Embed Size (px)
Citation preview
CAMDEN AND ISLINGTON
NHS FOUNDATION TRUST
MEETING OF THE BOARD OF DIRECTORS
HELD IN PUBLIC
CONFERENCE HALL
ST PANCRAS HOSPITAL
4 ST PANCRAS WAY
LONDON, NW1 0PE
Thursday 28 November 2013 at 2:00pm
Membership: Ms Leisha Fullick, Trust Chair
Ms Wendy Wallace, Chief Executive
Ms Cha Patel, Deputy Trust Chair / Non-Executive Director
Dr Sylvia Tang, Deputy Chief Executive & Medical Director
Mr Richard Brooman, Non-Executive Director
Mr Paul Calaminus, Chief Operating Officer
Ms Sarah Charles, Senior Independent Director / Non-Executive Director
Dr Susan Goss, Non-Executive Director
Ms Angela Harvey, Non-Executive Director
Ms Claire Johnston, Director of Nursing & People
Mr David Wragg, Director of Finance
Mr Colin Plant, Director of Integrated Care (non-voting member)
Enquiries to Trust Board Office Telephone 020 3317 3184 / 3192 Email: [email protected]
1 of 132

C&I Public Board Agenda 28 November 2013
Meeting Ground Rules
a) Apologies for non-attendance or lateness to be provided to the Board Secretary before the meeting. Chair will ask for apologies at the meeting.
b) All actively engage and are individually accountable.
c) Views are listened to and built on constructively.
d) There is mutual respect.
e) The Board works within a climate of giving and receiving constructive challenge (of ideas and not people).
f) Everyone is equal in the process while having regard to role of the Chair.
2 of 132
C&I Public Board Agenda 28 November 2013
PUBLIC BOARD AGENDA
Thursday 28 November 2013
2:00pm
1. GENERAL BUSINESS Time: Page No:
1.1 WELCOME AND APOLOGIES
2:00-2:10pm
Verbal
1.2 DECLARATIONS OF INTEREST 5
1.3 SERVICE USERS’ EXPERIENCE PRESENTATION
A presentation by service users, accompanied by staff 2:10-2:35pm Presentation
1.4
PREVIOUS MINUTES
Minutes from the previous Public Board meeting on 31 October 2013.
2:35-2:40pm 7
1.5 MATTERS ARISING
Matters arising from the previous Public Board meeting on 31 October 2013.
21
2. STRATEGIC / GOVERNANCE
(No Items) - -
3. STATUTORY / REGULATORY
3.1 RESPONSE TO THE KEOGH REVIEW
A paper presented by Ms Claire Johnston 2:40-2:50pm 25
4. OPERATIONAL
4.1 CHIEF EXECUTIVE’S REPORT
A report presented by Ms Wendy Wallace
2:50-3:00pm 33
4.2 FINANCIAL POSITION - MONTH 7, 2013/14
A paper presented by Mr David Wragg
3:00-3:10pm 43
4.3 HUMAN RESOURCES & WORKFORCE PERFORMANCE REPORT – QUARTER 2, 2013
A Report presented by Ms Claire Johnston
3:10-3:30pm 59
4.4 ICT STRATEGY
A paper presented by Mr David Wragg 3:30-3:40pm 73
5 SUB-COMMITTEES
5.1 QUALITY COMMITTEE
Minutes from the Quality Committee Meeting on 2 July 2013
3:50-3:55pm 121
3 of 132

C&I Public Board Agenda 28 November 2013
6. ANY OTHER BUSINESS
6.1 ANY OTHER BUSINESS THAT THE CHAIR CONSIDERS URGENT
3:55-4:00pm -
6.2 NEW RISKS IDENTIFIED DURING THE MEETING OR RISKS REFERRED FROM/TO COMMITTEES
6.3 PUBLIC BOARD PLANNING
(For Information)
6.4
DATE OF THE NEXT MEETING
30th January 2014
7. CLOSE 4:00pm -
4 of 132
25/09/13
Board of Directors – Register of Interests
Board Member: Interest Declared:
Ms Leisha Fullick (Trust Chair)
Governor of City & Islington College.
Ms Cha Patel (Deputy Trust Chair / Non-Executive Director)
Trustee of the Shaw Trust charity; Director of Igloo Consultants Limited; Director, and Finance & Audit Committee Chair, for CityWest Homes; Director, and Audit & Risk Committee Chair, for Gateway Housing Association; and Vice Chair and Audit & Risk Committee Chair, Bromley Healthcare.
Ms Sarah Charles (Senior Independent Director / Non-Executive Director)
Chair of Croydon Care Solutions Ltd; and Married to a Non-Executive Director for Barnet, Enfield and Haringey Mental Health Trust.
Mr Richard Brooman (Non-Executive Director)
Deputy Chairman of Invesco Perpetual UK Smaller Companies Investment Trust plc; Director of HgCapital Trust plc; Director of Acal Plc; Director Governor and Trustee for Merchant Taylors’ School Limited; Founder and Director of Incrementum Limited; Trustee for Leonard Cheshire Disability; and Trustee of the British Youth Opera.
Ms Sue Goss (Non-Executive Director)
None.
Ms Angela Harvey (Non-Executive Director)
Councillor, Westminster City Council. Married to a Westminster City Councillor, who is currently the Adult, Heath, Community Protection Policy & Scrutiny Chair.
Ms Wendy Wallace (Chief Executive)
Trustee for Interactive – a charity for inclusion in sport; and Married to a Director of CareTech plc – provider of community care & children’s services.
Dr Sylvia Tang (Deputy Chief Executive / Medical Director)
Psychiatric Advisor to CARIS Bereavement Counselling Service; and Non-Executive Director for Vision Mental Health Care.
Mr David Wragg (Director of Finance)
Married to the National Development Lead at the Healthcare Quality Improvement Partnership (HQIP), which is a charity and a company limited by guarantee that promotes clinical audit and has contracts with the Department of Health and NHS Bodies.
Ms Claire Johnston (Director of Nursing & People)
None.
Mr Paul Calaminus (Chief Operating Officer)
Married to the Assistant Board Secretary at the Department of Health.
Non-Voting Board Member: Interest Declared:
Mr Colin Plant (Director of Integrated Care)
Trustee for Ponayi - a charity that provides health support and advice for people from South African origin.
5 of 132

6 of 132

MINUTES OF A MEETING OF THE
CAMDEN AND ISLINGTON NHS FOUNDATION TRUST
BOARD OF DIRECTORS HELD IN PUBLIC IN THE
CONFERENCE HALL, ST PANCRAS HOSPITAL,
ST PANCRAS WAY, LONDON, NW1 0PE.
ON THURSDAY 31 OCTOBER 2013 AT 2:00pm
Board Members Present:
Ms Leisha Fullick Chair
Ms Wendy Wallace Chief Executive
Ms Cha Patel Deputy Chair / Non-Executive Director
Dr Sylvia Tang Deputy Chief Executive and Medical Director
Ms Sarah Charles Senior Independent Director / Non-Executive
Mr Richard Brooman Non-Executive Director
Dr Sue Goss Non-Executive Director
Mr David Wragg Director of Finance
Ms Claire Johnston Director of Nursing and People
Mr Paul Calaminus Chief Operating Officer
Mr Colin Plant Director of Integrated Care (non-voting member)
In Attendance:
Mr Kevin Monteith Associate Director of Strategy and Corporate Development / Trust Secretary
Ms Paulina Wolan Interim Board Administration Assistant (items 1.122.13 – 1.127.13, and 1.129.13 only)
Ms Susan Harrison Interim Head of Learning Disabilities Services, London Borough of Camden (item 1.134.13 only)
Mr David Cotson Lead Clinician and Clinical Psychologist, Camden Learning Disabilities Service (item 1.135.13 only)
Ms Sue Powell Head of Learning Disabilities Services, London Borough of Islington (item 1.134.13 only)
Ms Dawn Southgate Team Manager, Learning Disabilities, London Borough of Islington (item 1.135.13 only)
Mr Martin Zielinski Board Secretary (Minutes)
This meeting was open to the public
7 of 132

Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 2 of 14
GENERAL BUSINESS
1.122.13 WELCOME, APOLOGIES AND QUORACY
Ms Fullick welcomed those present. Apologies had been received from Ms Angela Harvey, Non-Executive Director. The meeting was quorate.
1.123.13 DECLARATIONS OF INTEREST
The schedule of declared interests was noted and no amendments were notified. The Board were satisfied that there was no conflict between these declared interests and any item on the agenda.
1.124.13 MINUTES OF THE MEETING OF THE BOARD OF DIRECTORS HELD IN PUBLIC ON 26 September 2013
The Board reviewed the minutes from its last meeting and agreed one minor amendment.
The Board AGREED the minutes of its previous meeting on 26th September as a true and correct record, subject to the agreed amendment.
1.125.13 MATTERS ARISING
The Board considered the matters arising from its previous meeting on 26 September 2013. These were considered to have been completed, or covered elsewhere on the agenda, with the exception of - It was agreed that the updated report on London Mental Health
Act activity would, when available, be taken to a relevant Committee rather than come back to the Board.
Details of the final cost of implementing automated pension enrolment would be included in the Finance Report to the November Board.
Ms Charles stated that the provision of positive evidence detailing other Trusts’ usage of DBS checks had not been included in the Governor e-mail as stated. Ms Fullick asked that this action be re-visited.
Ms Johnston confirmed that examples of patient experience were on track to be reported at the next meeting of the Board.
Mr Plant
Mr Wragg
Mr Zielinski
STRATEGIC / GOVERNANCE
1.126.13 MONITOR FINANCE DECLARTION – QUARTER TWO, 2013/14 (1 JULY – 30 SEPTEMBER 2013)
(See item 1.129.13 below)
8 of 132

Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 3 of 14
1.127.13 MONITOR GOVERNANCE DECLARTION – QUARTER TWO, 2013/14 (1 JULY – 30 SEPTEMBER 2013)
Dr Tang introduced this paper drawing the Board’s attention to the fact that all of the service performance targets and indicators had been met during quarter two. It was advised that a CQC report had been received the previous day in relation to a recent inspection of a care pathway in Camden. It was reported that two moderate concerns had been noted, out of seven assessed standards, and that robust action plans were already in place to address these concerns. It was highlighted that these concerns, under the new risk assessment framework, did not mean that the Trust would have a ‘red’ governance rating. Dr Tang recommended that the Board approve the Trust’s Governance Declaration for quarter two, 2013/14. With reference to the section of the report detailing the recent election results, Ms Charles noted that the Trust only had 261 eligible service user votes and queried why service users were not automatically made members, unless they chose to opt out, as was the case with staff members. Mr Monteith advised that this issue is complex and raises issues in relation to consent and capacity and that a wider discussion would be required regarding the introduction of such a change. Ms Charles stated that she would discuss this matter further with Mr Jonathan Fisher, the Trust’s Interim Membership Manager. Mr Brooman referred to the action plans to address the CQC’s concerns and asked how these would be reported and monitored. Ms Johnston advised that a group would meet weekly to monitor progress against the required actions and that this group would report to the Quality Committee. She assured Mr Brooman that relevant risks were already recorded in the Trust’s risk register. Ms Wallace assured the Board that actions to address the CQC’s concerns were already underway. Ms Fullick queried whether the listed examples of exception reporting were exhaustive, or if there were other potential exceptions of which the Board should be aware. Mr Monteith advised that the examples given fully reflected Monitor guidance and that there were no other areas of concern to report, although this list could be added to in future, should such action be necessary. The Board APPROVED the Governance Declaration to Monitor of quarter two, 2013/14.
Ms Charles
OPERATIONAL
1.128.13 CHIEF EXECUTIVE’S REPORT
Ms Wallace provided an update on activity in, and affecting, the Trust since the Board’s last meeting. She highlighted several points. With regards the appointment of Monitor’s next Chair, she advised that, since she had written her report, the situation had changed as the Health Select Committee had not supported his
9 of 132

Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 4 of 14
appointment, Mr Dodds has subsequently withdrawn from the process and has not been appointed as the new Chair of Monitor, as detailed in her paper. She added that Mr Dodds would continue as Chair at the Royal Free NHS Foundation Trust. It was advised that Mr Simon Stevens had just been appointed as the Chief Executive for NHS England and would take up this post on 1 April 2014. The Board was advised that there remained a lack of clarity over how ‘Patient Choice’ would be introduced in mental health services, although the Department of Health had indicated that it should take effect from 1 April 2014. Ms Wallace cautioned that changes related to ‘Patient Choice’ could be introduced quite quickly after this due implementation date and management needed to stay alert to this and any possible effects this may have. Ms Wallace advised that she had been invited to present to the London Leadership Group on acute bed pressures in London. Ms Fullick asked if this was an NHS group and was advised it consisted of both NHS and local authority members. It was a senior strategic group. In relation to the development of the St Pancras site, Ms Wallace advised that the Trust was considering a number of potential partners to take forward future site developments. The Board were advised that a new ‘iCope’ website had been successfully launched to raise awareness about the Trust’s IAPT services. Mr Richard French-Lowe, Training Manager, was commended for winning the CMI’s national Training and Development Manager of the Year, 2013. Mr Brooman added that this was a fantastic achievement which should be openly celebrated by the Trust. Ms Fullick requested that the minutes record the Board’s congratulations to Mr French-Lowe and their pride in his achievement. Ms Wallace added that, in addition to the items in her paper, a number of Board members had recently attended a research and development showcase event that had been very interesting and worthwhile.
The Board of Directors NOTED the Chief Executive’s Report.
1.129.13 FINANCE POSITION – MONTH 6, 2013/14
This item was taken after the matters arising as this finance paper included the information required for the Monitor declaration. (Item 1.126.13 above) Mr Wragg presented this update advising that, halfway through the year, the Trust was £254k ahead of plan on income and expenditure. In addition, a £1.6m gain on sale had been received from the disposals of Fordwych Road, Ashley Road and Cleveland Street. He advised that the ‘EBITDA’ was ahead of target and that the planned QIPP was expected to be delivered. He drew the Board’s attention to the fact that the Monitor quarter 2 return had shown unplanned decreases in the ‘EBITDA’ margin over the last
10 of 132
Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 5 of 14
two quarters. However, he advised that this reflected an error in Monitor’s spreadsheet where it reported actual instead of planned figures. The Trust’s performance was ahead of plan for both Quarters 1 and 2, although Quarter 2 was marginally less than Quarter 1. The Trust’s liquidity was as expected, with £7.5m in the bank and £42m invested in the National Loan Funds. He added that this should ensure that the Trust retained its risk rating of ‘3’ or more over the next year. Mr Brooman queried if Mr Wragg had notified Monitor of the error in their spreadsheet. Mr Wragg responded that the Deputy Director of Finance would do so when submitting the Trust’s quarterly return. Ms Patel advised that the Trust’s financial position had previously been discussed in detail by the Finance and Estates Committee. She had been pleased to note the positive financial position that the Trust was in and acknowledged the hard work by staff in achieving this. Mr Brooman commented that it had been previously reported that capital expenditure was behind plan and that the Trust had re-submitted its capital plan to Monitor. He queried if activity was still behind plan as it was of note that the retained cash balance continued to increase. Mr Wragg advised that backlog maintenance had been less costly than expected and the development of the new crisis house was behind plan. He added that the Trust advised Monitor of this position and submitted a new capital plan before the Trust exceeded Monitor’s trigger point, 15% divergence from plan. At Quarter 2, the Trust is back within tolerance. Ms Wallace added that there had been a recent increase in capital works, advising that tenders were now being signed off on a regular basis. Ms Fullick queried whether slippage in capital works was the norm. Mr Wragg advised that there was still some slippage, which was not unexpected with a capital programme twice the normal size. He added that current slippage was not material enough to trigger Monitor’s concern and would be caught up in the following months. Mr Wragg recommended to the Board that the Trust declare that that it ‘will continue to maintain a financial risk rating of at least 3 over the next year’, which was agreed. The Board of Directors NOTED the financial update as at month 6, 2013/14 and APPROVED the Finance Declaration to Monitor of quarter two, 2013/14.
Mr Wragg
1.130.13 BOARD PERFORMANCE REPORT
Ms Johnston presented this report which summarised the Trust’s performance during the second quarter against a range of national and commissioner requirements and benchmarks. She was pleased to report that a large number of the required targets had been met or exceeded. She highlighted that all Monitor targets had been met during the quarter, as they had been for the previous 12 months, and that all local authority delegated targets were expected to be met by the end of the year. It was advised that the CQC had just concluded a consultation on
11 of 132

Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 6 of 14
its review process. The Board noted that a recent review in Camden (see 1.127.13 above) had mainly followed the expected new inspection framework. Ms Johnston added that staff and service users had provided positive feedback on their inspection experience. In relation to safety, Ms Johnston advised that the Trust was still considered a low reporter, in terms of incidents, but that work was underway to encourage divisional reporting and improvements have been made to the ‘datix’ incident recording system. It was considered that low reporting was more prevalent in inner city trusts where staff were more acclimatised to verbal abuse and did not consider this a matter to be reported. Ms Johnston was confident that a current campaign to increase reporting would show evident improvements in the next quarter. In relation to the CQC’s Quality Risk Profile, the Board were advised that the Trust was rated as ‘similar or better than expected’ against 717 out of 763 measures (94%). Ms Johnston advised that the CQC had undertaken three Mental Health Act monitoring visits during August, which was slightly more than normal. A full action plan had been generated as a result of each visit and progress against these was being monitored by the Mental Health Law Group. It was advised that the format of the ‘New Outcome Reporting’ had been improved, based on the Board’s previous feedback. Mr Calaminus added that this diagram aimed to concisely show the amount of work underway on one page. He explained how the diagram should be read. Ms Wallace added how the appendices to this paper gave more detail behind the diagram and highlighted how reporting had become more sophisticated. Ms Charles was pleased to note this fact, and that statistical evidence was beginning to be reported. Dr Tang commented that the provided table demonstrated acute services and should be taken as an example of the new reporting system being trialled. She added it was interesting to note that it showed service users, whilst their symptoms were diminished, experienced reduced social functioning after an acute episode and that had not been as obvious previously. In relation to SUI investigations, Ms Johnston advised that a newly agreed review process was now in place to allow the Trust to meet new tighter reporting deadlines. Ms Johnston drew attention to the risks detailed in the report and stated that the status looked worse than the actual position, mainly due to time lags in reporting. She gave the CDAT patient flow as an example, advising that this ‘red’ rated risk would actually be ‘amber’ or ‘green’ if it were to be reviewed today. It was highlighted that there had been an increase in the number of complaints. This was not unexpected due to the current pressures on services and measures were in place to ensure that required response times were being met. Bed occupancy rates were reported to be approximately 94.2%, which was above the target of 85% set by the Royal College of Psychiatrists. Ms Johnston advised that while, this had been a challenging quarter, staff had managed the pressures well.
12 of 132

Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 7 of 14
It was highlighted that the Trust was rated ‘amber’ in relation to the annual independent service users survey, although it was rated ‘green’ for providing at least four activity sessions for service users each week. Ward staff were praised for their positive and imaginative approach to inpatient service user activities. Mr Calaminus gave an update on the Assessment Service and IAPT. He advised that performance had improved in Camden but dipped in Islington. He added that Productivity Consultants had been engaged to work with the relevant teams, improve performance, and that daily reviews were being conducted to review capacity requirements over the next two week period. He advised that 100% of referrals in the last two weeks had been assessed within 10 days and, where it was taking 48 hours to acknowledge referrals six months ago this was now being achieved within 3 hours. In relation to the table of IAPT performance, Mr Calaminus advised that this related to quarter two, not quarter one as detailed in the table’ headings. He added that a working group had been established with the aim of improving recovery rates, as the national target of 50% was still not being met. The Trust was also working with commissioners with a view towards reaching this target. It was advised that there had been some transitional issues with service provision in Kingston over the summer. Mr Calaminus stated that the IAPT services engaged a large number of graduate psychologists, a large number of which left over summer after successfully gaining training places, causing a backlog in the provision of psychological services. Elsewhere this is planned for by over recruiting in April/May but this had not been possible when taking on this new service. It was, however, reported that this issue had not negatively affected recovery rates in Kingston. Ms Charles asked what action was being taken to address the backlog and Mr Calaminus advised that weekend groups were being held. Ms Johnston advised that 799 incidents had been reported during quarter two and updated the Board on the Trust’s performance against its CQUIN indicator targets. It was confirmed to Ms Fullick that responses to complaints and incidents were carefully monitored. Ms Johnston moved on to the Quality Account priorities for 2013/14 and was pleased to advise how well performance was going against the Trust’s six chosen themes. It was noted that consultation on next year’s quality priorities had already begun and would include increased input from stakeholders. The Board’s attention was drawn to the ‘Divisional Performance Ratings’ report, being the first time that this new reporting framework had been presented. Ms Johnston stressed how this chart highlighted areas of strong and weak performance on a monthly basis, allowing management action to be targeted at the latter. Ms Johnston added that each stated RAG rating was made up of a number of different indicators and that the presented data was very current, reflecting the previous week’s position. Ms Charles assumed that Directors were aware of the detail behind these ratings and asked if, where a category was ‘amber’ or ‘red’ over several months, whether this reflected an on-going weakness or different issues arising and being resolved underneath a
13 of 132

Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 8 of 14
consistent rating. Mr Calaminus responded that either situation could exist and highlighted that some underlying measures, such as waiting times, may not change on a monthly basis as outcome data was reliant on quarterly reporting. Ms Charles noted that ‘the Substance Misuse Service’ was performing the best in terms of finance and quality and queried why this was the case. Mr Calaminus advised that this service had undertaken a lot of work on recruitment and mandatory training, while having a strong focus on the recovery model and forward planning, looking 12-18 months ahead. He confirmed to Ms Charles that those teams that were not working so effectively were learning from those that were. Ms Fullick noted that the report’s executive summary detailed a comprehensive list of concerns and suggested that it would be helpful if the cover sheet was used to focus the Board’s attention on 4-5 key issues. The Board of Directors NOTED the Performance Report for quarter two, 2013/14.
Ms Johnston
1.131.13 EMERGENCY PLANNING AND RESILIENCE ANNUAL REPORT 2012/13
Mr Calaminus presented this report, which was supported by two large appendices that had been circulated for background information and not included in the meeting’s papers. Mr Brooman commented that if a document related to an agenda item then it should be in the pack, otherwise members may not have read them. Mr Calaminus advised that the Trust needed to have processes in place to respond to local and London-wide incidents. This was a CQC and Monitor licence requirement. The Trust’s six main duties under the ‘Civil Contingencies Act’ were detailed to the Board, along with a number of emergency planning risks that the Trust may face. The Board were assured that the Trust had appropriate major incident and business continuity plans in place, with the latter being enacted more frequently. It was explained that existing plans had been written on the basis of historic british standards and were now required to be reviewed to reflect new standards. This piece of work would be undertaken over the next few months. It was also highlighted that the Trust had a duty to co-operate with other agencies, and share relevant information, to ensure emergency preparedness. It was noted that two London-wide emergency planning and resilience exercises had recently taken place, along with an internal table top exercise. It was noted that a need had been noted to rediscover command and control channels following the recent NHS restructuring and the dissolution of PCTs. Ms Charles queried the outcome of the stated two recent London-wide exercises. Mr Calaminus advised that the first exercise went well and that the second had highlighted that CCGs did not have a regional response role, but did hold a significant amount of local knowledge should an emergency arise. It was confirmed to Mr Brooman that existing plans covered all potential civil contingencies
14 of 132
Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 9 of 14
and that any newly identified risks would be appropriately incorporated into the Trust’s risk registers. Ms Fullick concluded that the Trust did have relevant plans in place but that they were not fully compliant with new ISO requirements. Mr Calaminus agreed that this was the case but that, as stated, work was underway to bring Trust plans in line with all new ISO requirements. He also confirmed that these plans were reviewed on at least an annual basis. Mr Brooman commented on the reported breakdown of NHS command and control and suggested that, should a major incident occur, poor national action may negatively reflect on this Trust. He requested that this reputational risk be considered for the risk register until this issue was resolved. Ms Patel was pleased to see that there were processes in place to deal with emergencies but, since C&I is a Foundation Trust with a degree of independence, queried whether the Board should have a more active role in ensure emergency preparedness. Mr Calaminus advised that the Trust had its own internal response processes in place. Mr Brooman asked how many incidents, covered by such plans had occurred in the last 24 months. Mr Calaminus stated he had not been with the Trust that long but that there had been seven incidents in the last six months, such as a fire, adverse weather and transport disruption. In each case business continuity plans were in place to deal with such incidents.
The Board of Directors NOTED Emergency Planning and Resilience Annual Report 2012/13
Mr Calaminus
1.132.13 INFORMATION GOVERNANCE ANNUAL REPORT 2012/13
Mr Wragg presented this report which included details of received FoI requests and how these had been dealt with by the Trust. He highlighted that the Trust’s rating on the IG Toolkit was unsatisfactory, due to the fact that the mandatory target for information governance training had been missed by 2-3%. He advised that e-learning and awareness training were being pursued to manage an increased uptake of this training. It was noted that the Version 10 submission of the IG Toolkit had been in 2013, not 2012 as stated in the report. Ms Charles commented that the Trust had failed against the toolkit for two successive years. Mr Wragg concurred that this was the case, adding that the failure margin was less in the latter year. Dr Tang advised that the requirements of the toolkit changed each year and that the required level of full in-year training was difficult to achieve. She added that there were no material consequences to failing against the toolkit and that the Trust needed to balance the cost of resourcing improvements against any potential benefits achieved. Ms Wallace added that the toolkit was not risk based and did not highlight any gaps in information governance that may actually affect service users or staff. Ms Fullick asked why, with little consequence, the Trust undertook the toolkit assessments. Dr Tang advised that it was required to do so and to submit the results
15 of 132

Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 10 of 14
to the Information Commissioner. Ms Patel stated that she had been alerted, at a recent presentation, to the risk of cyber-attacks and had raised this at the Finance & Estates Committee. She suggested that it would be assuring if controls against such attacks were covered by future IG Toolkit self-assessments. It was acknowledged that the requirements of each year’s assessment were set externally. Dr Goss queried what would be the most efficient way to achieve compliance with the IG Toolkit. Dr Tang advised that e-learning was cheaper and less disruptive to staff and that was why it was being promoted. Mr Wragg concluded by advising that the Trust’s auditors annually reviewed its self-assessment against the IG Toolkit. The Trust’s performance had been rated as average. He added that the Trust maintained a good relationship with the office of the Information Commissioner. Ms Charles highlighted that the Trust was required to publish its FoI statistics on a monthly basis. Mr Wragg advised that this was the case and the required data was available on the Trust’s public website. The Board of Directors NOTED the Information Governance Annual Report, 2012/13.
1.133.13 RESEARCH AND DEVELOPMENT ANNUAL REPORT 2012/13
Dr Tang was pleased to present this report to the Board, highlighting that the Trust was second only to the South London and Maudsley NHS Foundation Trust in attracting mental health research grants. It was also fifth, out of 31 mental health trusts, in receipts of research capacity funding. The Trust actively supported; research; funded research posts; and hosted DeNDRoN (a network that supports research delivery in neurodegenerative diseases such as Parkinson’s, Huntington’s and Alzheimer’s). The Board were advised that there had been a reduction in recruitment to research trials in the last year. This reflected the national position but it was also noted that trials tended to operate on a cyclical basis, with periodic periods of recruitment. Dr Tang was pleased to advise that research income had continued to grow in the last three years. This was especially of note because it had been expected that income would decrease when block funding ceased. The Trust had actually increased its funding by £1m. It was also of note that research conducted within Trust had made a significant impact on NICE and overseas guidance. The Trust was best known for its service model research, along with work in areas such as dementia and learning disabilities. Looking forward, it was advised that the Trust was starting to develop evidence to verify its impact on, and service delivery within, social care. The Board’s attention was drawn to the details of major research grants received in 2012/13 and the 123 publications related to Trust
16 of 132
Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 11 of 14
based work during 2012. Mr Fullick thanked Dr Tang for the report and stated how research and development work had really been brought to life for those Board members who attended the research and development event the previous week. Dr Goss congratulated the Trust on its research and development successes and was pleased to see its work was having an external impact. She supported this positive news being shared with the Trust Governors and membership. Ms Charles added that it was terrific to see that the Trust’s research work was so practical and applicable to service users. Ms Patel stressed the importance of feeding back to stakeholders on the Trust’s research successes as the hard work and dedication of a small number of individuals made such achievements possible and their work should be celebrated. It was also noted that such work materially enhanced the Trust’s reputation and attracted high calibre staff and further research. Ms Fullick asked if there were any risks to the Trust maintaining this position. Dr Tang responded that there were no concerns that the Trust would not continue to be successful in this field and attract research in the medium term. She added that she was frequently approached by those interested in bringing their research work to the Trust. The Board of Directors NOTED the Research and Development Annual Report 2012/13.
Dr Tang
1.134.13 CAMDEN LEARNING DISABILIITIES 2013
Mr Plant introduced Ms Harrison and Mr Cotson to present this annual report on the learning disabilities service which had been delivered in partnership by the London Borough of Camden and the Trust during 2012/13. Ms Harrison gave some context to the report advising that in a borough, such as Camden, there were 5,000 people with an IQ of less than 70, with 2,500 considered to have learning disabilities. There were 600 people in specialist services at any one time, with £2m spent on staffing to deliver £23m worth of services. The service was fully active in research and fully participative in the development of national, evidence based guidelines. Ms Harrison made reference to the impact of the Winterbourne review on how services were delivered. She highlighted that Camden had no clients placed at this service but it had made them think about their approach to placing service users in distant specialist services, with more focus on the quality of care provided. Mr Cotson added that the impact of Winterbourne could not be underplayed and that the service was increasing its oversight on distant services and re-shaping the planning of care for those with similar needs. Looking forward, Ms Harrison outlined how the borough was progressing to establish S75 agreements with NHS partners and had produced a DVD to recruit trainee psychiatrists. Work was also being undertaken with the national development team to create a
17 of 132

Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 12 of 14
health equalities tool with the aim of obtaining some form of evident measure of how learning disability services were positively impacting on service users. Dr Tang thanked the presenters for an interesting report, which included references to clinical audit. She queried the clinical audit process used and how it related to the measures and standards used by the Trust for such reviews. Ms Harrison advised that there probably were variances in the approaches adopted but that performance teams were working to address this. Mr Brooman queried the number of service users being treated in remote locations. Mr Cotson advised that there were a number of individuals in specialist healthcare placements, with 5 currently in the cohort similar to Winterbourne View. He added that there were a further 13-14 individuals in out-of-borough care with continuing healthcare funding. Ms Harrison added that residential care was not pursed for those with learning difficulties unless such care was absolutely essential. Ms Wallace advised that the majority of those affected by the events at Winterbourne View should not have been placed there. She highlighted the need to provide services locally with appropriate health and social care support. She stated that giving care was not just a case of providing accommodation and that a whole range of support workers had to be skilled up to deal with those with complex needs. Ms Harrison agreed, advising that 3 service users had recently been brought back into the borough and were being cared for locally. Mr Cotson added that significant work was being undertaken to retain service users within the borough and active support training programmes were in place with local providers. Ms Wallace asked if local providers were being supportive of these aims and Mr Cotson confirmed that this was the case. Dr Goss, referring to the number of potential service users stated at the start of this presentation, queried if there was further preventative work that the Trust should be doing. Ms Harrison advised that the aim was not to label those with low IQs or interfere in their lives, whilst acknowledging that events may occur that resulted in such individuals needing a period of support. Discussions were underway with CCGs to establish how primary care supported learning disabilities and that the Trust may wish to engage in such discussions. Ms Fullick thanked Ms Harrison and Mr Cotson for presenting Camden’s report. The Board of Directors NOTED the Camden Learning Disabilities Report, 2012/13.
1.135.13 ISLINGTON LEARNING DISABILITIES 2013
Mr Plant introduced Ms Powell and Ms Southgate to present this annual report on the learning disabilities service which had been delivered in partnership with the London Borough of Islington and the Trust during 2012/13. Ms Powell advised that Islington had a similar profile to that of its
18 of 132
Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 13 of 14
neighbouring borough, Camden. Islington were in the process of reviewing its S75 arrangements, including those involving clinical governance and CQC registration requirements. It was highlighted that services were delivered through two specialist multi-disciplinary teams focussed on mental health or forensic needs; and those with challenging behaviour. Ms Powell took the report as read and invited questions from the Board. Ms Johnston thanked the presenters for a fascinating report. She queried the references to a ‘virtual team model’. Ms Powell acknowledged that this title was confusing as the service team actually meet face to face following ward rounds to discuss the inpatient and community service users and their care. She proposed that the term ‘virtual’ would be dropped when S75 arrangement were refreshed. Ms Wallace stated that there had been much discussion of physical healthcare needs and queried whether arrangements were in place. She considered that working links with healthcare were the best they had been with a learning disabilities champion GP now in post. It was advised that the borough was also working closely with the neighbouring borough of Haringey. Ms Powell highlighted the development of ‘health passports’ for learning disabilities service users, which they could take with them when attending primary care. These were somewhat bulky at present but they were still being developed and explained to acute services providers how to communicate effectively with the relevant learning disabilities service user. Ms Wallace asked if there were plans for both boroughs to work more closely together to provide one coherent service. Ms Powell responded that the boroughs did work together and that the degree of joint working was increasing with some posts already merged and plans in place to roll this out to some nursing posts. She hoped to see closer working relationships in the future but advised that this would be dependent on the political will of both boroughs. Dr Tang asked a question related to clinical audit and its relationship to the work of the Trust. Ms Powell responded that some reviews should be readily accessible and comparable to Trust audits as these were conducted on RiO, the system used by the Trust. She added that a significant amount of work was underway to improve access to RiO within the borough and to refresh research and development arrangements, which should increase the amount of audit activity relevant to and useable by both parties. Ms Fullick thanked Ms Powell and Ms Southgate for presenting Islington’s report The Board of Directors NOTED the Islington Learning Disabilities Report, 2012/13.
SUB-COMMITTEES
1.136.13 (There were no new sub-committee minutes due since the last meeting of the Board.)
19 of 132
Minutes of the Public Board Meeting on 31October 2013 Version: DRAFT ver.2
Page 14 of 14
I certify that these are fair and accurate minutes of the stated meeting. ……………………………..…… ……………………. (Trust Board Chair) (Date) Note: Minutes are numbered sequentially throughout the calendar year.
OTHER BUSINESS
ANY OTHER BUSINESS THAT THE CHAIR CONSIDERS URGENT
1.137.13 No other matters of urgent business were raised at this meeting.
RISKS IDENTIFIED DURING THE MEETING OR RISK REFERRED FROM/TO OTHER COMMITTEES
1.138.13 The Committee noted the following risks for notification to the Risk Management Team for review: The risk to the security of the Trust’s data and its ability to
operate services from potential cyber-attacks; and The potential reputational risk should a major incident occur
while there were command and control concerns in relation to nation and local emergency and resilience plans.
1.139.13 PUBLIC BOARD PLANNING DOCUMENT
The Board was requested to note the plan and advise any required changes to the Board Secretary.
DATE OF NEXT MEETING
1.140.13 28 November 2013.
CLOSE
1.121.13 The Chair declared the meeting closed at 4:15pm.
20 of 132

Matters Arising from C&I Board Meeting (Public) 31 October 2013 Page 1 of 3
MATTERS ARISING FROM THE BOARD MEETING HELD IN PUBLIC
On 31 October 2013 Minute
No. Matters Arising:
Action Owner:
By When:
Update/Status:
1 1.125.13 Matters Arising from 26th September 2013
Mr Plant is to take the updated report on London Mental Health Act activity to a relevant Committee rather than the Board.
Mr Plant
To Be Advised
Will be taken to a Committee when ready.
2 1.125.13 Matters Arising from 26th September 2013
Mr Wragg is to include the details of the final cost of implementing automated pension enrolment in the Finance Report to the November Board.
Mr Wragg
21/11/13
Completed – this is included in the November Board Report.
3 1.125.13 Matters Arising from 26th September 2013
Mr Zielinski is to re-visit an earlier action around providing Governors with evidence of other Trusts making use of DBS checks for Governors
Mr Zielinski
21/11/13
Completed – Governors were provided with this evidence in a Governor email sent on 08/11/2013.
21 of 132

Matters Arising from C&I Board Meeting (Public) 31 October 2013 Page 1 of 3
Minute
No. Matters Arising:
Action Owner:
By When:
Update/Status:
4 1.127.13 MONITOR GOVERNANCE DECLARTION – QUARTER TWO, 2013/14 (1 JULY – 30 SEPTEMBER 2013)
Ms Charles is to discuss the possibility of automatic enrolment of service users as Trust members with Mr Jonathan Fisher, Interim Assistant Board Secretary and Membership Manager.
Ms Charles
21/11/13
Completed
5 1.129.13 FINANCE POSITION – MONTH 6, 2013/14
The Deputy Director of Finance is to notify Monitor of an error in their spreadsheet, when submitting the Trust’s quarterly return.
Mr Wragg
21/11/13
Completed
6 1.130.13 BOARD PERFORMANCE REPORT
Ms Johnston to ensure that the executive summary on the cover sheet used for the Board Performance Report focuses the Board’s attention on 4-5 key issues, rather than providing a comprehensive list of concerns.
Ms Johnston
20/01/14
Action underway to revise report, with full expectation of completion by Board deadline.
7 1.131.13 EMERGENCY PLANNING AND RESILIENCE ANNUAL REPORT 2012/13
Mr Calaminus is to consider for the risk register the reputational risks associated with the breakdown of command and control in the event of a major incident.
Mr Calaminus
21/11/13
Completed – Risks notified to Head of Risk and Patient Safety on 11/11/2013
22 of 132

Matters Arising from C&I Board Meeting (Public) 31 October 2013 Page 1 of 3
8 1.133.13 RESEARCH AND DEVELOPMENT ANNUAL REPORT 2012/13
The news about research and development successes is to be shared with the Trust Governors and members.
Dr Tang
21/11/13
Completed – a feature on the recent Research and Development Conference will be included in future newsletters to Governors and the membership. This will also be included in the Trust’s Annual Report.
23 of 132

24 of 132
Report To: Board of Directors (Public)
Paper Number: 3.1
Report For: Information
Report Type: Quality Governance
Date: 28 November 2013
Report Author: Claire Johnston, Director of Nursing and People
Report of: Claire Johnston, Director of Nursing and People
FoI Status: Report can be made public
Title: The Keogh Mortality Review and roles, responsibilities and
accountability in the New NHS Architecture for system wide quality. Executive Summary
This paper informs the Board of the outcome of the Chief Medical Officer, Bruce Keogh’s review of the quality of care and treatment provided by NHS trusts that were persistent outliers on mortality indicators. All 14 trusts were found to have performance concerns in six key areas, determined by extensive review of available data and soft intelligence as being the most significant reflectors of performance. A ‘data pack’ was built on each trust for:
Mortality;
Patient Experience;
Safety;
Workforce;
Clinical and Operational Effectiveness; and
Leadership and Governance.
The findings and recommendations of the Keogh review are considered, with a particular focus on the use of specific methodologies by the inspection team to maximise quality scrutiny, which the trust is now considering for adoption as part of its own adjustment to the new quality regulatory framework. Specifically these were
i) the use of a Rapid Responsiveness Review and Report, which provided each trust with findings, data and the basis of a turnaround plan;
ii) Risk Summit Action Plan, through which the inspectors and the trust produced a timed response; and
iii) the use of ‘Special Measures’ as an open and transparent means of making sure each trust produced a meaningful Improvement Plan.
As part of the response to Keogh, the combined regulatory and accountable bodies for health care in England have published a joint statement on how the wider system should respond to future quality challenges and ensure effective working together and clarity of roles and accountabilities.
25 of 132
2
The impact of this statement locally along with the implications from the findings and recommendations of the Keogh Review for the trust are also briefly considered. Further detailed work arising from the inspection review will be progressed by the Director of Nursing and People and Deputy Chief Executive and Medical Director and their respective teams in quality assurance and regulation and governance, accounting to the Quality Committee.
Recommendation to the Board:
The Board of Director is requested to:
note the report.
Trust Strategic Priorities Supported by this Paper
Excellence
E1 Continually improve the quality and safety of service delivery, service user experience and improving outcomes.
E2 Delivering the highest level of quality and financial performance.
Innovation
I1 Rapidly adopt best practice and maintain a culture of innovation in service development.
Risk Implications
Board Assurance is provided that the trust is preparing appropriately for the new regulatory expectations. There is a risk for health and social care providers that the commitments and ambitions in response to the Keogh and Francis Inquiry in particular, are not coherent with the NHS financial strategy.
Legal and Compliance Implications
The paper reinforces the Trust’s legal obligation to ensure quality is at the heart of service provision and that patient safety is the Trust’s primordial objective as per the requirements of the Health and Social Care Bill, (2012) and the Trust’s terms of authorisation.
Finance Implications
To meet and stay ahead of the expected response to the Keogh – and other recent quality reviews – additional resources for posts to work in quality compliance and regulatory management have been proposed through the ‘invest to save’ fund.
Single Equalities Impact Assessment
All of the Trust’s services give consideration to equality of access taking into account all characteristics of the equality act. All impacts are dealt with in a fair and equitable way regardless of ethnicity, disability or religion of patients.
Requirement of External Assessor/Regulator
There are no requirements to present this report to regulatory bodies but the discussion and action emanating from it will form part of our approach to both our Quality Account for 14/15 and our quality performance review of contracts with commissioners.
26 of 132

3
The Keogh Mortality Review
Professor Sir Bruce Keogh, Chief Medical Officer, published a detailed report of the care and treatment of patients in fourteen English acute trusts in July 2013. He summarised them, despite finding pockets of excellence, as being ‘trapped in mediocrity’ with staff who lacked the confidence to achieve excellence and boards who could not understand how to oversee and interpret quality assurance information. The review was initiated by the Prime Minister in February 2013 and trust’s to be investigated were selected because they had been outliers for the previous two years, on either the Summary Hospital Level Mortality indicator or the Hospital Standardised Mortality Ratio. Broadly this data showed that they had experienced avoidable deaths of patients. This then led to an inspection of each of the trusts with teams of experienced clinical and managerial staff, using a variety of approaches, which have been considered ground breaking.
The trust board has considered the changing regulatory regime throughout 2013, and we have assessed the implications for the trust of a more stringent quality assurance framework as set out by Monitor in April 2013. The board has taken reports on the Francis inquiry and its recommendations, along with its own action plan in response, the Berwick review of patient safety and the Care Quality Commission’s new approach to inspections against the essential standards.
The Quality Committee is overseeing the work underway within the trust to understand and actively respond to the necessary changes in roles, responsibilities and accountability, which the changes to systems for the management of patient safety and quality assurance demand. The Keogh review has led to a combined statement from NHS England, Monitor, The CQC and Health Education England which clarifies how each part of the system supporting high quality care should function related to its accountabilities and responsibilities. This was produced to support leaders from each part of the system, so that everyone plays their part in securing improvements for patients without duplication or complications. The core principles of the statement are to ensure: clarity about responsibility for quality, alignment of all relevant bodies working in tandem, accountability for improvement with effective delivery plans and a shared view of success for quality standards.
Following the publication of the individual inspection reports of the 14 hospital trusts involved, Keogh has defined eight ambitions for quality improvement which were common to all of the trusts involved and has set actions against these, which it is proposed all trust boards consider and respond to by 2016.
These are summarised below along with the trust’s response:
AMBITION ONE
All trusts to have early warning systems in place to prevent patient harm and to reduce avoidable death.
TRUST RESPONSE
The trust is designing a ‘cultural barometer’ tool using a range of data and intelligence to act as an early warning monitor, which it then acts on as part of its risk regime.
AMBITION TWO
Boards will confidently and competently use data for the forensic pursuit of quality improvement, including accurate quality data at service line level. Boards of the inspected trusts were found to use transparency of information for blame rather than support and improvement, with some using data simply for reassurance, rather than the pursuit, sometimes uncomfortably, of improvement.
Boards should have a clear lead for quality in each service line and a board level chief quality officer, as in many US hospitals
27 of 132

4
TRUST RESPONSE
The Clinical Divisional Leads are accountable to the Deputy Chief Executive and Medical Director, and the Chief Operating Officer for quality improvement programmes in each division. The trust’s Director of Nursing and People is accountable to the board for directing quality assurance programmes and management.
The trust board has developed a comprehensive integrated performance tool and considers a performance report including quality improvement measures at aggregate and service line level. The board’s Quality Committee dedicates priority time to quality improvement data oversight and has further plans to refine and improve this scrutiny.
AMBITION THREE
The use of patients as equal members of the review team for Keogh, was he has reported, along with staff views and the inclusion of junior medical staff and student nurses ‘the most powerful aspect of the review process’. Keogh has advocated the need for greater insight into listening to and involving patients and staff, as well as governors who are representing the interests of the local population by all boards.
Real time patient feedback must become a normal part of each trust’s customer service and reach well beyond the Friends and Family Test.
Embracing feedback, concerns and complaints with transparent reporting and lessons and actions arising which are then widely shared and published to show real shifts in cultural mind sets of trusts are advocated.
TRUST RESPONSE
The trust is reviewing its service user involvement strategy, which takes further the voice and inclusion of those who use our services at every level of engagement. The Service User Alliance, along with each divisional service user forum, is developing a strong patient improvement and experience plan which will be presented to the forthcoming Service User and Patient Experience Committee. The trust has created this new committee in anticipation of the benefits of viewing improvements in patient experience, as only being successful if its culture and staff engagement is healthy.
The trust is investing in software to enable it to audit and produce meaningful, quick and accurate patient and staff experience measures which can be monitored at team, service line and board level.
Our training doctors have monthly meetings with consultants and the matrons at the Highgate Centre and the Trust has a Local Negotiating Committee which is attended by a British Medical Association representative, training doctor representatives, consultants, and is attended by the Trust Chief Executive and Medical Director and Human Resources.
AMBITION FOUR
Boards are asked to consider how they could apply aspects of the Keogh review methodology to speed up and assist their quest for improved quality.
TRUST RESPONSE
The Quality Committee has agreed an approach to quality assurance trust wide which incorporates central tenets of the Keogh review, including an early warning system, an internal review system of essential standards with a development programme and inspection, a rapid improvement team to support the findings from reviews and inspections and a review of its approach to aspects of risk management and training.
28 of 132
5
AMBITION FIVE
‘No hospital will be an island unto itself. Professional, academic and managerial isolation will be a thing of the past’. The 14 trusts inspected variously lacked a culture of professional and academic ambition and there were many examples of staff being ‘behind the curve’.
TRUST RESPONSE
The trust has strong and effective engagement in research programmes, an innovative audit driven culture and works closely with its Academic Health Science Network, through UCLP. Professional networking and alliances are encouraged throughout all clinical professions and the Medical Director has recently been appointed to the board of London’s Clinical Senate.
AMBITION SIX
Nurse staffing levels and skill mix will reflect patient workload appropriately and be transparently reported every six months by trust boards
TRUST RESPONSE
As set out in the Chief Nursing Officer’s ‘Compassion in Practice’ and the Francis action plan approved by the board, the Director of Nursing has ensured that the best available evidence based tools and expert opinion are used to determine appropriate and safe staffing levels for nursing, working with the Chief Operating Officer for all other staff, using workforce planning methodologies from the HR directorate. We are working to introduce by December a system of publishing level information for the board as well as providing daily/shift by shift assurance for all wards and teams on staffing levels which will be visible to patients and staff.
AMBITION SEVEN
Junior Doctors who move between trusts are potentially powerful agents of change, as are student nurses who bring innovation to nursing practice. Both doctors in training and student nurses can become ambassadors for the trust and should have a means of their voices being heard. Junior doctors must routinely participate in trust’s mortality and morbidity review meetings.
TRUST RESPONSE
We already recognise the contribution that doctors in training make to our clinical audit programmes and anywhere they are working they are welcomed and included in clinical learning about quality or risk issues arising from patient care. The arrangements for student nurses to form a closer bond with their commissioning trust is current being reviewed but working with their mentors (qualified nurses with experience) they are also encouraged to speak up and share their perspectives on patient care – often their challenge can be perceptive and refreshing.
Also of relevance is the trust’s Clinical Leadership Programme (CLP) for Higher Trainees and other multi-professional staff which was developed and implemented in C&I by the Trust’s Darzi Fellow and the Medical Director alongside the Learning & Development, Clinical Governance and Medical Education departments and attending training at Middlesex University.
The programme provides opportunities for trainees and other multi-professional staff to improve their managerial and leadership skills, as well as a better understanding of the NHS. All the projects undertaken were central to the Trusts core objectives.
29 of 132

6
AMBITION EIGHT
All trusts will understand the positive impact that happy and engaged staff have on patient outcomes and will make this a key part of their quality improvement strategy. All trusts must think innovatively about how to engage their staff with an agree action plan setting this out.
TRUST RESPONSE
The trust has established a sub board committee concerned with service user and staff experience, this has membership from both the staff governor constituency and staff side. The trust has developed a draft staff engagement strategy which supports the goals and ambitions of our clinical strategy, this will be endorsed at the next staff partnership meeting. It has an ambitious action plan concerned with staff’s morale and wellbeing at work and the impact on patient care standards when staff are not considered and respected.
CONSIDERATIONS FOR THE TRUST ARISING FROM THE KEOGH REVIEW’S METHODOLOGY
The review process involved training for selected reviewers for the hospital inspections who were all clinically experienced staff or users by experience. We had adopted this approach to our first phase of reviews of services/teams to explore their compliance with the CQC’s essential standards and it has been well received as an approach. Following the Quality Committee’s approval of a paper setting out a proposal to develop this model, further work to recruit more clinical leaders to take part, supported by two dedicated compliance leads – who will also have clinical backgrounds is underway.
Pre visit indicators for each trust were studied and the quality information brought together. It is of note that the 14 trusts had scored themselves generally well in self-assessments, e.g. for PLACE or patient voice, whereas the Keogh reviewers who observed the trust in action for 2 – 3 days and had access to data quality analysts, found many more of these same indicators outside the expected range. Some board members and clinical leaders could not evidence that findings from quality and safety reviews undertaken internally and externally were used to consistently learn from adversity. The capability of Medical and/or Nursing Directors were questioned by the review team at some of the participating trusts.
The review process ended with a ‘risk summit’ which brought together regulators, CCG leads, Local Education and Training personnel and members of the trust’s board to reflect on the findings and to agree a plan of action for quality improvement. A rapid, responsive review was compiled and then shared with the CEO. Some action was taken immediately for safety reasons, such as changes to staffing levels or dealing with complaints backlogs.
The trust’s benefitting the most from the reviews were those who engaged positively in the process. The review observed that, ‘A small number spent disproportionate time challenging the findings of the review team’. Some trusts briefed their staff on what to say to the reviewers, this ill-conceived manipulation reflected a less than open culture and was easily exposed by visiting teams.
All of these valuable insights from the experience of the review into acute hospital trusts have learning for the trust as it strengthens its internal quality governance. We are also mindful that our commissioners and partners in education and health education London, will be considering how to apply the learning as we all work together to improve quality for patients.
30 of 132

7
POST PUBLICATION ACTION AND IMPACT FOR THE TRUST
Following the report’s publication and the placing of 11 of the 14 trusts on ‘special measures’, a combined response setting out the respective responsibilities and accountabilities for all regulatory and statutory health organisations has been published. This shared statement is supported by NHS England, The NHS Trust Development Agency, Monitor, the CQC and Health Education England.
Taking forward responsibility for quality assurance in trusts is set out in the National Quality Board’s document, Quality in the New NHS, (January 2013). The joint statement re-states that documents principles:
1. That trust boards have the accountability and responsibility for quality for their organisation
2. That CCGs manage quality improvements through provider contracts agreed in partnership
3. That CQC assesses trusts against agreed essential standards and takes enforcement action if fundamental standards are breached
4. Monitor holds trusts to account for the delivery of quality standards
5. Quality Surveillance groups at local level are where regulatory and commissioning bodies come together to share concerns and agree action for trusts but they are not accountable bodies in themselves for implementation and delivery. Relevant accountable bodies oversee actions which QSG’s agree
6. Risk Summits can now be called as well as rapid responsiveness reviews with defined criteria and processes, if thresholds of quality or safety are triggered. This will be led by QSGs.
7. Health Education for England is accountable for the quality of educational contracts with providers and taking action about quality concerns in education and training.
8. NHS England is the lead body for support resources, such as the NHS Leadership Academy and the arrangements for Academic Health Science Networks.
CONCLUSIONS
The trust has studied the Keogh review and the joint statement responding to it from accountable health bodies and has started a programme of work to maximise the learning from it, so that its own quality assurance systems are effective and benefit from the methodology used. The emerging roles and responsibilities for quality regulation and monitoring against quality performance locally by CCGs, LETBs, AHSNs and Quality Surveillance Groups involve active contribution from the trust, and we believe we have a thorough understanding and confident approach to utilising the new quality assurance architecture.
The trust has clarified its quality failure and risk regime to ensure clarity and purposeful action for remedy and escalation where quality and safety standards are not met. The work on Changing Lives with restated trust values has been communicated widely to staff and partners as part of a cultural shift to listening and valuing staff. Effective stakeholder engagement continues, with exercises such as the Governors pledges on the fundamentals of the Francis inquiry and strong patient involvement in safety and quality programmes in the trust.
We are awaiting the announcement of the deputy chief inspector for Mental Health, who will support Sir Mike Richards, Chief Inspector of Hospitals and who will lead the first phase of those Mental Health trusts which have been identified for CQC reviews this winter.
31 of 132

8
Meanwhile we are anticipating the Government’s final response to the Francis inquiry to be announced on 19 November 2013 which may well re-emphasise the expectations for trusts to act on the element arising from the Keogh review set out in this paper.
RECOMMENDATIONS
The trust board is asked to note this report.
32 of 132
Report to: Board of Directors (Public)
Paper Number: 4.1
Report For: Information
Report Type: Strategy and Operational Performance
Date: 28 November 2013
Report Author: Ms Wendy Wallace, Chief Executive
Report of: Ms Wendy Wallace, Chief Executive
FoI Status: Report can be made public
Title: Chief Executive’s Report
Executive Summary
The Chief Executive has a duty to keep the Board informed on all matters relating to the health of the organisation and provide a status and progress report on the use of the Trust Seal, key strategic developments and significant events since the last Board meeting. This report includes updates supplied by members of the Foundation Trust Executive and the Trust Secretary. Recommendations to the Board
The Board of Directors is requested to: Note the contents of this report; and
Ratify the use of the Trust Seal.
Trust Strategic Priorities Supported by this Paper Excellence
E1 Continually improve the quality and safety of service delivery, service user experience and improving outcomes.
E2 Delivering the highest level of quality and financial performance. Innovation
I1 Rapidly adopt best practice and maintain a culture of innovation in service development. Growth
G1 Pursue organic and inorganic growth opportunities through strategic partnerships and research and development.
33 of 132

2
Risk Implications
The paper covers developments in areas already identified within the risk register.
Legal and Compliance Implications
The report includes a summary of national developments which will affect the Trust’s compliance requirements. Finance Implications
None. Single Equalities Impact Assessment
As this report summarised the external environment and internal issues it does not of itself require a SEIA, although elements within the report may and would be conducted as part of their separate governance processes.
Requirement of External Assessor/Regulator
Monitor is responsible for ensuring that Foundation Trusts are well governed. Best practice guidance concerning Board Governance includes an expectation that the Board is kept fully appraised about the external environment, the strategic implications for the Trust and internal matters. This report contributes to this requirement.
34 of 132

3
CHIEF EXECUTIVE’S REPORT 1. NATIONAL STRATEGIC ENVIRONMENT
1.1
NHS Mandate 2014-16
The NHS Mandate is an agreement between the Department of Health and NHS England. The agreement sets out the objectives and finances for NHS England. The areas of the mandate correspond to the 5 parts of the NHS Outcomes Framework. In addition to this there are priority areas where significant progress is expected. These are: improving standards of care and treatment especially for older people at the end of their
lives; diagnosis, treatment and care of people with dementia; supporting people with multiple long term conditions… delivering in a way which values
mental and physical health; preventing premature deaths; and supporting people with health conditions to remain in or find work.
Of particular note for mental health providers are:
Outcome: preventing people from dying prematurely
Ensuring people have access to the right people when they need it, including drug treatments recommended by NICE for services for children and adults with mental health problems; and
Preventing illness through every staff contact taking opportunity to reduce smoking, improve healthy eating, drinking less alcohol and exercising more.
Outcome indicator: Excess under 75 mortality rate for people with MH.
Outcome: Enhancing quality of life for people with long term conditions
Progress in diagnosis, treatment & care of dementia; Better integration of services; Offered personalised care plan; Option to hold personalised health budget; and Plans for secure linking electronic health records and with consent to be passed to
any part of the NHS or social care. Outcome indicators: Employment of people with mental illness.
Diagnosis rate for dementia. Sustaining independence post diagnosis dementia.
Outcome: Recovery from episodes of ill health
Shine a light on variation and unacceptable practice- revolution in transparency Systematic PROMs and PREMs; Close the gap between people with MH problems and population as a whole; and Extend IAPT to 15% of adults and 50% recovery rate. Outcome indicator: psychological therapies outcome.
35 of 132

4
Outcome: Positive experience of care
Substantially reduce reliance on inpatient care for people with a learning disability; More regular feedback on friends and family test as the norm; Introduction of the F&FT to ‘rest of the NHS’ from Oct 2013, good scores financially
rewarded; and Access to mental health services – will establish comprehensive levels of access to
and waiting times for MH services. CCG’s to address unacceptable delays; and significantly improve waiting times. NHSE Board to consider new access standards, including the financial implications of the standard.
Outcome indicator: Experience of mental health services.
Outcome: Safe environment and protection from avoidable harm
Culture of safety through improved reporting of incidents; and
Identify those groups at higher risk of suicide – CCG’s ensure providers take all reasonable steps to reduce number of suicides and incidents of serious self-harm, including effective crisis response.
Outcome Indictor: safety incidents resulting in severe harm or death.
In addition the Mandate includes offering choice of any qualified provider in community and mental health services, in line with local circumstances.
1.2 Strategic and Operational Planning 2014-16
At the beginning of November Monitor, NHS England the LGA and TDA wrote to all Trusts, CCG’s and Directors of adult Social Services to outline the strategic and operational planning process for the next year and beyond. This letter included further information about the processes expected in relation to the £3.8bn ‘Integration Transformation Fund’. This guidance set out a number of important changes to both the annual process and the ambition for the planning: Instead of a 1+2 plan Trusts will be required to submit to Monitor a 2+3 year plan, with
the full 5 year plan submitted in June; The 2 year plan is required to be submitted to Monitor by 4th April, this is 2 months
ahead of the usual submission date of 31st May; CCGs must come together in planning units to produce an integrated longer-term
strategic plan. This plan should be consistent across the CCG’s; Commissioners and local authorities should engage with providers in developing the
plans and provider plans should be consistent with the CCGs plans; The CCG plans must develop bold and transformative long term strategies and plans
for services that are financially sustainable and safe; The CCG plans must focus on improving the outcomes set out in each domain of the
NHS Outcomes framework; Subject to final decisions for 2014/15 the NHS efficiency expectation is 4%, inflation
2.1% and price deflation 1.9%. In December the equivalent figures for 2015//16-2020 will also be published;
Contracts are expected to be signed by 28th February 2014. The NHS has never achieved the expected contract signing date and indeed many organisations have still not signed off this year’s contract. Last year we did not have a contract offer by this date; and finally
CCGs will receive notice of their allocations in w/c 16th Dec. In addition to this I have learned that it is likely that there will be a national CQUIN associated with completeness of diagnosis recording in mental health services and a penalty of £10 per person for each patient without a NHS number recorded.
36 of 132
5
1.3 Government response to the Francis report
The Government response to the Francis report has just been published. The key issues are: a fit and proper persons test for Board members and greater performance management
of very senior managers; a statutory duty of candour on organisations and professional duty on individuals, with
financial penalties if mistakes have been found to be covered up; greater senior involvement in complaints handling and annual publication by trusts of a
review of complaints; guidance and tools for setting staffing levels and regular publication of actual levels;
and regular publication of patient safety data, including never events.
1.4 London Mental Health Trusts
Paul Jenkins has been appointed as the new Chief Executive for the Tavistock and Portman NHS FT. Paul is currently Chief Executive of Rethink a national mental health charity and has previously worked in the NHS and central government. He does not have a starting date as yet. Simon Young, who is the Director of Finance at the Tavistock & Portman will continue as acting Chief Executive until Paul arrives.
1.5 Kings Fund Commission
The mental health CEOs have commissioned a project and report from the Kings Fund. The first part of the work – to identify the lessons from mental health’s move into community for integration in other parts the NHS- is due to be launched in early December.
2. SERVICE DEVELOPMENTS AND CHANGES
2.1 St Pancras Hospital Development
Since my last report, engagement with staff, service users and carers has continued to generate ideas and views about how the site should be developed for the future. A service user and carer focused event was held at St Pancras on 8th November and was attended by a number of service users. A further member’s event has been organised for 4th December and Governors have been invited to attend this event and be available to meet with those members who attend.
2.2 Crisis House Development at St Pancras
Construction work continues to get the Crisis House at St Pancras ready for opening in January 2014. The recent competition to name the new service has now closed and the name will be agreed and announced in the coming weeks. Work continues to engage with the local community on the operation of this new service, which is also expected to impact on the levels of bed occupancy in the Trust.
2.3 Additional Funding for Mental Health Liaison Services
The Trust has received over £300k additional funding to further develop the liaison services at two of the 3 Acute Trusts (Royal Free and Whittington). This will see the models of liaison developed using the Rapid Assessment, Intervention and Discharge (RAID) model and increased levels of input to A&E over a 24 hour period.
37 of 132

6
2.4 Children and Adolescent Transitional Care Arrangements
Work continues to review and strengthen the transitional care arrangements for adolescents moving to adult services, with additional funding from Islington CCG being used to develop a new model of joint working across the two services to better meet the needs of young people transitioning between CAMHs and AMH services.
3. REGULATION & LEGISLATION
3.1 Monitor
As detailed above, NHS England, the Local Government Association, Monitor, and the Trust Development Authority issued a joint letter providing initial guidance on the 2014/15 strategic and operational planning process. We expect further guidance from Monitor during the week of 16th December. Monitor has also issued a draft revised Code of Governance for NHS Foundation Trusts on 8th November for a 3 week consultation with a deadline for feedback on 29th November. A great deal has changed since Monitor last updated the Code in 2010 and many of these changes have implications for how NHS Foundation Trusts are expected to establish and report on corporate governance arrangements. The changes largely result from the following: The Health and Social Care Act 2012; The new Provider Licence; The Risk Assessment Framework; The Francis Inquiry Report; and A new edition of the UK Corporate Code of Governance.
3.2 Care Quality Commission (CQC)
As reported last time the way that CQC inspects services is being radically changed with a new approach involving large inspection teams and significantly greater use of service users and professional peer assessors. This approach is currently being developed for mental health services. The CQC have published a list of eight mental health and community services provider organisations that will be inspected between January and March 2014. This will be in addition to a second wave of 19 further acute trust inspections using the new model. The mental health and community Trusts included are all aspirant FTs and have been recommended by the NTDA. The only London mental health Trust included in this list is SW London & St George’s mental health Trust.
Internal Quality Assurance Framework
The Quality Committee has approved proposals which set out the Trust’s approach to put in place a robust internal quality assurance framework. The key aspects of the proposed internal model and approach to quality assurance are detailed below: The ability to triangulate data through a new integrated quality assurance dashboard
(IQAD); An annual internal inspection programme carried out by internal clinical experts drawn
from all professions. This would also include ‘privacy and dignity walks’ including service users, as well as ad-hoc visits informed by the IQAD;
The use of Rapid Improvement Teams. such as the approach adopted successfully at Stacey Street; and
The provision of compliance reports on a monthly basis to the divisional performance meetings and aggregated quarterly reports to the Quality Committee.
38 of 132

7
It’s important to stress that this approach needed to be implemented thoughtfully and communicated clearly to staff throughout the organisation to gain full engagement in creating a positive service improvement and learning culture. The Board of Directors need to fully embrace this approach and receive regular updates via the Quality Committee.
4. EXTERNAL PROFILE
4.1 Pentonville day care centre service users succeed at awards ceremony
The Koestler annual national showcase of arts by prisoners, offenders on community sentences, secure mental health patients and immigration detainees was opened on 25 September at the Southbank Centre. Each year a curator is chosen to select art works that they feel should be preserved as a testament to the importance of human creation. This year’s theme is ‘Strength and Vulnerability’ and it is curated by the Mercury Prize winner and Rapper called Speech Debelle. The Koestler competition gives the opportunity to show the range of talents that prisoners have and can offer back to society. This year we had a number of entrants to the competition from the Day Care Centre at HM Pentonville Prison which is a C&I service offering occupational and purposeful activity for mentally ill offenders. The art works are judged by professionals in the fields of arts, ceramics, drama, music and others and all Day Care Centre entrants this year were in the ceramics field. They were awarded with two gold awards, four highly commended awards, one platinum award, two silver awards, five bronze awards and one first time entrant’s award. Those who attend the day care centre have expressed how extremely proud they are for what they have achieved. The exhibition is run by ex-offenders and it is currently exhibited on a daily basis at the Southbank Centre London until 1 December 2013.
4.2 Professor Brewin Received the Robert S. Laufer Memorial Award for Outstanding Scientific Achievement
Professor Brewin, who is a consultant clinical psychologist at C&I’s Traumatic Stress Clinic, received an award on the 7 November in Philadelphia, USA. He received the Robert S. Laufer Memorial Award for Outstanding Scientific Achievement, presented by the International Society of Traumatic Stress Studies, for his overall contribution to research and development in the field. This is a prestigious award in the field of Traumatic Stress Studies and Chris is the first person from the UK to ever receive this award.
4.3 Increasing Awareness of the Trust’s London Veterans’ Assessment and Treatment Service
Dr Tess Browne, C&I Clinical Psychologist at the London Veterans’ Assessment and Treatment Service (LVS) was interviewed by ITV London on 8 November in the run-up to Remembrance Sunday. The LVS is jointly provided by Camden and Islington NHS Foundation Trust and South London and Maudsley NHS Foundation Trust and comprises of psychiatry, psychology and nursing staff to provide a multi-disciplinary team. The news segment can be viewed on our website. The service was also featured in the Camden New Journal.
39 of 132
8
5. INTERNAL EVENTS
5.1 C&I is participating in the 12000 Trained in Dementia awareness project
C&I is pleased to participate in the 12000 Trained in Dementia awareness project. The project, supported by UCLPartners, aims to train 12000 Healthcare staff by the end of March 2014 across North Central and East London. A wide range of training sessions are currently being delivered across the trust ranging from a one-hour introductory awareness session, to more advanced training modules. Our first session saw a number of Balfour Beatty Workforce colleagues attending. The feedback received was highly encouraging with colleagues recognising areas where current work practices could be improved and considered people with dementia they may come in contact with.
6. COUNCIL OF GOVERNORS
6.1 Governor Developments
The next Council of Governors meeting is on 3 December which will be the first meeting including all the recently elected Governors. Following their induction on 22 October, the Chair has been meeting with, and getting to know, many of the Governors and considering ways in which to improve engagement and better support them to fulfil their statutory duties. This will be discussed in full at the Council meeting on 3 December.
6.2 C&I Members’ Newsletter and Events
The winter edition of the C&I News including the Members’ Newsletter was sent out in mid-November and included a range of information on Trust developments and events as well as a message from our Lead Governor, David Barry. Details of a St Pancras Hospital development members’ forum was also included which is to be held on 4 December from 6.00-7.00pm in the conference centre at SPH. A further event to which members have been invited include the Dementia Awareness event on 27th November. Members have been invited to drop into this event anytime between 2.00-7.00pm with an opportunity to meet Governors from 5.00-6.30pm.
7. STAFF CHANGES
I am very sorry to report that Professor Hugh Gurling passed away on 2nd November. Professor Gurling was an honorary consultant psychiatrist at the trust who worked at St Luke’s Hospital and more recently on Coral Ward at Highgate Mental Health Centre. An eminent psychiatrist with an international reputation for his work in molecular psychiatry, Professor Gurling’s ground-breaking research used genetics as a method to understand the abnormal neurobiology causing schizophrenia, affective disorders, Tourette syndrome, attention deficit hyperactivity disorder, autism and alcoholism. Hugh will be sorely missed by all who knew and worked with him. Lynda McDonald is leaving C&I on 29th November to take up a promotion opportunity; as Assistant Director of Programme and Change Management in Barnet, Enfield & Haringey Mental Health Trust. Lynda has had a varied career at C&I since 1998 - she initially managed a number of operational services, before taking on lead responsibility for delivering our high level change programmes and played an instrumental role in the Trust’s implementation of Agenda for Change between 2004-2006. We wish Lynda well in her new post.
40 of 132

9
Karl Heidel joined the Trust as Head of Communications and Engagement in November. Karl has been in communications for the last 16 years, most recently working for Princess Alexandra Hospital (PAH) in Essex. When Karl joined that trust they were a failing organisation and were suffering from severe reputational failure. In just over a year they managed to turn that around so PAH is now considered by Department of Health to be one of the best performing trusts in the country. He joined the NHS in 2009 and his first role was in the NHS Sustainable Development Unit, a national organisation helping the Health Service to become more environmentally friendly. Prior to that he worked for ITV and ITN news. Karl can be reached on 020 3317 3089 or [email protected]
8. SERVICE VISITS
Since my last report at the end of October 2013, I have visited the following services: Margarete Centre; Westminster Drug Service; and Traumatic Stress Service.
9. FTE MEETINGS (30th October to 20th November 2013)
The following table gives a brief summary of the areas covered in the weekly Foundation Trust Executive meeting.
Topic:
Received a report on the staffing issues associated with the safe restraint of service users in inpatient settings.
Approved proposals to deal with staffing issues.
Reviewed a detailed implementation plan associated with taking forward a new membership strategy.
Approved proposals
Business Development and planning
Received updates on current opportunities and tenders.
Operational Performance Received summary of the September monthly Divisional performance.
Finance and QIPP Received monthly finance and QIPP reports including service allocations for Christmas.
Reports for November Board Reviewed a number of reports in preparation for Board
41 of 132
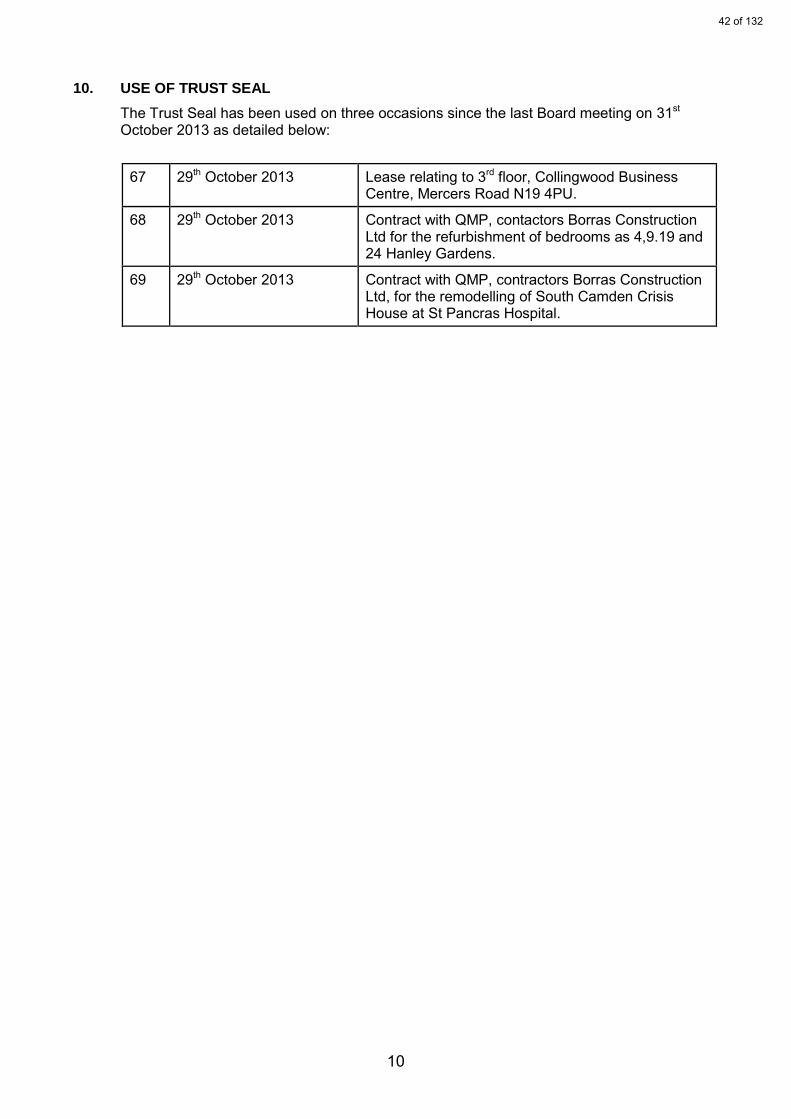
10
10.
USE OF TRUST SEAL
The Trust Seal has been used on three occasions since the last Board meeting on 31st October 2013 as detailed below:
67 29th October 2013 Lease relating to 3rd floor, Collingwood Business Centre, Mercers Road N19 4PU.
68 29th October 2013 Contract with QMP, contactors Borras Construction Ltd for the refurbishment of bedrooms as 4,9.19 and 24 Hanley Gardens.
69 29th October 2013 Contract with QMP, contractors Borras Construction Ltd, for the remodelling of South Camden Crisis House at St Pancras Hospital.
42 of 132

Report to: Board of Director (Public)
Paper Number: 4.2
Report For: Monitoring
Report Type: Performance
Date: 28 November 2013
Report Author: Mike Piercy, Deputy Director of Finance
Report of: David Wragg, Director of Finance
FoI Status: Report can be made public
Title: Month 7, 2013/14 - Financial Position
Executive Summary This paper updates on the financial position as at the end of October 2013 (month 7). The Trust has submitted a plan to Monitor based on a full year normalised surplus of £2,000k. As a result, the planned surplus for month 7 is £1,167k. At month 7, the Trust is ahead of this level, showing a normalised surplus of £1,457k (£289k ahead of plan). The Trust has sold of Fordwych Rd, Ashley Rd and Cleveland St during months 5 and 6, 2013/14. The impact of these asset sales has been reflected in the month 7 position. Recommendation to the Board
The Board of Directors is requested to: note the month 7 position
Trust Strategic Priorities Supported by this Paper Excellence
E2 Delivering the highest level of quality and financial performance.
43 of 132

Risk Implications
Achievement of planned outturn position. Legal and Compliance Implications
Remain within Monitor’s licence terms. Finance Implications
Delivery of financial plan. Single Equalities Impact Assessment
N/A Requirement of External Assessor/Regulator
The financial position supports the financial element of the Trust’s in-year governance declaration to Monitor.
44 of 132

4
%age of
Turnover
Actual Normalised Outturn Month 7 £1,457k surplus 1.9%
Planned Normalised Outturn 7 £1,167k surplus 1.6%
Planned Actual Normalised Outturn £2,000k surplus 1.6%
EBITDA Month 7 £5,033k surplus 6.7%
Variance from EBITDA target (YTD) £263k favourable
Cash in held at bank G
Funds deposited with NLF G
Liquidity ratio (days) G
Capital service ratio (times) G
Overall Rating G
Full Year Full Year
Target Forecast
£k Q1 Q2 Q3 Q4 £k
Schemes:
Full year effect of 12/13 schemes 2,500 G G G G 2,500Administration & Management 1,200 G G G G 1,200Bed management 872 G G G G 872Estates 819 G A A A 819Skillmix 509 G G G G 509
Less: Headroom -1,000 -1,000
4,900 4,900
The Trust has a full year normalised surplus target of £2,000k, which at equates to a YTD position of £1,167k. As at month 7, the Trust is ahead of plan by £289k (£254k as at month 6).
Risks
Rating
QIPP comments
4
-2.0 4105
Temporary Staffing
Continuity of Service Risk Rating - In year achievement
3.7
FINANCIAL PERFORMANCE OVERVIEW AS AT OCTOBER 2013
Cumulative Net Position
Cash
Threshold*
£4,503£50,000
Income and Expenditure
Actual
Lower
Overall Rating
QIPPProgress
£k
4
*The lower threshold is the point at which each of the respective ratios will
fall from their current level.
2.5
i) Non achievement of run rates in year against budgetary levelii) Failure to identify sufficient mitigations for any adverse run rates
- The full year effect of schemes actioned in 12/13 accounts for a significant amount of the target and has been secured for the year. - Other schemes are on the whole identified and targets have been applied to budgets.- The working assumption is full delivery will be achieved.
0.00
0.25
0.50
0.75
1.00
1.25
1.50
1.75
2.00
2.25
M1 M2 M3 M4 M5 M6 M7 M8 M9 M10 M11 M12
£m
Financial Position - Normalised Surplus
Actual Plan
-
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
M1 M2 M3 M4 M5 M6 M7 M8 M9 M10 M11 M12
£m
EBITDA - Performance
Actual Plan
-
0.10
0.20
0.30
0.40
0.50
0.60
0.70
12/13M08
12/13M09
12/13M10
12/13M11
12/13M12
13/14M01
13/14M02
13/14M03
13/14M04
13/14M05
13/14M06
13/14M07
£m
Spend on Temporary Staffing
Actual
45 of 132
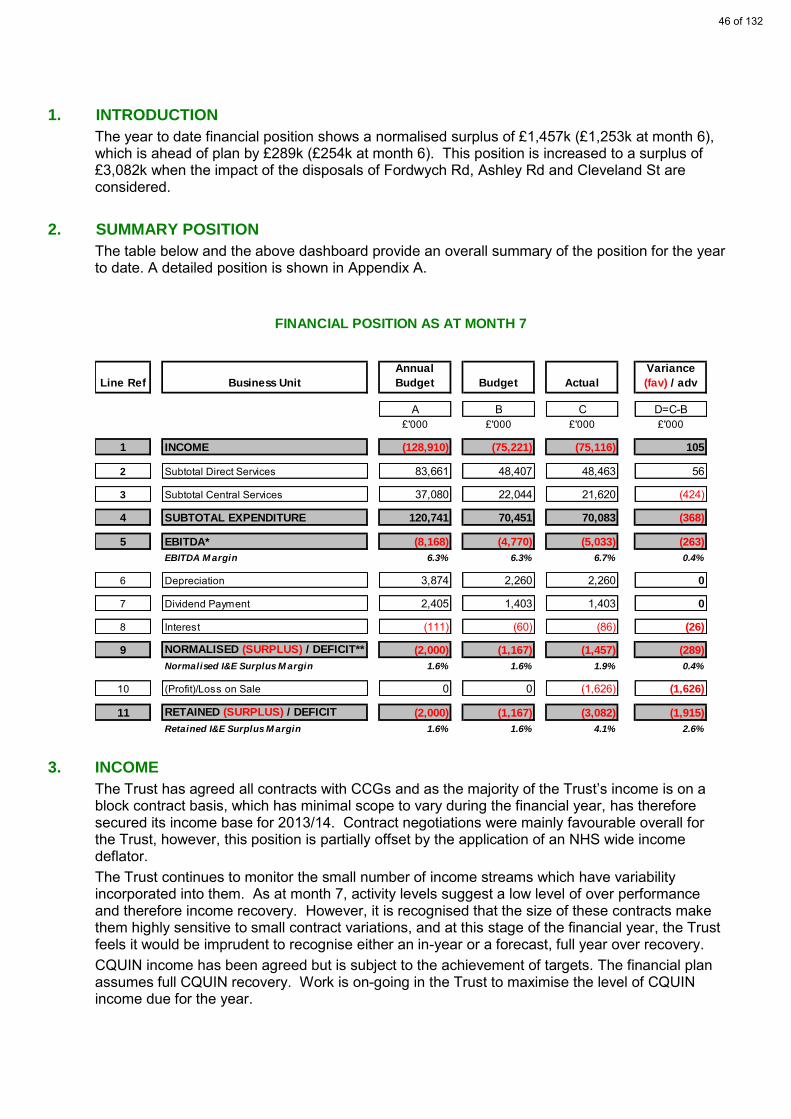
1. INTRODUCTION
The year to date financial position shows a normalised surplus of £1,457k (£1,253k at month 6), which is ahead of plan by £289k (£254k at month 6). This position is increased to a surplus of £3,082k when the impact of the disposals of Fordwych Rd, Ashley Rd and Cleveland St are considered.
2. SUMMARY POSITION
The table below and the above dashboard provide an overall summary of the position for the year to date. A detailed position is shown in Appendix A.
3. INCOME
The Trust has agreed all contracts with CCGs and as the majority of the Trust’s income is on a block contract basis, which has minimal scope to vary during the financial year, has therefore secured its income base for 2013/14. Contract negotiations were mainly favourable overall for the Trust, however, this position is partially offset by the application of an NHS wide income deflator. The Trust continues to monitor the small number of income streams which have variability incorporated into them. As at month 7, activity levels suggest a low level of over performance and therefore income recovery. However, it is recognised that the size of these contracts make them highly sensitive to small contract variations, and at this stage of the financial year, the Trust feels it would be imprudent to recognise either an in-year or a forecast, full year over recovery. CQUIN income has been agreed but is subject to the achievement of targets. The financial plan assumes full CQUIN recovery. Work is on-going in the Trust to maximise the level of CQUIN income due for the year.
Line Ref Business Unit
Annual
Budget Budget Actual
Variance
(fav) / adv
A B C D=C-B£'000 £'000 £'000 £'000
1 INCOME (128,910) (75,221) (75,116) 105
2 Subtotal Direct Services 83,661 48,407 48,463 56
3 Subtotal Central Services 37,080 22,044 21,620 (424)
4 SUBTOTAL EXPENDITURE 120,741 70,451 70,083 (368)
5 EBITDA* (8,168) (4,770) (5,033) (263)
EBITDA M argin 6.3% 6.3% 6.7% 0.4%
6 Depreciation 3,874 2,260 2,260 0
7 Dividend Payment 2,405 1,403 1,403 0
8 Interest (111) (60) (86) (26)
9 NORMALISED (SURPLUS) / DEFICIT** (2,000) (1,167) (1,457) (289)
Normalised I&E Surplus M argin 1.6% 1.6% 1.9% 0.4%
10 (Profit)/Loss on Sale 0 0 (1,626) (1,626)
11 RETAINED (SURPLUS) / DEFICIT (2,000) (1,167) (3,082) (1,915)
Retained I&E Surplus M argin 1.6% 1.6% 4.1% 2.6%
FINANCIAL POSITION AS AT MONTH 7
46 of 132

4. OUTTURN POSITION AT MONTH 7
Service and corporate budgets have been allocated QIPP Targets of £5,900k (£3,442k YTD). Opening budgets have been adjusted for these amounts, and the month 7 position reports against the reduced budgetary level. The month 7 position is ahead of plan, which represents not only a positive financial position and is also positive affirmation of the robustness of QIPP identification. The position is predominantly due to underspends within operational services. As at month 7, there are indications that NHS Pension auto enrolment is having an impact on the Trust’s ability to maintain financial balance. Payments to the NHS Pensions Scheme averaged £612k per month in months 1 to 5. The average has risen by between £30k and £40k per month for Month 6 and 7, a full year pressure of up to £500k, or £250k this year. It may be that the pressure falls as more staff opt out (as 108 staff did in Month 6), but the pressure, although budgeted for, is a significant one.
Operational Divisions
Operational divisions are, at month 7, underspent by £48k (£162k at month 6). The main component of the respective underspends relates to vacancies within the system. Planned and on-going recruitment will continue to reduce vacancy levels, and must be offset with corresponding reductions in temporary staffing usage, in order that there is not a financial pressure as a consequence. However, there has been a planned transfer of budgetary responsibility for the service related, substantive medical posts, from THQ to Operational Services. The budget associated with this is circa £4,400k annually, with an associated QIPP target of 194k for the year, and has resulted in a worsening of the position, in month, of £125k. The Operational Services Management statement is overspent against budget by £403k (£397k at month 6). This overspend is as a result of residual QIPP targets being held centrally while final identification and clearance takes place. This exercise needs to be progressed and once finalised the underlying financial positions within Operational Services will be clearer. There have been two compensating changes in month 7 in the Operational Services Management area. The transfer of medical budgets to the Operational Services Management statement (as described above) has been offset by the agreed transfer of an outstanding QIPP target of £315k to the Rehabilitation & Recovery division, which has resulted in a £184k benefit in Operational Services Management in month 7, but has been neutral across the overall Operational Services position. Acute Services are showing an over spend of £172k (£182k overspent at month 6), with the main contributor, to both the in-month and year to date position, being the significant overspends on PICU/Private Placements. Further pressure is being experienced from overspends on inpatient budgets and unidentified QIPP, which are partially offset by a non recurrent underspend in the Camden Crisis Service. Month 7 has shown a continued and welcome decrease in the value of PICU/Private Placements, which has contributed to the in-month underspend across the division. The following chart shows the trend of expenditure on PICU/Private Placements during 2013/14.
47 of 132
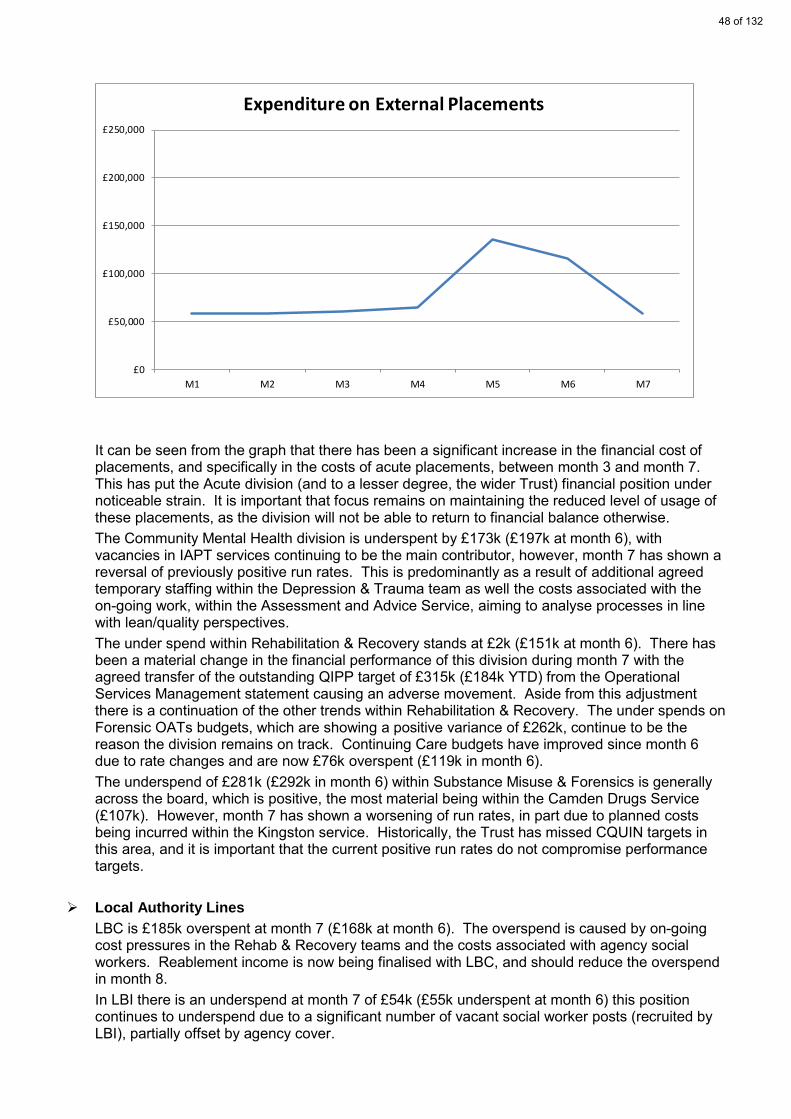
It can be seen from the graph that there has been a significant increase in the financial cost of placements, and specifically in the costs of acute placements, between month 3 and month 7. This has put the Acute division (and to a lesser degree, the wider Trust) financial position under noticeable strain. It is important that focus remains on maintaining the reduced level of usage of these placements, as the division will not be able to return to financial balance otherwise. The Community Mental Health division is underspent by £173k (£197k at month 6), with vacancies in IAPT services continuing to be the main contributor, however, month 7 has shown a reversal of previously positive run rates. This is predominantly as a result of additional agreed temporary staffing within the Depression & Trauma team as well the costs associated with the on-going work, within the Assessment and Advice Service, aiming to analyse processes in line with lean/quality perspectives. The under spend within Rehabilitation & Recovery stands at £2k (£151k at month 6). There has been a material change in the financial performance of this division during month 7 with the agreed transfer of the outstanding QIPP target of £315k (£184k YTD) from the Operational Services Management statement causing an adverse movement. Aside from this adjustment there is a continuation of the other trends within Rehabilitation & Recovery. The under spends on Forensic OATs budgets, which are showing a positive variance of £262k, continue to be the reason the division remains on track. Continuing Care budgets have improved since month 6 due to rate changes and are now £76k overspent (£119k in month 6). The underspend of £281k (£292k in month 6) within Substance Misuse & Forensics is generally across the board, which is positive, the most material being within the Camden Drugs Service (£107k). However, month 7 has shown a worsening of run rates, in part due to planned costs being incurred within the Kingston service. Historically, the Trust has missed CQUIN targets in this area, and it is important that the current positive run rates do not compromise performance targets.
Local Authority Lines
LBC is £185k overspent at month 7 (£168k at month 6). The overspend is caused by on-going cost pressures in the Rehab & Recovery teams and the costs associated with agency social workers. Reablement income is now being finalised with LBC, and should reduce the overspend in month 8. In LBI there is an underspend at month 7 of £54k (£55k underspent at month 6) this position continues to underspend due to a significant number of vacant social worker posts (recruited by LBI), partially offset by agency cover.
£0
£50,000
£100,000
£150,000
£200,000
£250,000
M1 M2 M3 M4 M5 M6 M7
Expenditure on External Placements
48 of 132
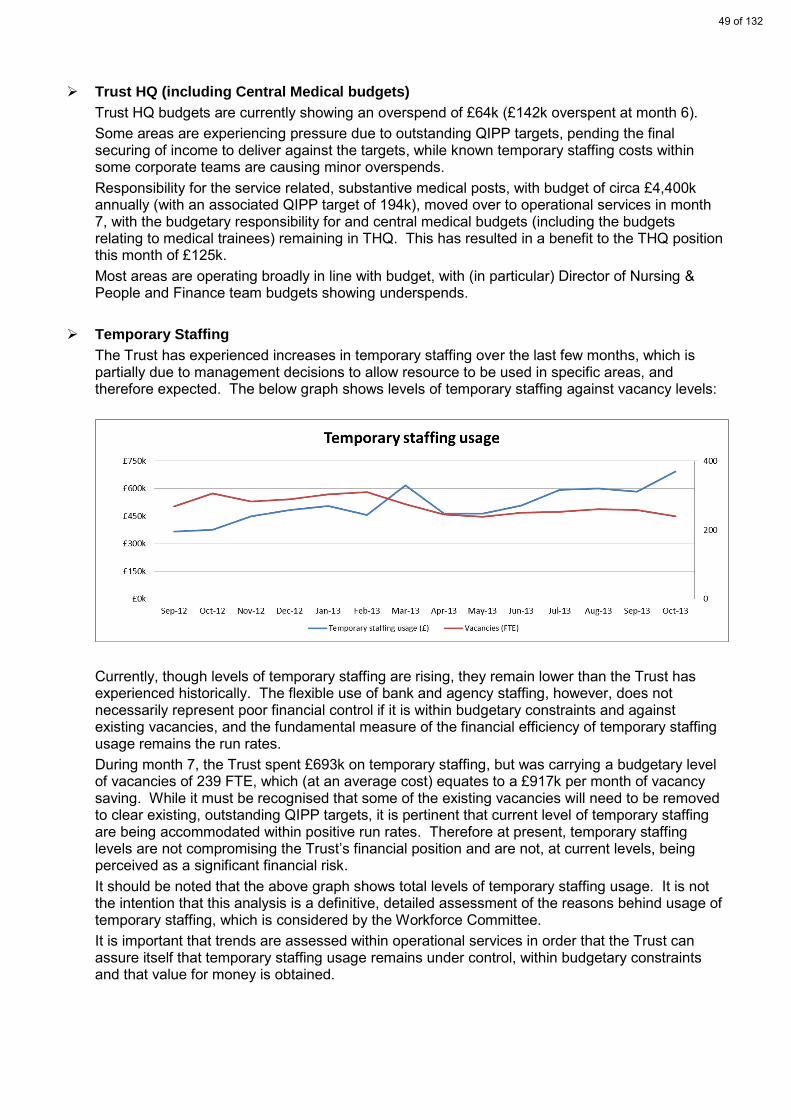
Trust HQ (including Central Medical budgets)
Trust HQ budgets are currently showing an overspend of £64k (£142k overspent at month 6). Some areas are experiencing pressure due to outstanding QIPP targets, pending the final securing of income to deliver against the targets, while known temporary staffing costs within some corporate teams are causing minor overspends. Responsibility for the service related, substantive medical posts, with budget of circa £4,400k annually (with an associated QIPP target of 194k), moved over to operational services in month 7, with the budgetary responsibility for and central medical budgets (including the budgets relating to medical trainees) remaining in THQ. This has resulted in a benefit to the THQ position this month of £125k. Most areas are operating broadly in line with budget, with (in particular) Director of Nursing & People and Finance team budgets showing underspends.
Temporary Staffing
The Trust has experienced increases in temporary staffing over the last few months, which is partially due to management decisions to allow resource to be used in specific areas, and therefore expected. The below graph shows levels of temporary staffing against vacancy levels:
Currently, though levels of temporary staffing are rising, they remain lower than the Trust has experienced historically. The flexible use of bank and agency staffing, however, does not necessarily represent poor financial control if it is within budgetary constraints and against existing vacancies, and the fundamental measure of the financial efficiency of temporary staffing usage remains the run rates. During month 7, the Trust spent £693k on temporary staffing, but was carrying a budgetary level of vacancies of 239 FTE, which (at an average cost) equates to a £917k per month of vacancy saving. While it must be recognised that some of the existing vacancies will need to be removed to clear existing, outstanding QIPP targets, it is pertinent that current level of temporary staffing are being accommodated within positive run rates. Therefore at present, temporary staffing levels are not compromising the Trust’s financial position and are not, at current levels, being perceived as a significant financial risk. It should be noted that the above graph shows total levels of temporary staffing usage. It is not the intention that this analysis is a definitive, detailed assessment of the reasons behind usage of temporary staffing, which is considered by the Workforce Committee. It is important that trends are assessed within operational services in order that the Trust can assure itself that temporary staffing usage remains under control, within budgetary constraints and that value for money is obtained.
49 of 132
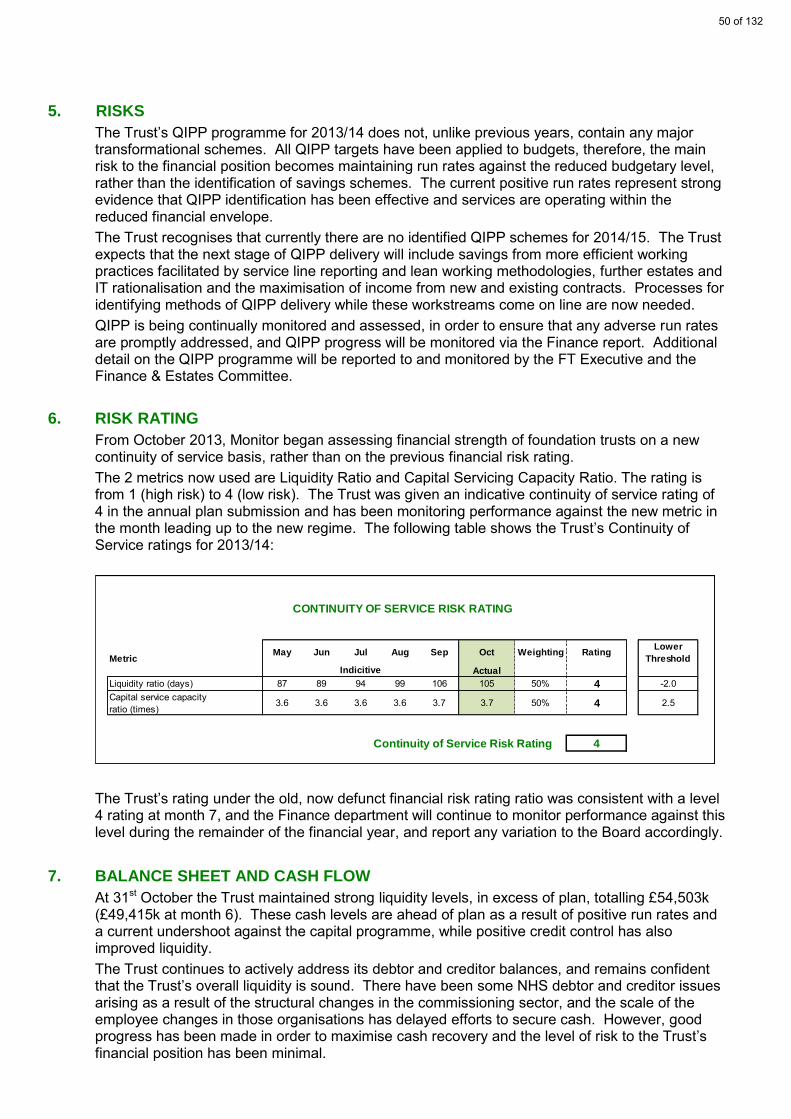
5. RISKS
The Trust’s QIPP programme for 2013/14 does not, unlike previous years, contain any major transformational schemes. All QIPP targets have been applied to budgets, therefore, the main risk to the financial position becomes maintaining run rates against the reduced budgetary level, rather than the identification of savings schemes. The current positive run rates represent strong evidence that QIPP identification has been effective and services are operating within the reduced financial envelope. The Trust recognises that currently there are no identified QIPP schemes for 2014/15. The Trust expects that the next stage of QIPP delivery will include savings from more efficient working practices facilitated by service line reporting and lean working methodologies, further estates and IT rationalisation and the maximisation of income from new and existing contracts. Processes for identifying methods of QIPP delivery while these workstreams come on line are now needed. QIPP is being continually monitored and assessed, in order to ensure that any adverse run rates are promptly addressed, and QIPP progress will be monitored via the Finance report. Additional detail on the QIPP programme will be reported to and monitored by the FT Executive and the Finance & Estates Committee.
6. RISK RATING
From October 2013, Monitor began assessing financial strength of foundation trusts on a new continuity of service basis, rather than on the previous financial risk rating. The 2 metrics now used are Liquidity Ratio and Capital Servicing Capacity Ratio. The rating is from 1 (high risk) to 4 (low risk). The Trust was given an indicative continuity of service rating of 4 in the annual plan submission and has been monitoring performance against the new metric in the month leading up to the new regime. The following table shows the Trust’s Continuity of Service ratings for 2013/14:
The Trust’s rating under the old, now defunct financial risk rating ratio was consistent with a level 4 rating at month 7, and the Finance department will continue to monitor performance against this level during the remainder of the financial year, and report any variation to the Board accordingly.
7. BALANCE SHEET AND CASH FLOW
At 31st October the Trust maintained strong liquidity levels, in excess of plan, totalling £54,503k (£49,415k at month 6). These cash levels are ahead of plan as a result of positive run rates and a current undershoot against the capital programme, while positive credit control has also improved liquidity. The Trust continues to actively address its debtor and creditor balances, and remains confident that the Trust’s overall liquidity is sound. There have been some NHS debtor and creditor issues arising as a result of the structural changes in the commissioning sector, and the scale of the employee changes in those organisations has delayed efforts to secure cash. However, good progress has been made in order to maximise cash recovery and the level of risk to the Trust’s financial position has been minimal.
MetricMay Jun Jul Aug Sep Oct Weighting Rating
Lower
Threshold
Actual
Liquidity ratio (days) 87 89 94 99 106 105 50% 4 -2.0Capital service capacity ratio (times)
3.6 3.6 3.6 3.6 3.7 3.7 50% 4 2.5
Continuity of Service Risk Rating 4
Indicitive
CONTINUITY OF SERVICE RISK RATING
50 of 132
8. CAPITAL PROGRAMME
The Trust had planned to commit £7,444k on its capital budget for 2013/14, which includes the reinvestment of some of the proceeds of planned disposals. However, Monitor have a number of financial risk indicators which are reported in the Trust’s quarterly submission. One indicator is triggered if capital expenditure is less than 85% of the year to date plan. The Trust’s month 3 position, as reported in the Q1 return, failed this test as the year to date capital spend only equated to 42% of planned spend, and as expected that Monitor has mandated that the Trust submit a revised capital plan. The Trust’s Estates & Facilities and IT departments have revised the profile of their capital expenditure plans and the Trust is now forecasting an overall capital programme for 2013/14 of £6,754k. The revised forecast is reflected in Appendix F. Works on the South Camden Crisis House are progressing, though there are indications that completion may slip into early 2014 (though there has been agreed expansions of works to try and achieve a pre-Christmas delivery in response to this), while St Pancras remedial works continue. During month 7, the Trust spent £741k on its capital programme, with total year to date capital spend standing at £1,839k. This is behind the planned position by £147k YTD. The Trust has now completed the disposal of the 3 properties that were planned for 2013/14: The sale of Fordwych Road was completed in late July 2013, for £1,600k. In March 2013, as
part of the disposal process, the property was required to be revalued by the District Valuer. As a result, the valuation increased from £1,264k to £1,700k. The Trust’s financial position is therefore showing a book loss on disposal of circa £100k.
In August, Ashley Road was disposed of for £1,200k, against a book value of £675k. The disposal of Cleveland Street was completed in September, producing a capital receipt of
£2,475k which is significantly in excess of its book value of £1,180k. Therefore, the 3 disposals will achieve an aggregated profit on sale of circa £1,700k before costs of sale, and as a result the Trust has the financial flexibility to consider expanding the capital programme if required.
9. SUMMARY
The month 7 financial position shows an overall normalised surplus of £1,457k, and is in excess of plan by £289k. This is increased to an overall surplus position of £3,082k, when the impact of property disposals is included. At this stage of the year, the overall financial position is positive and does not constitute a material risk to the achievement of the financial plan. However, management action is needed to ensure that run rates are consolidated and the financial position maintained.
51 of 132

Appendix A
Business UnitAnnual
BudgetBudget Actual
Variance
(favourable)
/ adverse
13/14
Forecast
Outturn
13/14
Forecast
Variance
A B C D=C-B E F£'000 £'000 £'000 £'000 £'000 £'000
Income
1 Service Level Agreements (88,686) (51,733) (51,733) 0 (88,686) 0
2 Local Authority (16,964) (9,895) (9,895) 0 (16,964) 0
3 Education and Training (19,229) (11,217) (11,217) 0 (19,229) 0
4 Research and Development (2,584) (1,531) (1,531) 0 (2,584) 0
5 Other (1,448) (845) (739) 105 (1,398) 50
6 SUBTOTAL CENTRAL INCOME (128,910) (75,221) (75,116) 105 (128,860) 50
Expenditure
7 Operational Divisions 61,624 35,633 35,585 (48) 61,424 (200)
8 Camden Social Services 4,223 2,467 2,651 185 4,423 200
9 Islington Social Services 2,999 1,665 1,611 (54) 2,949 (50)
10 PWLD 1,303 760 760 0 1,303 0
11 Psychology SLAs 13,512 7,882 7,856 (26) 13,512 0
12 Subtotal Direct Services 83,661 48,407 48,463 56 83,611 (50)
13 Trust Headquarters (incl Central Medical and Training & Ed'n) 15,791 9,121 9,185 64 15,791 0
14 Central Services, SLA's & reserves 21,290 12,923 12,434 (489) 21,290 0
15 Subtotal Central Services 37,080 22,044 21,620 (424) 37,080 0
16 SUBTOTAL EXPENDITURE 120,741 70,451 70,083 (368) 120,691 (50)
17 NORMALISED EBITDA* (8,168) (4,770) (5,033) (263) (8,168) 0
18 Depreciation 3,874 2,260 2,260 0 3,874 0
19 Dividend Payment 2,405 1,403 1,403 0 2,405 0
20 Interest Received (121) (71) (97) (26) (121) 0
21 Interest - unwinding of discount on provisions 10 10 10 0 10 0
22 NORMALISED (SURPLUS) / DEFICIT** (2,000) (1,167) (1,457) (289) (2,000) 0
23 (Profit)/Loss on Sale 0 0 (1,626) (1,626) (1,626) (1,626)
24 RETAINED (SURPLUS) / DEFICIT (2,000) (1,167) (3,082) (1,915) (3,626) 0
FINANCIAL POSITION AS AT MONTH 7
Forecast
* Earnings Before Interest, Tax, Depreciation and Amortisation [calculated as line 6 less line 16]
**Normalised surplus excludes technical adjustment relating to profits/losses on sale of fixed assets, impairments of the Trust's Estate and any
restructuring costs in order to show the underlying position of the Trust
52 of 132

Appendix B
Line Ref Operational Service Annual Budget Budget Actual
Variance
(favourable) /
adverse
A B C D=C-B£'000 £'000 £'000 £'000
1 Acute Services 16,721 9,644 9,816 172
2 Community Mental Health 9,660 5,625 5,452 (173)
3 Rehabilitation & Recovery / Outreach 16,049 9,400 9,398 (2)
4 Services for Ageing & Mental Health 4,965 2,838 2,670 (168)
5 Substance Misuse & Forensic 7,760 4,529 4,248 (281)
6 Operational Services Management 6,469 3,597 4,000 403
7 TOTAL OPERATIONAL SERVICES 61,624 35,633 35,585 (48)
OPERATIONAL DIVISIONS EXPENDITURE POSITION AS AT MONTH 7
53 of 132

Appendix C
Current as at 31.03.13 Movement
A B C=A-B
£'000 £'000 £'000
NON CURRENT ASSETS
1 Property, plant and equipment 116,371 80,101 36,270
2 TOTAL NON CURRENT ASSETS 116,371 80,101 36,270
CURRENT ASSETS
3 Stocks 0 0 0
4 Receivables - NHS 5,106 3,041 2,065
5 Receivables - Non NHS 1,911 2,878 (967)
6 Non current assets held for sale 0 3,555 (3,555)
7 Cash at bank and in hand 54,503 47,821 6,682
8 TOTAL CURRENT ASSETS 61,520 57,295 4,225
CURRENT LIABILITIES
9 Payables - NHS (2,266) (8,198) 5,932
10 Payables - Non NHS (23,311) (16,068) (7,243)
11 Provisions for liabilities and charges (763) (1,308) 545
12 TOTAL CURRENT LIABILITIES (26,341) (25,574) (767)
NON CURRENT LIABILITIES
13 Provisions for liabilities and charges (186) (186) (0)
14 TOTAL NON CURRENT LIABILITIES (186) (186) (0)
15 TOTAL ASSETS EMPLOYED 151,364 111,636 39,728
TAXPAYERS EQUITY
16 Public dividend capital 66,533 59,048 7,485
17 Revaluation reserve 53,526 24,365 29,161
18 Income and expenditure reserve 31,305 28,223 3,082
19 TOTAL TAXPAYERS EQUITY 151,365 111,636 39,729
BALANCE SHEET AS AT MONTH 7
54 of 132

Appendix D
£'000
1 TOTAL OPERATING SURPLUS / (DEFICIT) 2,678
2 Depreciation 2,260
3 (Increase)/decrease in stocks 0
4 (Increase)/decrease in receivables (1,098)
5 Increase/(decrease) in payables 518
6 Increase/(decrease) in provisions (544)
7 NET CASH INFLOW / (OUTFLOW) FROM OPERATING ACTIVITIES 3,814
RETURNS ON INVESTMENTS AND SERVICING OF FINANCE:
8 Interest received 97
9 Interest paid 0
NET CASH INFLOW/(OUTFLOW) FROM RETURNS ON
10 INVESTMENTS AND SERVICING OF FINANCE 97
CAPITAL EXPENDITURE:
11 (Payments) to acquire fixed assets (1,409)
12 Receipts from sale of fixed assets 5,275
13 NET CASH INFLOW/(OUTFLOW) FROM CAPITAL EXPENDITURE 3,866
14 DIVIDENDS PAID (1,095)
15 NET CASH INFLOW/(OUTFLOW) BEFORE FINANCING 6,682
FINANCING:
16 New public dividend capital received 0
17 Public dividend capital repaid 0
18 NET CASH INFLOW/(OUTFLOW) FROM FINANCING 0
19 INCREASE/(DECREASE) IN CASH 6,682
CASH FLOW STATEMENT AS AT MONTH 7
55 of 132

Appendix E
CASH AND LIQUIDITY
£0.0m
£10.0m
£20.0m
£30.0m
£40.0m
£50.0m
£60.0m
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14Actual cash £50.0m £47.3m £50.3m £57.3m £49.4m £49.4m £54.5mPlanned cash £45.9m £43.9m £42.0m £40.7m £39.3m £38.0m £38.0m £38.0m £38.0m £38.7m £39.3m £40.0m
In year cash balances (including deposits)
56 of 132

Appendix F
13/14 Plan13/14
Committed
13/14
Actual
£'000 £'000 £'000
1 St Pancras Works 1,710 1,448 405Major building, plant, M&E repair, H&S works. Incl HQ consolidation, ward improvements & Traumatic Stress Clinic relocation
2 South Camden Crisis House - St Pancras Hospital
1,080 1,082 453 Nursery conversion at St Pancras Hospital, work progressing
3 Isledon Road Day Centre Internal Refurbishment
380 0 0 Internal refurbisment works
4 Margarete Centre Refurbishment 299 236 80 Internal & external refurbishment works & lift replacement
5 Camden Mews Day Centre Refurbishment 288 288 67 Day Centre internal refurbishment & boiler renewal works
6 Hanley Gardens Bedroom Refurbishment 221 221 82 Residential unit bedroom refurbishment works
7 Highgate Mental Health Centre 505 505 106 Investment and refurbishment works
8 ICT Schemes 1,344 750 228 Rolling ICT programme throughout 13/14
9 Other Service Use Based Refurbishments & Reconfigurations
927 1,395 418 Completion of minor schemes brought forward from 12/13 and rolling programme of works throughout 13/14
10 Total 6,754 5,925 1,839
Planned YTD Capex 1,986
CAPITAL PROGRAMME AS AT MONTH 7
57 of 132

58 of 132

Report To: Board of Directors (Public)
Paper Number: 4.3
Report For: Information
Report Type: Operational Performance
Date: 28 November 2013
Report Author: Adam Van Huet, Interim Workforce Planning and Information Manager
Report of: Claire Johnston, Director of Nursing & People
FoI Status: Report can be made public
Title: Human Resources and Workforce Performance Report – Quarter 2
2013-14
Executive Summary
The attached report r is the Human Resource and Workforce component of the Quarter 2 2013-14 Performance Report.
The report details the summary position for the Trust and the directorates, together with trend data. An implementation report on pension automatic enrolment is also included at the Board’s request. The points below capture the significant issues for quarter 2:
1. The sickness absence rate has reduced to 3.3%, 0.3% above our target of 3%.
2. The Trust vacancy rate as at the end of September 2013 reduced to 11.8%, following planned recruitment exercises, with divisions, and we are on track with further phasing against revised workforce plans, which are anticipated to reduce bank and agency spend.
3. Mandatory training compliance has improved significantly to 79.4% across the Trust, which is 0.6% from our target for year end. Compliance is continuing to increase during Quarter 3 and is currently above the 80% target.
4. The Trust is fully compliant with its legal obligations with regard to pension automatic enrolment and the financial impact has been minimal.
Recommendation to the Board
The Board of Directors is requested to:
note the Quarter 2 report.
59 of 132

2
Trust Strategic Priorities Supported by this Paper
Excellence
E2 Delivering the highest level of quality and financial performance.
Risk Implications
Any failure to implement good human resource management and workforce planning may adversely affect Trust performance.
Legal and Compliance Implications
CQC standards require good HR management practices.
Finance Implications
70% of the Trust’s expenditure is on its workforce and therefore good workforce management is essential to good financial performance.
Single Equalities Impact Assessment
This paper does not affect one group less or more favorably on the basis of race/ethnicity, disability, sex/gender, religion/belief, sexual orientation or age.
Requirement of External Assessor/Regulator
This report is not related to any specific requirements of any external assessor or regulator.
60 of 132

Produced by Human Resources
Human Resources and Workforce
Performance Report
2nd Quarter 2013-14 (July to September 2013)
61 of 132

PAGE 2 HR Performance Report 2nd Quarter 2013-14
Index
Trust and Directorate Summary 3-5
Trust Graph Dashboard including trends 6
Trust and Directorate Commentary 7
Data Definitions 8
RAG Ratings & Data Sources 9
Hot Topic: Pension Auto Enrolment 10
2nd Quarter 2013-14
62 of 132

PAGE 3
2nd Quarter 2013-14
Data for Quarter 2 2013/14 can be seen in the table below, the table on page 5 and the graphs on page 6. Narrative relating to these pages can be
found on page 7.
Please see the notes on page 4 for information relating to the above table.
Summary 2nd Quarter 2013-14 (Data)
Acute
Community Mental Health
R&R SAMH SMS & Fo-
rensics Corporate
Medical Di-rectorate
Other Total
Staff in Post (Headcount) as at 30th Sep 13
359 230 272 128 112 134 118 95 1448
Staff in Post (FTE) as at 30th Sep 13
340.14 189.31 251.15 118.94 106.93 127.54 109.08 76.55 1319.64
Budgeted Establishment (FTE) as at 30th Sep 13
399.22 200.53 309.93 145.33 127.01 124.00 109.52 80.17 1495.71
Vacancy Rate (%) as at 30th Sep 13
14.8% 5.6% 19.0% 18.2% 15.8% -2.9% 0.4% 4.5% 11.8%
Bank Use (FTE) Average for Q2 N.B. Agency Use not included
52.85 1.92 32.94 7.76 12.31 6.33 1.20 0.90 116.21
Bank Use (% of total establish-ment) Average for Q2
13.2% 1.0% 10.6% 5.3% 9.7% 5.1% 1.1% 1.1% 7.8%
Bank Spend (£) total for Q2
£453,228.94 £11,836.6 £250,995.4 £58,834.3 £106,565.1 £37,270.0 £101.6 £11,119.0 £929,950.9
Agency Spend (£) total for Q2
£15,466.4 £23,952.5 £82,477.8 £22,334.2 £57,290.6 £281,603.0 £58,896.5 £139,359.9 £681,380.8
Sickness Absence (%) total for Q2
4.9% 1.2% 4.7% 3.1% 3.3% 2.7% 2.5% 0.5% 3.3%
Sickness Absence Cost (£) total for Q2
£134,487.39 £18,387.58 £100,347.09 £31,913.15 £25,353.06 £37,109.19 £50,437.02 £6,557.36 £404,591.83
Staff Turnover (%) Quarterly 1st Jul - 30th Sep 13
1.4% 4.7% 5.3% 5.4% 5.3% 9.0% 0.8% 5.1% 4.2%
Mandatory Training (% compliant) as at 30th Sep 13
79.7% 80.6% 77.3% 91.0% 86.3% 71.0% 88.3% 59.5% 79.4%
63 of 132
PAGE 4
2nd Quarter 2013-14
Notes regarding the table on Page 3 The staff in post FTE and headcount information is sourced from ESR which feeds the Finance General Ledger with the actual FTE used in each Payroll period. The Budg-eted FTE information is held in the Finance General Ledger. Work has been done to map the information so that it reflects the current Trust structure and meetings are go-ing to be held with each of the Divisional Managers, HR and Finance to ensure that budgets are correct. All figures exclude trainee clinical psychologists, bank staff, career breaks, Trust staff on secondment to other organisations (external secondments), secondments to the Trust for whom the Trust is being recharged and honorary contracts. The structure reflects the new Divisions. The Medical Directorate is shown separately to the Corporate figures. ‘Other’ includes PWLD, Business Unit staff, Psychology SLAs, trainee mental health workers and sponsored nursing students. These are as per the cost centre codings in the Trust Structure. Bank use (FTE), bank cost and agency cost are sourced from the Finance Ledger. N.B. the data for the FTE of Agency usage is not currently available and therefore not shown. The bank spend for the Medical Directorate is a combination of bank and agency spend as this is how Finance report on it. Medical bank/ agency FTE and Spend in the SMS and Forensic Divison has been incorporated in the figures for the Medical Directorate. Sickness absence cost is calculated as the cumulative based absence cost (OSP/ OMP adjusted) plus the cumulative employers cost (OSP/ OMP adjusted). The turnover figure is the total for the 3 month period. Turnover is based upon staff that leave the Trust completely, it does not include internal movement of staff. The RAG rating for mandatory training has been altered following discussions with the Executive which bring them in line with other organisations and NHS London targets. Please refer to page 11 for details of the data definitions to understand the calculations behind the figures. The RAG ratings and data sources can be found on page 12.
Summary 2nd Quarter 2013-14 (Data)
64 of 132
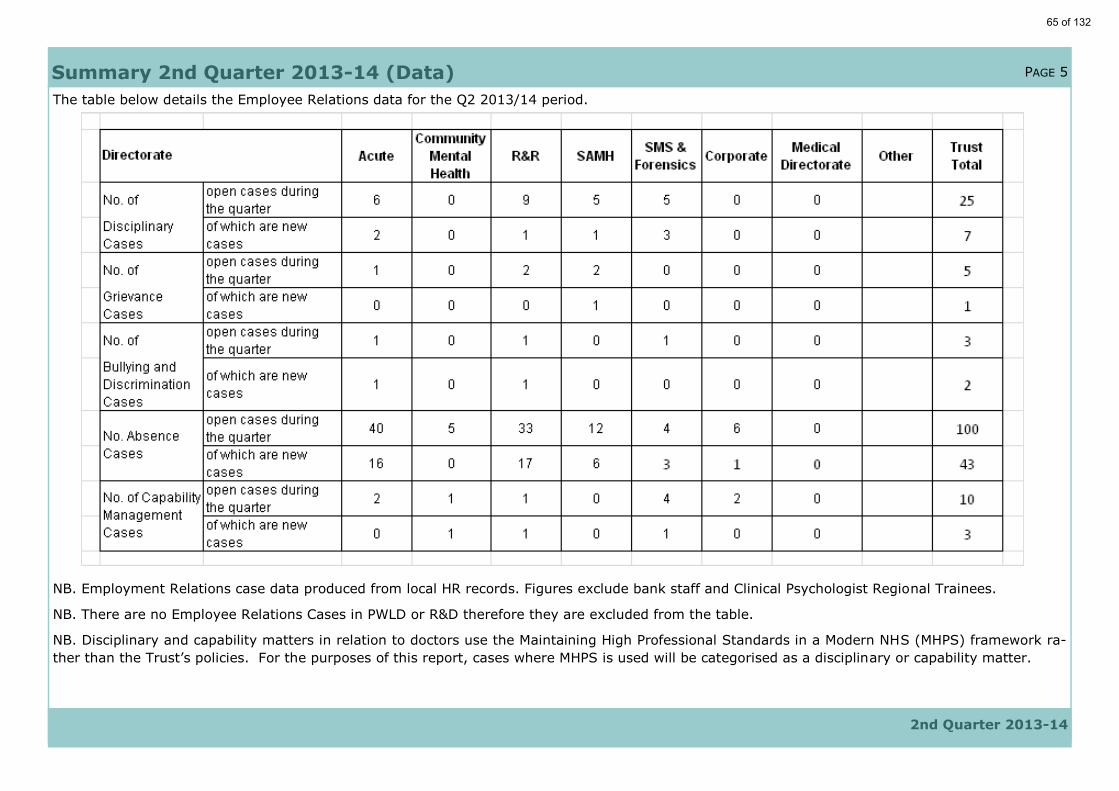
PAGE 5
2nd Quarter 2013-14
The table below details the Employee Relations data for the Q2 2013/14 period.
NB. Employment Relations case data produced from local HR records. Figures exclude bank staff and Clinical Psychologist Regional Trainees.
NB. There are no Employee Relations Cases in PWLD or R&D therefore they are excluded from the table.
NB. Disciplinary and capability matters in relation to doctors use the Maintaining High Professional Standards in a Modern NHS (MHPS) framework ra-
ther than the Trust’s policies. For the purposes of this report, cases where MHPS is used will be categorised as a disciplinary or capability matter.
Summary 2nd Quarter 2013-14 (Data)
65 of 132

PAGE 6
2nd Quarter 2013-14
.
Trust Graph Dashboard
Data sources:- Establishment - Finance; Bank Use - Bank Department and NHS Professionals report; All other information sourced from ESR.
Commentary
relating to the
graphs on this
page and the
tables on
page 3 and 5
can be found
on page 7.
66 of 132

PAGE 7
2nd Quarter 2013-14
The Trust’s vacancy rate has shown significant improvement over the last six months, falling from 17% at the end of the last financial year to 11.8% in quarter 2 of this year. All divisional rates are under 20%, with the highest being 19% in Recovery and Rehabilitation and the lowest being 5.6% in Community Mental Health. Significant recruitment activity has been undertaken in the Acute division, with Wave 1 of the Acute Mass Recruitment Plan complete and Wave 2 underway. The vacancy rate in Acute has fallen from 19.6% at 2012-13 year end to 14.8% in quarter 2 of this year and it is anticipated that the Mass Recruitment Plan will have further impact in quarter 3, and that bank and agency spend will fall accordingly. The Recovery and Rehabilitation division will embark on their mass recruitment plan in November 2013, which is anticipat-ed to reduce their vacancy rate and subsequently, bank and agency expenditure.
Although turnover in quarter 2 has increased slightly compared with the particularly low figure for the last quarter, the current level is typical of the trend over the last year.
Sickness absence rates in all five divisions have fallen, although the Trust rate remains above the Trust’s target of 3%, with Acute at 4.9%, Re-covery and Rehabilitation at 4.7%, Substance Misuse and Forensic Services at 3.3% and Services for Ageing and Mental Health at 3.1%. Fur-ther work to identify issues, root causes and solutions in teams with high absence rates in ongoing.
Mandatory training rates have shown significant improvements across the five divisions, with compliance over 75% in all divisions. Compliance in Community Mental Health is at 80.6%, in Substance Misuse and Forensic Services is 86.3% and in Services for Ageing and Mental Health is 91%. Rates will continue to be monitored at monthly Performance Meetings to ensure compliance across all divisions meets Trust targets and is maintained.
Summary 2nd Quarter 2013-14 (Commentary)
67 of 132
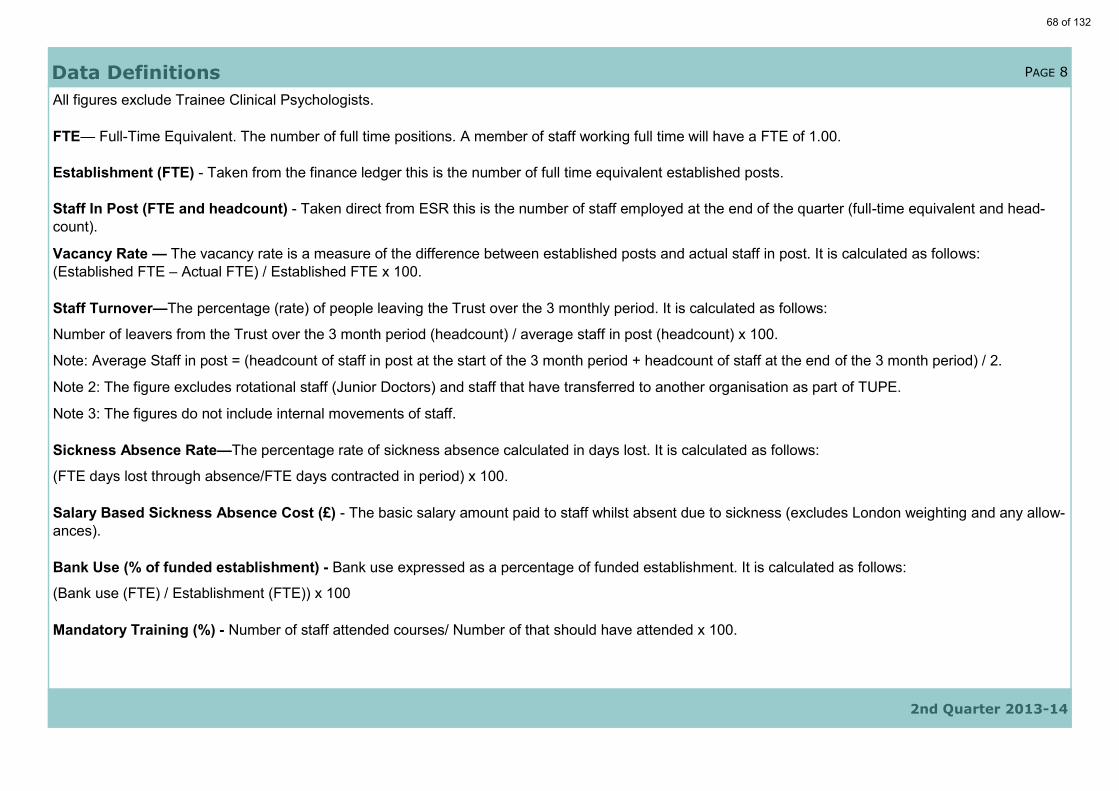
PAGE 8
All figures exclude Trainee Clinical Psychologists.
FTE— Full-Time Equivalent. The number of full time positions. A member of staff working full time will have a FTE of 1.00.
Establishment (FTE) - Taken from the finance ledger this is the number of full time equivalent established posts.
Staff In Post (FTE and headcount) - Taken direct from ESR this is the number of staff employed at the end of the quarter (full-time equivalent and head-
count).
Vacancy Rate — The vacancy rate is a measure of the difference between established posts and actual staff in post. It is calculated as follows:
(Established FTE – Actual FTE) / Established FTE x 100.
Staff Turnover—The percentage (rate) of people leaving the Trust over the 3 monthly period. It is calculated as follows:
Number of leavers from the Trust over the 3 month period (headcount) / average staff in post (headcount) x 100.
Note: Average Staff in post = (headcount of staff in post at the start of the 3 month period + headcount of staff at the end of the 3 month period) / 2.
Note 2: The figure excludes rotational staff (Junior Doctors) and staff that have transferred to another organisation as part of TUPE.
Note 3: The figures do not include internal movements of staff.
Sickness Absence Rate—The percentage rate of sickness absence calculated in days lost. It is calculated as follows:
(FTE days lost through absence/FTE days contracted in period) x 100.
Salary Based Sickness Absence Cost (£) - The basic salary amount paid to staff whilst absent due to sickness (excludes London weighting and any allow-
ances).
Bank Use (% of funded establishment) - Bank use expressed as a percentage of funded establishment. It is calculated as follows:
(Bank use (FTE) / Establishment (FTE)) x 100
Mandatory Training (%) - Number of staff attended courses/ Number of that should have attended x 100.
Data Definitions
2nd Quarter 2013-14
68 of 132

PAGE 9
RAG rating details (table page 3) The RAG rating for mandatory training has been altered following discussions with the Executive which bring them in line with other organisations. Trust targets to reduce both sickness absence and bank use are reflected in the scoring parameters set for both these areas. Vacancy rate RAG ratings have been set at a level that takes account of the need to keep some vacancies open for potential redeployments from organisational change, whilst safely running services. RAG ratings have not been used for staff in post data but the vacancy rate rating can be used as an indication for performance in this area as the measures are closely linked.
Data Sources (table Page 3)
Measure Green Amber Red
Vacancy Rate <15% 15%-20% >20% or
Bank Use (% of funded establish- <10% 10%-14% >14%
Sickness Absence Rate <3% 3%-3.5% >3.6%
Staff Turnover (annual) <16% 16%-20% >20%
Mandatory Training >80% 68%-79% <68%
Data Definitions
2nd Quarter 2013-14
Data Item Data Source
Establishment (FTE) Finance Ledger
Staff in Post (Headcount & FTE) ESR
Bank Use (FTE) Bank Department and NHS Professionals
Bank & Agency Spend (£) Finance Ledger
Sickness Absence (% and £) ESR
Turnover % (Leavers and Headcount) ESR
Mandatory Training ESR/ OLM
69 of 132
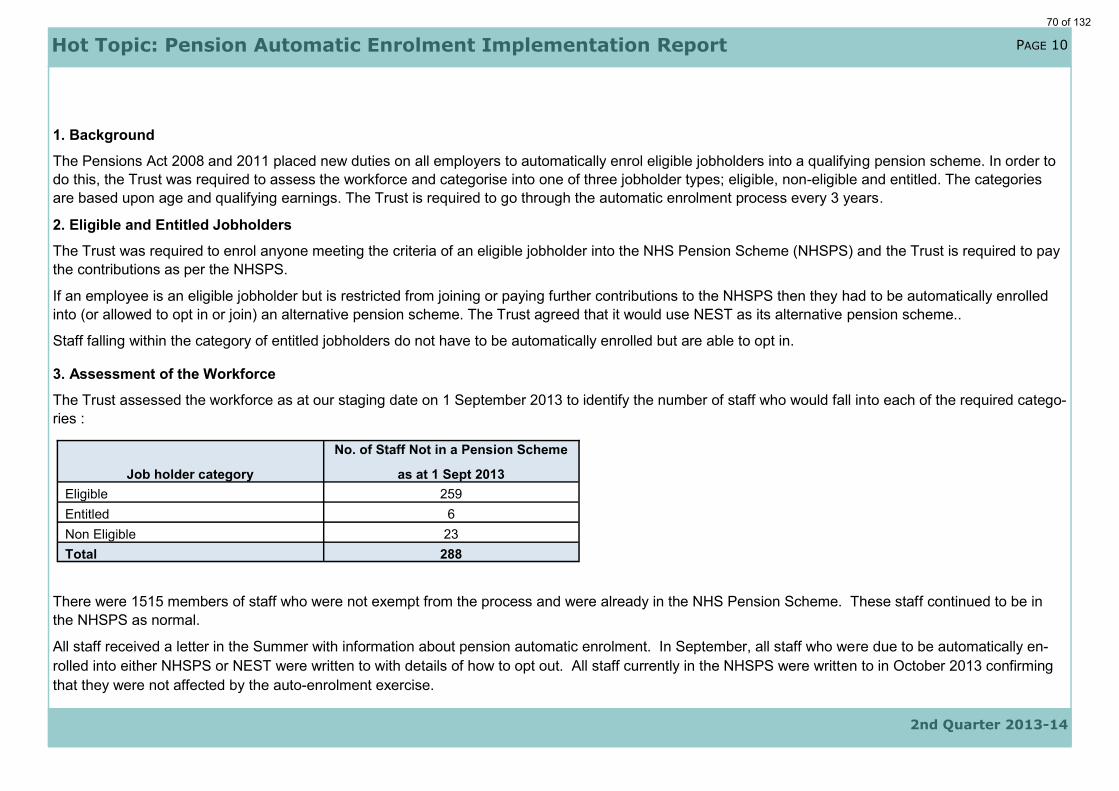
PAGE 10
2nd Quarter 2013-14
1. Background
The Pensions Act 2008 and 2011 placed new duties on all employers to automatically enrol eligible jobholders into a qualifying pension scheme. In order to
do this, the Trust was required to assess the workforce and categorise into one of three jobholder types; eligible, non-eligible and entitled. The categories
are based upon age and qualifying earnings. The Trust is required to go through the automatic enrolment process every 3 years.
2. Eligible and Entitled Jobholders
The Trust was required to enrol anyone meeting the criteria of an eligible jobholder into the NHS Pension Scheme (NHSPS) and the Trust is required to pay
the contributions as per the NHSPS.
If an employee is an eligible jobholder but is restricted from joining or paying further contributions to the NHSPS then they had to be automatically enrolled
into (or allowed to opt in or join) an alternative pension scheme. The Trust agreed that it would use NEST as its alternative pension scheme..
Staff falling within the category of entitled jobholders do not have to be automatically enrolled but are able to opt in.
3. Assessment of the Workforce
The Trust assessed the workforce as at our staging date on 1 September 2013 to identify the number of staff who would fall into each of the required catego-
ries :
There were 1515 members of staff who were not exempt from the process and were already in the NHS Pension Scheme. These staff continued to be in
the NHSPS as normal.
All staff received a letter in the Summer with information about pension automatic enrolment. In September, all staff who were due to be automatically en-
rolled into either NHSPS or NEST were written to with details of how to opt out. All staff currently in the NHSPS were written to in October 2013 confirming
that they were not affected by the auto-enrolment exercise.
Job holder category
No. of Staff Not in a Pension Scheme
as at 1 Sept 2013
Eligible 259
Entitled 6
Non Eligible 23
Total 288
Hot Topic: Pension Automatic Enrolment Implementation Report
70 of 132

PAGE 11
2nd Quarter 2013-14
4. Cost
The Trust is required to pay contributions in line with the NHSPS or the NEST scheme in regards to eligible jobholders (to be auto enrolled) and non-eligible
jobholders (who can choose to opt in). Entitled workers can join a pension scheme, however, the Trust does not have to make contributions on their behalf.
For employees enrolled in to the NHSPS the Trust is required to make the 14% employer contribution as per the rules of the scheme. For employees en-
rolled into NEST, the contribution is initially 1%, rising to 2% in October 2017 and 3% in October 2018.
As at the Trust’s staging date on 1 September 2013, four employees were automatically enrolled into NEST, however, three opted out before any deductions
were made. 205 staff were automatically enrolled into the NHSPS and 108 have since opted out, with 103 receiving refunds through payroll. The other five
opt out decisions were received after the close of the opt out window and will be refunded by NHS Pensions.
The pre-automatic enrolment NHSPS costs were £625,987.81 in August 2013. This rose to £691,676.94 in September. However, once the opt outs were
processed in October and the Trust was reimbursed for these in the amount of £50,000, the costs fell to £603,281.67 (including the £50,000 refund). The on-
going costs of pension automatic enrolment therefore appear to be around £30,000 to £40,000 per month or £500,000 per year. Finance will continue to be
advised of the costs each month.
5. Legal Compliance
The Trust was legally obliged to comply with various elements of the process. All our legal obligations have been met within the required timeframes.
Hot Topic: Pension Auto-Enrolment
71 of 132

72 of 132

Report To: Trust Board (Public)
Paper Number: 4.4
Report For: Decision
Report Type: Strategy
Date: 28 November 2013
Report Author: Peter Gooch, Associate Director of ICT
Report of: David Wragg, Director of Finance
FoI Status: Report can be made public
Title: C&I Information & Communications Technology Strategy 2013 to
2016 Executive Summary:
The purpose of this document is:
to present the Camden & Islington NHS Foundation Trust (C&I) ICT Strategy for 2013 to 2016, which covers information and communications technology, and the development projects within the Trust;
to gain the Trust Board’s approval for the ICT Strategy; and
to define the key activities, resource implications and associated costs to delivering the Information, Communication & Technology (ICT) Strategy, within the ICT Department’s area.
This forward strategy also has some key objectives built within it reflecting a legal requirement to replace the current Electronic Patient Record (EPR) System, RiO. The core objectives are:
to ensure that the trust safely migrates onto a new EPR solution prior to October 2015 with minimal impact on clinical and operational services;
to leverage existing ICT investments rather than introduce unnecessary additional new technologies. This approach supports staff resource challenges associated with the first objective; and
to continue to deploy flexible mobile solutions to facilitate more agile working practices across all Trust locations and services.
Recommendation to the Board
The Board of Directors is requested to:
approve the C&I Information & Communications Technology Strategy 2013 to 2016 strategy.
73 of 132

Trust Strategic Priorities Supported by this Paper:
Excellence
E1 Continually improve the quality and safety of service delivery, service user experience and improving outcomes.
E2 Delivering the highest level of quality and financial performance.
Innovation
I1 Rapidly adopt best practice and maintain a culture of innovation in service development.
Growth
G1 Pursue organic and inorganic growth opportunities through strategic partnerships and research and development.
Risk Implications:
The paper relates to a corporate risk relating to the requirement to replace the Trusts Electronic Record System.
Legal and Compliance Implications:
The paper supports the annual IT Toolkit Return requirements and Monitor reporting.
Single Equalities Impact Assessment
The paper does not affect one group less or more favorably on the basis of race/ethnicity, disability, sex/gender, religion/belief, sexual orientation or age.
Requirement of External Assessor/Regulator
No external assessor requirement.
74 of 132

Camden & Islington NHS Foundation Trust
ICT Strategy 2013/2016 (V0.6)
Mr Peter Gooch Associate Director of ICT November 2013
75 of 132

1 Document Control
1.1.1 Document Status This is a controlled document. Information here summarises the specific workstream activities associated with the over-arching ICT Strategy.
Document Title
C&I ICT Strategy 2013/16
File path\Filename Format Comments
C&I to determine and insert the file path and location of this document
MS Word
Main Document
1.1.2 Document Change History
Version Date Author Title Reviewed by Description of Changes
Draft 4/2/2013
Peter Gooch
AD ICT N/A New Content Added
V0.01 24/4/2013
Peter Gooch
AD ICT N/A New Content Added
V0.02 25/4/2013
Peter Gooch
AD ICT T. Evans, J.Artigstall,
M.Tailor
New Content Added Edits and proof reading
V0.03 29/4/2013
Peter Gooch
AD ICT David Wragg SIRO & FD
SIRO Review & Input
V0.04 Oct 2013
Peter Gooch
AD ICT CEO, NED Exec
CEO & NED Review & Input
V0.05 Nov 2013
Peter Gooch
AD ICT FTE FTE review new content added
V0.06 Nov 2014
Peter Gooch
AD ICT David Wragg SIRO & FD
New content
1.1.3 Document Information Document Title : C&I ICT Strategy 2013/16 Aim:
To gain the Board’s approval for the ICT Strategy.
To define the key activities, resource implications and associated costs to delivering the strategy.
Document Supports: Trust Business Plan and Strategic Objectives at Camden and Islington NHS Foundation Trust (C&I) Summary:
Sets out the ICT Work Programme over the next three (3) years. Sets out the ICT priorities and costs. Sets out Risks.
76 of 132

C&I ICT Strategy 2013 / 16 3
Recommendations:
Consider the cost and benefits of implementing the ICT Strategy at C&I. Review the ICT Strategy Projects, Timescales and costs against the Plan. That the Trust Project Board approves the ICT Strategy 2013/16.
1.1.4 Document Review This document requires a review from:
Name Role Review Date Signature
David Wragg Senior Responsible Owner (SRO)
ICT Sub Committee Project Governance TBC
1.1.5 Document Approval This document requires an approval from:
Name Role Approval Date Signature
David Wragg Senior Responsible Owner (SRO)
DD/MM/YYYY
ICT Sub Committee Project Governance DD/MM/YYYY 1.1.6 Location of Final Version
Copy Keeper Area Purpose Media
1 ICT Dept CIFT Trust Shared Drive Master Electronic
2 Electronic MHR’s CIFT Trust Shared Drive Reference Electronic 1.1.7 Responsibilities Classification Project Management Office Document
Distribution ICT Sub Committee, IG and Risk Management Department
Ownership C&I - ICT Department
Maintenance ICT Project Management Office
77 of 132
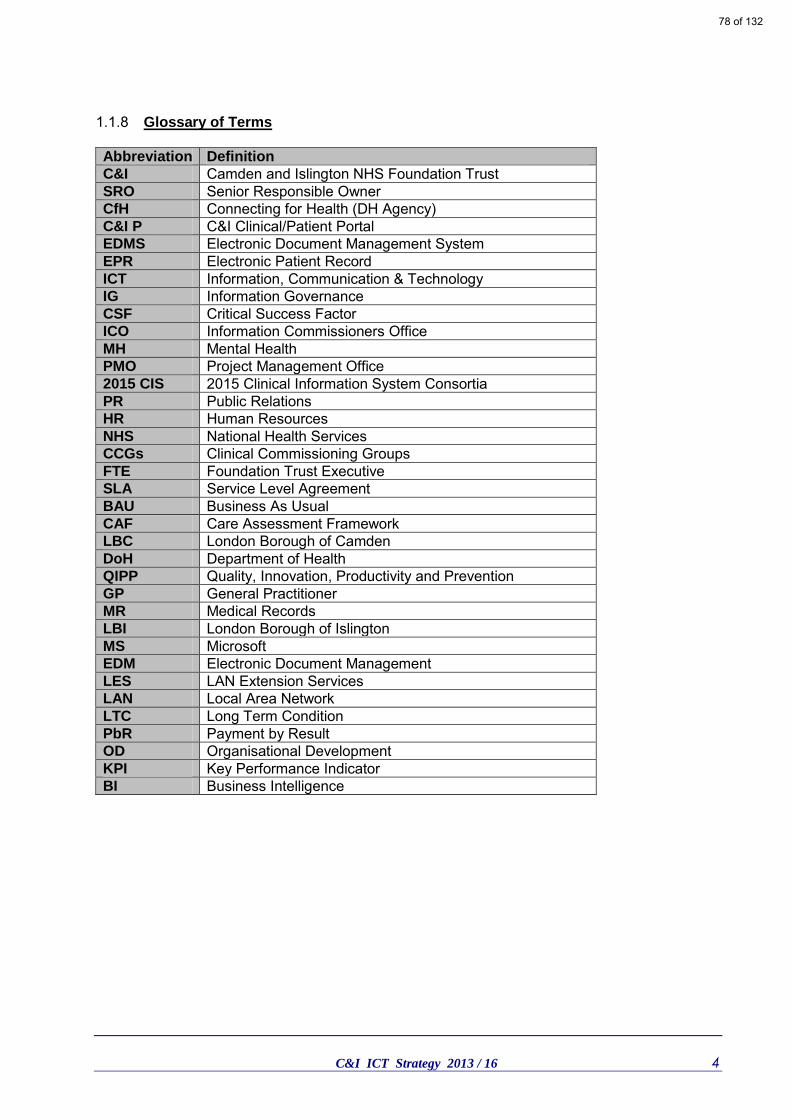
C&I ICT Strategy 2013 / 16 4
1.1.8 Glossary of Terms Abbreviation Definition
C&I Camden and Islington NHS Foundation Trust SRO Senior Responsible Owner CfH Connecting for Health (DH Agency) C&I P C&I Clinical/Patient Portal EDMS Electronic Document Management System EPR Electronic Patient Record ICT Information, Communication & Technology IG Information Governance CSF Critical Success Factor ICO Information Commissioners Office MH Mental Health PMO Project Management Office 2015 CIS 2015 Clinical Information System Consortia PR Public Relations HR Human Resources NHS National Health Services CCGs Clinical Commissioning Groups FTE Foundation Trust Executive SLA Service Level Agreement BAU Business As Usual CAF Care Assessment Framework LBC London Borough of Camden DoH Department of Health QIPP Quality, Innovation, Productivity and Prevention GP General Practitioner MR Medical Records LBI London Borough of Islington MS Microsoft EDM Electronic Document Management LES LAN Extension Services LAN Local Area Network LTC Long Term Condition PbR Payment by Result OD Organisational Development KPI Key Performance Indicator BI Business Intelligence
78 of 132
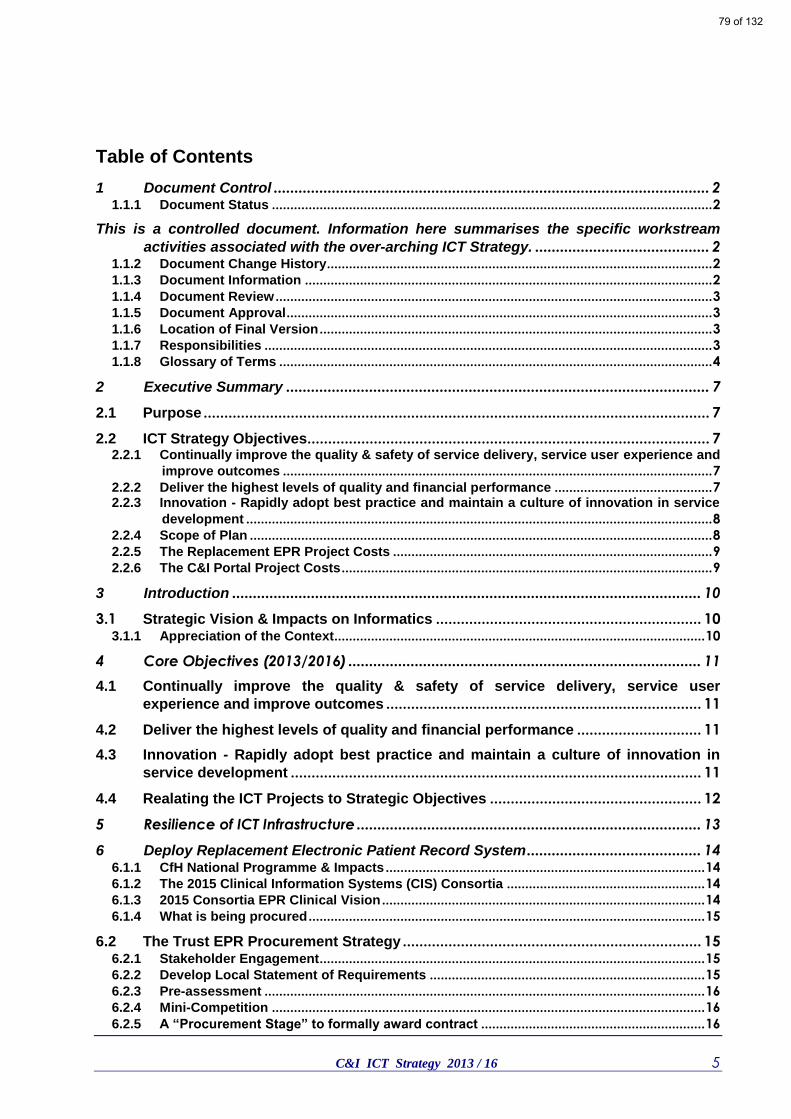
C&I ICT Strategy 2013 / 16 5
Table of Contents
1 Document Control ......................................................................................................... 2 1.1.1 Document Status ........................................................................................................................ 2
This is a controlled document. Information here summarises the specific workstream
activities associated with the over-arching ICT Strategy. .......................................... 2 1.1.2 Document Change History ......................................................................................................... 2 1.1.3 Document Information ............................................................................................................... 2 1.1.4 Document Review ....................................................................................................................... 3 1.1.5 Document Approval .................................................................................................................... 3 1.1.6 Location of Final Version ........................................................................................................... 3 1.1.7 Responsibilities .......................................................................................................................... 3 1.1.8 Glossary of Terms ...................................................................................................................... 4
2 Executive Summary ...................................................................................................... 7
2.1 Purpose .......................................................................................................................... 7
2.2 ICT Strategy Objectives................................................................................................. 7 2.2.1 Continually improve the quality & safety of service delivery, service user experience and
improve outcomes ..................................................................................................................... 7 2.2.2 Deliver the highest levels of quality and financial performance ........................................... 7 2.2.3 Innovation - Rapidly adopt best practice and maintain a culture of innovation in service
development ............................................................................................................................... 8 2.2.4 Scope of Plan .............................................................................................................................. 8 2.2.5 The Replacement EPR Project Costs ....................................................................................... 9 2.2.6 The C&I Portal Project Costs ..................................................................................................... 9
3 Introduction ................................................................................................................. 10
3.1 Strategic Vision & Impacts on Informatics ................................................................ 10 3.1.1 Appreciation of the Context..................................................................................................... 10
4 Core Objectives (2013/2016) ..................................................................................... 11
4.1 Continually improve the quality & safety of service delivery, service user
experience and improve outcomes ............................................................................ 11
4.2 Deliver the highest levels of quality and financial performance .............................. 11
4.3 Innovation - Rapidly adopt best practice and maintain a culture of innovation in
service development ................................................................................................... 11
4.4 Realating the ICT Projects to Strategic Objectives ................................................... 12
5 Resilience of ICT Infrastructure ................................................................................... 13
6 Deploy Replacement Electronic Patient Record System .......................................... 14 6.1.1 CfH National Programme & Impacts ....................................................................................... 14 6.1.2 The 2015 Clinical Information Systems (CIS) Consortia ...................................................... 14 6.1.3 2015 Consortia EPR Clinical Vision ........................................................................................ 14 6.1.4 What is being procured ............................................................................................................ 15
6.2 The Trust EPR Procurement Strategy ........................................................................ 15 6.2.1 Stakeholder Engagement ......................................................................................................... 15 6.2.2 Develop Local Statement of Requirements ........................................................................... 15 6.2.3 Pre-assessment ........................................................................................................................ 16 6.2.4 Mini-Competition ...................................................................................................................... 16 6.2.5 A “Procurement Stage” to formally award contract ............................................................. 16
79 of 132
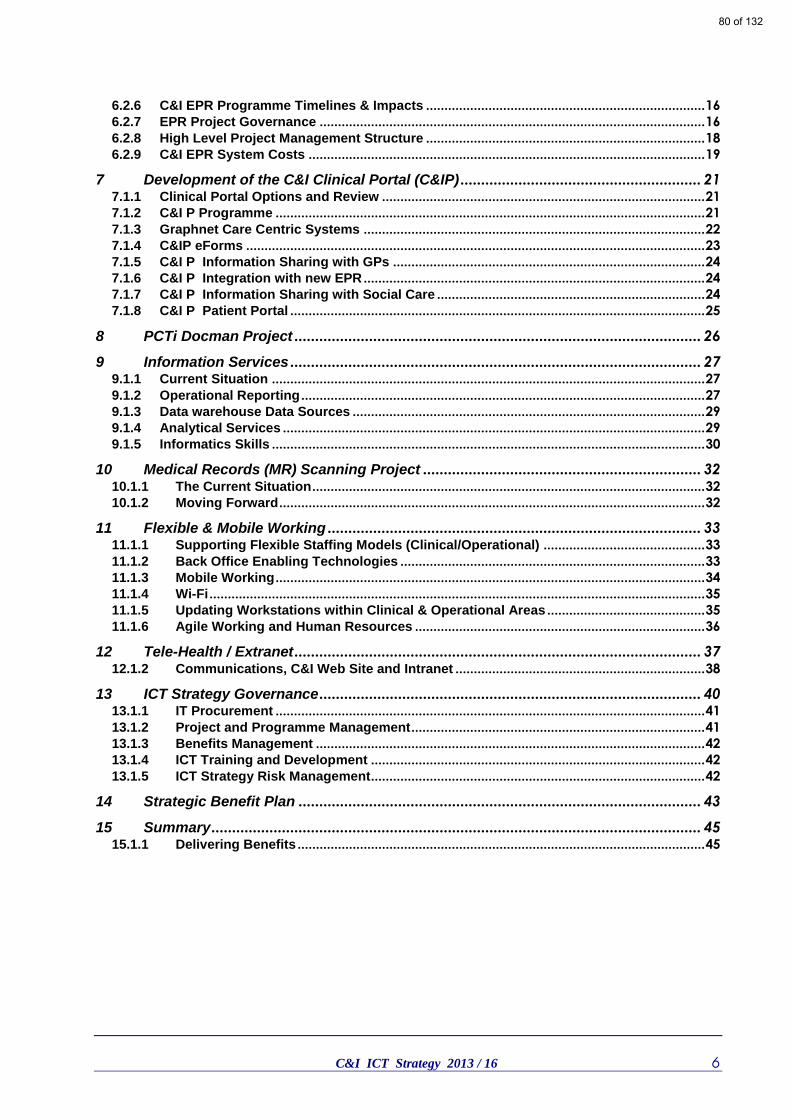
C&I ICT Strategy 2013 / 16 6
6.2.6 C&I EPR Programme Timelines & Impacts ............................................................................ 16 6.2.7 EPR Project Governance ......................................................................................................... 16 6.2.8 High Level Project Management Structure ............................................................................ 18 6.2.9 C&I EPR System Costs ............................................................................................................ 19
7 Development of the C&I Clinical Portal (C&IP) .......................................................... 21 7.1.1 Clinical Portal Options and Review ........................................................................................ 21 7.1.2 C&I P Programme ..................................................................................................................... 21 7.1.3 Graphnet Care Centric Systems ............................................................................................. 22 7.1.4 C&IP eForms ............................................................................................................................. 23 7.1.5 C&I P Information Sharing with GPs ..................................................................................... 24 7.1.6 C&I P Integration with new EPR ............................................................................................. 24 7.1.7 C&I P Information Sharing with Social Care ......................................................................... 24 7.1.8 C&I P Patient Portal ................................................................................................................. 25
8 PCTi Docman Project .................................................................................................. 26
9 Information Services ................................................................................................... 27 9.1.1 Current Situation ...................................................................................................................... 27 9.1.2 Operational Reporting .............................................................................................................. 27 9.1.3 Data warehouse Data Sources ................................................................................................ 29 9.1.4 Analytical Services ................................................................................................................... 29 9.1.5 Informatics Skills ...................................................................................................................... 30
10 Medical Records (MR) Scanning Project ................................................................... 32 10.1.1 The Current Situation ........................................................................................................... 32 10.1.2 Moving Forward .................................................................................................................... 32
11 Flexible & Mobile Working .......................................................................................... 33 11.1.1 Supporting Flexible Staffing Models (Clinical/Operational) ............................................ 33 11.1.2 Back Office Enabling Technologies ................................................................................... 33 11.1.3 Mobile Working ..................................................................................................................... 34 11.1.4 Wi-Fi ....................................................................................................................................... 35 11.1.5 Updating Workstations within Clinical & Operational Areas ........................................... 35 11.1.6 Agile Working and Human Resources ............................................................................... 36
12 Tele-Health / Extranet .................................................................................................. 37 12.1.2 Communications, C&I Web Site and Intranet .................................................................... 38
13 ICT Strategy Governance ............................................................................................ 40 13.1.1 IT Procurement ..................................................................................................................... 41 13.1.2 Project and Programme Management ................................................................................ 41 13.1.3 Benefits Management .......................................................................................................... 42 13.1.4 ICT Training and Development ........................................................................................... 42 13.1.5 ICT Strategy Risk Management ........................................................................................... 42
14 Strategic Benefit Plan ................................................................................................. 43
15 Summary ...................................................................................................................... 45 15.1.1 Delivering Benefits ............................................................................................................... 45
80 of 132

C&I ICT Strategy 2013 / 16 7
2 Executive Summary
2.1 Purpose
The purpose of this document is:- To present the Camden & Islington NHS Foundation Trust (C&I) ICT Strategy 2013/2016. To gain the Board’s approval for the ICT Strategy. To define the key activities, resource implications and associated costs to delivering the
Information, Communication & Technology (ICT) Strategy. This forward strategy also has some key objectives built within it reflecting a legal requirement to replace the Electronic Patient Record (EPR) System, RiO. The core objectives are: To ensure that the trust safely migrates onto a new EPR solution prior to October 2015
with minimal impact on clinical and operational services. To leverage existing ICT investments rather than introduce additional new technologies.
This approach supports staff resource challenges associated with the first objective. To continue to deploy flexible mobile solutions to facilitate more agile working practices
across all Trust locations and services.
2.2 ICT Strategy Objectives
The ICT Strategy cannot be seen in isolation of the core business and development strategies of the Trust. In effect it is a sub-set strategy that helps facilitate; meeting the wider strategic objectives within the Business Plan.
2.2.1 Continually improve the quality & safety of service delivery, service user experience and improve outcomes
ICT objectives: Improve the quality and safety of clinical information and decisions through having
maximum information about service users easily and clearly accessible in one place. Improve the communication between staff working with service users in various agencies
to improve quality and safety through quicker and easier electronic means. Enable service users independent access to their care plans and records. Facilitate the electronic collection and analysis of outcomes measures.
2.2.2 Deliver the highest levels of quality and financial performance
ICT objectives:
Improve Trusts delivery of quality and performance through easy to use dashboards with comprehensive live and summary performance information at staff member, service user, team, divisional and Trust level.
Ensure the informatics functions fully support the MHPbR, contracting, information reporting and business functions of the Trust.
Ensure the administrative burden of clinical information recording is reduced to the minimum.
Ensure the business systems of the Trust are fully supported, fit for purpose and integrated where required.
81 of 132

C&I ICT Strategy 2013 / 16 8
2.2.3 Innovation - Rapidly adopt best practice and maintain a culture of innovation in service
development
ICT objectives:
Support the development of mobile and flexible working through technology. Develop telemedicine and ICT solutions which enable self-care, self-monitoring and
treatment. Develop solutions that put the service user at the centre of everything. Over the last three years, the Board of C&I have made considerable investment in new ICT Infrastructures that have facilitated considerable change in working practices and culture throughout the Trust. Service led demand for more flexible and agile working solutions has been driven by previous investments in flexible mobile working solutions. More and more staff have now adopted working practices were reliance upon a physical desk and space within a health centre is becoming increasingly irrelevant. In three years we have moved from thirty-five (35) laptops to four hundred and fifty plus (450+) laptops, shortly to be increased by an additional one hundred (100) tablet devices. For every single (1) desktop PC purchased we buy four (4) laptop/tablet devices. All mobile devices are encrypted and underpinned by fast, secure remote access solutions allowing access to systems from anywhere within the UK. These investments have allowed C&I to work beyond its traditional geographical boundaries and to take advantage of virtual working uninhibited by geographical location. This current ICT Strategy will continue to support C&I’s growth potential and support working in new locations and service areas.
2.2.4 Scope of Plan
The key priority of the current strategy is to continue to focus on building upon the previous investments already made and ensuring the return on those investments are achieved. Some of the key objectives facilitated by the plan are: (Highest Priority) Deploy a replacement Electronic Patient Record (EPR) Solution by
October 2015. The other priority is the C&I Clinical & Patient Portal which has a number of key objectives:
Facilitates longitudinal care pathways involving multiple organisations within the care community.
Supports an approach that puts the patient at the centre of their own care and provides a Service User sub-Portal providing access, and input, into key elements of their care (i.e. care plans, medications etc.).
Supports Trust working outside geographical boundaries, extending service reach. Provides fall-back contingency of patient information access during EPR migration.
Further expand mobile and flexible working linked to changing Estate locations and operational and service priorities.
Further deploy electronic information sharing with GP’s to new practices and areas. Improved scope and analysis of data, reporting and dashboards. Further development of Tele-health & Extranet Solutions. Deployment of faster network Cable Modems to Tier 4 sites (small locations/low
headcount). Replacement of old Mitel Phone switches with two updated resilient switches. Introduce replacement IT services due to administration of 2E2 UK Ltd.
82 of 132

C&I ICT Strategy 2013 / 16 9
Throughout the Strategy, other systems and workstreams are identified with associated actions. However, it is the two major programmes, EPR and C&I Portal, that will be pivotal to the Trusts service delivery, development and approach for a number of years. The importance of these two systems and the impact on the Trust future development should not be underestimated.
2.2.5 The Replacement EPR Project Costs
The Outline Business Case for the EPR Project recommended two main choices for the Trust, which were: Option 2 Do Minimum - Procure a system that provides the same level of capabilities and functions as currently provided by RiO (National Programme) and other EPR systems e.g. PCMIS used by the Trust Psychology service and Advantage (NTDMS) substance misuse services. The Trust can consider a systems replacement on a like-for-like basis. This would provide a similar level of functionality and service capability as at present, but would nevertheless, incur additional capital and revenue support costs, owing to the Department of Health (DoH) central contract and termination. Option 3 Enhanced System - Procure systems and services that make maximum use of the best and most cost-effective available IT support tools to support the transformation in care that is the declared aim of the Trust. In order to evaluate the options in terms of their economic value the capital and revenue costs along with the estimated cash releasing savings were been discounted to present day values. This sets out the discount calculation for the net present costs (NPC) and equivalent annual costs (EACs) for each option. The cost of both options was evaluated over a seven (7) year period. The Trust also intends to explore with NHS partners from within the London and South RiO Replacement 2015 Consortium, whether a further joint procurement by a subset of the group would improve price, quality and optimum implementation date.
2.2.6 The C&I Portal Project Costs
The development of a clinical portal is a long-term strategic programme which has multiple dependencies and constraints due to multi-agency working and the complexity of longitudinal patient pathways of care across a health economy and beyond. Further investment and decisions regarding the Clinical Portal should be addressed once the Trust has decided which EPR system it wishes to migrate onto. The variety of different EPR system approaches and functionalities means that some systems may already partially address Portal requirements. The Trust already has a Clinical Portal but would require additional investment to enable it to be developed further, especially around Patient Portal requirements. This additional investment would be approximately £350k and would save the Trust on the 2015 CIS Consortia costs.
83 of 132

C&I ICT Strategy 2013 / 16 10
3 Introduction
The purpose of this document is:- To present the Camden & Islington NHS Foundation Trust ICT Strategy 2013/2016.
To gain the Board’s approval for the ICT Strategy.
To define the key activities, resource implications and associated costs to delivering the strategy.
3.1 Strategic Vision & Impacts on Informatics
3.1.1 Appreciation of the Context
One of the greatest changes to the National Health Services (NHS) in twenty-five (25) years came into effect in April 2013. These key changes dismantled most of the health service’s policy and commissioning bodies, including the National Programme for IT in the NHS. The changes brought in a new focus on public health through a new agency, Public Health England. A NHS Commissioning Board, now called NHS England, has been formally setup. The Board will be responsible for specialist and primary care commissioning, as well as the NHS Outcomes Framework that provides NHS performance information to the Health Secretary. Within ICT a new Patients and Information Directorate will be responsible for commissioning and sponsoring new digital services for the NHS, including a customer service platform to replace NHS Direct and NHS Choices and a new online service NHS 111. It will be responsible for commissioning new standards and information governance for the NHS that will have a significant impact on the development of healthcare IT in the future. Two hundred and twelve (212) Clinical Commissioning Groups (CCGs) have commenced work and these new bodies are also responsible for GP IT. Many of the CCGs will have IT, information and analysis support from nineteen (19) commissioning support units as suppliers of commissioning, HR, finance, analysis and IT. The former NHS Information Centre has become the Health and Social Care Information Centre and has a role as the ‘safe haven’ for patient identifiable data, and the repository of the ‘single version of the truth’ that the government has promised on NHS performance. At the time of writing this strategy in October 2013, the detail and actually working arrangements of many of the organisations mentioned are still being formulated. We are in a period of great change and considerable upheaval which will take time to settle down.
84 of 132
C&I ICT Strategy 2013 / 16 11
4 Core Objectives (2013/2016)
The ICT Strategy cannot be seen in isolation of the core business and development strategies of the Trust. In effect it is a sub-set strategy that helps facilitate; meeting the wider strategic objectives within the Business Plan.
4.1 Continually improve the quality & safety of service delivery, service user experience and improve outcomes
ICT objectives:
Improve the quality and safety of clinical information and decisions through having maximum information about service users easily and clearly accessible in one place.
Improve the communication between staff working with service users in various agencies to improve quality and safety through quicker and easier electronic means.
Enable service users independent access to their care plans and records. Facilitate the electronic collection and analysis of outcomes measures.
4.2 Deliver the highest levels of quality and financial performance
ICT objectives:
Improve Trusts delivery of quality and performance through easy to use dashboards with comprehensive live and summary performance information at staff member, service user, team, divisional and Trust level.
Ensure the informatics functions fully support the MHPbR, contracting, information reporting and business functions of the Trust.
Ensure the administrative burden of clinical information recording is reduced to the minimum.
Ensure the business systems of the Trust are fully supported, fit for purpose and integrated where required.
4.3 Innovation - Rapidly adopt best practice and maintain a culture of innovation in service
development
ICT objectives:
Support the development of mobile and flexible working through technology. Develop telemedicine and ICT solutions which enable self-care, self-monitoring and
treatment. Develop solutions that put the service user at the centre of everything.
85 of 132
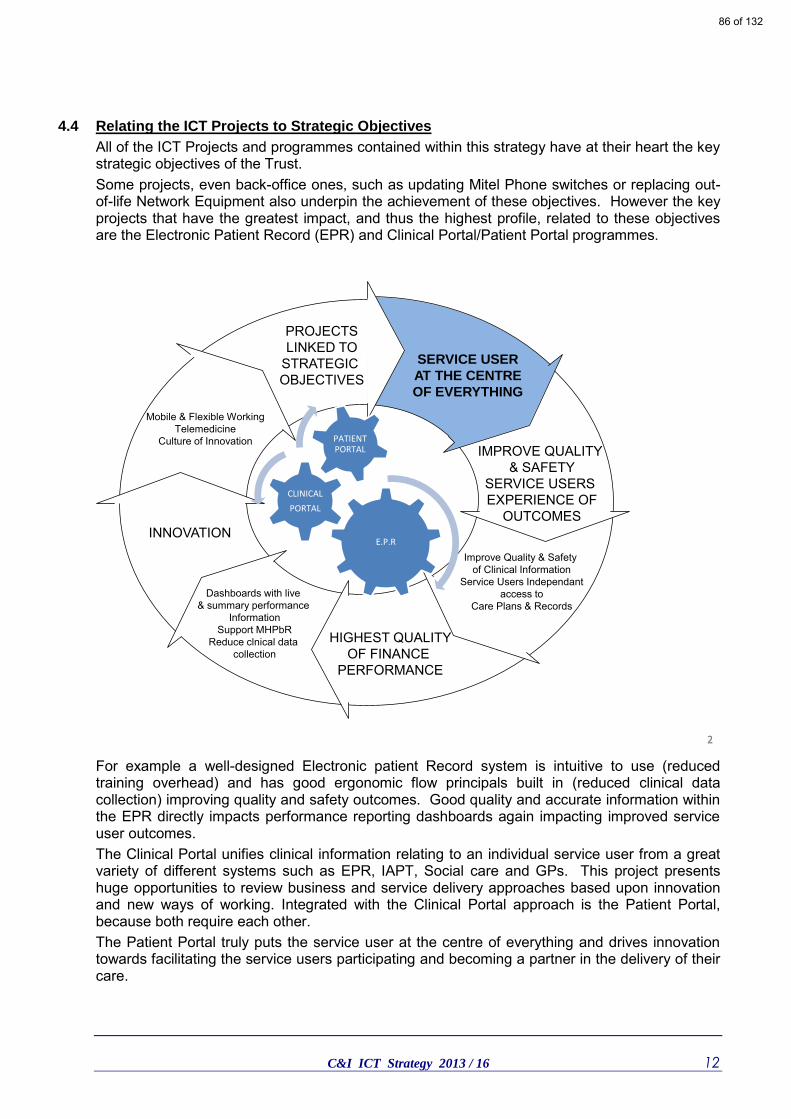
C&I ICT Strategy 2013 / 16 12
4.4 Relating the ICT Projects to Strategic Objectives
All of the ICT Projects and programmes contained within this strategy have at their heart the key strategic objectives of the Trust. Some projects, even back-office ones, such as updating Mitel Phone switches or replacing out-of-life Network Equipment also underpin the achievement of these objectives. However the key projects that have the greatest impact, and thus the highest profile, related to these objectives are the Electronic Patient Record (EPR) and Clinical Portal/Patient Portal programmes.
2
Text
Text
Text
2
PROJECTSLINKED TO
STRATEGIC OBJECTIVES
Improve Quality & Safety of Clinical Information
Service Users Independantaccess to
Care Plans & Records
SERVICE USER
AT THE CENTRE
OF EVERYTHING
IMPROVE QUALITY & SAFETY
SERVICE USERS EXPERIENCE OF
OUTCOMES
HIGHEST QUALITYOF FINANCE
PERFORMANCE
Dashboards with live & summary performance
InformationSupport MHPbR
Reduce clnical data collection
INNOVATION
Mobile & Flexible WorkingTelemedicine
Culture of Innovation
E.P.R
CLINICAL
PORTAL
PATIENT PORTAL
For example a well-designed Electronic patient Record system is intuitive to use (reduced training overhead) and has good ergonomic flow principals built in (reduced clinical data collection) improving quality and safety outcomes. Good quality and accurate information within the EPR directly impacts performance reporting dashboards again impacting improved service user outcomes. The Clinical Portal unifies clinical information relating to an individual service user from a great variety of different systems such as EPR, IAPT, Social care and GPs. This project presents huge opportunities to review business and service delivery approaches based upon innovation and new ways of working. Integrated with the Clinical Portal approach is the Patient Portal, because both require each other. The Patient Portal truly puts the service user at the centre of everything and drives innovation towards facilitating the service users participating and becoming a partner in the delivery of their care.
86 of 132
C&I ICT Strategy 2013 / 16 13
5 Resilience of ICT Infrastructure
Considerable investment has been made in the Technical Infrastructure at C&I over the last three (3) years. This has resulted in a step change improvement in reliability, speed and flexibility of systems for end-users. This has led to ICT services becoming an intrinsic part and supporting facilitator for service delivery across the Trust. The reliance on these systems being available is profound with little tolerance to non-availability being accepted. This could be perceived as a success criterion but, it comes with the caveat that increasing funding may have to be directed at ICT service resilience. The Trust will continue to embed a Flexible & Agile working agenda that has now become a normal part of day-to-day working practices within many operational areas of the Trust. Underpinning these flexible working practices are complex technical sub-systems which the Trust is constantly developing and refining. A capital investment programme in key technology systems ensures that current equipment is managed and maintained to prevailing technical standards and requirements whilst obsolete equipment is replaced. The Trust now has extremely good resilience within the data networks, data centres, telecommunications and reporting systems. There has been only a single instance of total service down time (of 2hrs) in three and a half (3.5) years with rare cases of service unavailability usually caused by National electrical grid failure in central London. The ICT Strategy integrates with the Estates & Facilities Strategy in ensuring that as sites are closed, improved or developed every opportunity is taken to ensure that the ICT Infrastructure is enhanced and optimised. For example installing more and more WiFi points so that a wide variety of mobile devices can be used, and new ways of working within existing buildings introduced. ICT will work closely with E&F to ensure a new E&F System is introduced that allows improved management of the Trust estate and has functionality to support innovations and new ways of working. The investments in these technologies have to be set against the criticality of current and new systems such as the EPR and Clinical Portal to service delivery. However, there also has to be an appreciation of demands upon investment within the Trusts Estates Infrastructure and the cost of secondary power generators at our multiple sites. The resilience is such that we are now in a position of reducing returns for further investment with a trade off in risk-vs-cost-vs-benefit.
87 of 132

C&I ICT Strategy 2013 / 16 14
6 Deploy Replacement Electronic Patient Record System
6.1.1 CfH National Programme & Impacts
The Trust is legally obliged to migrate off the RiO system provided under the Connecting for Health (CfH) National contracts by October 2015. However, the National CfH contracts are also attempting to deploy a new version of RiO called R2 in 2014. The following key issues have to be recognised: CfH RiO R2 project has slipped with three month delayed pilots only going live in October
2013. All follow-on Trusts will then deploy at some stage during 2014. Trusts migrating onto the new CfH RiO R2 version will potentially have to a start mini-
competition and deployment onto new EPR systems also in 2014, possibly within a few months of deploying RiO R2.
The deployment of RiO R2 clashes with the migration of Trusts onto new contracts procured with the 2015 Clinical Information Systems (CIS) Consortia.
CfH is currently reviewing a variety of impacts, issues and constraints inherent within the National Contracts. Clarity of some key issues has still to be resolved by CfH.
There are approximately 90 NHS Trust using CfH systems that will have to migrate onto new contracts/solutions by Oct 2015. The supplier marketplace has limited capacity and will struggle to resource such a volume. This means that some Trust may not be able to migrate off in time for CfH contract end and additional funding may be required to extend existing CfH contracts. The Department of Health (DoH) has been approach about potentially funding an extension period.
6.1.2 The 2015 Clinical Information Systems (CIS) Consortia
In 2012, Thirty (30) Trust across London and the South joined together to form the 2015 CIS Consortia. The purpose of the Consortia was to join together to undertake a procurement programme designed to create a Framework Agreement. The framework allows Trusts to rapidly procure a new EPR system by undertaking a twelve to sixteen (12-16) weeks mini-competition of suppliers on the framework. The first (1st) year of the Consortia has completed successfully with a new Framework Agreement in place for the Trusts to use. At the time of writing this strategy, the Consortia is running a second (2nd) year to support individual Trusts mini-competitions and Exit/Transition planning work from the old CfH Contracts. C&I is the host Trust for the new contract framework and are managing and leading the Consortia and currently the largest NHS EPR group procurement in the UK/Europe.
6.1.3 2015 Consortia EPR Clinical Vision
The NHS is entering a period of significant change and financial constraints. This brings a degree of uncertainty as to future requirements therefore the Consortia Trusts have highlighted that any new system/solution suppliers that the following are high on the agenda: o Patient-centred: the patient is able to determine and control their care, and their
interactions with the health system; o Networked: works in synergy with health, social care, third sector systems to provide an
overarching patient record; o Intelligent: able to extract and display data in clear numerical, written or graphical formats o Intuitive: simple, easy to use and does not require complex training. o Future-proof: able to adapt to changing platforms and end-user devices and capable of
supporting future development of integrated care systems. o Innovative: use of advanced technologies, e.g. tablets, Apps, mobile working, remote
telemedicine, etc.
88 of 132

C&I ICT Strategy 2013 / 16 15
o Flexible: to meet new approaches to patient care. o Agile: rapid system development to service evolving requirements. o Local: configuration and control by individual organisations. o Performance: high level of service performance with continuous improvement.
6.1.4 What is being procured
The procurement has been split into three (3) separate lots in order to provide each individual Trust with as much flexibility and choice as possible. The approach ensures these Trusts only purchase those services that they require, when they require them, and are not locked into large inflexible contracts. 1. The first lot is for application software along with deployment, change management and
maintenance to support the delivery of community health services, child health services and mental health services.
2. The second is for a robust, secure and flexible infrastructure to support the current and future needs of the participating trusts in relation to the running of the hosting arrangements.
3. The final lot will cover a full range of reporting, integration, interoperability and cross care functional modules and their associated services.
6.2 The Trust EPR Procurement Strategy
As the Framework Agreement is in place and indicative costs are known, an Outline Business Case will be presented to the Trust Board for approval, ahead of the tendering that the Trust will undertake against the Framework. The tendering exercise would conclude with the selection of preferred supplier(s), the finalisation of costs, and presentation of the Full Business Case (FBC) to the Trust Board for approval. The preferred Trust Procurement Strategy is to undertake 12 – 16 weeks of further competition to evaluate short-listed systems. The high level approach the project will undertake is as follows:
6.2.1 Stakeholder Engagement
An ‘Evaluation and Selection Committee’ will be established to undertake the evaluation process. Membership for this committee will be clinical and operational staff working across the five (5) divisions – Acute, Recovery and Rehabilitation, Services for Ageing and Mental Health, Substance Misuse and Forensic Services and Community Mental Health. This group will be focus on the Application and Reporting requirements, ensuring that the Trust selects the most appropriate solution(s) available. The core project team will be formed from appropriate groups of staff from across the Trust, thus ensuring all Trust groups: clinical, operational and technical, are represented during the evaluation process to short list the required products and services.
6.2.2 Develop Local Statement of Requirements
The Trust Evaluation & Selection Committee will have the opportunity to develop the Trust specific Statement of Requirements (SoRs) and amend the weighting criteria in line with local requirements and priorities. The Evaluation and Selection Committee will reuse the objective assessment and evaluation tools developed by the 2015 Consortium; a conservative estimate of the number of Trusts Clinicians, IT Directors and senior officers who have been involved in the process of capturing the requirements and developing the evaluation process and tools was circa 400.
89 of 132
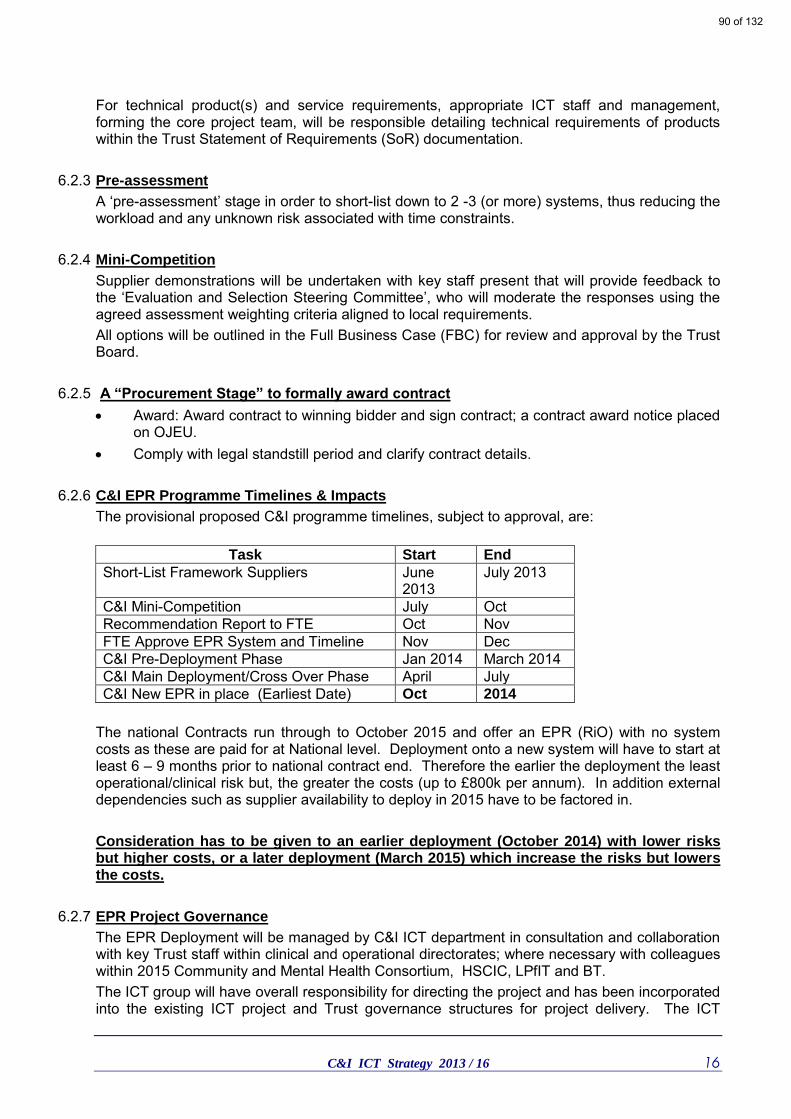
C&I ICT Strategy 2013 / 16 16
For technical product(s) and service requirements, appropriate ICT staff and management, forming the core project team, will be responsible detailing technical requirements of products within the Trust Statement of Requirements (SoR) documentation.
6.2.3 Pre-assessment
A ‘pre-assessment’ stage in order to short-list down to 2 -3 (or more) systems, thus reducing the workload and any unknown risk associated with time constraints.
6.2.4 Mini-Competition
Supplier demonstrations will be undertaken with key staff present that will provide feedback to the ‘Evaluation and Selection Steering Committee’, who will moderate the responses using the agreed assessment weighting criteria aligned to local requirements. All options will be outlined in the Full Business Case (FBC) for review and approval by the Trust Board.
6.2.5 A “Procurement Stage” to formally award contract
Award: Award contract to winning bidder and sign contract; a contract award notice placed on OJEU.
Comply with legal standstill period and clarify contract details.
6.2.6 C&I EPR Programme Timelines & Impacts
The provisional proposed C&I programme timelines, subject to approval, are:
Task Start End
Short-List Framework Suppliers June 2013
July 2013
C&I Mini-Competition July Oct Recommendation Report to FTE Oct Nov FTE Approve EPR System and Timeline Nov Dec C&I Pre-Deployment Phase Jan 2014 March 2014 C&I Main Deployment/Cross Over Phase April July C&I New EPR in place (Earliest Date) Oct 2014
The national Contracts run through to October 2015 and offer an EPR (RiO) with no system costs as these are paid for at National level. Deployment onto a new system will have to start at least 6 – 9 months prior to national contract end. Therefore the earlier the deployment the least operational/clinical risk but, the greater the costs (up to £800k per annum). In addition external dependencies such as supplier availability to deploy in 2015 have to be factored in. Consideration has to be given to an earlier deployment (October 2014) with lower risks but higher costs, or a later deployment (March 2015) which increase the risks but lowers the costs.
6.2.7 EPR Project Governance
The EPR Deployment will be managed by C&I ICT department in consultation and collaboration with key Trust staff within clinical and operational directorates; where necessary with colleagues within 2015 Community and Mental Health Consortium, HSCIC, LPfIT and BT. The ICT group will have overall responsibility for directing the project and has been incorporated into the existing ICT project and Trust governance structures for project delivery. The ICT
90 of 132

C&I ICT Strategy 2013 / 16 17
Group will be chaired by the Director of Finance, and will be attended by representatives for the Trust Executive team; this group will encompass ‘Project Board’ responsibilities for the Project In relation to the various stages of the local EPR Project, each stage will be subject to an approval process (“gateway”) at which the approval for the Project to proceed into the next stage will only be given when pre-set conditions have been met. At Trust local level, the overall Project Management will be with the Associate Director of ICT (designated as the PRINCE2, Project Assurance) and the Trust corporate responsibility for the Project will rest with the Director of Finance (designated as the PRINCE2, Senior Responsible Officer (SRO) to the Project). The project will update the Trust’s FT Board, Estates and Facilities Committee and the Executive management team with appropriate project documentation including Highlight and Exception reports. Delivery of the Project will be managed through an ICT Project Team, headed by the Project Manager, with management, administrative and clinical representatives from across the Trust. The Local Project Team will be led by a Project Manager with responsibility for the day-to-day management and delivery of the Project.
91 of 132
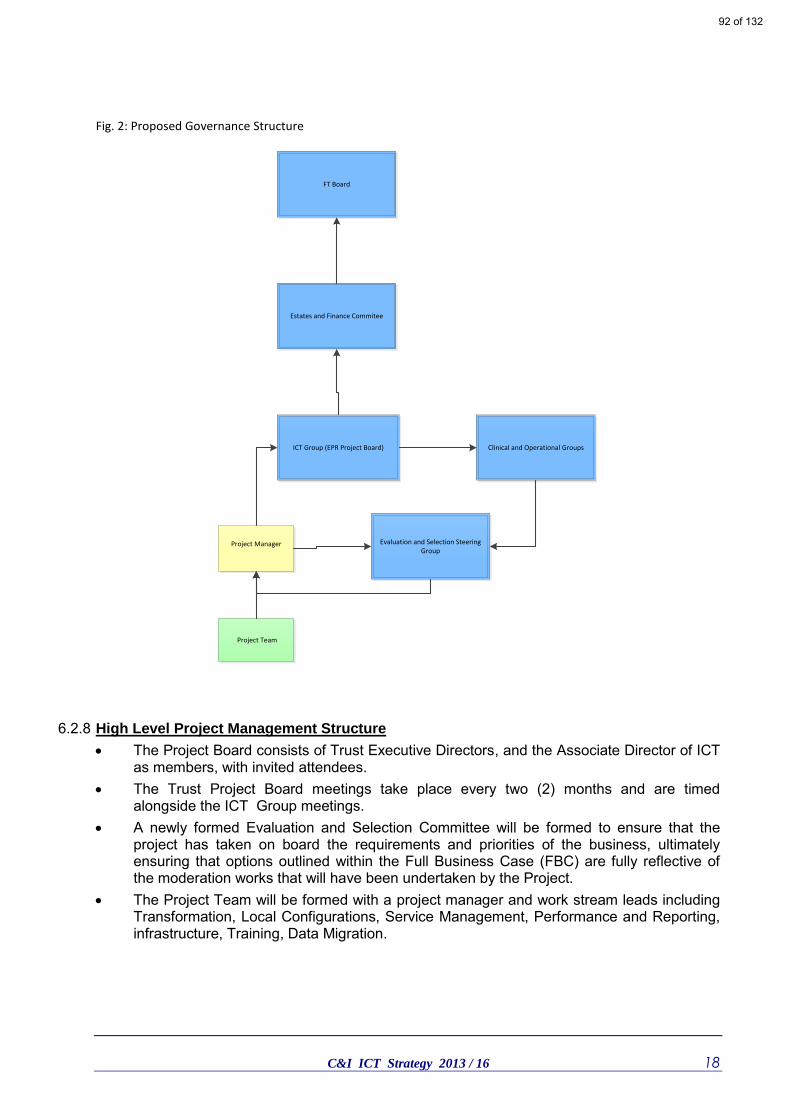
C&I ICT Strategy 2013 / 16 18
Fig. 2: Proposed Governance Structure
Project Manager
Project Team
ICT Group (EPR Project Board) Clinical and Operational Groups
Estates and Finance Commitee
FT Board
Evaluation and Selection Steering Group
6.2.8 High Level Project Management Structure
The Project Board consists of Trust Executive Directors, and the Associate Director of ICT as members, with invited attendees.
The Trust Project Board meetings take place every two (2) months and are timed alongside the ICT Group meetings.
A newly formed Evaluation and Selection Committee will be formed to ensure that the project has taken on board the requirements and priorities of the business, ultimately ensuring that options outlined within the Full Business Case (FBC) are fully reflective of the moderation works that will have been undertaken by the Project.
The Project Team will be formed with a project manager and work stream leads including Transformation, Local Configurations, Service Management, Performance and Reporting, infrastructure, Training, Data Migration.
92 of 132
C&I ICT Strategy 2013 / 16 19
6.2.9 C&I EPR System Costs
The following indicative costs (Fig 3) are based upon the mean average costs of the three lots derived from the 2015 CIS Framework tender responses. They take the mid-point average costs for medium Service Level Agreement (SLA) levels for a Trust of C&I’s size. The Outline Business Case for the EPR Project recommended two main choices for the Trust, which were: Option 2 Do Minimum - Procure a system that provides the same level of capabilities and functions
as currently provided by RiO (National Programme) and other EPR systems e.g. PCMIS used by the
Trust Psychology service and Advantage (NTDMS) substance misuse services.
The Trust can consider a systems replacement on a like-for-like basis. This would provide a similar
level of functionality and service capability as at present, but would nevertheless, incur additional
capital and revenue support costs, owing to the Department of Health (DoH) central contract and
termination.
Option 3 Enhanced System - Procure systems and services that make maximum use of the best and
most cost-effective available IT support tools to support the transformation in care that is the declared
aim of the Trust.
In order to evaluate the options in terms of their economic value the capital and revenue costs along with the estimated cash releasing savings were been discounted to present day values. This sets out the discount calculation for the net present costs (NPC) and equivalent annual costs (EACs) for each option. The cost of both options were evaluated over a seven (7) year period.
93 of 132

C&I ICT Strategy 2013 / 16 20
Key Cost Saving Options
The benchmark for the same systems and services through the National Programme CfH is £9m per Trust, so considerable saving have been made through the 2015 CIS Consortia tenders.
It should be noted that the Trust already has a well-structured Data Warehouse developed internally that supports multiple reporting facilities such as Qlickview electronic dashboards. The 2015 CIS Consortia tenders showed an average cost of £303k for a similar system.
A critical enabler technology to facilitate the EPR/ Clinical Vision expressed within the 2015 CIS Consortia tenders was for an Interface Engine. A high-level technology that facilitates complex electronic messaging between different computer systems. The Trust already has an Interface Engine and further investment in this technology is not required. The 2015 CIS Consortia tenders showed an average cost of £558k for a similar system.
The Trust already has a Clinical Portal but would require additional investment to enable it to be developed further, especially around Patient Portal requirements. This additional investment would be approximately £350k and would save the Trust on the 2015 CIS Consortia costs.
The Trust will have to undertake an appraisal using the 2015 Framework Lot 3 (Portal) contract to determine if it wishes to continue developing the current C&I Portal or start gain with a new Portal supplier.
94 of 132
C&I ICT Strategy 2013 / 16 21
7 Development of the C&I Clinical Portal (C&IP)
7.1.1 Clinical Portal Options and Review
Further investment and decisions regarding the Clinical Portal should be addressed once the Trust has decided which EPR system it wishes to migrate onto. The variety of different EPR system approaches and functionalities means that some systems may already partially address Portal requirements. The development of a clinical portal is a long-term strategic programme which has multiple dependencies and constraints due to multi-agency working and the complexity of longitudinal patient pathways of care across a health economy and beyond. The following paragraphs describe the current C&I Portal activities which have taken two years of constant effort to achieve. The achievements reference well to other similar projects within the health economy that are not as well advanced over similar timeframes.
7.1.2 C&I P Programme
During 2011/12, C&I was part of a National Demonstrator Pilot (11 in UK) working on a Care Assessment Framework (CAF) programme that shared MH data with the London Borough of Camden (LBC). As part of this programme the Trust installed both an Interface Engine and Portal/Repository application funded by the Department of Health (DoH). Now that the original CAF Project has completed, the Trust has used these two advanced applications to develop a wider strategy of electronic information sharing with partner organisations. The main focus of the C&I P is to collect a wide diversity of information from both electronic and paper based sources into a single unified patient record view. To achieve this, a great deal of high-end technical work utilising complex interface engine technology has been completed (see Fig. 4). To date the C&I P has the following links: All Patient Demographics transferred creating a Master patient Index of 85,000 records. All key RiO EPR patient files transferred nightly. Scanned Paper Based Medical Records linked to individual patient record. Two-way links to C&I Data Warehouse for reporting. Currently working on amalgamating IAPT/Psychology data.
95 of 132

C&I ICT Strategy 2013 / 16 22
INTERFACE ENGINE
ElectronicForms(Locally Configurable)
C&I Portal
Data Warehouse
OTHER SYSTEMSSocial Care3rd Sector
Prison - Etc
RIOAcute Hospital
GP’s
Elec
tro
nic
M
essa
gin
g
Pap
er D
ocu
men
ts
Scanned Medical Records &Document
Report Dashboards
C&I Portal
Safe GuardingTrips & FallsCQUIN DataNew Requirements
Figure 4: C&I Portal Information Flowchart
7.1.3 Graphnet Care Centric Systems
The C&I Repository/Portal is built using systems provided by Graphnet Ltd who provide systems to over 40 Trusts across the UK with over 20 million patients registered in Graphnet systems. The systems have expanded functionality to include shared electronic records between GPs, Acute Trusts, Community, Mental Health and more recently Local Authority service providers. Table showing systems Interfaced with Graphnet
GP Systems Acute Community Social Care
EMIS (PCS/LV/WEB) Ascribe Symphony RiO v1.1 Framework-i InPS PASɸ: iPm/Lorenzo, iCM,
Medway, Bedman, Ref Solution (iPM LE2.2), CaMIS Ultragenda
OOH: Adastra (single-sign-on)
CAF
Microtest Order Comms: Plumtree DART, HD Clinical Prism Telepath; Winpath; Anglia ICE; CRIS
Paris
iSoft; Synergy; Premiere; iSoft Ganymede
CareFirst
Exeter Demographics (Orglinks)
Liquid Logic
96 of 132
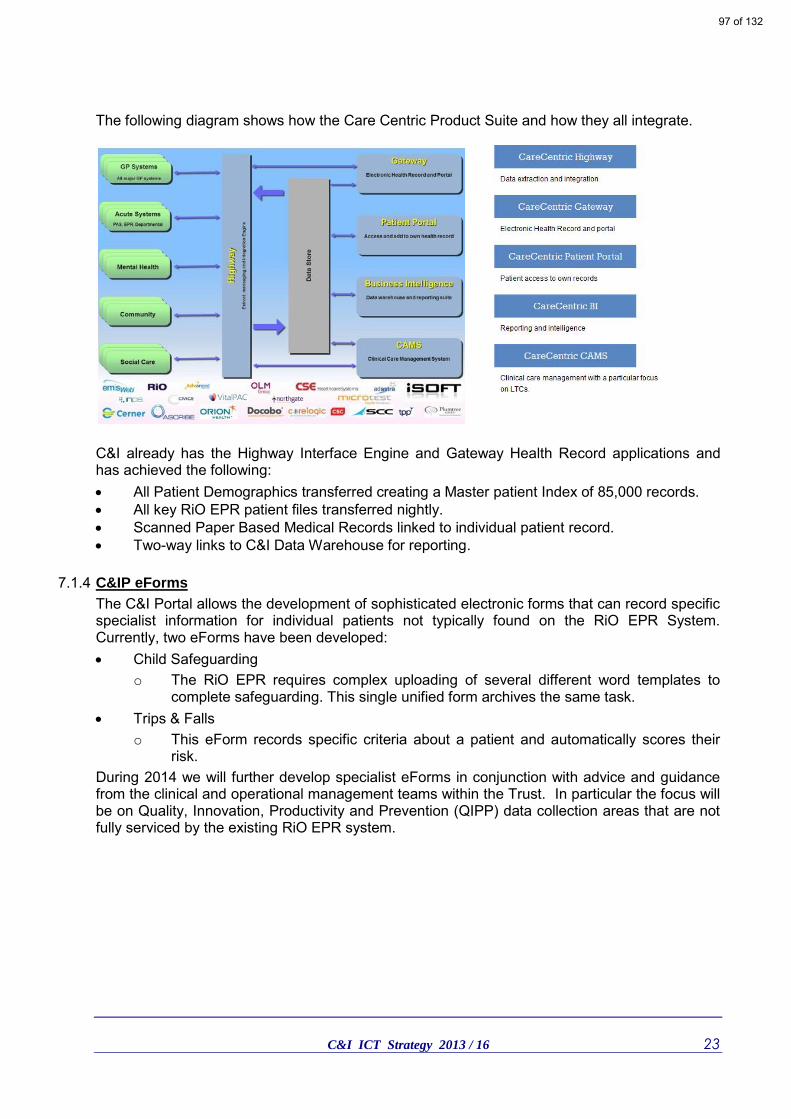
C&I ICT Strategy 2013 / 16 23
The following diagram shows how the Care Centric Product Suite and how they all integrate.
C&I already has the Highway Interface Engine and Gateway Health Record applications and has achieved the following: All Patient Demographics transferred creating a Master patient Index of 85,000 records. All key RiO EPR patient files transferred nightly. Scanned Paper Based Medical Records linked to individual patient record. Two-way links to C&I Data Warehouse for reporting.
7.1.4 C&IP eForms
The C&I Portal allows the development of sophisticated electronic forms that can record specific specialist information for individual patients not typically found on the RiO EPR System. Currently, two eForms have been developed: Child Safeguarding
o The RiO EPR requires complex uploading of several different word templates to complete safeguarding. This single unified form archives the same task.
Trips & Falls o This eForm records specific criteria about a patient and automatically scores their
risk. During 2014 we will further develop specialist eForms in conjunction with advice and guidance from the clinical and operational management teams within the Trust. In particular the focus will be on Quality, Innovation, Productivity and Prevention (QIPP) data collection areas that are not fully serviced by the existing RiO EPR system.
97 of 132

C&I ICT Strategy 2013 / 16 24
7.1.5 C&I P Information Sharing with GPs
The ICT Strategy has a two option approach to this challenge that allows flexibility around what GP Practice Patient Record System is being used (i.e. EMIS, TPP etc.) and how well GP Practices can support electronic links. These are:
1. The C&I Portal runs on an application supplied by Graphnet Ltd. Graphnet already collaborate with EMIS and have developed a two-way interface to share information.
2. Utilise the PCTi Docman solution to allow ‘drag and drop’ sharing of information with GP Practice Docman servers. PCTi has developed integration links with Graphnet Ltd; therefore, the option remains to link this solution into the C&I P.
The main constraint for fast roll-out of both these approaches will be C&I Technical resources and external GP IT Support services managed by the CCGs. C&I are about to embark on a deployment programme with all practices in the London Borough of Islington (LBI) to provide one-way (outbound) electronic information to GP’s. This programme follows on from CCGs GP IT Support and we would envisage it completing in early summer 2014. The two-way Graphnet to EMIS deployment could happen at any time but needs to phase in with the Docman LBI programme. So ideally this will be progressed during 2014–2015 to better balance with ICT technical resource constraints.
7.1.6 C&I P Integration with new EPR
The C&I P flowchart (Fig. 4) illustrates the integration with the current RiO EPR is undertaken through the Trusts Data Warehouse application. This has been deliberately done so that any change(s) of EPR means just changing the links to the Data Warehouse rather than the development of several complex technical interfaces.
7.1.7 C&I P Information Sharing with Social Care
This approach initially focuses upon getting a single data extraction feed (secure extract) from the London Borough of Camden (LBC) Core Logic system for inclusion in C&I Care Centric. The same approach and interface structures could be amended to also take a data feed from the London Borough of Islington (LBI) Social care system. The LBC Core Logic data can be unified within the C&I Portal repository against an individual service user record. In time the C&I Care Centric system will also potentially have additional information such as GP, LBI and Acute data all unified against a single service user/patient record. The approach does not attempt to send information back to LBC unless they want the existing CAF interface to LBC Core Logic switched on again. Instead C&I could provide C&I Portal access (RBAC role based) to participants within the local Health/Social Care economy. It should be noted that C&I Portal has far bettered security, access and audit controls than the RiO system.
98 of 132

C&I ICT Strategy 2013 / 16 25
7.1.8 C&I P Patient Portal
The Graphnet Care Centric system has a Patient Portal that lets patients log in from any Internet Browser and access their personal records. The system allows C&I to define the type of data which will be shared with patients and how it will be displayed. It includes all of the security controls you would expect from this type of solution including secure registration and high security password management. The Patient Portal is more than just a way to review appointments. It helps ensure that patients are more involved in the care they are receiving, which in turn improves both the quality of the record and health outcomes. Patient Portal features include: A registration administration function which ensures that the patient is identified and
verified before being allowed access to the system. The ability for the patient to view any documents or data made available for that purpose. A facility for the patient to enter data into the system and contribute to their own records. A facility for the patient to grant access to health care professionals outside of the local
care community. A complete audit trail of when patients log in and what they look at.
99 of 132

C&I ICT Strategy 2013 / 16 26
8 PCTi Docman Project
The Trust was the first Mental Health (MH) organisation within the UK to introduce the PCTi Docman application which facilitates the sharing of electronic patient information with GP Practices. In common with other ICT initiatives, it aims to reduce the administrative burden of clinical information recording to a minimum. Docman is a piece of software that enables the safe and efficient electronic transfer of Microsoft (MS) Word documents to GP’s. As C&I staff automatically creates a variety of assessment plans using the RiO Word templates; a version can be ‘drag-and-drop’ into an icon on their desktop screen.
Figure 6: Print screen shot of electronic document transfer icon
Some of the benefits are: • Faster communications with GP's of key patient information. • Reduction in costs (including admin time & postal charge). • Safer transfer of patient information. • Reduced reliance on fax machines to communicate information. 95% of all Camden GPs and 18% of Islington GPs are now receiving electronic patient information from C&I. During 2013/14 the CCG GP IT Support unit will roll-out PCTi Docman to all remaining Islington GP Practices. As the PCTi server is installed, C&I will follow-on and link it to our Trust clinical teams. The CCG roll-out and C&I roll-out will take until early 2014. Currently the following electronic reports are sent to GPs: • Referral acknowledgements and feedback letters. • CPA documents. • Admission Summaries. • Discharge summaries and notifications. • Assessments summaries. • Clinic letters. • Requests for further information.
100 of 132

C&I ICT Strategy 2013 / 16 27
9 Information Services
9.1.1 Current Situation
The overarching need for the Trust to co‐ordinate, standardise and maximise its use of operational data is articulated in the strategy. The Trust faces many internal and external pressures to provide management information of a higher quality, which is more timely, sometimes in new, yet to be defined, currencies, which can be analysed and reported easily and flexibly. The drivers behind this required “step change” in information management include mental health payment by results (MHPBR), new commissioning arrangements, requirements from the Care Quality commission and the performance management agenda within the Trust and wider health economy. Increased competition, service line management and the new divisions all require more information, outcome measurement, performance metrics, dashboards and benchmarks. This requires detailed records of what is being undertaken for each patient, so that the time and costs can be recorded systematically and analysed at a patient level. The Trust is responding to these pressures with initiatives to address: Operational reporting. Data warehouse, data sources and quality. Analysis tools and skills. Informatics skills.
9.1.2 Operational Reporting
A data warehouse has been developed internally, undergoing an upgrade to the industry standard SQL Server 2008R2 to offer greater resilience, performance and scalability. Loading of the data warehouse moved from a 3 day processing cycle, to an overnight load offering the timeliest access to data of any London mental health trust. The data warehouse delivers a single place for corporate data to be retrieved from, standard structured reports defined to enable the organisation at all levels to monitor performance and to support operational service delivery. At the presentation layer, benefits from previous investments where realised with the migration from over 220 legacy and undocumented Reporting Services reports down to just 6 Qlikview dashboards, allowing the presentation of 16 million data variants. Over time, data sources from all activity systems (i.e. IAPT), finance, commissioning and other sources will be linked to enable a consistent view of service delivery to be obtained, including service line costing and comprehensive modelling against planned activity. The results of this work has increased data use within all aspects of the Trust, demonstrating the power and value of good data and laid the foundation on which the Information Services department can further develop business intelligence. It is envisaged that changes to operational reports will come in four main areas.
101 of 132
C&I ICT Strategy 2013 / 16 28
Performance Framework
The existing core dashboards provide a wide range of metrics. The first area of development within the operational reporting is to augment the existing reports by alignment with the emerging Performance Framework within C&I. Building on the data controls and management now in place between Information Services and the business, consistent and accurate performance reporting can be developed within the Information department. Further operational reports can be consolidated to focus specifically on key performance indicators, allowing more timely and effective management of performance information. The performance framework, supported by adequate dashboards will become the principle way of managing operational performance. Linkage to service line performance and the emerging MH PBR tariff is also crucial to integrate activity and quality performance management, with resource control, costing and pricing. Responsiveness
The second area of development will be to ensure that operational reporting was response to changing demands. Initiatives such as the eForm development within the C&I Portal or the emergence of the new Clinical Commissioning Groups require a flexible and response approach to data provision. As the Trust moves to commissioning using Payment by Results, the ability to quickly develop and adapt reporting output to meet the needs of clinical services will be a key objective. As mental health in the NHS moves towards a more acute model of payment, the ability to quickly adjust reporting outputs to focus on areas of profitability or high costs has to be available to the Trust. As the conduit between data collection and service management, the Information Services department will need to ensure it remains responsive to controlled change. Increased Scope
Business intelligence maturity will increase within the Trust by the incorporation of additional data sources into operational reporting. Whether internal or external in origin, additional data will provide greater contextualisation to reports. Sources from across the health economy, via the integration engine within the C&I Portal or standard outputs from the Information Centre for Health and Social Care, need to be incorporated into standard reporting to increase richness. Specialisation
Finally, as operational reporting develops and in addition to the core performance outputs, a program of divisional or customer specific specialisation would be required. Whilst core KPIs remain, for improved clinical knowledge, service specific dashboards will be developed. Lead by divisions, this development lifecycle will be repeated to ensure that the necessary and appropriate information continues to be delivered in a timely and appropriate manner. This development would focus both internally and across the health and commissioning domain, to ensure the Trust provide appropriate information in a timely, accurate and secure manner.
102 of 132
C&I ICT Strategy 2013 / 16 29
9.1.3 Data warehouse Data Sources
To provide increasing maturity to operational reporting, a key initiative for Information Services over the course of this strategy is to consolidate existing data sources whilst adding new and varied additional data. Contract Changes
Core throughout this ICT strategy is the requirement to manage the clinical information system with the end of the Connecting for Health national contract in 2015. Depending on the direction the Trust wishes to take, there is a requirement to ensure both internal operational reports and external mandatory requirements are maintained. The development of the Qlikview report set and underlying data warehouse has already placed the Trust in a good position regarding a change in EPR. The data warehouse has been designed in such a way as to minimise this risk as much as possible, by ensuring that operational reporting are system agnostic. However, core functions of Information Service such as the delivery of the MHMDS, Commissioning Datasets, DH returns and commissioner requirements will need to be adjusted for any newly acquired clinical system. Data migration, changes in reference data, warehouse reconfiguration and training of IS staff all need to be considered with any change. This adjustment will be core to the Information Services department throughout 2014/15.
Additional data Sources
In addition to this BAU operation, it is vital for the Trust’s business intelligence maturity for a greater depth to be included into core reporting. As the NHS becomes a more competitive market place under PbR, this development of reporting is a necessity if C&I are to maintain their status amongst other trusts. To facilitate this, the Information Services department will run a series of agile development cycles to deliver projects incorporating additional data into the data warehouse. Requirements need to remain flexible and developed in conjunction with Trust colleagues, but at time of writing suggestions would include the following: ESR data, used to enhance corporate data quality and consolidate Performance
Framework reporting. RosterPro data, which can add value to any efficiency analysis and add additional insight
into clinical outcomes investigation. Datix data, again to allow consolidation with other performance reporting, or used to
contextualise information from other clinical systems. IAPTus, PC-MIS and DET data, which is all key C&I clinical services information, but
currently sits outside of the core Information remit. External data, such as published MHMDS, CQUIN or HES data, which adds maturity to
the information usage in the Trust by offering benchmarking opportunities. Data from the C&I Portal – eForms and data sourced from incoming Integration Engine
messages. The last requirement offers real benefit to service users by offering a holistic view of care across the health economies. As health and social care colleagues gather pace with integration and interoperability initiatives, C&I Information Services will be well places to incorporate this data into the data warehouse and therefore into operational reporting. The possibilities of data integration are almost limitless, and to help C&I achieve business intelligence maturity, with appropriate resourcing, Information Services will be prepared to take this opportunity.
9.1.4 Analytical Services
103 of 132

C&I ICT Strategy 2013 / 16 30
As the plans outlined above materialise and C&I’s business intelligence matures, the Trust can begin to realise the value in its data. The information collected across the Trust can be harnessed to drive forward clinical improvements. Through developments in ICT and specifically Information Services, this will be achieved by introducing the following features. Benchmarking
As mentioned previously, the ability and need to benchmark the Trust has never been greater. PbR commissioning along with the structural changes with the introduction of Clinical Commissioning Groups will result in greater scrutiny that ever. The realms of data completeness benchmarking will be superseded with comparative analysis of our efficiency and quality of services. Information Services will make available routine benchmarking opportunities to ensure we understand and control the view others will be able to have of us. Forecasting
As maturity increase, the Information Services department will need to adjust to provide a greater and more appropriate level of analysis. Automation of routine tasks will continue, allowing analysts in the department to develop more in-depth skills. The service provided will evolve from data processing and delivery to actual analysis of the rich data set available. This will then offer the Trust more advanced techniques for service management, including predictive analysis, multivariate analysis and data mining. Working with the combined datasets outlined previously will allow the Trust to incorporate evidence based analysis into key business decisions. Research
When C&I get to this point in their maturity model, advanced features of health informatics begin to become possibilities. The Trust warehouse will contain consolidated, accurate and relevant information from a range of sources. With true data warehouse design, data quality will be effectively and efficiently managed, and information will become key enabler within healthcare provision. Data within the Trust can be used in collaboration with our research partners, such as using free text analysis techniques across all data. The possibility of using routine outcomes data, contextualised with data from across the health economy can lead to prototypes in decision support tools.
9.1.5 Informatics Skills
As part of the Trust’s ICT Restructure, development of information management capacity was seen as an important theme. Over the next three years the Information department will continue to develop and enhance reporting dashboards and data standards whilst implementing EPR and Clinical Portal solutions. The pressures on the information team will grow with: Introduction of EPR. Creating new data streams into Data Warehouse and other reporting tools (Qlickview). Development of a Clinical Portal. The introduction of MHpBR. New commissioning arrangements. Requirements from the Care Quality commission. And the Performance Management agenda within the Trust and wider health economy. The responsibilities and breadth of activities undertaken by the Information Team has expanded considerably over the last two years. This is due to the ICT Department being a
104 of 132

C&I ICT Strategy 2013 / 16 31
projects driven department with multiple on-going concurrent projects aligned to various business programmes within the Trust. The work increasingly encompasses the configuration changes and impacts into the data Warehouse and associated reporting mechanisms such as the Qlickview dashboards. The sophistication of the Trust information systems and supporting applications (i.e. interface engine, docman, qlickview and portal etc.) has meant increasing knowledge and skills requirements within the Information Department. The department has one of the more advanced interoperability agendas currently within the sector and staff are increasing getting involved in the electronic sharing of information, agreeing data schemes and event triggers for advanced data sharing projects: Docman GP Information sharing. Clinical Repository Development and data sharing. LBC & LBI Social care data sharing. EPR interoperability – i.e. RiO Pathology reporting. To meet the above capacity challenges the ICT Department will increase the number of staff, grades and skill-sets within the Information Department.
105 of 132
C&I ICT Strategy 2013 / 16 32
10 Medical Records (MR) Scanning Project
10.1.1 The Current Situation
In 2012, the Trust commenced a Medical Records (MR) Scanning project aimed at centralising the storage and management of paper based medical records retained at over forty (40) sites. The original brief was to incrementally migrate paper based records from specific sites, scanned them, quality assure and shred the old paper record. However, in 2012 the Trust rapidly closed four (4) main sites which necessitated the realignment of the project to one; ensuring the safe collection and management of records from closing sites. The original plan aimed at around 5,000 records at any one time within the MR Department but this had to rapidly rescale due to the site closures. Currently we have: 25,000 Paper Medical Records maintained within the main MR Department with two (2)
temporary emergency over-flow storage areas. There are still more medical records to be migrated from all sites subject to space availability at St. Pancras Hospital.
1,000 Medical Records have been scanned. 90,000 individual pages scanned. The ICT Department is bringing in two (2) additional MR Staff to join the two (2) current staff members. This will enable the project to restart on its original brief to scan active patient records and shed the old paper based record. However, it should be noted that it will take between two (2) to three (3) years to scan all the medical records for active patients under treatment at the Trust.
10.1.2 Moving Forward
The Trust has set up a centralised office with paper records racking, large centralised scanner and large shredder, plus desk/table space.
All requests for medical records to be pulled from the off-site Iron Mountain store are processed through this office. The office scans the records, validates it for quality and accuracy and sends it into the clinical repository under specific easily searchable records structures. Staff requesting the record are then trained and shown how to view the scanned record.
All returned records go to a centralised records office for scanning, validating, processing and shredding instead to Iron Mountain.
All remaining paper medical records stored throughout the Trust will be collected in batches and processed by the MR Department and converted to electronic format, then shredded.
All scanned medical records are retained within an Electronic Document Management System (EDM). This EDM is electronically interfaced so that all scanned records are linked to the patient record within the C&I P.
This provides a unified view of all key RiO EPR Patient files plus their scanned paper medical records.
106 of 132

C&I ICT Strategy 2013 / 16 33
11 Flexible & Mobile Working
11.1.1 Supporting Flexible Staffing Models (Clinical/Operational)
One of the key aspirations of the strategy is to facilitate new flexible staffing models of care through better staff support, information provision and governance. Key objectives are: Break down silos and encourage information sharing across C&I and partner service
providers. Generate a more efficient, better informed, more collaborative workforce that makes the
best use of the expertise available within the Trust. Deliver more joined-up services, more effectively and at lower cost. Make staff more productive in their jobs and their teams more effective at delivering on
their goals. These objectives can be met by a varied number of approaches and examples are: Position Role based Access Controls (PBAC) within Clinical Systems access that allows different professionally qualified and non-qualified staff to undertake activities whilst maintaining risk governance controls. Enhanced eForm development within the Care Centric approach that allows process driven activities and risk controls to be embedded within set actions. If a key action (i.e. risk assessment) is not delivered by a specific date then an automatic process flow to a manager/ colleague to action is invoked. Clinical Governance and risk controls will be built into new system configurations allowing a more adaptable and flexible approach to skill and grade mix of staff within specific care settings and care pathways.
11.1.2 Back Office Enabling Technologies
During 2011/2012, the Trust has expanded its mobile devices from thirty-five (35) laptops to four hundred and fifty plus (450+) laptops, shortly to be increased by an additional one hundred (100) tablet devices. For every single desktop PC purchased the Trust purchases four (4) laptop/tablet devices. All mobile devices are encrypted and underpinned by fast, secure remote access solutions allowing access to systems from anywhere within the UK. These investments have allowed C&I to work beyond its traditional geographical boundaries and to take advantage of virtual working uninhibited by geographical location. This ICT Strategy will continue to support C&I’s growth potential and support working in new geographical locations and service areas. Increasingly staff require 3G mobile broadband within devices to facilitate access to the EPR and key files from wherever they are working within the U.K. The demand for this service will increase with the pending deployment of 4G faster broadband within our localities. The previous ICT Strategy 2010/13 provided the platform to redesign existing services: for example: providing remote workers with access to Emails, Corporate Files, Databases, Applications and Voice. Basically, everything staff have accessible to in the office and out of the office. The current strategy 2013/16 further builds upon this investment with the introduction of faster networks, faster broadband and greater access to a wider variety of information through clinical portals.
107 of 132

C&I ICT Strategy 2013 / 16 34
Fast Broadband Modems – C&I have sixteen (16) Tier four (4) sites which are smaller locations which typically between five and twenty (5 – 20) staffs work from. It has not been cost-effective to run fast 10mb Local Extension Service (LES) network lines to these locations and instead 8mb ADSL broadband circuits have been used. This has proved less than ideal with staff experiencing slow network performance resulting in slow system access. During early 2013, the Trust successfully piloted a new technology being delivered by Virgin Media which replaces the slower 8mb broadband with fast 50mb modem port lines. We will roll-out this new faster service to all tier four (4) sites during 2013. This is cost neutral- as the service it replaces cost the same. Mitel Phone Switches – During 2013/14 we will replace end-of-life Mitel Phone Switches and replace with two new switches covering all Trust locations. There will be a phone number change sub-project associated with this programme covering the St Pancras site. The new Mitel Switches integrated with the new 50mb Modems should support voice call routing over the current data networks to the Trusts smaller tier 4 sites. If successful this will enable the Trust to replace a small number of local Telecom Phone switches and put the site onto the integrated Trust wide phone service. Web and Audio Conferencing – During 2011/12 C&I successfully introduced video conferencing WeBex facilities into the Trust. Several teams are now using this service to meet and discuss patient care planning remotely. In addition, the service is widely used for RiO training and a wide variety of meetings and conferences. In 2013/14 this service will be expanded to include fifteen (15) Inpatient areas linking up to a Productive Ward project being undertaken across the Trust. This will allow ward round meetings to include other staff such as social workers based in non-Trust locations via video conferencing. We will undertake limited pilots to access the viability of using this type of service for remote consultations with clinicians and patients. BT is introducing a new virtual meeting room facility which supports clinical group work. The Trust was the runner up in the National 2012 IT Industry Awards for the use of this
technology for RiO EPR staff training.
11.1.3 Mobile Working
The Trust started introducing 3G mobile broadband enabled laptops/notebooks for mobile workers in 2010. By 2013 over 50% of all mobile devices used within the Trust have 3G services built-in allowing staff to access key services such as the RiO EPR from anywhere within the UK that has a 3G signal. From 2013 onwards, where applicable we will phase in faster 4G services as they become more widely available and cost-effective. The Smartphone - In general, Smart phone provide additional features including, email, scheduling, internet connectivity and the ability to load additional 3rd party applications. A growing use of Smart phones is to enable remote access to key files and to provide email access. The Trust has a dichotomy of need: 1. Reduce the burgeoning mobile phone costs and numbers of handsets. It is typically 30%
– 50% higher than in similar sized Trusts. 2. Provide more functional Smart phones to those that ideally require them for their roles
within the community.
108 of 132
C&I ICT Strategy 2013 / 16 35
During 2012 continuing into 2013 a programme was been put in place to drive down inappropriate mobile phone use and facilitate better mobile phone solutions to those staff that really require them for their roles and functions. This has resulted in a large increase in 3G mobile broadband access whilst keeping the overall telecommunications costs within budgetary constraints. Tablet Devices - Guidance from the Leading Edge Clinical group has demonstrated that clinical staff would prefer a smaller lighter tablet device in preference to a laptop computer. However, access to the RiO EPR requires back-end security and system access through Microsoft technologies as part of the National System Contracts. This is why iPads cannot be used for RiO EPR access. In April 2013 C&I successfully tested a new Windows Tablet device which allow access to RiO EPR and incorporated NHS Smartcard security access. From 2013 onwards we will purchase 80% tablets to 20% Laptops for mobile working. The former (tablets) being ideal for clinical patient facing activities, the laptops being better for more intensive note writing entry requirements.
11.1.4 Wi-Fi
The original Wi-Fi Project in 2010/13 aimed to put this service into the two main sites within the Trust at St. Pancras Hospital and Highgate Mental Health Centre (HMHC). These original two (2) sites have Wi-Fi coverage extended to cover all the clinical and office areas. The Trust has further expanded Wi-Fi to a further nine (9) health centre locations. The ICT Department will continue to work closely with the Estates and Facilities Department and every opportunity will be taken to incorporate Wi-Fi facilities in all new buildings, site relocations and site upgrades. This is an on-going work that is driving down the number of fixed network points and introducing more working flexibility for staff across the Trust. During 2013/16, the ICT Department will assess emerging Wi-Fi technologies that allow a wider coverage and reach (Wi-Fi Max). We will attempt to incorporate this with emerging 4G and Wi-Fi Hot Spots to provide faster and more flexible coverage for staff.
11.1.5 Updating Workstations within Clinical & Operational Areas
There is a constant need to annually refresh twenty percent (20%) of the installed base of one thousand and five hundred (1500) network devices located across the Trust. This annual update ensures reliable access to workstations which facilitate clinical care. It also ensures the cost of a five (5) year refresh cycle is spread annually, reducing the cost impact to the Trust. It should be noted that ward and clinical environments are harsh environments for workstations which show considerable wear and reliability issues after two (2) or three (3) years within such locations. With a new ratio of one (1) desktop to four (4) laptop/tablets (1:4) being purchased the overall count of fixed desktop devices will reduce in 2013/16. However, the desktop device count will still remain above one thousand (1,000); as not all system access is requires or needs mobile devices. It should also be noted that mobile devices require fifty percent more (50%+) support and maintenance than fixed desktop devices. This is in part to small integrated components and difficulty updating their operating systems in the same way as a fixed desktop device. In 2013, the ICT department is introducing improved network monitoring and remote access solutions to better support fixed and mobile devices. So whilst the overall count of mobile devices continues to increase this should maintain current support cost levels.
109 of 132
C&I ICT Strategy 2013 / 16 36
11.1.6 Agile Working and Human Resources
A new innovative approach is being introduced within the Trust.as part of its commitment to quality of life, the provision of excellent services, sustainability, equality and best value. The Trust is putting in place new ways of working which will make staff more efficient and able to provide better services for our service users. A Mobile & Flexible Working Programme is being introduced targeting groups of staff across a range of Services and supporting them to work in the work style most suited to the delivery of their services. Over the last three years the ICT Group has been overseeing the progress of a number of ICT infrastructure projects which have provided the technological environment required. This includes increased connectivity capacity, improved security, virtualisation of software applications and provision of a wider range of mobile hardware options including ‘Home Access'. There are also projects to provide the HR Policy framework we require, Health and Safety guidance, a new building security and a corporate booking system for hot desks, meeting rooms etc. A combined programme by ICT, Estates & Facilities and Human Resources will drive new ways of working forward and have a profound impact on how staff work on a day-to-day basis. The objective is to make ICT and Facilities and enabler rather than a barrier to innovations in practice and service delivery.
110 of 132

C&I ICT Strategy 2013 / 16 37
12 Tele-Health / Extranet
Successive governments have factored Long Term Condition (LTC) control models into their strategic thinking over a considerable number of years with limited service change. However, recently government rhetoric and policy has started to coalesce and facilitate real traction into driving service delivery change around LTC management. If the government strategy succeeds, there will be less traditional ‘case management’ service delivery episodes per care community cohort. C&I will have to adapt its service delivery model so they better support both traditional case management and enhanced self-care management solutions. The Extranet & Tele-Health Project is an enabler solution for the Trust to build a variety of future service delivery strategies and options upon. It is not just a finite IT project that completes at the end of two (2) years, but rather a strategic solution set to position the Trust for the future. The project needs to be recognised as a service delivery innovation enabler, an approach recognised by our commissioners. The commissioners seek the inclusion in such innovations in new service delivery approaches from the Trust. Much of this adaptive thinking and innovative solutions for these approaches is already being developed within the service side at C&I. At the heart of the approach is the recognition that the Trust needs to develop tools and techniques which enhance patient self-care support and management opportunities. Using ICT solutions in a flexible and adaptive way, aligned to service delivery innovation, is a structured and coherent way to meet these objectives.
12.1.1 Approach Supports Multi-disciplinary inter-agency teams (MDTs) Mental Health services within C&I have moved from an institutional setting to a patient and outcomes focused care pathways approach delivering both health and social care to service users in the community supported by high quality residential and inpatient facilities. Since 2010, the use of information technology within the care pathway has become more prevalent and important to the delivery of quality.
Figure 9: Timeline of care pathway approach
111 of 132
C&I ICT Strategy 2013 / 16 38
Expected benefits
Improved Service Experience for Service Users
New Cost Effective Ways to Deliver Services
Building up a C&I Service Delivery Web-Presence
More Agile, Innovative & Flexible Service Delivery
More Inclusive Stakeholder Engagement
Improved communication across the care community Enhanced Trust identity supporting Business Development The Virtual Trust Concept – geographical boundaries become obsolete Provides Trust with Competitor Advantage Possible cost-savings – enables processes and pathways to be shortened through
better information flow; and reducing duplication/interventions across the Trust because information is readily accessible.
12.1.2 Communications, C&I Web Site and Intranet
The current Trust external website is maintained by a third (3rd) party supplier which makes development both costly and slow. There is currently a backlog of improvements, such as restructuring content for easy navigation and the creation of areas for carers and service users. Maintaining the public facing web site is taking considerable time and efforts from a limited resource (Communications & ICT). Bringing the web site in-house under local Trust control will speed up the timeliness and relevance of the information contained within the website and will improve the presentation. The objectives are: Rebuild external C&I web site and bring under Trust control and management. Create Social Media contact points for service users. Refresh and update internal Trust Intranet. External Web-Site - the Trust Web Site is the ‘shop window’ to the Trust services and it is critical for a modern dynamic Trust to have a contemporary interesting and informative web site. The web site will require constant updating in order to keep information fresh and relevant to a wide variety of end-users. Social Media Pages - Social media has been a massive driving force behind large group communications, extended audience and community for organisations communications. Social media empowers people with the knowledge that their voice matters and can make a difference, social media technologies have changed forever the way people communicate and act online. Currently, Twitter and Facebook are favorite channels for social media communicators aligned with a vast number of dedicated blogs. The use of social media is gaining ever increasing importance for organisations communications in describing an organisations practices, ambitions, aspirations and corporate social responsibility. Intranet Refresh & Update - The current Trust Intranet has a huge wealth of information easily accessible to staff. However, a corporate intranet is a different tool than a smaller external web site. The depth of information and granularity of resources far exceeds what is normally found within an external web site. In addition the corporate intranet has far more robust security and access control than a web site. During the month of March 2013, we had 126, 321 page hits and 43, 014 site visits. The Intranet is a well-used Trust resource that is provides a wide source of information ranging
112 of 132

C&I ICT Strategy 2013 / 16 39
from Trust policies and procedures, clinical information, training resources, videos and links to key clinical sites such as the eBNF. However, like all such communication tools, the Intranet now requires a refresh to keep the site looking up-to-date and pertinent to its wide range of Trust users. Some of the expected benefits are: Enhanced Trust identity. Improved document management. Improved communication. Project communications. Cost-savings.
113 of 132

C&I ICT Strategy 2013 / 16 40
13 ICT Strategy Governance
The over-arching governance and monitoring of the ICT Strategy will be by the Estates and Finance Committee and the Executive management team with appropriate programme documentation including Update and Review reports. Beneath this committee sits the Information, Communication & Technology Group who manage all ICT programmes, projects and activities. The role of the ICT Group is to: provide ratification of the ICT strategies and subsequent implementations. review all issues related to ICT through the Trust. strategic oversight of all the ICT operations and projects. The Leading Edge Group provides input and advice from the Clinical and Operational Service to the ICT Group. This role of the leading Edge Group is to: Provide service led input into what sort of technologies should be introduced to meet
service requirements. Provide advice on specific service led priorities for technology investments and the
distribution of devices such as laptops and tablets. Review new technologies and provide advice regarding their appropriateness for
deployment within the Trust. Provide a feedback mechanism from the service about ICT Services and technologies.
ICT Sub-GroupLeading Edge Group
(Clinical/Operational Input)
Estates and Finance Commitee
FT Board
The scale of the ICT agenda and the critical dependence of the Trust’s strategy on delivery of information and IT solutions mean that the management and governance of ICT must be robust and fit for purpose. This section covers the Trust’s approach to: Procurement. Programme Management. Benefits Management. Programme Governance. ICT Training. Informatics Services.
114 of 132
C&I ICT Strategy 2013 / 16 41
Systems Development. Information Governance.
13.1.1 IT Procurement
IT Procurement needs to fit in with agreed contracts and utilise the catalogue on the system and the procurement web site to ensure the right models are purchased. The current Framework contracts with the London Procurement Partnership (LPP) ensures that PCs, Laptops etc. are imaged appropriately in the factory, ensure they are asset‐tagged and provides three‐year onsite maintenance. In addition optional IT services for delivery, installation and data transfer enable the service to be responsive to urgent needs. All IT hardware that will be attached to the Trust network must be approved by the IT department before being purchased. The department will normally have standard desktop computer, printer and software that will be approved for users. Any hardware installed without the knowledge of the IT department will not be supported and may be removed if it poses a risk to security of data or system operations. Any significant IT system purchase, which could be a departmental system or a significant piece of equipment attached to the network, will need to be approved by the Information Communication & Technology Group. The request will be assessed in terms of: degree of fit to local and national strategy and policies. ability to link to core systems particularly EPR. whether the core EPR can provide the information – where it can it should be mandated. Information Governance, security and robustness. completeness of data sets measured against local and national requirements where
relevant. reporting and data extraction support. viability of the supplier and ability to provide necessary support.
The Finance & Estates Committee is responsible for accepting bids and allocating ICT capital according to priority. The Trust’s Associate Director of ICT is responsible for managing allocated ICT capital with specific projects bidding for resource through the standard business planning process.
13.1.2 Project and Programme Management
All significant software system implementations will be managed according to Prince 2 project management methodology. Any large system implementation (a total cost of over £100,000) should have a Prince 2 qualified Project Manager appointed and have a properly constituted Project Board and Project Team appointed according the Prince 2 standards. A supplier Project Manager should be expected as well as supplier representation on the Project Board. The Chairperson of the Project Board will be a senior executive at Director level or immediately below, depending on the value of the project and the likely impact on the Trust.
115 of 132

C&I ICT Strategy 2013 / 16 42
13.1.3 Benefits Management
Any IT system, no matter how well implemented, will not deliver significant benefits unless the organisation makes the necessary changes to processes to deliver benefits. All significant ICT deployments will take a systematic approach to benefits management. This means that the benefits should be stated up front and should contain, as a minimum, the following: The benefit is to the Trust. Who is responsible to making the changes and hence delivering the benefit. if possible how the benefit is to be measured and baseline values. expected timescale for the benefit will accrue. These benefits will be held in a Benefits Register and the Project Board will ensure that the expected benefits are being realised. Some benefits will continue to be delivered long after the project is complete, so the ICT Group may monitor delivery of benefits on the Trust’s behalf.
13.1.4 ICT Training and Development
For the successful exploitation of ICT systems, considerable training will be required for all staff. Training requirements will be integral to each major system deployment project plan and intended users will not be given access to any significant Trust systems without appropriate prior training. ICT and systems training is undertaken by a dedicated Applications Support and training team who are responsible for: basic PC skills including use of keyboard, mouse and Windows. Microsoft office application skills including basic use of Email and the Internet. Corporate application training which will be predominantly focussed on EPR in all its
modules , re-enforcing messages around data quality. As well as scheduled courses there will be targeted training where a significant need is identified for a particular group of staff or for using a specific part of a system. Professional training for both Information and IT technical skills is essential to ensure that best use of the systems and resources is maintained.
13.1.5 ICT Strategy Risk Management
The risk management table is contained in Appendix A (ICT Strategy Risk Management) attached with this document.
116 of 132
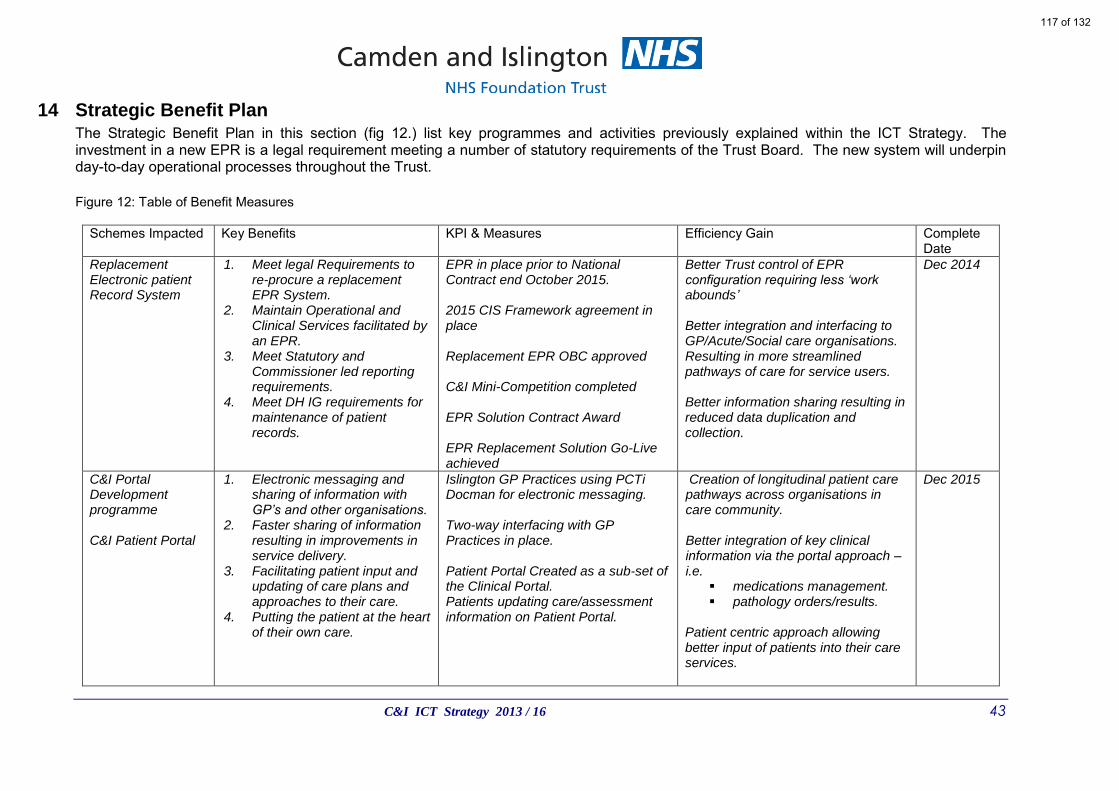
C&I ICT Strategy 2013 / 16 43
14 Strategic Benefit Plan The Strategic Benefit Plan in this section (fig 12.) list key programmes and activities previously explained within the ICT Strategy. The investment in a new EPR is a legal requirement meeting a number of statutory requirements of the Trust Board. The new system will underpin day-to-day operational processes throughout the Trust. Figure 12: Table of Benefit Measures
Schemes Impacted Key Benefits KPI & Measures Efficiency Gain Complete
Date Replacement Electronic patient Record System
1. Meet legal Requirements to re-procure a replacement EPR System.
2. Maintain Operational and Clinical Services facilitated by an EPR.
3. Meet Statutory and Commissioner led reporting requirements.
4. Meet DH IG requirements for maintenance of patient records.
EPR in place prior to National Contract end October 2015. 2015 CIS Framework agreement in place Replacement EPR OBC approved C&I Mini-Competition completed EPR Solution Contract Award EPR Replacement Solution Go-Live achieved
Better Trust control of EPR configuration requiring less ‘work abounds’ Better integration and interfacing to GP/Acute/Social care organisations. Resulting in more streamlined pathways of care for service users. Better information sharing resulting in reduced data duplication and collection.
Dec 2014
C&I Portal Development programme C&I Patient Portal
1. Electronic messaging and sharing of information with GP’s and other organisations.
2. Faster sharing of information resulting in improvements in service delivery.
3. Facilitating patient input and updating of care plans and approaches to their care.
4. Putting the patient at the heart of their own care.
Islington GP Practices using PCTi Docman for electronic messaging. Two-way interfacing with GP Practices in place. Patient Portal Created as a sub-set of the Clinical Portal. Patients updating care/assessment information on Patient Portal.
Creation of longitudinal patient care pathways across organisations in care community. Better integration of key clinical information via the portal approach – i.e.
medications management. pathology orders/results.
Patient centric approach allowing better input of patients into their care services.
Dec 2015
117 of 132
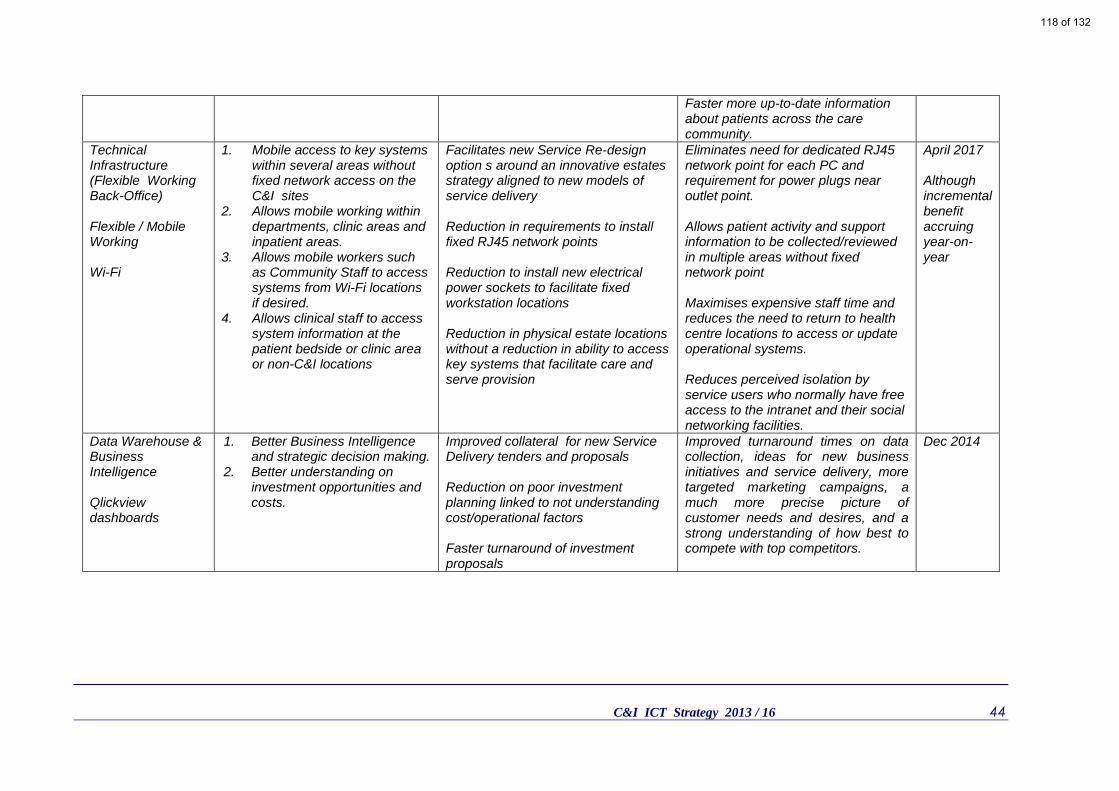
C&I ICT Strategy 2013 / 16 44
Faster more up-to-date information about patients across the care community.
Technical Infrastructure (Flexible Working Back-Office) Flexible / Mobile Working Wi-Fi
1. Mobile access to key systems within several areas without fixed network access on the C&I sites
2. Allows mobile working within departments, clinic areas and inpatient areas.
3. Allows mobile workers such as Community Staff to access systems from Wi-Fi locations if desired.
4. Allows clinical staff to access system information at the patient bedside or clinic area or non-C&I locations
Facilitates new Service Re-design option s around an innovative estates strategy aligned to new models of service delivery Reduction in requirements to install fixed RJ45 network points Reduction to install new electrical power sockets to facilitate fixed workstation locations Reduction in physical estate locations without a reduction in ability to access key systems that facilitate care and serve provision
Eliminates need for dedicated RJ45 network point for each PC and requirement for power plugs near outlet point. Allows patient activity and support information to be collected/reviewed in multiple areas without fixed network point Maximises expensive staff time and reduces the need to return to health centre locations to access or update operational systems. Reduces perceived isolation by service users who normally have free access to the intranet and their social networking facilities.
April 2017 Although incremental benefit accruing year-on-year
Data Warehouse & Business Intelligence Qlickview dashboards
1. Better Business Intelligence and strategic decision making.
2. Better understanding on investment opportunities and costs.
Improved collateral for new Service Delivery tenders and proposals Reduction on poor investment planning linked to not understanding cost/operational factors Faster turnaround of investment proposals
Improved turnaround times on data collection, ideas for new business initiatives and service delivery, more targeted marketing campaigns, a much more precise picture of customer needs and desires, and a strong understanding of how best to compete with top competitors.
Dec 2014
118 of 132

C&I ICT Strategy 2013 / 16 45
15 Summary
15.1.1 Delivering Benefits
Within the strategy, we have differentiated primary and secondary objectives. This is to ensure that the considerable risks to operational and clinical management processes are reduced whilst migrating onto a new EPR solution. These risks and their impacts should not be underestimated as recent reports from Trusts incorrectly deploying new EPR systems has resulted in millions of pounds of unplanned additional costs. The strategy seeks to eliminate the introduction of new technologies during the critical EPR deployment phases. The result will be that some secondary projects will be positioned immediately before EPR deployment or afterwards. There will be a requirement to manage staff expectations throughout the Trust as key strategic systems are given priority. The Trust has the option of paying more for some ICT resources to bring in some projects sooner. However, in some cases such as the EPR replacement this may not be possible due to limited supplier and project support resources.
Primary
1. Procure and Deploy an new Electronic Patient Record (EPR) Solution
2. Deploy the new EPR whilst minimising operational and clinical risks
Secondary
1. Minimise introducing new systems and technologies so that the primary objectives can me met.
2. Incrementally expand and scale up previous ICT investments that have delivered clear benefits.
3. Build upon solutions that enhance and facilitate flexible and agile working.
4. Deliver technical solutions that support expansion of services both within and outside existing geographical working locations.
119 of 132

120 of 132

Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 1 of 12
MINUTES OF THE QUALITY COMMITTEE MEETING HELD ON TUESDAY 2nd JULY 2013 at 2.30 p.m.
EXECUTIVE MEETING ROOM, 2nd FLOOR, EAST WING, ST PANCRAS HOSPITAL
PRESENT: Dr Sue Goss (Chair) Non-Executive Director Ms Sarah Charles
Ms Wendy Wallace Non-Executive Director Chief Executive
Dr Sylvia Tang Deputy Chief Executive & Medical Director Ms Claire Johnston Director of Nursing & People Mr Paul Calaminus Chief Operating Officer IN ATTENDANCE: Mr Richard Arthur Trust Chair Mr Colin Plant Director of Integrated Care Ms Alison Martin Head of Risk & Patient Safety Ms Acosia Nyanin Interim Head of Performance and Regulation Ms Karoline Lye Clinical Audit & Service Improvement Facilitator
(item 12 only) Mr Martin Zielinski Board Secretary (minutes)
INTRODUCTORY ITEMS Action By:
1.
Welcome, Apologies and Quoracy
The Chair welcomed those in attendance, especially Mr Arthur as this was his last meeting. Apologies had been received from Ms Roz Jones, Clinical Policy Development Manager. The meeting was quorate Mr Arthur commented that this was the worst set of Committee papers he had ever received. He complained about the errors on the pack's agenda, which inaccurately reflected the papers attached, and the lack of analysis contained in the actual papers presented. Dr Goss commented on the length of the papers. She said that what was needed in the papers was not simply the statistical detail, but judgements, analysis and commentary from clinicians and managers writing the papers as to the quality issues emerging that would enable NEDs to reach informed conclusions. It was helpful to know not only the trend of statistics but the management thinking and action that accompanied them. She added that there should be greater clarity about the purpose and focus for the discussion of each item. Mr Arthur concurred, stating that the presented papers should include more feedback and clearly establish relevant quality aims and any quality improvements achieved. Ms Charles supported this opinion, adding that the Committee needed to know outcomes, not just receive data. Dr Tang commented that Dr Goss, as Chair, was responsible for agreeing the agenda for each meeting. Dr Goss acknowledged that point and, being reliant on executive support, agreed that she would meet with Ms Johnston to discuss the agendas for future meetings. Mr Zielinski requested that Committee members notify him immediately if any problem with an agenda is noted, rather than waiting until the actual meeting takes place, as this would allow time to rectify any errors.
Ms Johnston / Dr Goss
121 of 132

Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 2 of 12
2.
Minutes of the Quality Committee previous meeting
The minutes of the meeting held on 9th April 2013 were received and agreed, with a small number of amendments, as a fair and accurate record. Dr Tang advised that the recorded need to meet locally and discuss ‘grab packs’ had been superseded as this was now a pan-London measure. The Committee AGREED the minutes of its meeting held on 9th April 2013, subject to requested amendments.
3. Matters Arising from the Previous Meeting
The schedule of matters arising from the meeting on 9th April 2013 was reviewed and the required actions were considered to have been completed, or were addressed elsewhere on the agenda, with the exception of: Aggregate Incidents, Complaints, Contacts, Compliments and Claims
Report
Ms Charles acknowledged the feedback provided but queried how informal complaints would be registered. Ms Martin advised that these would be included in reports from the next quarter.
Policy for Approval – Self Harm
It was noted that incorrect titles had been used in the matters arising when referring to Drayton Park and Emergency Department Liaison Teams.
Ms Martin
BUSINESS ITEMS
4. Aggregated Incident, Complaints and Contacts, Compliments and Claims Report – Quarter 4, 2012/13
Ms Martin presented this report advising that, due to the way the Committee’s dates fell, her team were midway through the preparation of the next quarter’s report. The report was split over 4 sections and she highlighted key points. The Committee’s attention was drawn to the table of ‘incidents per 1,000 bed days for 24 hours service’, where Ms Martin advised that she was reviewing reporting levels with the aim of improving data collection across all services and teams. It was noted that Montague and Malachite, both recovery and rehabilitation wards, had significantly different numbers of reported incidents. It was advised that these reflected a high number of AWOL incidents, which would need to be reviewed on a case by case basis, and that the two wards would be meeting to discuss their reporting variances and to address any issues that may be identified. Mr Calaminus added that these wards often dealt with service users transferred from other services (e.g. Pentonville) where they had problems with learned behaviours, on top of any mental health issues. He stressed the need for management to develop a management strategy that considered each service user on an individual basis. He went on to say that some related issues were beginning to be identified from reported incidents and aspects such as service access and staffing were being reviewed. He added that, in his experience, reporting levels were quite low which signified that the Trust was either offering the right services or under reporting incidents. Dr Goss queried if the Committee should be concerned about the overall number of incidents being reported. Ms Martin had no undue concern and advised that she expected numbers to increase as under reporting was a possible problem that was being looked into. Dr Goss asked if the aim was to identify all incidents and address these with relevant management. Mr
122 of 132

Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 3 of 12
Calaminus confirmed this to be the case, adding that the reasons behind incidents would also be examined with any learning used to make improvements. Ms Martin concurred, stating that the aim was to provide a true reflection of what was actually happening within services. Mr Arthur stated that the given information gave a much clearer perspective on the incident position, which was not clear from reading the report. Dr Goss agreed, requesting that the report gave more examples of actual incidents and detailed actions taken to address identified issues. Mr Arthur commented on the comparatively high number of incidents on the Rosewood unit, in relation to other treatment wards. Ms Wallace advised that the reported figure related to Q4, 2012/13 and that this unit no longer treated high dependency cases. Mr Calaminus added that the number of incidents on the unit had been adversely affected by one extremely challenging service user who generated a large proportion of the reported incidents. Ms Martin added that, from April 2013, wards had improved the recording of service user data, making it more evident where a number of incidents related to one service user. In relation to slips, trips and falls, Ms Charles commented that, whilst the numbers were not high, there had been no evident reduction in incidents. She asked what preventative action was being taken and suggested that this should be detailed in the report. Dr Goss added that more detail was required. (e.g. if these incidents mainly involved older service users then the outcome may be more serious.) Ms Wallace drew attention to the stated 14% decrease in the number of minor or moderate injuries in the last quarter. Dr Goss commented that she had noted claims in the press that acute services were withholding diabetes medication from patients and queried if this was an issue for this Trust. Dr Tang responded that this was not a material issue, with the majority of Trust service users having type 2 diabetes, which was mainly managed by diet. She added that where insulin was required to be used, this would be in line with NICE guidance. In relation to the table detailing the number of complaints and complements, Dr Goss stated that it would be good to know main themes. Ms Charles stated that Mr Tony Fisher (Service Users Alliance) had undertaken an exercise to encourage service user feedback. She asked whether this had evidently affected the number of issues reported. Mr Calaminus was unaware of any residual effect from this and provided brief details on the types of complaints that had been received. He highlighted that the Trust did not always agree with received complaints, providing examples where service users had not fully understood their need for medication or treatment. He advised that the Acute Care Forum was undertaking a review of the main reasons for complaints and how these could be addressed. It was confirmed to Ms Charles that both formal and informal complaints were recorded. Ms Martin stated that she had, as requested, reviewed the shift in the majority of complaints from acute to community services. She added that the ratio between formal and informal complaints had not changed. Ms Wallace commented that this was not an overall increase in the number of complaints, but a change in their source. Dr Tang added that this increase may reflect an overall increase in the number of service users seen due to service expansion and increased transfers from Community Mental Health Teams. Ms Martin advised that she was planning to undertake a specific review that would break down complaints data; ensure that lessons have been learnt; and appropriate action taken. She confirmed to Dr Goss that she expected the results from this review to available in 6 months. Dr Goss queried whether the restructuring of services had resulted in an increased number of complaints. Mr Calaminus advised that there had been no material increase, adding that feedback had been directly invited from GPs and only 3 complaints received over a number of months. Mr Arthur was
Ms Martin
Ms Martin
123 of 132
Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 4 of 12
reassured that this was the case. Ms Martin advised that the Trust’s annual Risk Management Report was due in September. Work was underway to gather the necessary data and the report would incorporate benchmarking for the first time. Ms Martin advised that the final report would be presented to the Audit & Risk Committee. Mr Arthur referred to the high number of incidents RAG rated as ‘red’ in the table under ‘likelihood / consequence of incidents’. These were obviously major concerns but the underlying causes were not clear. Ms Martin advised that any service user death was recorded at the highest risk score. Mr Calaminus confirmed to Mr Arthur that the 180 plus ‘red’ rated incidents were not all deaths. Ms Martin advised that, as part of the work to improve reporting levels, teams would be educated in scoring risks to improve the consistency in how different risks were rated. She was concerned that inconsistencies currently existed. It was noted that the pie chart detailing the severity of incidents reflected the position as at 22nd May 2013. Ms Martin advised that this data was updated daily and more up to date information would be presented in future. The Quality Committee NOTED quarter 4’s Aggregated Incident, Complaints and Contacts, Compliments and Claims Report Trust.
5. Clinical Quality Strategy 2013/14 (and 2015; 2016)
Dr Tang presented this strategy along with an attached action plan that was associated to, but not part of, the strategy. She highlighted that the appendices provided Divisional reporting and the clinical leadership structure for the Trust. Dr Tang invited questions from the Committee. Dr Goss stated that the objectives and timescales set out in the action plan were very informative in detailing what action was being taken. She particularly appreciated the thought and imagination that had gone into some of the new proposals, such as that for a ‘recovery college’. In relation to ‘Rehabilitation and Recovery’, Dr Goss sought to confirm her understanding that Service Users transferred between service teams. Dr Tang confirmed that this was the case, advising that the assessment of needs and handover arrangements were set out in a legal framework. Mr Calaminus added that CQINN targets required an evaluation of the extent to which care plans were personalised for each service user and to what degree they were involved in their own care. Ms Nyanin added that these measures were included in the patient experience feedback element of the Quality Account report. Ms Wallace highlighted the increased caseload being managed by the Assertive Outreach Teams. Dr Goss summarised that the presented documents were extremely useful and informative but queried how the action plans would be monitored going forward, given the proximity of some of the due dates. Mr Calaminus advised that a cross-divisional forum were consolidating models of care and would monitor progress, which would be reported into FTE. It was agreed that a quarterly report would be prepared feeding back progress to this Committee. Referring to the appended ‘outcomes framework’, Ms Charles queried how the change to outcome reporting had been reflected in the strategy. She was advised that Ms Nyanin was undertaking a piece of work to establish a meaningful outcomes based report that could be presented to the Board. Ms Johnston confirmed that this report would clearly define the purpose of different indicators and focus on improvements made. Dr Tang added that a piece of work, covering 6 MHTs, was underway to develop a value based scorecard
Mr Calaminus
124 of 132

Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 5 of 12
that could be used to facilitate comparative reporting. She added that this would use measures already taken although the format of the report would change. The Quality Committee NOTED the Clinical Quality Strategy 2013/14 (and 2015; 2016)
6. Quality Accounts 2013/14 Ms Nyanin presented this item. She summarised how actions agreed from the previous year’s Quality Accounts would be monitored. She highlighted that the July Performance Report would reflect Trust performance, in comparison to other bodies. Required actions would be monitored by divisional performance groups. She advised that work was underway to develop innovative ways of computing soft service user data and a quality assurance dashboard that reflected both hard and soft data. The Trust’s quality risk profile would be developed further and validated by service visits and mock inspections. It was expected that the Trust would have more detailed assurances on performance by the sign off of year end quality accounts 2013/14. Dr Goss stated that, in addition to reported successes, the Board should also see negative patient feedback and queried how this could be achieved. Ms Johnston responded that she would identify appropriate cases with management and arrange for details to be presented to the Board. Dr Goss queried whether this Committee could receive the same quality information that was presented to commissioners. Ms Nyanin advised that she would make a relevant request to the CQRG. She added that the CQRG’s work plan should be reviewed and considered when developing a work plan for this Committee. Dr Goss stated that hearing Ms Nyanin’s explanations behind the soft data presented in the papers provided a much clearer picture. She added that the details of service users’ views were much more effective feedback than pages of data. Ms Nyanin advised that, in line with her work plan, she was working to link more narrative to the presented heat maps. Ms Charles stated that it was important to clarify the scope of the new Service Users and Staff Experience Committee, which was being established, and how this would differ from the scope of this Committee. It was agreed that work should not be duplicated across both these Committees. Ms Charles stated that she would work with Dr Goss and Ms Johnston to clarify the roles of each. Ms Wallace queried whether the existing balanced scorecard would change. Ms Nyanin stated that the scorecards would remain but the questions would be amended to become more quality focused. Ms Wallace advised that the scorecards and local audit plans should reflect each Division. Ms Nyanin stated that this was largely the case already but acknowledged that further work was required. Ms Charles supported the need to take a fresh view on obtaining reliable outcome reporting. Ms Nyanin advised that the triangulation of different data was being developed to strengthen outcome reporting. Dr Goss, referring to the consultation on service user engagement in the Quality Accounts, asked if these had been taken to Healthwatch in June as stated. Ms Nyanin confirmed that this was the case. Dr Goss requested a paper detailing new means by which the Trust could engage with service users at its next meeting. Ms Johnston agreed and advised that a consultation process on this topic was underway, with progress regularly
Ms Johnston
Ms Nyanin
Ms Charles / Ms Johnston/
Dr Goss
Ms Nyanin
125 of 132

Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 6 of 12
monitored. The Quality Committee NOTED the Content of the monitoring arrangements and action plans for developing the 2013/14 Quality Accounts.
7. Serious Incidents Framework – March 2013
Ms Martin advised the Committee on this new guidance, which did not represent a fundamental change in process but did reflect the re-direction of responsibilities from PCTs to CCGs. She advised that relevant Trust policies were compliant with national guidance, although there may be a need to strengthen evident learning and Board oversight. The Quality Committee NOTED the Serious Incidents Framework.
8. Delivering a Single Operating Model for investigating serious patient safety incidents (mental health homicides) for the NHS Commissioning Board
Ms Martin provided a summary on the proposed development of a single operating model. A single standardised report would be introduced covering homicide and other investigations. Mr Calaminus queried if the paper set out how domestic homicides, which were different, would be integrated into reporting. Ms Martin advised that this was not covered. Ms Wallace stressed that this was only a proposal to establish a standard operating model and that full details would be unclear until the final version of the process was produced. The Quality Committee NOTED the update on the proposal to deliver a single operatiing model for investigating serious patient safety incidents.
9. Trust Response to the Francis Inquiry Recommendations
Ms Goss raised the fact that she had only received this paper ten minutes before this meeting commenced. Ms Johnston advised that the Trust Board would be required to report annually on how the Trust would take these recommendations forward. The paper had been tabled at this meeting to demonstrate how those responses relevant to the Trust would be developed into an action plan for reporting to the Board. Mr Arthur queried the need for yet another action plan to be presented to the Board and whether the required reporting could not be incorporated into existing reports. Ms Johnston advised that, due to the significance currently being placed on the Francis Inquiry, the item should be reported separately, at least in the short term. It was agreed that comments from the Committee members would be e-mailed to Ms Johnston. The Quality Committee members AGREED to review the Trust’s response to the Francis Inquiry Recommendations outside of the meeting and provide any necessary feedback to Ms Johnston.
Committee Members / Ms
Johnston
126 of 132

Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 7 of 12
10. Creating a Culture of Learning from Service Users’ Experiences
It was noted that time had already been allocated to discussing this issue with management and to identify planned actions. Dr Tang advised that relevant data had been subject to a high level of scrutiny by other Board level Committees; relevant groups; and at a divisional level. Recently produced data provided significantly more granular detail, e.g. wards could view infection control audit results and dashboard data relevant to their local level. This encouraged a sense of pride within well performing teams and encouraged others to improve. Dr Goss asked whether management were aware of any problem areas where improvements were required. Ms Johnston advised that the development of heat maps and triangulated data has provided much more detailed information. This would enhance identification of issues that may be of concern within individual teams and allow support to be directed to address specific problems. Ms Nyanin added that dedicated support teams were being put together to assist, and deal, with any identified clinical or governance issues. Ms Wallace added that Rapid Improvement Teams would also be established to respond to any break in reporting thresholds, as had previously happened at Stacey Street. It was noted that a 3 stage process would operate whereby: level 1 threshold breaches would require the provision of general support
and advice; level 2 threshold breaches would require a Rapid Improvement Team to be
sent in; and Level 3 threshold breaches would require formal management intervention. Ms Johnston assured the Committee that regular operational processes already monitored the quality of service delivery. Mr Calaminus assured Dr Goss that, the introduction of the outlined improvements was going well. He gave examples such as CDAT, where management had reviewed their data and created an action plan to address identified pressure points. He added that any issues identified from reviewed data were being addressed through meaningful discussions with managers. If such action failed to achieve results, a rapid improvement process would be instigated. Dr Goss acknowledged that managers, knowing what was behind the reported data, were best placed to tackle identified problems. Dr Tang advised that thought would be given to how triangulated data could be reported to this Committee. She added that the quality self-assessment tool by Monitor asks whether NEDs can name the 3 worst performing teams but these can be difficult to identify due to divergent views on overall balance of performance measures. Ms Charles stated that NEDs should be in a position where they can confidently state which services performed well, and which did not, but this was not the case. Dr Goss viewed that the 3 key parts to good performance to be: clinical leadership; operational management; and governance. Ms Wallace stated that senior management did note concerns during service visits but that a piece of work was required to verify whether material problems actually existed before a matter was reported to this Committee. Ms Johnston stated that she would report on the cultural barometer and the RIP process at the next meeting. Dr Goss requested results, rather than just details on the process, be reported. Ms Wallace advised that the process had to be agreed before data could be gathered and results obtained. Ms Charles commented on Dr Tang’s statement that clinical teams were becoming increasingly competitive as the level of comparative data improved and thought that this would prove beneficial in improving performance. Ms Wallace stated that clinical audit already created such an environment, with
Ms Johnston
127 of 132

Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 8 of 12
evident improvements in poorly performing teams post audit. Dr Goss stated that the true aim was to move towards a culture of having local pride in performance. Dr Tang responded that this had always been an aim of clinical governance and that these new processes supported that goal. The Quality Committee DISCUSSED the Creating a Culture of Learning from Service Users’ Experiences.
11. Mental Health Law Annual Report 2012/13
This item was deferred until the next agenda.
Mr Zielinski
12. Trust Clinical Audit Programme 2013/14
Ms Lye attended to present this paper that set out the Trust’s centrally supervised clinical audit programme for 2013/14. The programme incorporated the statutory requirements set by NICE and the CQC, and had been aligned to the Trust’s CQUIN targets. The document included detailed programmes for two Divisions, acute and SAMH. Programmes specific to other divisions were in development, along with those for pharmacy and psychology. In reference to the clinical audit programme set out in appendix 1, Ms Lye highlighted that quarterly balanced scorecards had been carried forward into 2013/14 as it has been noted how valuable teams had found data in this format. She also drew attention to the fact that the clinical audit team would directly manage 8 CQUIN targets during the year and advised that that marked improvements were already being noted in related reviews. The Committee noted that the required national suicide audit was being co-ordinated by Ms Martin. It was also noted that the NHSLA audit process remained under review although internal audit reviews would continue to keep the Trust prepared should these be re-introduced. It was also highlighted that the programme covered required reviews in relation to the POMH-UK (Prescribing Observatory in Mental Health) and the Mental Health Act. Mystery shopper audits would be reintroduced for 2013/14. A pilot of this process during 2011/12 had proved very successful and this would be expanded upon. The Quality Committee APPROVED the Trust’s Clinical Audit Programme for 2013/14.
13. Clinical Quality Review Group (CQRG): Arrangements for Quality Review by Clinical Commissioning Groups (CCGs) Ms Nyanin provided a briefing on the function of the CQRG, and its role in ensuring that CCGs have significant input into deciding quality improvement priorities and in setting quality indicator targets. She confirmed to Ms Charles that feedback from the Group would be reported to the Committee. The Quality Committee NOTED the provided briefing on the CQRG.
14. Draft Annual Safeguarding Report: April 2013 – March 2013
Ms Johnston advised that this draft report was presented for information and
128 of 132

Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 9 of 12
that the final version would be presented to the Board. Ms Wallace commended Ms Wiener, who had prepared a clear and well written report. Ms Charles noted the lack of any performance data from Islington and was advised that this borough’s feedback was outstanding but was expected to be received in the near future. The full report would be presented to a future Board meeting. The Quality Committee NOTED the Annual Safeguarding Report and ENDORSED the proposed priorities for 2013/14.
SUB-GROUPS MINUTES, REPORTS & ITEMS
15. Drugs & Therapeutics Group
No minutes were presented from this group.
16. Equality & Diversity Group
No minutes were presented from this group.
17. Infection Control Group
The Quality Committee RECEIVED the minutes from the Infection Control Group’s meeting on 4th February 2013.
18. Mental Health Law Group
No minutes were presented from this group.
19. Research & Development Group
The Quality Committee RECEIVED the minutes from the Research & Development Group’s meetings on 27th October 2012, 25th January and 26th April 2913.
20. Safeguarding Strategy Group
The Quality Committee RECEIVED the minutes from the Safeguarding Strategy Group meetings on 22nd February and 17th May 2013.
21. Clinical Quality Standards & Outcomes Group (CQSOG)
It was noted that this group has been disbanded and its duties will be covered by Divisional Quality Groups.
22. Performance Group
It was noted that this group now reports to FTE.
23. Physical Health & Nutrition Group
It was noted that this group now reports to the Nursing Executive.
24. Service User Experience & Involvement Group (SUEIG)
It was noted that this group will be replaced by a Service User & Staff Experience Committee.
129 of 132

Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 10 of 12
25. Stacey Street Sub-Group
Mr Arthur queried the current position at Stacey Street. Mr Calaminus advised that a useful set of reports had been discussed at the last group meeting. Ms Johnston added that corrective action was underway to address any outstanding issues and that the newly appointed management were finding their feet. Ms Nyanin added that two mock inspections had been carried out and that the latest, on 18th June, had shown marked improvements in the service. Mr Arthur further questioned whether staffing issues at the site had been addressed. Mr Calaminus responded that recruitment was progressing well, adding that plans were now in place to expand the services over two floors. It was noted that the last CQC visit was on 8th February 2013 where concerns had been noted in relation to feeding a patient. Mock inspections on 1st May and 18th June 2013 indicate these concerns have been addressed. Dr Goss asked if the site would now pass a CQC inspection and Ms Nyanin advised that she had no concerns in relation to issues previously noted by the CQC. Ms Wallace added that compliance would be required across all inspected criteria, not just those issues previously highlighted as a concern. Ms Nyanin advised that all areas of the service have been reviewed, with the focus being on the patient experience. Mr Arthur asked whether the CQC would return. Mr Calaminus advised that they would almost certainly return to Stacey Street, as well as attending at other Trust sites. The Quality Committee RECEIVED the minutes of the Stacey Street Sub-group meetings on 4th April, 22nd April, 13th May, 3rd June and 24th June 2013.
REGULAR COMMITTEE BUSINESS
26. Committee’s Terms of Reference The Quality Committee AGREED that its terms of reference was appropriate and should be forwarded to the Board for approval.
27. Consideration of Committee Work Plan and Reporting to the Board
28. Sub-group Terms of Reference for Approval
Drugs & Therapeutics Group
The Committee APPROVED the Drug & Therapeutics Group’s Terms of Reference.
AD HOC ITEMS
29. Annual Plan for Updating Clinical Policies
130 of 132
Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 11 of 12
The Quality Committee NOTED the schedule of policies expected for approval at future meetings.
30. Policies for Approval
CLINICAL POLICIES
Ms Wallace commended Ms Jones for providing an introductory table that clearly set out the changes made to each of the policies presented below: i. Food & Nutrition Policy;
ii. Seclusion Policy;
iii. Patient Leave Policy;
iv. Observation and Engagement Policy; and
v. Controlled Drugs Policy.
The Quality Committee APPROVED the above policies, updated in line with notified changes.
31. Clinical Audit Reviews
The papers included details on two clinical audit reviews: Physical Health and Substance Use Recording on RiO
Nutrition Recording on RiO
It was decided that these clinical audit reviews would not be considered at this meeting.
CLOSING ITEMS
32. Any Other Business
Mr Arthur stated that, despite the issues raised at the start of this meeting, he had enjoyed his time on this Committee and was pleased to see how the issue of quality had been moved forward within the Trust. Dr Goss thanked Mr Arthur for his input to the Committee and acknowledged his contribution towards improving quality throughout the Trust. Ms Johnston stated that she would sit down with Ms Nyanin and Mr Zielinski in advance of the next meeting to increase the level of planning for meeting agendas. Dr Tang added that feedback will be given to those preparing papers to consider how their content could be improved. Dr Goss asked all members to give thought to potential themes for discussion and future meetings and to e-mail her with ideas.
Ms Johnston
Committee Members
33. New Risks Identified during the Meeting, referred to/from other Committees
No new risks were identified during this meeting of referred to or from any other Committee.
34. Date of Next Meeting
Tuesday, 12th November 2013, 2.30pm The Executive Meeting Room, 2nd Floor, East Wing, St Pancras Hospital.
131 of 132

Quality Committee Minutes – 2nd
July 2013 Version: FINAL Page 12 of 12
5. Close
The Chair closed the meeting at 5.10pm
I certify that these are fair and accurate minutes of the stated meeting. ………………………………………… ……………………….
(Quality Committee Chair) (Date)
132 of 132





























