Embed Size (px)
Citation preview

Caffeine Does NotEnhanceEndurance Performance (CP)
Alex Dunbar
Malcolm MacRitchie
Sabina Wu

Road Map
1. Hypothesis
2. Mechanism of AcFon
3. RDA, Clinical, and Normal Use
4. Research SupporFngCP
5. Research RefuFng P
6. RefuFng OpposiFon's Claims
7. Conclusion
8. Reference List

Hypothesis
*Counterpoint: Caffeine does notimprove endurance sportsperformance.
Point: Caffeine improvesendurance sports performance.

Caffeine Mechanism• 2 metabolites
1) 1,7 - Dimethylxanthine2) 1,3 - Dimethylxanthine(Theophylline) which ↑Systolic BP:- ↑ Renal plasma flow- ↑ Glomerular filtraFon rate(DehydraFon = ↓ Endurance)(Cornish and Christman, 1957)
• ↑ SNS- ↑ Adrenaline- ↑ Vasoconstrictor tone- ↑ Vascular resistance- ↑ Mean blood pressure (ANG II)- ↑ K clearance (Na-K ATPase)=> hypokalemia = ↓ Endurance(Graham et al, 2000)
Fig. 1
(Cornish and Christman, 1957)

RDA, Clinical Use, Safe Dosage
• Coffee/tea = average40-100 mg of caffeine
• Over the countersupplements have100-200 mg of caffeine
• Clinical dose = average32- 200 mg
• NoRDA forcaffeineexists
• To overdose on caffeineone needs to ingest > 5 gor have 183 mg per litreof blood
• It is used as a mildcentral nervoussFmulant
(Kerrigan and Lindsey, 2005)

Research Results SupporFng CP - 1DehydraFon
• At caffeinedoses >90mg↑ urinary sodium (Na+) excreFon
• Doses of 360mg caffeine:↑ Urine volume↓ Serum Potassium (K+)
• Dehydra@on = ↓ performance
• DiureFc effect may be dueto:– ↑ glomerular filtraFon rate– ↑ renal blood flow– ↓ tubular reabsorpFon of Na+
(Passmore et al, 1987)
Fig. 2
Treatments: Caffeine 45mg, 90mg, 180mg, 360mg, placebo

• Pressure from loweresophageal sphincter (LES)separates esophagus from theintra-abdominal stomach
• LESdysfuncFon canlead toeither gastric reflux disease ordysphagia
Results: 3.5mg/kg caffeineaffected esophageal funcFon
• ↓ in basal LESpressure &distal esophageal contracFon(known to promote gastricreflux)
(Lohsiriwat et al, 2006)
Research Results SupporFng CP - 2aGastrointesFnal Distress
3
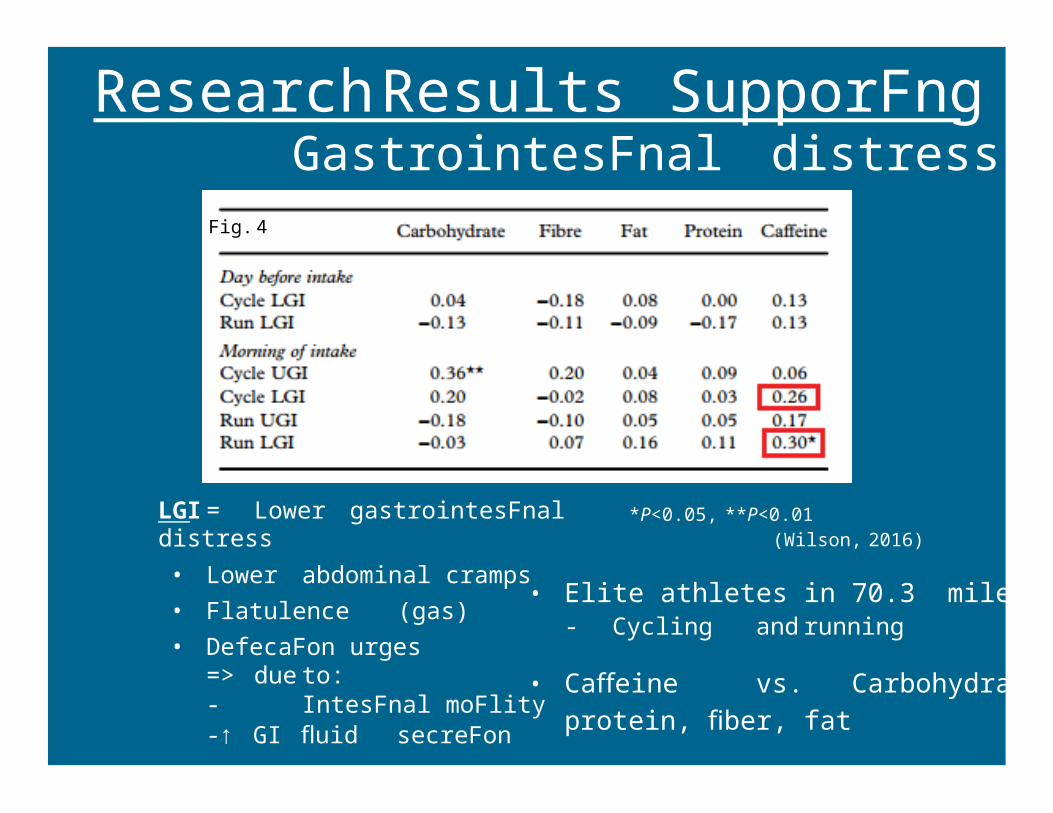
Research Results SupporFng CP - 2bGastrointesFnal distress
• Eliteathletes in 70.3miletriathlon- Cycling and running
• Caffeine vs. Carbohydrates,protein, fiber, fat
LGI = Lower gastrointesFnaldistress• Lower abdominal cramps• Flatulence (gas)• DefecaFon urges
=> due to:- IntesFnal moFlity-↑ GI fluid secreFon
Fig. 4
*P<0.05, **P<0.01(Wilson, 2016)

Research Results SupporFng CP - 3SubstrateUFlizaFon
Experimental Groups:• decaffeinated coffee (D)• decaffeinated coffee +
400mg caffeine (CA)→ following a controlrun(C)
• 400mg of caffeine didn’tchangethe respiratoryexchange raFo (RER) orsupport carbohydrate sparingat 75% of VO2max
• Both caffeinated anddecaffeinated had the sameRPE that was less than thecontrolgroup for running(Casal & Leon, 1985)
(Casal and Leon, 1985)
*Caffeine stimulated the SNS but did not alter the carbohydrate or fat metabolism (Graham et al, 2000)
Fig. 5

Research Results RefuFng Point - 1Tolerance
• 18 low-habitual caffeineconsumers (<75 mg·day−1)randomly assigned caffeine(1.5–3.0 mg·kg−1day−1) or placebofor28 days
• 60 mincycling at 60% VO2peak
• ↑ work in iniFal caffeinetrial(precaf)trialvs placebo(testpla)in all subjects
• Performance benefit no longerapparent aOer 4 weeks ofcaffeine supplementa@on(Beaumont et al, 2016)
• chronic ingesFon of a lowdose ofcaffeine= tolerance developed
(Beaumont et al, 2016)
*substrate oxidaFon was not influencedeither by acute or chronic caffeinesupplementaFon
Fig. 6 Total external work produced (kJ) during the experimental trials(n=18) in iniFal placebo trial (testpla) , iniFal acute caffeine trial (precaf),& caffeine trial on day 29 (postcaf) where * and # denotea within-groupsignificant difference (P < 0.05) compared with testpla

Research Results RefuFng Point - 2Sub-Elite vs Elite Cyclists
• 3 days of idenFcalexperimentaltests (60min cycling Fme trialon70 % VO2max followed by test toexhausFon)
3 treatments:• No caffeine/Placebo(PLA)• 2 mg/kg body weight (CAF2)• 7 mg/kg body weight (CAF7)
• ↑ mean MPO in sub-elitecyclists was significantlyenhanced following caffeineingesFon in CAF7 treatment vsPLA (p = 0.05)
• No effect on elite cyclists!(Smolka et al, 2014)
Pla vs
CAF7
Fig. 7 Maximal power output during (MPO) experimental trials and statistical analysis of the experimental trials within sub-elite (n=10) and elite (n=8) groups (p)
CAF2 vs
CAF7
Pla vs
CAF2

Research Results RefuFng Point - 3Caffeine in Energy Drink
• The ingesFon of a caffeinatedenergy drink (Redbull) ↑ exerciseperformanceover a sweetenedflavoured water placebo
• The energy drink has vitamins B3,B5, B6, B12, taurine,glucuronolactone, andcarbohydrates. That creates manyconfounding variables
• ↑inblood glucose with ingesFonof the energy drink which leadtoan ↑ in Insulin inhibiFng lipolysis.
Fig. 8 PreD is blood glucose before ingestion of energy drink or placebo PreEcx is immediately before time trial *significant difference between trials (p<.05)
(Ivy et al, 2009)

RefuFng OpposiFon's Claims 1• Their argument: caffeine tolerance study is not an accurate representation of
performance as it used recreational athletes (Beaumont et al, 2016)
– Refute: elite & sub-elite level athletes compared after caffeine consumption • performance only enhanced in the sub-elite group and NOT the elite
(Smolka et al, 2014)
• Their argument: caffeine had no ergogenic effect due to ↑ dehydration (3.5% body mass) in caffeine group
Dehydration = ↓ work capacity & proper physiological function (Hunter et al, 2002)
– Refute: percent weight loss of subjects during the three trials were similar but greatest in Caf group (3.5 ± 1.8% Caf; 3.0 ± 1.7% Pl; 2.7 ± 1.5% Cho)
• Supports that caffeine has no ergogenic benefit
• Supports diuretic = ↓ performance (Passmore et al, 1987)

RefuFng OpposiFon's Claims 2SubstrateUFlizaFon
• Their argument: endurance performance is ↑ due to ↑ in serum FFA which spares muscleglycogen– refute: Davis et al, 2002 showed that the caffeine group had a ↓ liver glycogen
content , and Liverglycogen is a large cause of faFgue in prolonged exercise. Caffeinedid not affect liver and muscle glycogenolysis in the rats.• Casal and Leon, 1985 showed that in humans the RER doesnot change therefore
there is NO glycogen sparing in humans due to caffeine ingesFon.
(Casal and Leon, 1985)
Fig. 9

Conclusion
• Due to GI distress, dehydraFonandno change inRER
• Caffeine DOES NOT improveendurance sports performance.

References1. Beaumont, R., P. Cordery, M. Funnell, S. Mears, L. James, and P. Watson. Chronic ingesFon of a low dose of caffeine induces tolerance to the performance
benefits of caffeine. J. Sports Sci. 1-8, 2016.
2. Casal, D. L., and A. S. Leon. Failure of caffeine to affect substrate uFlizaFon changesduring prolonged running.Med. Sci. Sports Exerc. 17: 174-179, 1985.
3. Cornish,H. H., and A. A. Christman. A study of the metabolism of theobromine, theophylline, and caffeine in man. J. Biol. Chem. 228: 315-323, 1957.
4. Graham, T. E., J. W. Helge, B. Kiens, D. A. Maclean, and E. A. Richter. CaffeineingesFon does not alter carbohydrate or fat metabolism in human skeletalmuscle during exercise. J. Physiol. 529: 837-847, 2000.
5. Ivy, J. L., L. Kammer, Z. Ding, B. Wang, J. R. Bernard, Y. Liao, J. Hwang. Improved Cycling Time-Trial Performance awer IngesFon of a CaffeineEnergy Drink.Int. J. Sport Nutr. Exerc. Metab. 19: 61-78, 2009.
6. Kerrigan, S., and T. Lindsey.Fatal caffeine overdose: Two case reports. ForensicSci. Int. 153: 67-69, 2005.
7. Lohsiriwat, S., N. Puengna, and S. Leelakusolvong. Effect of caffeine on lower esophageal sphincter pressure in Thai healthy volunteers. Dis. Esophagus. 19:183-188, 2006.
8. Passmore, A. P., G. B. Kondowe, and G. D. Johnston. Renal and cardiovascular effects of caffeine: a dose-response study. Clin. Sci. 72: 749-756, 1987.
9. Smolka,O., and M. Kumstat. Caffeineintake enhances endurance performance in sub-elite but not in elite athletes. Ann. Kinesiol.5: 131-140, 2014.
10. Wilson, P. Dietary and non-dietary correlates of gastrointesFnal distress during the cycle and run of a triathlon. Eur. J. Sport Sci. 16: 448-454, 2016.
Extra References
Hunter, A. M., St, A., Gibson, C., Collins, M., Lambert, M., & Noakes,T. D. CaffeineingesFon does not alter performance during a 100-km cycling Fme-trialperformance. Int. J. Sport Nutr. Exerc. Metab. 12: 438-452, 2002.
Davis, J. M., Zhao, Z., Stock, H. S., Mehi, K., Buggy, J., and Hand, G. A. Central nervous system effects of caffeine and adenosine on faFgue. Am. J. Physiol.284: 399-404, 2003.








![An Efficient Spare-Line Replacement Scheme to Enhance NVM … · 2020-07-03 · NVM cells show huge endurance variation due to the variation of advanced process [6 ,15 19]. The endurance](https://img.dokumen.tips/doc/110x75/5f723d98639aea234e1e0cab/an-efficient-spare-line-replacement-scheme-to-enhance-nvm-2020-07-03-nvm-cells.jpg)




















