Embed Size (px)
Citation preview
Calcific Aortic Valve disease and Lp(a)
Kate Kearney 4/17/2012

Outline Calcific Aortic Valve Disease (CAVD)—an
active process
Lp(a) is a lipid that appears to be important in CAVD
AGES-Reykjavik is an elderly Icelandic cohort
CAVD scored on CT scan correlates with Lp(a)
Calcific Aortic Valve Disease Aortic Sclerosis
Thickened, calcified valve
Lack of outflow obstruction Velocity <2.5m/s
across AV 25% in those >65yo1
Associated w/ 50% increased risk CV event2
Subset progress to Aortic Stenosis 1-2% per year
Aortic Stenosis AV velocitity >2.5m/s 2.5% in >65yo age
group Associated 80% 5-yr
risk progression to Heart failure Need for AV
Replacement Death
1. Stewart et al. Cardiovascular Health Study. 2. Otto et al N Engl J Med 1999

Calcific Aortic Valve Disease Age is a clear factor, but not the only one Progressive disease with no medical treatment
Valve replacement only definitive treatment, timing of surgery can be difficult
Increasing evidence for role of endothelial injury (inflammatory, high tensile stress) and lipid deposition in the early phases
Significant overlap with risk factors in CAD

CAVD risk factors overlap with CAD
Cardiovascular Health Study (Stewart et al JACC 1997)
Framingham Offspring Study (Thanassoulis et al JACC 2010)
Variable OR (95% CI)
Age (75th vs 25th)
2.18 (2.15-2.2)
Male Gender 2.03 (1.7-2.5)
Lp (a) (10 unit incr)
1.23 (1.14-1.32)
h/o HTN 1.23 (1.1-1.4)
Present Smoking
1.35 (1.1-1.7)
LDL (10 unit incr)
1.12 (1.03-1.23)
Variable OR (95% CI)
Age, per SD 3.25 (2.76-3.82)
Female gender 0.56 (0.41-0.76)
Total CH 1.74 (1.5-2.01)
Mean HDL 0.77 (0.66-0.91)
BMI 1.21 (1.05-1.4)
Cigarettes daily 1.23 (1.08-1.41)-Framingham CHD risk score also significantly correlated
with prevalence and severity of Aortic Valve Calcium

Aortic Stenosis pathophysiology Inflammatory Cells and
Lipoproteins, including Lp(a) co-localize in AV lesions, sim to Coronary atherosclerosis
Macrophages and T lymphocytes found in valves
LDL and Lp(a) deposits Oxidized lipids found in
human lesions, particularly developing calcifications
Calcification is active process
O'Brien K D et al. Arterioscler Thromb Vasc Biol 1996;16:523-532
apo B
apo (a)
macrophages
Ca++

Lipids and Calcific Aortic Valve Disease Strong association with CAD, CAD risk factors
Perhaps similar treatment will be effective?
Multiple trials looked at Statins and Aortic Stenosis
Three randomized prospective trials were negative for effect Ranging in size and f/u time 2-5yr, Atorvastatin, Simva
+Ezetimibe and Rosuvastatin failed to effect Jet velocity or peak gradient
Asymptomatic mild-moderate disease in SEAS and ASTRONOMER, SALTIRE included those with severe AS
Too little? Too Late?

Lipoprotein(a) consists of an LDL-like particle to which apolipoprotein(a) is covalently linked.
Nordestgaard B G et al. Eur Heart J 2010;eurheartj.ehq386
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2010. For permissions please email: [email protected]
Lp(a) CV risk factor with unclear role
Recommended by some authors to screen in high-risk patients
Appears important in setting elevated LDL Appears to be particularly important in those with
elevated LDL1
Niacin is currently available treatment Dose dependent reduction in levels 30-40%
Determinants: 90% genetics, mostly stable over lifetime Genetics LPA locus variations (encoding Lp(a)) strongly
associated with CAD Strong relationship with LPA locus recently demonstrated
1. Luc Lipoprotein (a) as a predictor of coronary heart disease: the Prime Study. Atherosclerosis 2002; 163(2):377-84.

GWAS demonstrates SNP at LPA locus associated with CAVD LPA locus encoding Lp(a) lipoprotein
Lp(a) levels known to be ~90% genetically determined
This SNP previously shown to associate with CAD risk
This study confirmed association with Lp(a) levels
Strongly associated with Aortic Valve Calcium Scores
Holds across multiple Euro-descent cohorts (including AGES), verified in other cultural groups (MESA database) Each risk allele confers 68% increased risk Correlated with clinical outcomes, need AVR
Thanassoulis G, Campbell CY, Owens DS et al . A genome wide association study identifies novel loci for aortic valvular and mitral annular calcium and implicates LPA in the development of Aortic Stenosis. (Unpublished)
AGES-R Study Age, Gene/Environment Susceptibility-Reykjavik
Study The Reykjavik study is an established population-
based cohort, established 1967 Men and Women born 1907-1935, followed by Icelandic
Heart Association for prospective study of CVD AGES initiated in 2002 to examine risk factors and
interaction with complex traits, using improved phenotypes based off subclinical disease
Reykjavik provides mid-life data, collected prospectively and followed therefore less biased than retrospective recall
AGES examining same subjects in old age, examining for clinical events and subclinical disease (labs, imaging)

Population
Our Study… Hypothesis: The lipoprotein Lp(a) is associated
with prevalence and severity of calcific aortic valve disease (CAVD) and interacts with individual LDL cholesterol levels.
Population: AGES-R elderly cohort with mid-life LDL levels and followup LDL and Lp(a) levels, CT scans scored for AVC. Exclusions: prior AVR, known CAD, statin use Cross sectional evaluation of interaction of LDL
and Lp(a) with Aortic Valve Calcification

CAVD scored by CT-Agatston method Areas of calcium defined by brightness
(Hounsfield un) in contiguous pixels Includes valve leaflets only, not aorta or coronary
arteries Scores can be used as continuous or
dichotomous variable Does not provide functional data, but scores
above a threshold predict stenosis or severe disease Suggestion of prognostic information Validated with and Complementary to TTE
Detects subclinical disease Important in our model of CAVDMessika-Zeitoun et al. Eval and clinical implications of aortic valve calcification measured by electron-beam CT. Circ 2004

Our Study… Evaluate relationship between Lp(a) and AVC
scores within these LDL groups Test variable interactions using multivariable
regression with the presence and severity of AVC, as measured by the Agatston method from AGES-Reykjavik baseline CT scans.
Control for confounders based off prior epidemiological data: Age, gender, smoking history, Statin and Niacin use (if not excluded) use anti-HTN, diabetic medications

LDL Distribution in AGES-R Separate subjects
into 3 groups based off clinical LDL cutpoints: <130, 130-160, >160 Approximate tertiles
Note persistence of elevated LDL in Elderly (lack expected
survival bias) After excluding statin-
users
01
002
003
004
00
70 80 90 100 70 80 90 100
Male Female
LDL cholesterol (mg/dL Fitted values
Subject age (years)
Graphs by Sex (0=Male 1=Female)
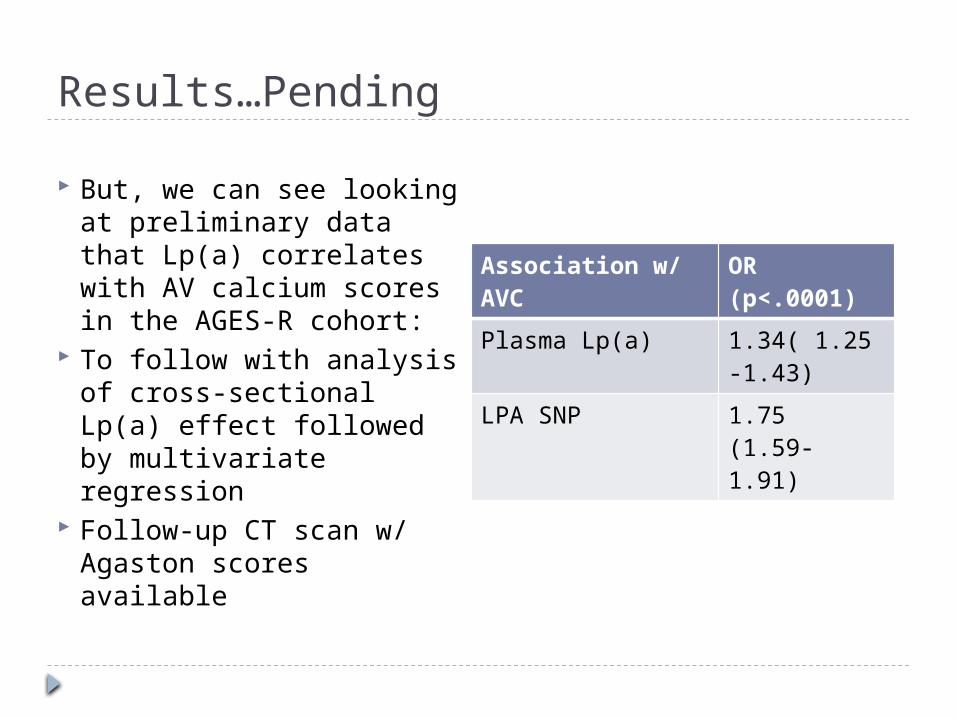
Results…Pending
But, we can see looking at preliminary data that Lp(a) correlates with AV calcium scores in the AGES-R cohort:
To follow with analysis of cross-sectional Lp(a) effect followed by multivariate regression
Follow-up CT scan w/ Agaston scores available
Association w/ AVC
OR (p<.0001)
Plasma Lp(a) 1.34( 1.25-1.43)
LPA SNP 1.75 (1.59-1.91)
Summary Calcific aortic valve disease and athersclerosis
have similar risk factors and overlap We now know lipids are involved in the
development of CAVD Lp(a) is similar to LDL, largely genetically
determined, and shown to correlate and demonstrate causal relationship with CAVD
LDL and Lp(a) appear to interact, but this has not been studied in a clinical cohort
Lp(a) is associated with CAVD in the AGES-R cohort





























