoded Neurofeedback in the clinical setng with real pa8ents this could be an issue. The findings of existent studies can be a subject to doubts as due to the novelty of the technique, there might have been a certain degree of inves8gator bias due to the excitement to find a ground-breaking evidence. Also, the limited findings cannot be generalised to all of the popula8on as each of them had different samples – par8cipants had different mental illnesses or were not clinically diagnosed with one at all.
2. The existent studies have small sample in studies . 67
This makes their findings less generalisable to the wider popula8on. In studies it is also primordial to establish a reliable metric system e.g change index with which scien8sts would be able to measure the clinical significance of r|MRI neurofeedback training-induced changes. Un8l this is done, some 68
study evidence can be ques8oned in terms of the extent to which it proves the efficacy of Decoded Neurofeedback.
L.E. Stoeckel et al., ‘Op8mizing real 8me fMRI neurofeedback for therapeu8c discovery and development.’, 63
2014, ‘US Na:onal Library of Medicine Na:onal Ins:tutes of Health’, NCBI, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC4141981/, [accessed 21 February 2017].
A. Koizumi et al, ‘Fear reduc8on without fear through reinforcement of neural ac8vity that bypasses 64
conscious exposure’ 2016, NCBI, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC5628620/, [accessed 21 February 2017].
‘How Neurofeedback Works’, ‘Brainwave Training. Makng good brains beXer.’, hXp://65
measurebrainwaves.com/index.php/how-neurofeedback-works, [accessed 21 February 2017].
Jack Smethells (youtube channel),‘Snake Phobia Behavioral (Exposure) Therapy’, hXps://www.youtube.com/66
watch?v=zKTpecooiec&t=427s, [accessed 21 November 2016].
Ibid.67
Ibid.,2.68

3. Is medica8on necessary before r|MRI? One ar8cle suggests that the par8cipants or pa8ents do not have to be exposed to any addi8onal pharmacological treatment. This could be an advantage as nowadays, some psychologists voice 69
their concern at the heavy medicalisa8on of psychological condi8ons. However, of course, in case if Decoded Neurofeedback replaced CBT completely, it would place pharmaceu8cal companies into a disadvantage. Furthermore, even though it has been suggested that the medica8on or any help as a prepara8on for training is not necessary, there is evidence that cogni8ve strategies performed before neurofeedback, enhanced learning. The inconsistency of evidence on this aspect of the technique 70
places it at a disadvantage as it appears to be not fully scru8nised to be used in treatment.
4. No evidence of causality of the effects.Many studies men8oned in the paper have not actually considered the causality of the findings. This factor is vital for establishing r|MRI decoded neurofeedback as a valid tool for treatment. As a 71
science, psychology strives to find explana8ons of distor8ons of the brain func8oning and their subsequent effects on behaviour. Hence, it is an undoub|ul requirement for the treatment to be proven to lead to recovery in order to be employed in clinical prac8ce. Otherwise, there is always a chance that other factors or phenomena such as placebo effect might be contribu8ng to the allevia8on of anxiety and not the method itself.
5. Another problem with the neuroscien8fic approach is in the idea of consciousness. It is unfortunate for modern science that consciousness cannot yet be studied in an empirical way. It is based on our interac8on with the environment as the brain interacts with the rest of the body; any changes in the environment or in the body result in changes in consciousness and the brain respec8vely, and vice versa. – Clark and Chalmers. Therefore, considering this opinion, the 72
biological approach is might not be as useful as it presents itself. However, even though, it is true that it cannot address consciousness it does not make it less efficient in treatment.To counter this, Davey (2007) suggests that the phobic response some8me is produces as a result of biophysiological responses of our body . The theory views some phobic responses as ‘the misaXribu8on of bodily 73
sensa8ons directly to a par8cular situa8on’ . For instance, a symptom such as nausea in a certain 74
situa8on can be interpreted as threatening and lead to a distorted percep8on of the event. 75
Therefore, this would suggest that the access to consciousness is redundant when trea8ng specific phobias.
‘How Neurofeedback Works’, ‘Brainwave Training. Makng good brains beXer.’, hXp://69
measurebrainwaves.com/index.php/how-neurofeedback-works, [accessed 21 February 2017].
L.E. Stoeckel et al., ‘Op8mizing real 8me fMRI neurofeedback for therapeu8c discovery and development.’, 70
2014, ‘US Na:onal Library of Medicine Na:onal Ins:tutes of Health’, NCBI, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC4141981/, [accessed 21 February 2017].
Ibid.71
T. Fuchs, ‘The Brain – A Media8ng Organ’, Imprint Academic 2011, available from hXps://www.klinikum.uni-72
heidelberg.de/fileadmin/zpm/psychatrie/fuchs/The_Brain_-_A_Media8ng_Organ.pdf, pp. 197, [accessed 11 December 2017].
S. Baldwin, ‘The classical condi8oning explana8on of phobias, and the treatment of such condi8ons.’, 73
hXps://www.academia.edu/7180734/The_classical_condi8oning_explana8on_of_phobias [accessed 17 November 2016]
ibid.74
Ibid.,2. 75

6. Nega8ve opinion of cliniciansAs a part of the research for this paper, two psychiatrists were interviewed – Dr. Catalan from a clinic in London and Dr.Bitensky from a clinic in Ukraine. Both of them voiced their concerns about the idea of replacing psychotherapeu8c treatments with the more advanced neuroscien8fic ones. Both stated that the methods are simply not fully advanced and not developed enough to be used as a standard prescribed treatment for mental disorders; even for the mild ones like specific phobias. Dr. Bitensly said that it is likely that it is the uniqueness of each pa8ents and their case that hinders it. Hence, he suggested that psychologists cannot apply something so controlled and limited in its func8on to something like human mind – an area where clinicians have liXle control and the limits of which have not yet been defined. To counter this, it should be taken into account that these opinions are very subjec8ve and provide liXle insight into the world of clinical prac8ce.
DISCUSSION
Neurobiological approach may help psychological therapies through evalua8ng and challenging their methods or otherwise suppor8ng them with the valid scien8fic evidence, rending them more credible. Biological and neurological research on its own can be too reduc8onist to serve as a complete explana8on of human behaviour. Considering the effect that the psychological state and the outer environment have on the brain, it is important to take them into account. This will help to achieve a whole wide panorama of each mental disorder, compare each case to the exis8ng ones and choose a suitable way of treatment. It is primordial to focus on the pa8ent’s wellbeing and not solely on acquiring strictly objec8ve, scien8fic procedures that could be applied to every individual, thus simplify the job of the clinician. Considering all the advantages and limita8ons of both techniques it is impossible to deem one to be more efficient and beneficial. A compromise between neuroscience and psychotherapy could be poten8ally found in the interac8onist approach, just like in nature-nurture debate. Instead of choosing one technique over the other, the ways of ameliora8on could be considered. For example, a new technique or an adjustment can be introduced in order to eliminate a common disadvantage of both techniques.
To provide a solu8on for the debate I am going to suggest a new method which could be used to improve both CBT and Decoded-Neurofeedback by elimina8ng one common limita8on that they share – the persistence of the effects.
Persistence of the results as the common limita8on of CBT and Decoded-Neurofeedback.
Due to the complex nature of the learning process, the persistence of the learned response is dubious. There is a sugges8on that learning is developed over different periods of 8me and that its persistence cannot be encaged into a specific 8me frame. Persistence depends on the type of learning and the brain system. Some studies found that the regula8on of the brain ac8vity could 76
not be performed without neurofeedback even aPer the par8cipants had undergone several sessions. Also, the first study assessed behaviour only at the 8me of r|MRI neurofeedback training so there is a shortage evidence of the effects in the long term. Therefore, one problem could be 77
the fact of individual differences of the par8cipants and the es8ma8on of the expected persistence
L.E. Stoeckel et al., ‘Op8mizing real 8me fMRI neurofeedback for therapeu8c discovery and development.’, 76
2014, ‘US Na:onal Library of Medicine Na:onal Ins:tutes of Health’, NCBI, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC4141981/, [accessed 21 February 2017].
Ibid.77

of the effects of training. Interes8ngly, CBT also can be cri8cised for this limita8on. Due to the social desirability bias or demand characteris8cs it can be difficult to assess the effec8veness of the therapy aPer many years post treatment. However, one study found that children (7 to 11-year-old) who were administered neurofeedback training showed more improvement in ADHD symptoms which persisted aPer 6 months from the last session, whereas, the children who were administered “the cogni8ve training” showed less improvement. Hence, according to this Neurofeedback is more persistent than Cogni8ve therapy in its effects. However, it is important to note that the study 78
involved “neurofeedback” but not Decoded-Neurofeedback and “Cogn8ve Therapy” but not CBT, therefore, the findings cannot be fully applied to the discussion of this paper as the independent variable are not iden8cal.
Why is this limita:on important?
Overall, the inability to measure the persistence of the effects of either technique makes them less valid as the main aim of psychological treatment is too accomplish complete recovery. However, it’s crucial to remember that this would be the case in the ideal world. In reality, even the well-established, efficient methods in medicine have to face the issue of unexpected remission.
Factors that prevent the eradica:on of the problem.
Arguably, the persistence of the beneficial effects is equally hard to measure as the persistent of the malignant condi8ons. Perhaps, it is more reasonable to put a greater focus on the difference of the aspects of procedure that contribute towards recovery because, ini8ally, any flaws in a treatment are caused by the flaws in its procedure. The persistence of the effects depends on its relatability and generalisability to different environments and context. This is one the gravest issues in CBT and Decoded Neurofeedback. Both techniques are used in the controlled 79
laboratory environments. This may be a problem when pa8ents comes to face their fear in a more natural setng where their emo8onal state and behavioural responses would not be under supervision. When the pa8ent unexpectedly encounters the object of fear, his cogni8ve processes that ‘control the brain ac8vity’ or the condi8oned response might not manifest themselves. The psychological theory of forgetng suggests that forgetng oPen occurs in the absence of ‘the keys’ that were present during learning. Therefore, this supports the argument that the ‘keys’ eg. the room itself, the clinician, his prompts etc. which all were present in the lab would not be there in real life, therefore, this could poten8ally hinder the reproduc8on of the learned response.
The method
As an example of a specific phobia, trypophobia (fear of a paXern of holes) will be used.
To start with, each pa8ent who undergoes either CBT or Decoded- Neurofeedback as a treatment for their trypophobia should receive a small white carton picture frame in the end of the first session. They should be asked to go back home and frame a picture that evokes pleasant emo8ons e.g a photo of their pet, beau8ful scenery, appe8sing food etc. with the received picture frame. The picture should be hanged or placed in the place where they spend the most of their 8me. It is
N. J. Steiner, El. C. FreneXe, K. M. Rene, R. T. Brennan, El. C. Perrin, ‘In-School Neurofeedback Training for 78
ADHD: Sustained Improvements From a Randomized Control Trial’, AAP News and Journals Gateway, 2014, VOLUME 133 / ISSUE 3 hXp://pediatrics.aappublica8ons.org/content/133/3/483.long, [accessed 11 December 2017].
L.E. Stoeckel et al., ‘Op8mizing real 8me fMRI neurofeedback for therapeu8c discovery and development.’, 79
2014, ‘US Na:onal Library of Medicine Na:onal Ins:tutes of Health’, NCBI, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC4141981/, [accessed 21 February 2017].

important that it is not the place where they feel the most safe and comfortable such as their bedroom. APer that, when the pa8ent is ready, they should start placing liXle dots of different colours onto the frame but not the picture itself. As the pa8ent becomes more comfortable with the ac8vity and its outcome, they should draw more dots and eventually enlarge them. APer at least one month, if the pa8ent feels at ease with the appearance of the picture frame, they should poke the first hole through one of the dots. As they become more used to it, the number of holes should increase. It is advised to create mul8ple holes at a 8me. The pa8ent should end up with the picture frame covered with small holes and no feeling of anxiety as a response to it.
Explana8on of the method.
Why should it be introduced?
The method should be incorporated into both CBT and Decoded Neurofeedback. It could bring an element of “homework” into Decoded-Neurofeedback that it currently lacks whilst for CBT it will enhance its exis8ng “homework”. As a result, ideally, persistence of the effects would be achieved in both techniques.
‘A carton picture frame’. It is cheap or can b hand-made which is an advantage for clinicians.
Why does it have to hand-made?
This idea is based on ‘The Ikea effect’ and operant condi8oning. ‘The Ikea effect’ is the theory of behavioural economics and consumer psychology that suggests that people value more the objects that they have made themselves. Therefore, with 8me, the affec8on towards the hand-made 80
objects strengthened by the affec8on towards the picture will be learned due to the con8nuous exposure to it during the day. Hence, when the pa8ent decides to create a fear s8mulus (make a hole in the picture frame) it will not provoke the same level of anxiety due to the Ikea Effect and due to the already learned posi8ve response to the picture. Due to the prolonged exposure, the pleasant picture will soon become associated with the picture frame, so the same feeling of pleasure will be experienced when looking at it. This will be due to both, posi8ve reinforcement of the pleasant feelings and the posi8ve punishment (providing the pa8ent with the pleasant picture to eliminate poten8al anxiety towards the transformed picture-frame). According to the reciprocal inhibi8on theory (studies in A Level Psychology), two opposing feelings cannot be experienced at the same 8me, therefore, the intensity of pleasure induced by looking at the photo and decora8ng the picture frame, in theory, should overpower the fear response. One study, further demonstrates the importance of the feeling of pleasure being elicited in the brain instead of the feeling of composure (aimed for in CBT when it involves elements of counter-condi8oning) for the most effec8ve ex8nc8on of fear response. The study showed that the disengagement of the par8cipants’ VMPFC (the ventral medial prefrontal cortex) which is responsible for the feeling of composure was strongly associated with the reduced fear response. Hence, the ‘safety’ feeling could be not the most suitable and effec8ve procedural aim of the psychotherapeu8c treatments of phobia. However, it is important to 81
Michael I.Norton, D. Mochon,D. Ariely ,’The IKEA effect: When labor leads to love’, 2012, Pages 453-460, 80
Journal of Consumer Psychology, Science Direct, hXp://www.sciencedirect.com/science/ar8cle/pii/S1057740811000829, [accessed 6 December 2017].
A. Koizumi et al., ‘Fear reduc8on without fear through reinforcement of neural ac8vity that bypasses 81
conscious exposure’, N. Hum Behav.Published online 2016 Nov 21, NCBI PMC US Na:onal Library of Medicine Na:onal Ins:tutes of Health, hXps://www.ncbi.nlm.nih.gov/pmc/ar8cles/PMC5628620/, [accessed 21 February 2017].

take into account that the study was conducted on healthy par8cipants, so the findings might not be generalisable to pa8ents with phobias.
Intensity of the feeling.
We need to take into account the Intensity of the feeling that is induced as it maXers for the successful elimina8on of anxiety. According to Mel Robbins’s , the mind-body connec8on must be 82
taken into account during elimina8on of anxiety. In any therapy, the goal is to eradicate anxiety and achieve the state of complete composure both for the body and the mind. However, most procedures ignore the effect that physiological changes such as adrenaline fluctua8ons have on our state. Hence, if we propel pa8ents into mental tranquillity, ignoring the state of the body, we will not be able to achieve the desired state. This is supported by Davey who claims that phobia is ‘the 83
misaXribu8on of bodily sensa8ons directly to a par8cular situa8on’. Therefore, the body which remains agitated will send messages to the brain eventually causing anxiety – a more powerful feeling that might overpower the neutral feeling of composure. Hence, a phobic response occurs. In order to achieve the desired state, we need to impel a feeling of the same intensity (e.g posi8ve excitement or pleasure) in the pa8ent’s mind so when the brain coordinates it with the received signals of excitement from the body it does not produce anxiety, but pleasure and eventually composure.
Importance of the place where it is kept.
The picture frame should be kept in the area where the pa8ent spends much of their 8me due to the available variety of ac8vi8es and situa8ons that they can experience there e.g. social interac8ons with different people in the office. This will ensure the presence of an unstable environment, different from the environment of CBT and Decoded Neurofeedback rooms. Instability of the environment will ensure that the pa8ent does not associate learned affec8on towards the picture frame with the environmental cues. This is why they must be advised against keeping the picture frame in their bedroom as they will associate it with the comfort and safety of their rooms so when these cues are not present, the effects of the “homework” will not persist. This is important as the main aim of the method is to prepare the pa8ent to confront their fear in any possible situa8on and environment.
CONCLUSION
Ideally, such method could lead to an increased value of persistence of the effects of the treatment in pa8ents with specific phobias. Although, the method is subjec8ve and based on the assump8ons of an unqualified individual, it was proposed solely to suggest how the debate between psychotherapy and neuroscience in mental health could be resolved. As said before, nowadays, for the pa8ent’s wellbeing it could be more important to consider the improvement of the exis8ng, working techniques than striving to contest one or the other.
Mel Robbins, ‘The Secret to Stopping Fear and Anxiety (That Actually Works)’ youtube.com, hXps://82
www.youtube.com/watch?v=6n8i7ua0mSw, [accessed 10 March 2017].
S. Baldwin, ‘The classical condi8oning explana8on of phobias, and the treatment of such condi8ons.’, 83
hXps://www.academia.edu/7180734/The_classical_condi8oning_explana8on_of_phobias [accessed 17 November 2016].


BIBLIOGRAPHY
1. Asher. T., figures: Wierbowski B. , ‘Brain training: The future of psychiatric treatment?’, 2017, ‘SITN Science In The News. Harvard University: The Graduate School of Arts and Sciences’, hDp://sitn.hms.harvard.edu/flash/2017/brain-training-future-psychiatric-treatment/ [accessed 30 January 2017]
2. Baldwin S., ‘The classical condiPoning explanaPon of phobias, and the treatment of such condiPons.’,hDps://www.academia.edu/7180734/The_classical_condiPoning_explanaPon_of_phobias [accessed 17 November 2016]
3. Basiri N., ‘Comparison of the EffecPveness of CogniPve Behavioral Therapy and Neurofeedback: Reducing Insomnia Symptoms’, Available from: A.H. Ghaderi, 2017, Global Journal of Health Science; Vol. 9, No. 7, available from hDps://www.researchgate.net/publicaPon/315682368_Comparison_of_the_EffecPveness_of_CogniPve_Behavioral_Therapy_and_Neurofeedback_Reducing_Insomnia_Symptoms [accessed December 2017]
4. Beck A.T., Emery G., Greenberg R., ‘Anxiety Disorders And Phobias: a cogniKve perspecKve’, Basic Books, 2005 (the United States of America, Cambridge), pp 3-53, 115-132, 167-230. [accessed 25 February 2017]
5. Bolsover N.,2002, ‘Commentary: The “evidence” is weaker than claimed’ 288–294; hDps://www.ncbi.nlm.nih.gov/pmc/arPcles/PMC1122202/ [assessed 29 November 2016]
6. Burkeman O., ‘Why CBT is falling out of favour. ‘Researchers have found that CBT is roughly half as effecPve in treaPng depression as it used to be’’, 2015, Theguardian, hDps://www.theguardian.com/lifeandstyle/2015/jul/03/why-cbt-is-falling-out-of-favour-oliver-burkeman, [accessed 25 January 2017]
7. ‘Can a high-tech treatment help combat some of our oldest fears?’, NHS choices, 2016,hDp://www.nhs.uk/news/2016/11November/Pages/Can-a-high-tech-treatment-help-combat-some-of-our-oldest-fears.aspx, [accessed 29 November 2016]
8. ‘CauPons Regarding CogniPve-Behavioral IntervenPons Provided Within a Month of Trauma. How effecPve is CogniPve-Behavioral Therapy for early intervenPon?’, U.S. Department of Veterans affairs, Excerpted with permission from Bryant, R.A., & Harvey, A.G. (2). Acute Stress Disorder: A handbook of theory, assessment, and treatment. Washington, D.C.: American Psychological AssociaPon Press, hDps://www.ptsd.va.gov/professional/treatment/early/cbi-aoer-trauma.asp, [accessed 5 May 2017]
9. Davey G.C.L (ed.), ‘PHOBIAS. A Handbook of Theory, Research and Treatment’, ‘Willey & Sons Ltd., 1997 (West Sussex, England), [accessed 20 June 2017]
10. ‘Decoded Neurofeedback (DecNef): Method, Research & PotenPal Benefits’, ‘Mental Health Daily. Mental Health Blog’, hDp://mentalhealthdaily.com/2015/07/16/decoded-

neurofeedback-decnef-method-research-potenPal-benefits/, [accessed 21 February 2017]
11. ‘Evidence-Based Psychological IntervenPons’, Australian Psychological Society, hDps://www.psychology.org.au/Assets/Files/Evidence-Based-Psychological-IntervenPons.pdf. [Accessed 28 November 2016]
12. ‘Exposure Therapies For Specific Phobias. Status: Strong Research Support’, Society of Clinical Psychology, Available from hDps://www.div12.org/psychological-treatments/treatments/exposure-therapies-for-specific-phobias, [accessed 29 October 2016]
13. Fuchs T., ‘The Brain – A MediaPng Organ’, Imprint Academic 2011, available from hDps://www.klinikum.uni-heidelberg.de/fileadmin/zpm/psychatrie/fuchs/The_Brain_-_A_MediaPng_Organ.pdf, pp. 196-218, [accessed 11 December 2017]
14. Holmes J., ‘All you need is cogniPve therapy?’, 2002, NaPonal Centre for Biotechnology InformaPon Search database 324(7332): 288–294, hDps://www.ncbi.nlm.nih.gov/pmc/arPcles/PMC1122202/ [assessed 29 November 2016]
15. ‘How Neurofeedback Works’, ‘Brainwave Training. Making good brains beDer.’, hDp://measurebrainwaves.com/index.php/how-neurofeedback-works, [accessed 21 February 2017]
16. Jacofsky M.D. et al, ‘Psychological ExplanaPons of Anxiety Disorders’, Rhode Island RISAS Student Assistance Services, hDp://www.risas.org/poc/view_doc.php?type=doc&id=38474&cn=1, [accessed 22 October 2016]
17. Koizumi A. et al., ‘Fear reducPon without fear through reinforcement of neural acPvity that bypasses conscious exposure’, N. Hum Behav.Published online 2016 Nov 21, NCBI PMC US NaPonal Library of Medicine NaPonal InsPtutes of Health, hDps://www.ncbi.nlm.nih.gov/pmc/arPcles/PMC5628620/, [accessed 21 February 2017].
18. Lewis R. D., ‘CogniPve Behavioral Therapy: The Good, The Bad, The LimitaPons’,2013, ‘Mad in America’,hDps://www.madinamerica.com/2013/05/cogniPve-behavioral-therapy-the-good-the-bad-the-limitaPons/, [accessed 25 January 2017]
19. Marx G., Gilon C., 'The Molecular Basis of Memory’, 2012, available fromhDp://pubs.acs.org/doi/pdf/10.1021/cn300097b, [accessed 16 October 2016]
20. Mohagheghi A., A Randomized Trial of Comparing the Efficacy of Two Neurofeedback Protocols for Treatment of Clinical and CogniPve Symptoms of ADHD: Theta Suppression/Beta Enhancement and Theta Suppression/Alpha Enhancement.’, NCBI, PubMed gov., US NaPonal Library of Medicine NaPonal InsPtutes of Health, 2017, hDps://www.ncbi.nlm.nih.gov/pmc/arPcles/PMC5340952/, [accessed 5 May 2017]
21. Moore A., ‘The Many Treatment Methodologies for Phobias: Finding the Best Fit’ ,NYU STEINHARDT,hDp://steinhardt.nyu.edu/appsych/opus/issues/2012/fall/many, [accessed 11 November 2016]

22. Moss D., Kirk L., ‘Evidence-Based PracPce in Biofeedback and Neurofeedback’, ‘applied psychophysiology and biofeedback’,hDps://www.aapb.org/files/public/Yucha-Gilbert_EvidenceBased2004.pdf; p.2 ,[accessed 27 February 2017]
23. Nordqvist C., ‘Everything you need to know about phobias’, Reviewed by Timothy J. Legg, PhD, CRNP, Medicalnewstoday, 2017 hDps://www.medicalnewstoday.com/arPcles/249347.php, [accessed 18 November 2016]
24. Norton m.J., Mochon,D., Ariely D.,’The IKEA effect: When labor leads to love’, 2012, Pages 453-460, Journal of Consumer Psychology, Science Direct,
25. hDp://www.sciencedirect.com/science/arPcle/pii/S1057740811000829, [accessed 6 December 2017].
26. Orosz S., Schwab, Nakataki, Wiest, Federspiel, ‘ CBT reduces CBF: cogniPve-behavioural therapy reduces cerebral blood flow in fear-relevant brain regions in spider phobia’, 2016, PubMed.gov, NCBI, hDps://www.ncbi.nlm.nih.gov/pubmed/27688940, [accessed 15 January 2017]
27. PBS NOVA Documentary ‘Memory Hackers’ 2016, uploaded by maktaba dz, available from hDps://www.youtube.com/watch?v=qyb8Ah3jChw, [accessed 13 November 2016]
28. ‘Phobias’, NHS choices, 2016, hDp://www.nhs.uk/condiPons/phobias/pages/introducPon.aspx [accessed 29 November 2016]
29. ‘RecondiPoning the brain to overcome fear. Researchers have discovered a way to remove specific fears from the brain’, University of Cambridge, AAAS and EurekAlert: The Global Source of Science news’, 2016, hDps://www.eurekalert.org/pub_releases/2016-11/uoc-rtb111816.php, [accessed 22 November 2016]
30. Robbins Mel, ‘The Secret to Stopping Fear and Anxiety (That Actually Works)’ youtube.com, hDps://www.youtube.com/watch?v=6n8i7ua0mSw, [accessed 10 March 2017]
31. Roes N. A., ‘Understand the limits of CBT’ 2011, AddicKon Professional, hDps://www.addicPonpro.com/arPcle/understand-limits-cbt, [accessed 17 November 2016].
32. Shibata K., ‘Perceptual Learning Incepted by Decoded fMRI Neurofeedback Without SPmulus PresentaPon’, NCBI, PubMed gov., US NaPonal Library of Medicine NaPonal InsPtutes of Health, 2009. hDps://www.ncbi.nlm.nih.gov/pmc/arPcles/PMC3297423/, [accessed 3 January 2017]
33. Smethelles Jack (Youtube channel), ‘Snake Phobias Behavioural (Exposure) Therapy’, available from hDps://www.youtube.com/watch?v=zKTpecooiec&t=413s, [accessed 21 November 2016]
34. Smith M., Segal R., Segal J., ‘Therapy for Anxiety Disorders. Cognitive Behavioral Therapy, Exposure Therapy, and Other Options’, December 2017, HELPGUIDE.ORG Trusted guide to mental & emotional health, https://www.helpguide.org/articles/anxiety/therapy-for-anxiety-disorders.htm [accessed

28 November 2016]
35. Soravia LM. et al.CBT reduces CBF: cogniPve-behavioral therapy reduces cerebral blood flow in fear-relevant brain regions in spider phobia’, NCBI, PubMed gov., US NaPonal Library of Medicine NaPonal InsPtutes of Health, 2016, hDps://www.ncbi.nlm.nih.gov/pubmed/27688940, [accessed 24 24 February 2017]
36. ‘Specific phobias’ WebMD < hDps://www.webmd.com/anxiety-panic/specific-phobias#1> [accessed 21 February 2017]
37. ‘Specific Phobias. Treatment’, Perelman School of Medicine of the University of Pennsylvania, Department of Psychiatry PENN BEHAVIORAL HEALTH, hDp://www.med.upenn.edu/ctsa/phobias_treatment.html, [accessed 10 November 2016]
38. Steiner N.J. et al., ‘In-School Neurofeedback Training for ADHD: Sustained Improvements from a Randomized Control Trial’, AAP News and Journals Gateway, 2014, VOLUME 133 / ISSUE 3 hDp://pediatrics.aappublicaPons.org/content/133/3/483.long, [accessed 11 December 2017]
39. Stoeckel L.E. et al., ‘OpPmizing real Pme fMRI neurofeedback for therapeuPc discovery and development.’, 2014, ‘US NaKonal Library of Medicine NaKonal InsKtutes of Health’, NCBI, hDps://www.ncbi.nlm.nih.gov/pmc/arPcles/PMC4141981/, [accessed 21 February 2017]
40. Vitelli R., ‘ImplanPng False Memories. How reliable are memories of abuse "recovered" during psychotherapy?’, PsychologyToday, 2012, hDps://www.psychologytoday.com/blog/media-spotlight/201211/implanPng-false-memories, [accessed 16 October 2016]
41. WaDs A., ‘Why Do We Develop Certain IrraPonal Phobias?’ 2014, ScienKfic American Mind, hDps://www.scienPficamerican.com/arPcle/why-do-we-develop-certain-irraPona/, [accessed 5 November 2016]
42. West A., ‘ManipulaPng Memory through OptogenePcs: A ConversaPon with NeuroscienPsts Xu Liu and Steve Ramirez’, in ConversaPons, Featured Research, Science, ‘thepsychreport’,2014. hDp://thepsychreport.com/research-applicaPon/featured-research/manipulaPng-memory-through-optogenePcs-qa-with-neuroscienPsts-xu-liu-and-steve-ramirez, [accessed 13 November 2016]
43. ‘Why CogniPve-Behavioural Therapy (CBT)? Advantages and Research Support, NaKonal AssociaKon of CogniKve-Behavioural Therapists, hDp://www.nacbt.org/whycbt-htm/, [accessed 20 December 2016]
44. Winerman L., ‘Figuring out phobia. Researchers are using neuroimaging techniques to delve into the neurobiological underpinnings of phobias, with a view to improving

treatments.’, American Psychological AssociaKon, 2005, Vol 36, No. 7, Print version p.96, available from hDp://www.apa.org/monitor/julaug05/figuring.aspx, [accessed 18 November 2016]
45. Wolizky-Taylor, K. B. et al., hDps://www.psychology.org.au/Assets/Files/Evidence-Based-Psychological-IntervenPons.pdf. p.48; (2008). Clinical Psychology Review, 28, 1021-1037, [accessed 18 November 2016]
46. Wright J.H., Davis D.,’ The TherapeuPc RelaPonship in CogniPve-Behavioral Therapy: PaPent PercepPons and Therapist Responses’ 1994, COGNITIVE AND BEHAVIORAL PRACTICE 1, pp. 26-27, Available from hDp://citeseerx.ist.psu.edu, [accessed 10 December 2017]