Embed Size (px)
Citation preview

MONTH
____
____
____
____
____
____
____
____
____
__YEA
R___
____
____
____
_
HOUR
S OF N
IGHTTI
ME SL
EEP
NUMB
ER OF
MOOD
CHAN
GES
SEVERE
HIGH M
ODERA
TE
HIGH M
ODERA
TE
MIXED
STATE
(✔
) IF YE
S
MOOD
(0–
10)
ANXIE
TY SYM
PTOMS
(✔
) IF YE
S
LOW M
ODERA
TE
LOW M
ODERA
TE
MILD
MILD
SEVERE
Esse
ntiall
y inc
apac
itated
or H
OS
PIT
ALI
ZED
GREA
T diffi
culty
with
goal-
orien
ted ac
tivity
SOME
diffic
ulty w
ith go
al-ori
ented
activ
ity
More
energ
ized &
prod
uctiv
e; us
ual ro
utine
not a
ffecte
d muc
h
Usua
l routi
ne no
t affe
cted m
uch
Func
tionin
g with
SOME
effor
t
Func
tionin
g with
GREA
T effo
rt
Esse
ntiall
y inc
apac
itated
or H
OS
PIT
ALI
ZED
-10 • •
• • • •
• • • •
• • • •
0 • •
• • • •
• • • •
• • • •
•+10
Most
depre
ssed
ever
Balan
ced
Most
manic
ever
USED
ALCOH
OL/DR
UGS
(✔) IF
YES
12
34
56
78
910
1112
1314
1516
1718
1920
2122
2324
2526
2728
2930
31
STABLE
TO
TA
L
NU
MB
ER
O
F
PI
LL
S
TA
KE
N
PE
R
DA
YME
DICATI
ON/SU
PPLEM
ENT N
AME
DAILY DOSE
# OF P
ILLS
PER DA
Y
LIFE E
VENTS
23
45
67
89
1011
1213
1415
1617
1819
2021
2223
2425
2627
2829
3031
1
OTHER
SYMPTO
MS
23
45
67
89
1011
1213
1415
1617
1819
2021
2223
2425
2627
2829
3031
1
IM
PA
CT
(
-1
0=
MO
ST
N
EG
AT
IV
E;
10
=M
OS
T
PO
SIT
IV
E)
IN
TE
RF
ER
EN
CE
W
IT
H
LIF
E
(0
=L
EA
ST
;
10
=M
OS
T)
M A N I A D E P R E S S I O N

Depression and Bipolar Support Alliance730 N. Franklin Street, Suite 501, Chicago, Illinois 60610-7224 USAPhone: (800) 826-3632 or (312) 642-0049 Fax: (312) 642-7243W
eb site: www.DBSAlliance.org
Symptoms of mania/hypomania• Increased energy• Agitated or irritable m
oods• Inflated self-esteem
or grandiose feelings• Decreased need for sleep• M
ore talkative than usual, or pressure to keep talking
• Flight of ideas or racing thoughts• Easily distracted• Excessive involvem
ent in pleasurableactivities (spending sprees, sexual activity,foolish investm
ents or business ventures)
Symptoms of depression•
Decreased energy•
Sad, empty feelings
•Loss of interest or pleasure in usualactivities
•Inability to concentrate
•Significant weight loss or gain
•Change in sleep patterns, inability tosleep, or increased periods of sleep
•Feelings of worthlessness or inappropriate guilt
•Inability to m
ake decisions•
Recurring thoughts of death or suicide
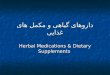
5.
Record
mix
ed s
tate
sIf
you
have
sym
ptom
s of m
ania
and
depr
essio
n at
the s
ame t
ime (
am
ixed
state)
put
a ch
eck m
ark (
✔) i
n th
e app
ropr
iate d
ay’s
spac
e.
6.
Rate
your
ove
rall m
ood
Rate
your
moo
d fo
r the
day
and
write
a nu
mbe
r bas
ed o
n th
e moo
d sc
alebe
low.
-10 . .
. . . .
. . . .
. . . .
. . . .
. . . .
. 0 . . . .
. . . .
. . . .
. . . .
. . . .
. . . +1
0Mo
st de
press
ed ev
erBa
lance
dMo
st ma
nic (a
ctiva
ted) e
ver
7.
Record
the n
um
ber
of
mood c
hanges
Enter
the
appr
oxim
ate n
umbe
r of t
imes
you
r moo
d ch
ange
d du
ring
the
day.
8.
Record
anxie
ty s
ympto
ms
Plac
e a ch
eck m
ark (
✔) b
y the
day
s you
hav
e sym
ptom
s of a
nxiet
y, pa
nic,
or ex
cess
ive w
orry.
9. R
ecord
oth
er
sym
pto
ms,
both
phys
ical
and m
enta
l
List
any p
hysic
al or
men
tal sy
mpt
oms y
ou h
ave t
hat i
nter
fere w
ith yo
ur li
fe,su
ch as
loss
of a
ppeti
te, p
ain, n
ause
a, pa
rano
ia or
thou
ghts
of su
icide
.Ra
te th
e effe
ct of
each
sym
ptom
on
the d
ay(s
) you
hav
e it.
0 . . . .
. . . .
. . . .
. . . .
. . . .
. . . .
. . . .
. . . .
. . . .
. . . .
. . . .
. . . .
. 10No
inter
feren
ce w
ith lif
eMo
st int
erfere
nce w
ith lif
e
10. R
ecord
sig
nif
icant
life
eve
nts
, both
posi
tive
and n
egati
ve
Reco
rd si
gnifi
cant
pos
itive
and
nega
tive e
vent
s eac
h da
y, su
ch as
anar
gum
ent w
ith a
love
d on
e, ill
ness
in th
e fam
ily, a
pro
mot
ion
at wo
rk o
ran
ythin
g els
e tha
t affe
cts yo
u. R
ate th
e im
pact
of ea
ch ev
ent o
n th
e day
(s)
the e
vent
affec
ts yo
u.
-10 . .
. . . .
. . . .
. . . .
. . . .
. . . .
. 0 . . . .
. . . .
. . . .
. . . .
. . . .
. . . +
10Mo
st ne
gativ
e imp
act
No im
pact
Most
posit
ive im
pact
Pers
onal
Cale
ndar
A m
onth
ly di
ary
We’
ve b
een
th
ere.
We
can
hel
p.
The Depression and Bipolar Support Alliance (DBSA)is the leading patient-directed national organization focusing on the m
ost prevalent mental illnesses. The
organization fosters an environment of understanding about the im
pact andm
anagement of these life-threatening illnesses by providing up-to-date, scientifically-
based tools and information written in language the general public can understand.
DBSA supports research to promote m
ore timely diagnosis, develop m
ore effectiveand tolerable treatm
ents and discover a cure. The organization works to ensure thatpeople living with m
ood disorders are treated equitably.Assisted by a Scientific Advisory Board com
prised of the leading researchers andclinicians in the field of m
ood disorders, DBSA has more than 1,000 peer-run
support groups across the country. Over four million people request and receive
information and assistance each year. DBSA's m
ission is to improve the lives of
people living with mood disorders.
We’ve b
een th
ere.W
e can h
elp.
Using
this
calen
dar t
o trac
k you
r moo
dTh
is ca
lenda
r help
s yo
u m
onito
r you
r moo
d on
a d
aily
basis
. It c
an h
elpyo
u an
d yo
ur h
ealth
car
e pr
ofes
siona
l rev
iew y
our s
ympt
oms
and
treatm
ent.
At th
e en
d of
eac
h da
y, tak
e a
few m
omen
ts to
thin
k ab
out y
our d
ay, w
hat
you
expe
rienc
ed, h
ow y
ou fe
lt, h
ow y
ou a
cted,
etc.
The
n sim
ply
follo
w th
ese
steps
for r
ecor
ding
the
info
rmati
on.
1.
Me
dic
ati
on
s/H
erb
al
sup
ple
me
nts
List
all th
e m
edica
tions
and
sup
plem
ents
you
take
in th
e sp
aces
prov
ided
, inc
ludi
ng th
e da
ily d
osag
es a
nd n
umbe
r of p
ills
that
shou
ldbe
take
n ea
ch d
ay. A
t the
end
of e
ach
day,
write
the
exac
t num
ber o
ftab
lets
or c
apsu
les o
f eac
h m
edica
tion
that
you
actu
ally
took
in th
eap
prop
riate
day’s
spa
ce.
2.
Alc
ohol or
dru
g u
se
Put a
che
ck m
ark
in th
e ap
prop
riate
spac
e if
you
dran
k or
use
d dr
ugs.
3.
Hours
of
sleep
Estim
ate th
e nu
mbe
r of h
ours
of s
leep
you
had
the
prev
ious
nig
ht.
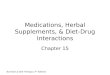
4.
Rate
the s
eve
rity
of
your
mood e
pis
odes
Indi
cate
how
your
moo
d ha
s aff
ected
you
r abi
lity
to fu
nctio
n at
hom
e, wo
rk, o
r sch
ool b
y pu
tting
an
✘in
the
appr
opria
te sp
ace.
Use t
he fo
llowi
ng sc
ale as
refer
ence
:M
AN
IASe
vere
Fami
ly an
d frie
nds w
ant m
e in t
he ho
spita
lHi
gh m
oder
ateMu
ch fe
edba
ck th
at be
havio
r is st
range
or bi
zarre
Low
mod
erate
Some
feed
back
that
beha
vior is
diffic
ult or
odd
Mild
Very
energ
etic;
functi
oning
may
be en
hanc
ed or
sligh
tly di
sorga
nized
STA
BLE
MO
OD
DEP
RES
SIO
NM
ildLo
w mo
od; e
ssen
tially
no im
pairm
ent in
usua
l func
tionin
gLo
w m
oder
ateSo
me ex
tra ef
fort n
eede
d in u
sual
roles
High
mod
erate
Much
extra
effor
t nee
ded;
marke
d diffi
culty
in us
ual ro
utine
sSe
vere
Large
ly un
able
to fun
ction
beca
use o
f dep
ressio
n