Embed Size (px)
Citation preview

Calculation of Premium Dynamics Based on
Epidemiological Models for Dengue Infection and
Reinfection
Helena Margaretha1,*, Arnold Reynaldi2, Reinhard Pinontoan3, Lucy Jap3, DinaStefani1 and Felicia Sofian1
1Department of Mathematics, Faculty of Science and Technology, UniversitasPelita Harapan, Tangerang, Indonesia
2The Kirby Institute, University of New South Wales, Australia3Department of Biology, Faculty of Science and Technology, Universitas Pelita
Harapan, Tangerang, Indonesia*corresponding author, email: [email protected]
November 1th 2018

Contents
1 Introduction 11.1 Facts on Dengue Desease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11.2 Infectious Desease and Insurance . . . . . . . . . . . . . . . . . . . . . . . . . . . 31.3 Research Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2 Existing Data 4
3 Epidemiological Models for Dengue Primary and Secondary Infection 113.1 Models . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113.2 Data Reconstruction Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
4 Micro-Insurance Pricing for Primary and Secondary Dengue Based on Epi-demiological Model 154.1 General Features and Assumptions . . . . . . . . . . . . . . . . . . . . . . . . . . 154.2 Product Description and Premium Calculation Method . . . . . . . . . . . . . . 17
4.2.1 Basic Insurance (NU ND HI) . . . . . . . . . . . . . . . . . . . . . . . . . 184.2.2 Underwriting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184.2.3 Death Benefit (NU D HI) . . . . . . . . . . . . . . . . . . . . . . . . . . . 204.2.4 Hospital Reimbursement . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
4.3 Forecasting Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 224.3.1 Exponential Triple Smoothing . . . . . . . . . . . . . . . . . . . . . . . . . 234.3.2 Exponential Distribution Fitting (R2) . . . . . . . . . . . . . . . . . . . . 264.3.3 Other Methods (I1 I2) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
4.4 Sample Calculation Result . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
5 Conclusions 355.1 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 355.2 Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
A Financial Report 39
1

Abstract
Dengue fever is one of the most common infectious disease in Indonesia. In the map of globaldengue risk, published by the World Health Organization in 2016, Indonesia is shown as red,which means high risk for dengue. WHO also reported that in 1990 - 2015 the number of denguecases increases both at a national level and worldwide. The severity of dengue fever varies frommild to deadly symptoms. Primary dengue infection only gives a partial immunity to thesurviving person. If he/she is re-infected for the second time (secondary infection), the severityof the illness will be higher. The increase of dengue cases as reported by WHO, implies thatthere are more people who are subjected to secondary infection, which is more severe and costly.The Indonesian Public Health Insurance (BPJS) covers cost for treatment and hospitalizationin the cases of dengue. Therefore it is important to analyze the economic cost of dengue to theIndonesian public insurance, to design a strategy for sustainability of the insurance plan. Toachieve the goal, first we want to formulate a multiple state model that describes the infection,re-infection and survival probability of dengue in Indonesia. The model must be able to capturethe increase of severity of illness in the case of re-infection. We need to find data or builda theoretical model for the re-infection case. The data or model will be used to calculate theparameters of the transition between each states. After getting an epidemiological model that fitswith the data, we proceed with calculating the premium dynamics of dengue insurance. We takea 1-year term insurance, and simulate the yearly premium for dengue insurance for year 1990-2015. From this projection, we predict the premiums for year 2016-2025. The implementationof epidemiological models in actuarial models is a promising approach to be studied further.This approach helps us in simulating the insurance costs for infectious deseases.

Chapter 1
Introduction
1.1 Facts on Dengue Desease
As an archipelago that is located at the equator, Indonesia enjoys the tropical climate. Theabundance of warmth from the sunlight, moisture, and rainfall give benefits as well as threatsto the people. Infectious diseases caused by mosquitoes are some of the threats. Dengue feveris the most common one. In the map of global dengue risk (Figure 1.1), published by the WorldHealth Organization (WHO) in 2016, Indonesia is shown as red, which means high risk fordengue. The global warming and climate change increase the population and the spreading ofmosquitoes. This may cause the spreading of dengue to regions that were dengue-free before[17].
Figure 1.1: Average number of dengue cases reported to WHO, 2010-2016 (source:http://www.who.int/denguecontrol/epidemiology/en/)
1

Figure 1.2: The percentage of circulating DENV serotypes from the observation of dengue casesin Purwokerto in 2015 (source: [13])
The existence of four strains of dengue viruses (DENV-1 to 4) adds to the complexity ofdengue infections. It has been studied that the mortality rate is higher in the case of re-infection, if the re-infection is caused by a strain of virus that is different than the one before[19]. The re-infection case is known as the secondary infection. All four strains of dengue virusoccur in Indonesia. An example is shown in Figure 1.2, which is taken from [13]. It shows thepercentage of DENV-1 to 4 that occur in a sample infected population from Purwokerto, a townin Cental Java.
People from all ages and races can suffer from dengue fever. Dengue fever causes economicallosses to the patient, his/her family and his/her workplace [6]. In the case of outbreak, thecountry may suffer a huge economical loss [7] [3]. There are direct and indirect economic costsof dengue. Indirect costs come from the loss of productivity or school days [22] and the financialburden to the family and the workplace when death occurs. Costs for health cares and/orinsurance claims are direct losses to the insurance companies and the government [7].
The significant increase of reported dengue cases implies to the increase of the economicburden to the insurance companies (public or private). Also, people who has been infected bythe primary infection are subject to the secondary infection, which is more severe and morecostly. We fear that in the future, cases of secondary dengue infection will also increase dueto the increase of dengue cases incidence rate. The Indonesian public insurance (BPJS) givesfull coverage to dengue cases. This fact must give a positive outcome to the effort of reducingmorbidity and mortality, which in the long run will decrease the probability of death because ofthe early detection of dengue fever and the improvement of overall health of the people. However,due to the dynamical interaction between hosts and vectors that is amplified by the climatologyfactors, a hyperendemic dengue outbreak might still happen especially in the rural areas wherepeople live very close to each other. It was reported by Suwandono et.al. that periodic outbreaks
2

of dengue have emerged in Indonesia since 1968, with the severity of resulting disease increasingin subsequent years [24]. They did a research from the 2004 dengue outbreak that erupted acrossIndonesia, with over 50000 cases and 603 deaths reported. When clinically assessed, 100 (55.6%)were classified as having dengue fever (DF), 17.2% as DF with haemorrhagic manifestations and27.2% as dengue haemorrhagic fever (DHF). Laboratory testing shows that 82.5% of those withDHF from which laboratory evidence was available suffered from a secondary dengue infection.All four dengue viruses were identified, with DENV-3 was discovered to be the most predominantserotype, followed by DENV-4, DENV-2 and DENV-1. Suwandono et. al. concluded that the2004 outbreak of dengue in Jakarta, Indonesia, was characterised by the circulation of multiplevirus serotypes and resulted in a relatively high percentage of a representative population ofhospitalised patients developing DHF.
1.2 Infectious Desease and Insurance
Threats from infectious deseases have got notices from the Society of Actuary (SoA) and Instituteand Faculty of Actuaries (IFoA). The UK actuarial profession discuss various aspects of themodelling, nature and mitigation of pandemic risk [10]. The US actuarial profession discussedlessons learned from the Ebola outbreak in 2014 and gave analysis on the impact to multipleinsurance industries [5]. Although dengue fever was not mentioned in both articles, the articleswere a sign of the raise of awareness in the actuarial professional society on risk exposuresfrom infectious deseases. The SoA’s article [5] mentioned two different methods for estimatingpandemic risk: the deterministic method and the stochastics method. In the deterministicmethod, stress-testing methodologies are often employed. In many cases (such as in the case ofinfluenza) the deterministic methods are useful. But if there is a great degree of uncertainty inthe outbreak, we may consider the stochastic methods. Some models that can be applied are:(1) time series models; (2) epidemiologic models; (3) catatrosphe models.
1.3 Research Methodology
This research consists of two parts. The first part deals with predicting the actual primaryand secondary infection from the total infection data. The prediction is done by searching theepidemiological model that gives the best fitting to the existing data (the dengue incidence datain Indonesia). The predicted values are the transition parameter between each state and therelevant initial conditions. Bayesian Monte Carlo method is implemented to get the posteriordistrbution of the parameters and the initial conditions.
Computational results from the first part is validated by doing an extensive review on clinicalfindings on dengue cases in Indonesia. We collect and review articles on this subject. We hirea team of life scientists to do the review, to derive the connection between theoretical andempirical studies on the complexity of dengue infections.
The second part of the research deals with pricing the insurance products and projecting thepremium dynamics for 10 years ahead. In this part we use the data that we get from the firstpart. We derive some insurance models that include the loss ratio, time series of the medicalinflation, and the insurance awareness factor. We calculate the dynamics of the insuranceproducts and do projections for 10 years ahead.
3

Chapter 2
Existing Data
The World Health Organization collects data on dengue cases reported by various countriesincluding Indonesia (http://www.who.int/denguecontrol/). The data is available from year1990 up to the most recent year. A longer historical data on dengue cases is reported by theIndonesian Ministry of Health in a bi-annual report on dengue [1] [2]. Figure 2.1 is takenfrom the 2016 report and shows a significant increase on the dengue incidence rate per 100000population in Indonesia (1968-2015). The total death is shown in Figure 2.2. From that figurewe observe that the death from dengue in considerably stable from 1990 until 2015. Despite thefact that the incidence rate of the illness increases, the case fatality rate per 100000 populationis stable. This is shown in Figure 2.3.
Figure 2.1: Data of Dengue Fever Incidence Rate 1968-2015 [2]. The recorded data does notdifferentiate primary and secondary infections.
The total population data is obtained from the World Bank. The data is shown in Figure2.4. The trend is linearly increasing. We can conclude that the total population growth rate isconstant over the past 60 years. We construct epidemiological models with main feature thatthe total population is not constant, which is realistic. The net growth rate was estimated
4

Figure 2.2: Total death from dengue fever in Indonesia (1968-2015). Source: [2]
directly using the observed total population (data from Worldbank, using log-linear regression).The crude death rate was around 7 per 1000 people per year (data from Worldbank, see Figure2.5). The net growth rate and the crude death rate were calculated using data from year 2000-2011. During and after this period, the population growth and crude death rate are stable andconstant.
Notice that the available data on dengue cases does not differentiate primary and secondarydengue infection. For an insurance model, we need at least yearly data on primary and secondaryinfection. In Table 2.1, 2.2, and 2.3 we report the summary on clinical studies that are relevantto our research [25], [15], [20], [13], [4], [16]. We see that the available clinical studies were doneat specific places at specific time intervals. We could not find a comprehensive clinical studythat represents cases on primary and secondary infection for the whole Indonesia. In the nextchapters we will discuss a computational approach to reassemble the existing data in such a waythat we get information on the primary and secondary infections.
5

Tab
le2.
1:C
lin
ical
stu
dy
data
for
DE
NV
-1an
dD
EN
V-2
.Sou
rce:
[25],
[15],
[20],
[13],
[4],
[16].
No
Year
of
Ob
serv
ati
on
Locati
on
Pop
ula
tion
DE
NV
-1D
EN
V-2
Tota
lP
rim
ary
Secon
dary
Tota
lP
rim
ary
Secon
dary
1F
ebru
ary
-A
ugu
st20
12S
ura
bay
a79
73%
33.3
0%
66.7
0%
8%
16.7
0%
83.3
0%
220
09-
2015
Bal
i154
28%
18.6
0%
81.4
0%
17%
11.5
0%
88.5
0%
3M
ay20
07-
Au
gust
2010
Mak
asar
126
41%
97.1
4%
2.8
6%
31%
88.4
6%
11.5
4%
420
15P
urw
oker
to47
23.4
0%
36.3
6%
63.6
4%
10.6
4%
60.0
0%
40.0
0%
5D
ecem
ber
2011
-Ju
ly20
12S
emar
ang
31
35.5
0%
18.1
8%
81.8
2%
12.9
0%
25.0
0%
75.0
0%
620
11-2
012
Su
kab
um
i25
20%
n/a
n/a
64%
n/a
n/a
6

Tab
le2.
2:C
lin
ical
stu
dy
data
for
DE
NV
-3an
dD
EN
V-4
.Sou
rce:
[25],
[15],
[20],
[13],
[4],
[16].
No
Year
of
Ob
serv
ati
on
Locati
on
Pop
ula
tion
DE
NV
-3D
EN
V-4
Tota
lP
rim
ary
Secon
dary
Tota
lP
rim
ary
Secon
dary
1F
ebru
ary
-A
ugu
st20
12S
ura
bay
a79
6%
0%
100%
8%
0%
100%
220
09-
2015
Bal
i154
48%
17.6
0%
82.4
0%
4%
16.7
0%
83.3
0%
3M
ay20
07-
Au
gust
2010
Mak
asar
126
20%
76.9
2%
23.0
8%
7%
83.3
3%
16.6
7%
420
15P
urw
oker
to47
55.3
2%
46.1
5%
53.8
5%
10.6
4%
20.0
0%
80.0
0%
5D
ecem
ber
2011
-Ju
ly20
12S
emar
ang
31
12.9
0%
25.0
0%
75.0
0%
9.7
0%
0.0
0%
100.0
0%
620
11-2
012
Su
kab
um
i25
0n
/a
n/a
16.0
0%
n/a
n/a
7

Tab
le2.
3:C
lin
ical
stu
dy
data
for
mix
edD
EN
Vze
roty
pes
.S
ou
rce:
[25],
[15],
[20],
[13],
[4],
[16].
No
Year
of
Ob
serv
ati
on
Locati
on
Pop
ula
tion
Mix
ed
DE
NV
DE
NV
DE
NV
Tota
lP
rim
ary
Secon
dary
1&
21&
31%
4M
ix
1F
ebru
ary
-A
ugu
st20
12S
ura
bay
a79
1%
3%
1%
5%
50%
50%
220
09-
2015
Bal
i154
0%
0%
-3%
0%
100%
3M
ay20
07-
Au
gust
2010
Mak
asar
126
0%
0%
-1%
n/a
n/a
420
15P
urw
oker
to47
0%
0%
0%
0%
n/a
n/a
5D
ecem
ber
2011
-Ju
ly20
12S
emar
an
g31
0%
0%
0%
29.0
3%
22.2
2%
77.7
8%
620
11-2
012
Su
kab
um
i25
0%
0%
0%
0%
n/a
n/a
8

Figure 2.3: The case fatality rate per 100000 for year 1968-2015. Source: [2]
Figure 2.4: The total Indonesian population according to World Bank (1968-2016). Source:https://data.worldbank.org/
9

Figure 2.5: Death rate, crude (per 1000 people). Source: https://data.worldbank.org/
10

Chapter 3
Epidemiological Models forDengue Primary and SecondaryInfection
3.1 Models
We approach the problem by formulating two mathematical/mechanistic state space models. Wemodel the complexity of dengue primary and secondary infection using compartment models.Flows between each compartment are defined from the specification of dengue illness. We triedthree compartment models:
1. A model that does not differentiate dengue primary and secondary infection (SIR). Here’S’, ’I’, and ’R’ refer to ’susceptible’, ’infected’, and ’recovered’, respectively.
2. A model that differentiate dengue primary and secondary infection (SIRSEIR) but doesnot differentiate the virus zerotypes that causes the primary infection. Here ’E’ refersto ’expose’, so in this model we take into account a certain period of immunity after theprimary infection.
3. A model that both differentiate dengue primary and secondary infection and also the viruszerotypes that causes the primary infection (Branched SIR-SEIR model)).
All models take death and population growth into account. Diagrams of the three modelsare given in Figure 3.1, 3.2, and 3.3 .
3.2 Data Reconstruction Method
Each epidemiological model is solved using a numerical method. The transition parameters arepredictd using Bayesian Markov Chain Monte Carlo method. The SIR model does not give agood prediction, because people do not get full immunity against all dengue zerotypes. TheSIRSEIR model and the branched SIRSEIR model are more promising. The prediction is givenin the Figure 3.4. We see that the model fits the data nicely within the 95% confidence interval.The model that we use allows us to get the predicted values for yearly number of the primaryand secondary infections.
11

Figure 3.1: The SIR model that does not differentiate primary and secondary infection
Figure 3.2: The SIRSEIR model. The primary and secondary infections are compartments ofthe model
12

Figure 3.3: The branched SIRSEIR model. This model assumes that the DENV zerotypes canbe clustered into two dominant groups.
Details on the computational methods and research outcomes will be presented in the paperthat is currently being prepared. In that paper we will discuss the analysis related to thecomplexity of dengue disease based on retrospective clinical studies in Indonesia. This discussionwill be a supporting evidence to our simulation results. The paper is planned to be publishedin a peer-reviewed journal.
13

Figure 3.4: Model fitting with the Indonesian dengue data year 1968-2015
14

Chapter 4
Micro-Insurance Pricing forPrimary and Secondary DengueBased on Epidemiological Model
Using the numbers from the model above, we will make a sample micro-insurance for primaryand secondary dengue. This product is yearly renewable with different premiums adjusted tocurrent and forecast conditions.
There are three conditions we are going to explore, as follows.
1. UnderwritingUnderwriting is always a vital component in every insurance product. Here we will explorethe effect of underwriting and the different premiums it produces. Non-underwrittenpremium is notated by ”NU”. Underwritten premium is notated by ”U”, divided into”U1” for people who have not contracted dengue (primary dengue protection), and ”U2”for people who have contracted dengue at least once (secondary dengue protection).
2. Death BenefitAnother common feature in every health insurance is death benefit. The beneficiary willhave the right to claim this if the insured dies of dengue (either primary or secondary).Product without death benefit is notated by ”ND” and with death benefit by ”D”.
3. Hospital Income and Hospital ReimbursementThere are two types of payment in health insurances. One is hospital income, which isa fixed payment paid for every claim. This will be noted by ”HI”. Another is HospitalReimbursement, in which the insurer pays the exact hospital billing for each claim, notatedby ”HR”.
4.1 General Features and Assumptions
In this section, we will discuss the features and assumptions used in all products.
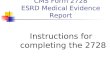
1. Data CharacteristicsIn this study, the data obtained is from 1968 to 2015. But in the premium calculation wewill not use data prior of year 2000. The reason is obvious when we see Figure 4.1, whichis graph showing the portion of primary (I1) and secondary (I2) infection divided by total
15

Figure 4.1: Primary (Blue) and Secondary (Red) Portion of Dengue Infection.
dengue infection (I) in percentage, as modelled above. Due to lack of records in earlierdecades, the infection trend is not visible until 2000s. Therefore, to ensure accuracy in wepricing and forecasting, we will use data which are still related to the current conditions.In this study, it starts from year 2000.
2. Loss Ratio (l%)Claims and benefit reserve is commonly the largest portion of premium income. Togetherwith other expenses, this portion of premium divided by premium income is called ”lossratio”. In this model, we will use net benefit reserve without other expenses nor additionalreserves.
For example, if the loss ratio is 70%, then for every $1000 premium income, 70%*$1000=$700is used for benefit. The other 30% may be used for cushion or other purposes.
Therefore, the loss ratio equation is:
Loss Ratio =Expected Benefit Payment
Premium Income(4.1)
Another form of the equation may be used to calculate premiums:
Premium Income =Expected Benefit Payment
Loss Ratio(4.2)
3. Inflation (i%)Inflation is the rate at which the general level of prices for goods and services is risingand, consequently, the purchasing power of currency is falling. [23] Specifically, medicalinflation is the rate at which medical costs rise. Unfortunately, studies on medical inflationin Indonesia has only been done since 2014. Therefore for years before 2014, we will usegeneral inflation instead of medical inflation. Inflation rate used for calculation is in Table4.1.
16

Table 4.1: General and Medical Inflation in Indonesia
Year General Inflation Medical Inflation2017 3.61% 15.00%2016 3.02% 15.00%2015 3.35% 9.30%2014 8.36% 9.50%2013 7.72%2012 4.30%2011 3.79%2010 6.96%2009 2.78%2008 10.23%2007 6.59%2006 6.60%2005 17.07%2004 6.47%2003 5.17%2002 9.92%2001 12.55%2000 9.35%
Source: inflation.eu [14] Multiple Sources[26][8]
Generally, inflation rate is calculated as follows:[23]
it =CPI(t+ 1)
CPI(t)− 1
CPI(t+ 1) = CPI(t) · (1 + it)
(4.3)
Using this formula, we can find out the estimate prices in certain years, even if we onlyhave the price from one year. For example, if we have benefit payment of Hospital Incomefor IDR 3,000,000 in 2018, then in 2017, the estimated benefit payment is:
BHI(2018) = BHI(2017) · (1 + i2017)
IDR 3, 000, 000 = BHI(2017) · (1 + 15%)
BHI(2017) = IDR 2, 608, 695.65
4. Insurance Awareness (a%)Another factor we need to address is the insurance awareness in Indonesia. Even in themodern times, there are still people who does not use any insurance for their own variousreasons. Therefore we should not assume that all eligible people will take part in thisinsurance, and instead adjust our price accordingly. In calculation, we will use a% toassume the portion of eligible people expected to buy the insurance.
4.2 Product Description and Premium Calculation Method
In this section, we will discuss the calculation of each condition mentioned in Section ??. Itshould be noted that this premium calculation does not include any expenses nor profit in itscalculation aside from the loss ratio.
17

4.2.1 Basic Insurance (NU ND HI)
The basic insurance is the simplest product which is free of any additional features. It will useno underwriting, no death benefits, and pays the same amount of money in each claim (HospitalIncome). This will be called ”NU ND HI” later on.
Calculating the premium of this product is very simple. Consider the following notation forthe average of 1000 Runge-Kutta runnings above:
• S1 = number of people susceptible of primary dengue infection.
• I1 = number of people infected with primary dengue.
• R1 = number of people recovered from primary dengue.
• S2 = number of people susceptible of secondary dengue infection.
• E2 = number of people already exposed to secondary dengue.
• I2 = number of people infected with secondary dengue.
• R2 = number of people recovered from secondary dengue.
Then, using the basic principle of actuarial product pricing,
Expected Premium Income = Expected Benefit Payment
p · Premium = q · Benefit
p · Premium · l0 = q · Benefit · l0(p · l0) · Premium = (q · l0) · Benefit
(4.4)
Since we know that the people eligible pay this insurance are those who are currently not infectedand are not immune to primary nor secondary dengue, and the ones eligible to receive benefitpayment are those who are currently infected, therefore:
Expected Premium Income = Expected Benefit Payment
(S1 +R1 + S2 + E2) · P = (I1 + I2) ·BHI(4.5)
where BHI is the Hospital Income benefit, and P is the premium price which we are goingto calculate. Incorporating the general features and assumptions above, such as Loss Ratio (l%),inflation, and insurance awareness (a%), then we will have:
(S1 +R1 + S2 + E2) · P = (I1 + I2) ·BHIa% · l% · (S1 +R1 + S2 + E2) · P = (I1 + I2) ·BHI(t)
P =(I1 + I2) ·BHI(t)
a% · l% · (S1 +R1 + S2 + E2)
(4.6)
4.2.2 Underwriting
Underwriting in this study simply means to differentiate between primary and secondary dengue.Either in its infection number, hospital prices, etc. In this section, we will further explore theoptions of underwritten insurance.
18

Same Premium but Different Benefits (U ND HI)
In this section, we will acknowledge the hypothesis that secondary treatments are more costlythan primary. Therefore, we will calculate the premium if both benefit payments differs. Con-sider two constants, k1 for primary and k2 for secondary, which is the ratio of benefit paymentfor specific type of dengue compared to the hospital income (BHI). These constants will bedefined as k1 = BHI,1/BHI and k2 = BHI,2/BHI. Therefore,
a% · l% · (S1 +R1 + S2 + E2) · P = [I1 ·BHI,1(t)] + [I2 ·BHI,2(t)]
a% · l% · (S1 +R1 + S2 + E2) · P = [I1 · k1 ·BHI(t)] + [I2 · k2 ·BHI(t)]
P =[(I1 · k1) + (I2 · k2)] ·BHI(t)
a% · l% · (S1 +R1 + S2 + E2)
(4.7)
Different Premiums, Different Benefits (U1 ND HI/U2 ND HI)
Obviously, primary susceptibles will think it is unfair for them to pay the same premium assecondary susceptibles, but receive less in terms of benefit. Therefore, we will try to calculatepremiums differently for each type of dengue.
Define P1 for primary protection premium and P2 for secondary protection.For primary,
S1 · P1 = I1 ·BHI,1 (4.8)
and for secondary,
(R1 + S2 + E2) · P2 = I2 ·BHI,2 (4.9)
Now, the result of this may be very different since S1 is vastly larger than R1, S2, and E2
combined. This will result in a very low premium for primary protection, and very expensiveone for secondary. A calculation using sample arbitrary values will result in Figure 4.2.
To solve this problem, we will transfer some of the primary susceptibles to help support thesecondary. We will need a constant s%, which is the portion of S1 accomodating the primary,therefore leaving S1(1− s%) to help the secondary.
Therefore, the equation becomes:
(S1 · s%) · P1 = I1 ·BHI,1
P1 =I1 ·BHI,1S1 · s%
(4.10)
and
[S1(1− s%) +R1 + S2 + E2] · P2 = I2 ·BHI,2
P2 =I2 ·BHI,2
S1(1− s%) +R1 + S2 + E2
(4.11)
To obtain the value of s, we have ran trial and errors, and found out that using the percentageof I1/I of each year as a base for s% works out nicely so that P2 is higher than P1, but is nottoo expensive.
Now, incorporating the general features, we obtain the following equations.
a% · l% · (S1 · s%) · P1 = I1 ·BHI,1(t)
P1 =I1 ·BHI,1(t)
a% · l% · S1 · s%(4.12)
19

Figure 4.2: Sample Product Premium with Underwriting, without Combining Support
for primary. Then, for secondary:
a% · l% · (S1(1− s%) +R1 + S2 + E2) · P2 = I2 ·BHI,2(t)
P2 =I2 ·BHI,2(t)
a% · l% · [S1(1− s%) +R1 + S2 + E2]
(4.13)
4.2.3 Death Benefit (NU D HI)
In most health insurance products, there is almost always a death benefit feature. This featuremay be attractive for buyers, but on the other hand, will increase the premium price, albeitslightly. In this section, we will discuss how to modify the basic insurance and add a deathbenefit feature in it. To make a underwritten insurance with death benefit, then we can simplymerge the two features into one product.
In the equation, we will simply break down the expected benefit payment. The benefitpayment now consists of two benefits, the infection benefit and death benefit. For the deathbenefit, we will use the case fatality rate of dengue from the Ministry of Health of RepublicIndonesia. In the equation, the case fatality rate will be notated as f%, and the death benefitas BD
Expected Premium Income = Expected Benefit Payment
Expected Premium Income = Expected Infection Benefit + Expected Death Benefit
(S1 +R1 + S2 + E2) · P = (I1 + I2) ·BHI + (I1 + I2) · f% ·BD
P =(I1 + I2) ·BHI + (I1 + I2) · f% ·BD
S1 +R1 + S2 + E2
P =(I1 + I2) · [BHI + f% ·BD]
S1 +R1 + S2 + E2
(4.14)
20

Incorporating the general features and assumptions,
a% · l% · (S1 +R1 + S2 + E2) · P = (I1 + I2) ·BHI(t) + (I1 + I2) · f% ·BD(t)
P =(I1 + I2) · [BHI(t) + f% ·BD(t)]
a% · l% · (S1 +R1 + S2 + E2)
(4.15)
4.2.4 Hospital Reimbursement
Insurances usually offer two kinds of health products, which are hospital income and hospitalreimbursement. With hospital income products, the insurer provides an income while the insuredis in the hospital. It is usually a fixed amount for a certain length of time, usually daily. Butthis study uses Indonesia’s national health insurance system (BPJS Kesehatan) as reference,and BPJS uses a hospital income for each claim, overlooking the length of stay of the insured.Therefore, we use the hospital income claim system as well. Calculation using the hospitalincome has been used in the formulations above.
Hospital reimbursement means the insurer pays the exact amount of the insured’s hospitalbill, though usually until a certain amount (maximum/ceiling). This is actually more compli-cated to calculate, and to do this we usually need a morbidity table to show the expected bill forany given age, policy year, et cetera. Unfortunately, there hasn’t been any study on morbiditytables conducted for dengue in Indonesia, so it isn’t possible to determine the expected benefitpayment for individual policies.
Hospital Reimbursement with No Limit (NU ND HRNL)
To make up for the morbidity table unavailability, the sample calculation will use an averagehospital cost for dengue from a general hospital in Jakarta [21] and Banjarnegara [18], which isobtained from other studies. Therefore, the premium is simply calculated as follows:
(S1 +R1 + S2 + E2) · P = (I1 + I2) ·BHR,NL
P =(I1 + I2) ·BHR,NLS1 +R1 + S2 + E2
(4.16)
Incorporating the general features and assumptions,
a% · l% · (S1 +R1 + S2 + E2) · P = (I1 + I2) ·BHR,NL(t)
P =(I1 + I2) ·BHR,NL(t)
a% · l% · (S1 +R1 + S2 + E2)
(4.17)
Hospital Reimbursement with Limit (NU ND HRL)
Not every insurance company is generous enough to compensate for the full hospital billing ofan insured person. This is why a maximum amount is set to minimise risk of extremely largelosses. Though the concept sounds simple, the calculation is rather complicated. Below we willcalculate the expected benefit payment for each insured with a maximum amount.
First, we will assume that benefit payments have normal probability distribution. Themean will be the average hospital reimbursement with no limit (BHR,NL), and the standarddeviation will be assumed (since there is no study about it yet). The distribution should besimilar to Figure 4.3, which uses standard deviation of IDR 1,000,000. Now we will calculatethe expected hospital reimbursement benefit payment, now with a limit. Let X be a randomvariable representing the benefit. First, we will choose a real number α ∈ [0, 1], so that P (X ≥1− xα) = α. In Figure 4.3, we will use α = 25%.
21

Figure 4.3: Hospital Reimbursement Probability Function using Normal Distribution
This xα is our hospital reimbursement limit. This will mean that for amounts of benefit abovexα - which is α portion of all payments - the insurer will only pay for xα. To determine theadjusted expected benefit payment per insured, we will use the expectation of random variableformula [9]. Let BHR,L be the adjusted expected benefit payment, then:
BHR,L =
∫ xα
0
x · f(x)dx+
∫ ∞xα
xα · f(x)dx (4.18)
Zero is used for the lower bound of the first integral because it is improbable to have negative
hospital costs, hence∫ 0
−∞ f(x) = 0. Using the adjusted benefit payment,
(S1 +R1 + S2 + E2) · P = (I1 + I2) ·BHR,L
P =(I1 + I2) ·BHR,LS1 +R1 + S2 + E2
(4.19)
and thus,
a% · l% · (S1 +R1 + S2 + E2) · P = (I1 + I2) ·BHR,L(t)
P =(I1 + I2) ·BHR,L(t)
a% · l% · (S1 +R1 + S2 + E2)
(4.20)
Any other product which is a combination of these three features can be calculated usingthe combination of these calculation methods.
4.3 Forecasting Method
The goal of this study is to price insurance products. obviously, to price the product we aregoing to launch, we need to forecast the variables needed in determining the price. In this
22

Figure 4.4: Predicted Number of People in the state of S1, R1 + S2 + E2, and Population
section, we will discuss the forecasting methods used for the variables.We should also note that since the trend is truly visible after year 2000. To be able to
forecast accurately, and to ensure our forecast is using the most related data, we will begin ourforecasting since year 2000.
4.3.1 Exponential Triple Smoothing
The forecasting method we are going to use the most in this study is exponential triple smooth-ing. Looking back at Figure 4.1, there are some obvious seasonality, especially since year 2000.To forecast this, it is crucial that we choose a method which includes seasonality in its calcu-lation. This is why the exponential triple smoothing is chosen, as it is an effective forecastingmethod which considers seasonality in its calculation.
Exponential Triple Smoothing (S1, I, R1+S2+E2, Population)
Specifically, we will use the AAA version of the advanced machine learning Exponential TripleSmoothing (ETS) algorithm to forecast future values based on historical data. This formula isbuilt in in excel, and is complicated and a bit out of this study’s scope, so we will use the builtin formula.
As we can see in Figure 4.4, there are no seasonality in these graphs. Therefore, we willnot use seasonality in our forecasting. The excel formula we are going to use is ”FORE-CAST.ETS(target date, values, timeline, seasonality, data completion, aggregation)”.
For example, if we are going to forecast the S1 for year 2016, then our formula shouldlook like ”FORECAST.ETS(2016,(S1 Data for Year 2000-2015),(Year 2000-2015),0,1,1)”. Afterforecasting, the three graphs will look like Figure 4.5.
23

Figure 4.5: Forecasted Number of People in the state of S1, R1 + S2 + E2, and Population
Seasonal Exponential Triple Smoothing (I, i%)
In this section, we will forecast the total infection rate per year (I). Note that we are notforecasting I1 nor I2, but the total infection which is I. This is because in Figure 4.1, there isa very visible correlation between I1/I and I2/I. Hence, we should forecast I first, then we canforecast I1 and I2 using its percentage (this will be done in Section 4.3.3.
If we look at Figure 4.6, it is obvious that there is a seasonality trend, especially since 2000where more study on dengue has been conducted, resulting in a more accurate form of predictedtotal infection. Now, in forecasting total number of infected people, we need to make sure thatthe total number of infected people is below the population. To ensure this, we will calculatethe rate of infection (I/Population) first, then perform the forecasting using the rate of infectionrather than the number of infection. The rate of infection can be seen in Figure 4.7.
First, we need to determine the period of seasonality. Since there is one local maximum andone local minimum in the graph, it should be reasonable to conclude that the time between thetwo local extremes are half a seasonality period. Hence we obtain 10 years of seasonality period.
Using the same excel formula, if we wish to obtain the forecasted value of I for 2016, on ex-cel we should calculate ”FORECAST.ETS(2016,(I/Population Data for Year 2000-2015),(Year2000-2015),10,1,1)”. The forecasted I/Population data should be similar to Figure 4.8.
It may also be beneficial to calculate the lower and upper bound for this forecast, since it mayvary with its seasonality parameter, etc. To do this, we will use the FORECAST.ETS.CONFINTformula in excel, which is ”FORECAST.ETS.CONFINT(target date, values, timeline, confi-dence level, seasonality, data completion, aggregation)”.
For example, using confidence interval of 95%, then the formula to calculate the difference be-tween the lower/upper bound and the forecasted value in 2016 is ”FORECAST.ETS.CONFINT(2016,(S1
Data for Year 2000-2015),(Year 2000-2015),0.95,10,1,1)”.
24

Figure 4.6: Predicted Total Number of People Infected by Dengue (Primary and Secondary)
Figure 4.7: Predicted Rate of Infection
25

Figure 4.8: Forecasted Rate of Infection
Finally, multiplying it back with the predicted population, the forecasted total number ofinfection should be similar to Figure 4.9.
For inflation, the same is used. If for example we use the inflation seasonality of 5 years(for every change in governmental leadership), then we get the following values in Table 4.2 andFigure 4.10.
4.3.2 Exponential Distribution Fitting (R2)
There is one variable which forecasting method is different from the others. R2, or the numberof people recovered from secondary dengue, is a number which constantly increases. Looking atFigure 4.11, we can conclude that the shape of R2 is similar to that of an exponential function.To forecast this, one method is to fit the shape into that of an exponential distribution. But it ispossible that this kind of forecasting may exceed the total population, therefore an adjustmentneed to be made. Another method, is to forecast R2/Population, or the secondary recoveryrate.
This rate is going to be fitted into an exponential function. One basic form of exponentialfunction is f(t) = A · eB·(t+C) +D, with t as its year. Minimising its normalised error, we foundthe best fitted function using the variables in Table 4.3. The comparison is shown in Figure4.12. Expanding the function into further years, and multiplying it back with the populationwill generate the forecasted number of people recovered from secondary infection.
4.3.3 Other Methods (I1 I2)
Lastly, we need to forecast the rate of I1/I and I2/I, to determine I1 and I2. As we can seein Figure 4.1 in Section ??, there are obvious patterns of interchanging hills and hollows. Theproblem is, with lack of data, the graph hasn’t form a full period. Therefore, when we try toforecast it using exponential triple smoothing or other functions, we get a repetitive ”∩” or ”∪”pattern. To solve this, we need to use more creative, yet laborous method, that is interchanging
26

Figure 4.9: Forecasted Number of Infected People
the historical data. We will use I1 data for forecasting I2, vice versa. The result is similar toFigure 4.14, and multiplying it back with the total infection results in Figure 4.15.
4.4 Sample Calculation Result
Using the methods in sections above, we are going to create sample products using severalarbitrary numbers listed in Table 4.4. The calculated premiums is shown in Figure 4.16.
27

Table 4.2: Forecasted Rate of Inflation
Year Inflasi CPI Lower Upper2000 9.35%2001 12.55%2002 9.92%2003 5.17%2004 6.47%2005 17.07%2006 6.60%2007 6.59%2008 10.23%2009 2.78%2010 6.96%2011 3.79%2012 4.30%2013 7.72%2014 8.36%2015 3.35%2016 3.02%2017 3.61%2018 6.85% 0.70% 13.00%2019 7.29% 1.39% 13.19%2020 4.12% -0.43% 8.68%2021 2.46% -1.88% 6.80%2022 2.98% -1.20% 7.17%2023 6.51% 2.45% 10.56%2024 7.24% 3.34% 11.15%2025 4.10% 0.30% 7.90%
Table 4.3: Exponential Fitting Function Variables of R2/Population
A B C D Normalized Error0.008203894 0.498081 -2002.63672 7.191401 0.000425
28

Figure 4.10: Forecasted Rate of Inflation
Figure 4.11: Predicted Number of People Recovered from Secondary Infection (R2)
29

Figure 4.12: Comparison between R2/Population Predicted and Exponential Fitting
Figure 4.13: Forecasted Number of People Recovered from Secondary Infection (R2)
30

Figure 4.14: Forecasted Primary and Secondary Portion of Infection (I1/I and I2/I)
Figure 4.15: Forecasted Primary and Secondary Infection (I1 and I2)
31

Table 4.4: Values for Sample Product Calculation
Asumsi Value SourceInsurance Awareness (a%) 50% Arbitrary
Loss Ratio (l%) 60% Arbitrary
HI Benefit Rp 3,021,400.00BPJS Kesehatan, Regional Hospital Type C,First Class [12]
U1/HI Benefit (k1) 0.80 ArbitraryU2/HI Benefit (k2) 1.30 Arbitrary
HRNL Benefit Rp 3,606,233.50 Dengue Cost Studies [21] [18]Std HRNL Rp 1,000,000.00 Arbitraryα for HRL 25% Arbitrary
Death Benefit (DB) 150,000,000.00 Prudential product: PRUprime healthcare
Death Rate (f%)Data from Ministry of Health of RepublicIndonesia [11]
Inflation (i%) Data from Section 4.1
Inflation Seasonality 5.00 yearsArbitrary (Change in GovernmentalLeadership)
I Seasonality 10.00 yearsPeriod between the I local extremesfrom Section 4.3
32

Tab
le4.5
:S
am
ple
Pro
du
ctC
alc
ula
tion
NU
ND
HI
UN
DH
IU
1N
DH
IU
2N
DH
IN
UD
HI
NU
ND
HR
NL
NU
ND
HR
L
Yea
rN
on-
Un
der
wri
tten
Sam
eP
rem
ium
,D
iffB
enefi
tP
rim
ary
Pro
tect
ion
Sec
on
dary
Pro
tect
ion
Dea
thB
enefi
tH
osp
.R
eim
bu
rsem
ent
Wit
hN
oL
imit
Hosp
.R
eim
bu
rsem
ent
Wit
hL
imit
2000
IDR
642.
79ID
R69
6.35
IDR
526.4
9ID
R821.0
2ID
R1,0
16.5
4ID
R767.2
2ID
R735.6
620
01ID
R80
3.12
IDR
826.
49ID
R658.2
4ID
R1,0
15.3
5ID
R1,1
70.0
3ID
R958.5
8ID
R919.1
520
02ID
R1,
069.
24ID
R1,
046.
25ID
R877.3
9ID
R1,3
29.9
5ID
R1,6
46.5
3ID
R1,2
76.2
0ID
R1,2
23.7
220
03ID
R1,
420.
46ID
R1,
329.
89ID
R1,1
67.7
8ID
R1,7
22.8
4ID
R2,3
05.3
7ID
R1,6
95.4
1ID
R1,6
25.6
820
04ID
R1,
811.
00ID
R1,
637.
58ID
R1,4
92.9
2ID
R2,1
16.7
8ID
R2,7
13.5
6ID
R2,1
61.5
4ID
R2,0
72.6
420
05ID
R2,
299.
03ID
R2,
027.
83ID
R1,9
02.2
2ID
R2,5
57.2
8ID
R3,6
35.7
9ID
R2,7
44.0
4ID
R2,6
31.1
920
06ID
R3,
101.
93ID
R2,
692.
77ID
R2,5
78.4
0ID
R3,2
56.6
2ID
R4,3
90.2
1ID
R3,7
02.3
5ID
R3,5
50.0
820
07ID
R3,
635.
24ID
R3,
129.
84ID
R3,0
37.9
5ID
R3,6
14.2
7ID
R5,1
45.0
3ID
R4,3
38.9
0ID
R4,1
60.4
520
08ID
R4,
032.
14ID
R3,
467.
40ID
R3,3
89.0
9ID
R3,8
71.5
9ID
R5,5
39.2
9ID
R4,8
12.6
1ID
R4,6
14.6
820
09ID
R4,
373.
66ID
R3,
784.
90ID
R3,6
97.0
8ID
R4,1
92.2
3ID
R6,0
08.4
7ID
R5,2
20.2
4ID
R5,0
05.5
520
10ID
R4,
214.
84ID
R3,
705.
28ID
R3,5
81.1
1ID
R4,1
79.8
3ID
R5,7
37.7
7ID
R5,0
30.6
8ID
R4,8
23.7
820
11ID
R4,
101.
26ID
R3,
709.
98ID
R3,4
99.2
6ID
R4,3
14.4
1ID
R5,6
34.2
6ID
R4,8
95.1
2ID
R4,6
93.8
020
12ID
R3,
872.
54ID
R3,
665.
46ID
R3,3
14.3
3ID
R4,3
49.5
3ID
R5,3
20.0
3ID
R4,6
22.1
2ID
R4,4
32.0
220
13ID
R3,
828.
97ID
R3,
858.
46ID
R3,2
83.5
6ID
R4,5
48.0
8ID
R4,9
42.1
4ID
R4,5
70.1
2ID
R4,3
82.1
720
14ID
R4,
254.
23ID
R4,
607.
64ID
R3,6
51.8
7ID
R5,2
56.4
1ID
R5,8
44.4
1ID
R5,0
77.7
0ID
R4,8
68.8
720
15ID
R5,
359.
28ID
R6,
204.
25ID
R4,6
01.1
7ID
R6,7
83.0
1ID
R7,4
99.7
5ID
R6,3
96.6
5ID
R6,1
33.5
7F
2016
IDR
7,02
2.06
IDR
8,39
6.66
IDR
6,0
47.3
2ID
R8,9
60.9
7ID
R8,7
64.3
1ID
R8,3
81.2
8ID
R8,0
36.5
8F
2017
IDR
8,88
9.25
IDR
10,8
26.7
6ID
R7,6
78.7
2ID
R11,3
90.8
3ID
R10,6
11.3
8ID
R10,6
09.8
8ID
R10,1
73.5
3F
2018
IDR
9,97
2.61
IDR
12,2
85.3
0ID
R8,6
38.4
0ID
R12,8
10.0
1ID
R11,4
37.9
2ID
R11,9
02.9
5ID
R11,4
13.4
1F
2019
IDR
10,6
18.2
3ID
R13
,156
.30
IDR
9,2
22.2
0ID
R13,6
54.1
0ID
R12,2
38.2
2ID
R12,6
73.5
4ID
R12,1
52.3
1F
2020
IDR
10,1
58.7
4ID
R12
,597
.42
IDR
8,8
46.5
0ID
R13,0
61.6
5ID
R10,9
86.9
4ID
R12,1
25.1
0ID
R11,6
26.4
3F
2021
IDR
9,73
5.29
IDR
12,0
19.3
3ID
R8,4
99.0
0ID
R12,4
98.6
2ID
R10,0
66.3
9ID
R11,6
19.6
9ID
R11,1
41.8
0F
2022
IDR
9,25
6.85
IDR
11,3
01.6
6ID
R8,1
00.9
9ID
R11,8
42.8
2ID
R9,5
91.3
1ID
R11,0
48.6
4ID
R10,5
94.2
4F
2023
IDR
9,45
4.82
IDR
11,3
02.3
4ID
R8,2
93.8
7ID
R12,0
11.6
0ID
R9,8
06.7
5ID
R11,2
84.9
3ID
R10,8
20.8
1F
2024
IDR
11,0
16.7
5ID
R12
,707
.53
IDR
9,6
85.7
8ID
R13,8
06.3
1ID
R11,7
88.4
5ID
R13,1
49.2
0ID
R12,6
08.4
1F
2025
IDR
13,0
40.8
2ID
R14
,244
.49
IDR
11,4
90.4
8ID
R15,9
12.1
7ID
R14,2
08.2
3ID
R15,5
65.0
5ID
R14,9
24.9
0
33

Fig
ure
4.16:
Com
pari
son
bet
wee
nS
am
ple
Pro
du
ctP
rem
ium
s
34

Chapter 5
Conclusions
5.1 Conclusions
In this study, we have created and priced sample micro-insurance products, based on data ofprimary and secondary dengue using an epidemiological model.
We use three general features in all of our sample products, which are loss ratio, inflation,and insurance awareness. Loss ratio is the comparison between expected benefit payment andexpected premium income. This functions to cushion the insurer from unexpected losses. In-flation, is the rate at which prices rise. Inflation is always a significant factor for everythingfinance-related, and adding this to our calculation will produce a more accurate price. Lastly,insurance awareness is our expected portion of eligible people who will buy the insurance, whichfunction is also to cushion insurer’s losses. There are three conditions we use to create six basicproducts. It is basic because some of the methods in creating these products can be combinedto create a more advanced product. The three conditions are underwriting, death benefit, andhospital income/reimbursement. Underwriting allows us to assess an individual’s risk and pricetheir premium accordingly. This results to different prices for people in different states, suchas primary susceptible or secondary susceptible. Death benefit is an add-on, in which the in-surer gives a benefit in case the insured dies because of dengue. This may be attractive to thebeneficiaries, but it does increase the premium. For payment method, the two most commonare hospital income and hospital reimbursement. Hospital income pays a fixed amount (per acertain length of time or per claim), while hospital reimbursement pays the exact amount of theinsured’s hospital billing (usually with a maximum limit). The latter is more complicated tocalculate and needs more information which are not currently available.
The formula we use is the basic principle of actuarial science: which is expected benefit andexpected income, but modified to incorporate loss ratio, inflation, and insurance awareness. Forunderwriting, we use a mutual-cooperation system, in which the primary susceptibles help coverthe secondary’s load. This way, the premium for secondary protection is consistently higher thanprimary, but not too expensive either.
For death benefit, we use the same formula. The difference is that the expected benefitpayment is not for infection benefit only, but added with the expected death benefit paymenttoo. This expected death benefit payment uses case fatality rate and a sample death benefit asits variable.
Between the two payment methods, the hospital income is quite simple. In this study, thehospital income is a fixed amount paid for every claim. Therefore, the benefit is fixed in everycalculation. For hospital reimbursement without limit, we use the average amount paid for each
35

dengue claim. With limit, first we assume that the hospital reimbursement benefit payment hasa normal probability distribution. Then, we set the limit, and we use the expectation of randomvariable to calculate the adjusted expected benefit payment.
The calculation result is shown in Table 4.5 as a table, or as a graph in Figure 4.16.
5.2 Recommendations
Methods and formulas used in this study still has a lot of room for development, in order toproduce a more accurate product pricing. Several items which can be developed are:
1. The assumption we use for benefit payment probability distribution is normal distribution.There are of course a lot of other distributions which may represent the benefit paymentdistribution more accurately. Some of the possible distributions are Generalized ExtremeValue, such as Weibull, Fretchet, Gumbel, etc.
2. For the product calculation, some of the values we use are arbitrary because of lack ofstudies about dengue, particularly in Indonesia. It would be better if the values is takenfrom appropriate studies which represents the actual conditions, given that there has beensuch studies conducted.
3. Data on dengue before year 2000 is very limited, which may affect the forecasting, resultingin inaccurate forecast values. With a heavy heart, we discard data prior to year 2000 inthis study. It is advised to find more data on prior years, or to wait another few years inorder to produce a more accurate forecast results.
36

Bibliography
[1] Situasi Demam Berdarah Dengue di Indonesia. Kementerian Kesehatan Republik Indone-sia, 2014.
[2] Situasi Demam Berdarah Dengue di Indonesia. Kementerian Kesehatan Republik Indone-sia, 2016.
[3] Canyon, D. V. Historical analysis of the economic cost of dengue in australia. Journalof vector borne diseases 45 (2008), 245–248.
[4] Fahri, S., Yohan, B., Trimarsanto, H., Sayono, S., Hadisaputro, S., Dharmana,E., Syafruddin, D., and Sasmono, R. T. Molecular surveillance of dengue in semarang,indonesia revealed the circulation of an old genotype of dengue virus serotype-1. PLoSneglected tropical diseases 7, 8 (2013), e2354.
[5] Fullam, D., and Madhav, N. Quantifying pandemic risk. The Actuary (The magazineof the Society of Actuary) (February-March 2015).
[6] Gubler, D. J. Epidemic dengue/dengue hemorrhagic fever as a public health, social andeconomic problem in the 21st century. Trends in microbiology 10, 2 (2002), 100–103.
[7] Halasa, Y. A., Shepard, D. S., and Zeng, W. Economic cost of dengue in puertorico. The American journal of tropical medicine and hygiene 86, 5 (2012), 745–752.
[8] Hewitt, A. 2017 Global Medical Trend Rates. Aon Hewitt, 2017.
[9] Hogg, R., McKean, J., and Craig, A. Introduction to Mathematical Statistics. Pearsoneducation international. Pearson Education, 2005.
[10] IFoA. Longevity Bulletin - The Pandemics Edition. The Faculty and Institute of Actuaries,July 2015.
[11] Indonesia, D. K. R. Situasi dbd di indonesia. Situasi DBD di Indonesia (Apr 2016).
[12] Indonesia, M. K. R. Peraturan menteri kesehatan republik indonesia nomor 59 tahun2014 tentang standar tarif pelayanan kesehatan dalam penyelenggaraan program jaminankesehatan, 2014.
[13] Kusmintarsih, E. S., Hayati, R. F., Turnip, O. N., Yohan, B., Suryaningsih, S.,Pratiknyo, H., Denis, D., and Sasmono, R. T. Molecular characterization of dengueviruses isolated from patients in central java, indonesia. Journal of infection and publichealth (2017).
[14] Media, T. Historic inflation indonesia - cpi inflation.
37

[15] Megawati, D., Masyeni, S., Yohan, B., Lestarini, A., Hayati, R. F., Meutiawati,F., Suryana, K., Widarsa, T., Budiyasa, D. G., Budiyasa, N., et al. Dengue inbali: Clinical characteristics and genetic diversity of circulating dengue viruses. PLoSneglected tropical diseases 11, 5 (2017), e0005483.
[16] Nusa, R., Prasetyowati, H., Meutiawati, F., Yohan, B., Trimarsanto, H., Se-tianingsih, T. Y., and Sasmono, R. T. Molecular surveillance of dengue in sukabumi,west java province, indonesia. The Journal of Infection in Developing Countries 8, 06(2014), 733–741.
[17] Patz, J. A., Martens, W., Focks, D. A., and Jetten, T. H. Dengue fever epidemicpotential as projected by general circulation models of global climate change. Environmentalhealth perspectives 106, 3 (1998), 147.
[18] Rejeki, V. M. M., and Nurwahyuni, A. Cost of treatment demam berdarah dengue(dbd) di rawat inap berdasarkan clinical pathway di rs x jakarta. Jurnal Ekonomi KesehatanIndonesia 2, 2 (2017).
[19] Rothman, A. L. Dengue: defining protective versus pathologic immunity. The Journalof clinical investigation 113, 7 (2004), 946–951.
[20] Sasmono, R. T., Wahid, I., Trimarsanto, H., Yohan, B., Wahyuni, S., Hertanto,M., Yusuf, I., Mubin, H., Ganda, I. J., Latief, R., et al. Genomic analysis andgrowth characteristic of dengue viruses from makassar, indonesia. Infection, Genetics andEvolution 32 (2015), 165–177.
[21] Sihite, E. W., Mahendradata, Y., and Baskoro, T. Beban biaya penyakit demamberdarah dengue di rumah sakit dan puskesmas. Berita Kedokteran Masyarakat 33, 7(2016), 357–364.
[22] Suaya, J. A., Shepard, D. S., Siqueira, J. B., Martelli, C. T., Lum, L. C., Tan,L. H., Kongsin, S., Jiamton, S., Garrido, F., Montoya, R., et al. Cost of denguecases in eight countries in the americas and asia: a prospective study. The American journalof tropical medicine and hygiene 80, 5 (2009), 846–855.
[23] Sukirno, S. Pengantar teori makroekonomi. Bina Grafika, 1981.
[24] Suwandono, A., Kosasih, H., Kusriastuti, R., Harun, S., Maroef, C., Wuryadi,S., Herianto, B., Yuwono, D., Porter, K. R., Beckett, C. G., et al. Fourdengue virus serotypes found circulating during an outbreak of dengue fever and denguehaemorrhagic fever in jakarta, indonesia, during 2004. Transactions of the Royal Society ofTropical Medicine and Hygiene 100, 9 (2006), 855–862.
[25] Wardhani, P., Aryati, A., Yohan, B., Trimarsanto, H., Setianingsih, T. Y.,Puspitasari, D., Arfijanto, M. V., Bramantono, B., Suharto, S., and Sasmono,R. T. Clinical and virological characteristics of dengue in surabaya, indonesia. PloS one12, 6 (2017), e0178443.
[26] Watson, W. T. 2016 Global Medical Trends Survey. Willis Towers Watson, Apr 2016.
38

Appendix A
Financial Report
39

Table A.1: Financial Expenditure READI Applied Research Funding
No Description Amount
1 Payment for research assistant (Felicia Sofian) 2,000,000
2 Payment for research assistant (Felicia Sofian) 2,500,000
3 Payment for research assistant (Lucy Jap) 6,000,000
4 Equipment (Laptop Dell Inspiron 13 7000) 17,799,000
5 Books (bought at UW Book Store):1. The Mathematics of Statistical Modeling2. Longitudinal Data Analysis3. Generalized Linear Model(Total: CAD 279.90)
3,130,123
6
SoA Actuarial Teaching Conference (HelenaMargaretha) July 8-9, 20161. Partial Airfare JKT-HK-JKTRp 4,741,900 - (USD 250 x 14.000 RP/USD)
1,241,900
2. Hotel Le Jen 1 night HKD 1,251.30 2,360,593
3. Registration fee USD 50 729,137
7 Books (bought at Amazon):1. Applied Semi-Markov Processes(Total: CAD 76.79 x Rp 11,183 / CAD)
858,743
8 Books (bought at Actex Book Store):1. Introduction to Credibility Theory2. Individual Health Insurance3. Regression Modeling with Actuarial andFinancial Applications
6,004,568
9 Payment for work assistant (Ferry V.F) 6,000,000
10 Publication fee 26,375,936
TOTAL 75,000,000
40