Embed Size (px)
Citation preview

This may be the author’s version of a work that was submitted/acceptedfor publication in the following source:
Buenzli, Pascal, Pivonka, Peter, Gardiner, Bruce, & Smith, David(2012)Modelling the anabolic response of bone using a cell population model.Journal of Theoretical Biology, 307, pp. 42-52.
This file was downloaded from: https://eprints.qut.edu.au/106759/
c© Consult author(s) regarding copyright matters
This work is covered by copyright. Unless the document is being made available under aCreative Commons Licence, you must assume that re-use is limited to personal use andthat permission from the copyright owner must be obtained for all other uses. If the docu-ment is available under a Creative Commons License (or other specified license) then referto the Licence for details of permitted re-use. It is a condition of access that users recog-nise and abide by the legal requirements associated with these rights. If you believe thatthis work infringes copyright please provide details by email to [email protected]
License: Creative Commons: Attribution-Noncommercial-No DerivativeWorks 2.5
Notice: Please note that this document may not be the Version of Record(i.e. published version) of the work. Author manuscript versions (as Sub-mitted for peer review or as Accepted for publication after peer review) canbe identified by an absence of publisher branding and/or typeset appear-ance. If there is any doubt, please refer to the published source.
https://doi.org/10.1016/j.jtbi.2012.04.019

Modelling the anabolic response of bone using a cell populationmodel
Pascal R. Buenzli1, Peter Pivonka, Bruce S. Gardiner, David W. SmithFaculty of Engineering, Computing & Mathematics,
The University of Western Australia, WA 6009, Australia
April 19, 2012
Abstract – To maintain bone mass during bone remodelling, coupling is required between bone resorptionand bone formation. This coordination is achieved by a network of autocrine and paracrine signalling moleculesbetween cells of the osteoclast lineage and cells of the osteoblastic lineage. Mathematical modelling of signallingbetween cells of both lineages can assist in the interpretation of experimental data, clarify signalling interactionsand help develop a deeper understanding of complex bone diseases. Several mathematical models of bonecell interactions have been developed, some including RANK–RANKL–OPG signalling between cells and systemicparathyroid hormone PTH. However, to our knowledge these models do not currently include key aspects of somemore recent biological evidence for anabolic responses. In this paper, we further develop a mathematical modelof bone cell interactions by Pivonka et al. (2008) [1] to include the proliferation of precursor osteoblasts into themodel. This inclusion is important to be able to account for Wnt signalling, believed to play an important role inanabolic responses of bone. We show that an increased rate of differentiation to precursor cells or an increasedrate of proliferation of precursor osteoblasts themselves both result in increased bone mass. However, modellingthese different processes separately enables the new model to represent recent experimental discoveries suchas the role of Wnt signalling in bone biology and the recruitment of osteoblast progenitor cells by transforminggrowth factor β. Finally, we illustrate the power of the new model’s capabilities by applying the model to prostatecancer metastasis to bone. In the bone microenvironment, prostate cancer cells are believed to release some ofthe same signalling molecules used to coordinate bone remodelling (i.e. Wnt and PTHrP), enabling the cancercells to disrupt normal signalling and coordination between bone cells. This disruption can lead to either bonegain or bone loss. We demonstrate that the new computational model developed here is capable of capturingsome key observations made on the evolution of the bone mass due to metastasis of prostate cancer to the bonemicroenvironment.
Key words: osteoblastogenesis, proliferation, Wnt signalling, prostate cancer metastasis, mathematical model
1 Introduction
Bone is a dynamic living tissue which continuously un-dergoes remodelling to ensure mineral homeostasis and torepair micro damage [2, 3]. The two main bone cell typesexecuting bone remodelling are osteoclasts which resorbthe mineralised bone matrix and osteoblasts which depositosteoid (which subsequently becomes mineralised) [3].The third cell type involved in bone remodelling are os-teocytes (i.e., terminally differentiated cells derived frommature osteoblasts that have been trapped in the miner-alised bone matrix [4]). The entire ensemble of bone cellscontributing to bone remodelling is referred to as basicmulticellular unit (BMU) [5,6].
Within the BMU, pre-osteoblasts, which express RANKL
have been hypothesised to control the differentiation ofosteoclasts from hematopoietic progenitors [7–10]. Thebone resorption phase is subsequently followed by boneformation, driven in part, by factors produced by theosteoclast that stimulate osteoblastogenesis [9]. This cou-pling between resorption and formation phase in BMUs isrequired to maintain bone mass. Many bone pathologies,such as osteoporosis, Paget’s disease and cancer metastasis
1Corresponding author. Email address:[email protected]
to bone, are associated with the dysregulation of this cou-pling process leading to abnormal bone loss or bone gain.Mathematical modelling can be employed to interpret ex-perimental data, clarify signalling interactions, investigatetherapeutic interventions, and to generally better under-stand bone remodelling from a systems perspective [11].
Bone remodelling has been represented mathematicallyin a variety of ways including bone cell population models(ODEs) [1,12,13], continuum models (PDEs) [14–16] anddiscrete cell models [17, 18]. The bone cell populationmodel by Lemaire et al. [13] proposes an interesting ap-proach based on fundamental chemical reaction principlessuch as material balance and mass action kinetics. Thismodel incorporates some of the most important bone bi-ology known at that time. Extensions to include furthercomponents of bone biology can be formulated using thesame framework. We have used this framework to includenew knowledge in bone biology in our bone cell populationmodel [1] (such as the expression of RANKL and OPG byosteoblasts of various maturities) [1], and to introducea spatial variation in cells numbers to represent a singlebasic multicellular unit [15]. We have also applied themodel by Pivonka et al. [1] to examine possible therapeuticinterventions to restore bone mass following dysregulationof the RANK–RANKL–OPG signalling system [19], coupled
1
arX
iv:1
112.
5685
v2 [
q-bi
o.T
O]
18
Apr
201
2

this model to a pharmacokinetic model of denosumab toexplore the effect of different dosing regimes [20], andstudied osteolytic lesions in multiple myeloma [21].
However, while the model by Pivonka et al. [1] doessome things well, it does not capture the anabolic effects ofprecursor osteoblast proliferation. Recent experimental ev-idence suggests that Wnt signalling is a critically importantregulator of bone remodelling—Wnt signalling plays an im-portant role in normal bone homeostasis under varying me-chanical loading, and excessive Wnt signalling is responsiblefor some osteopetrotic (excess) bone states [22,23]. In ad-dition, recent clinical evidence demonstrates that adminis-tration of intermittent PTH is an effective anabolic interven-tion [23, 24]. The exact molecular mechanisms leading toanabolic responses under intermittent PTH administrationare incompletely understood and probably multifactorial,involving differential regulations of osteoblast differentia-tion, proliferation and apoptosis [23]. While we do notmodel intermittent PTH administration in this paper, it isimportant to include these three cellular behaviours reg-ulating the number of osteoblasts for future investigations.In this paper, we thus further develop the model by Pivonkaet al [1] by introducing the proliferation of osteoblasts in away such that the new model is consistent with the originalmodel and can incorporate osteoblast proliferation throughWnt signalling or via other signalling systems. We thenexplore the effect of parameter changes in the new modelon net bone balance, and see that the new model is capableof effectively representing osteopetrotic bone disease statesarising from disruption of normal osteoblastic proliferation.
Finally we illustrate the capabilities of the new model ina complex bone disease that arises when prostate cancercells metastasise to the bone microenvironment. Thisdisease is characterised by a variable phenotype that ofteninvolves net bone gain (coupled with focal bone loss) [25–27], and finally net bone loss. We show that the new modeldeveloped here can model bone gain and bone loss viasecretion of signalling molecules such as Wnt, PSA and PTHrP
by the prostate cancer cells.
2 Background
A recent review by Khosla et al. highlights the importanceof osteoblast development in the regulation of bone re-modelling and the potential for therapeutic interventionsthat target the osteoblastic lineage [28]. Osteoblasts aremesenchymal cells derived from the mesoderm. Sequentialexpression of several molecules (such as RUNX2 and OSX),driven by signal transduction pathways, facilitates the dif-ferentiation of the progenitor cell into a proliferating pre-osteoblast, then into a bone matrix-producing osteoblast,and eventually into a mechanosensory osteocyte or a bone-lining cell (see Figure 1). As the cells of the osteoblasticlineage differentiate, they produce molecules essential forregulating BMU operation, including support of osteoclas-togenesis and angiogenesis in a BMU. Active osteoblastssecrete osteoid, which later mineralises to bone, whileosteocytes produce molecules that regulate BMU function.
The most extensively studied cell-kinetic model of os-teoblast development is that of mechanically induced bone
formation in experimental orthodontics [29–31]. Based onnuclear size, Roberts et al. [30] have characterised fourprecursor cell types to the functional osteoblast. This dif-ferentiation pathway has been confirmed (and refined) bymarker expression in vitro using functional assays [32,33].Asymmetrically-dividing mesenchymal stem cells recruitedto the BMU give rise to a population of osteoblast progeni-tors that are proliferating extensively (undergoing symmet-ric division). These osteoblast progenitors differentiate intopre-osteoblasts that undergo limited proliferation. Finally,pre-osteoblasts differentiate in turn into non-proliferativeactive osteoblasts [32].
Current bone biology literature identifies the centralrole played by the Wnt signalling pathway in regulatingosteoblast development (Figure 1). Wnts are a familyof over 20 secreted glycoproteins crucial for the develop-ment and homeostatic renewal of many tissues, includingbone [34]. Wnts stimulate canonical or non-canonicalsignalling pathways by binding a receptor complex con-sisting of LDL receptor-related protein 5 (LRP5) or LRP6
and one of ten Frizzled (Fz) molecules [35]. There are arange of soluble ‘decoy molecules’ secreted that regulateWnt signalling including sclerostin, Dkk1,2,3 and SFRP1,2,3.The canonical Wnt signalling pathway has been the mostextensively studied Wnt signalling pathway in osteoblasts.Wnt activation involves the stabilization of β-catenin (viainhibition of the GSK-3β, axin and APC complex), resultingin the translocation of β-catenin TCF/LEF to the cell nucleusand activation of various downstream transcription factorscritical for directing cell lineage and subsequent cell pro-liferation [36]. Wnt signalling has three major functionsin osteoblastic lineage cells: (i) dictating osteoblast spec-ification from osteo-/chondroprogenitors; (ii) stimulatingosteoblast proliferation; and (iii) enhancing osteoblast andosteocyte survival (Figure 1).
This brief overview of osteoblast development and theimportance of Wnt signalling highlights the complexity ofpotential bone cell interactions. A systems biology ap-proach to bone remodelling can help understand theseinterconnections and their importance for functional boneremodelling [11]. It is only recently that a few mathemati-cal models of interacting bone cells have been developed toexplore these fundamental aspects of the bone remodellingsequence.
In Lemaire et al. [13], a bone cell population model forbone remodelling is proposed and applied to the study ofbone diseases and therapeutic strategies. To restore bonemass following catabolic pathologies (such as due to estro-gen deficiency, vitamin D deficiency, and senescence), thegeneration of pre-osteoblasts by differentiation is shownby this model to be a powerful bone formative strategy.This occurs despite coupling of formation to resorptionthrough cells of osteoblastic lineage expressing RANKL,which binds to the RANK receptor of osteoclasts therebypromoting osteoclast activation and bone resorption. Thecomputational model of bone remodelling of Lemaire et al.has been refined by Pivonka et al. [1] who investigated theeffect of RANKL and OPG expression profiles on cells of theosteoblastic lineage.
The aim of this paper is to investigate the effects of dif-
2

Figure 1 – Osteoblast development and the Wnt signalling pathway. Canonical Wnt promotes the commitment of MSCs to the osteoblastic lineage,stimulates osteoblast proliferation and enhances osteoblast and osteocyte survival [28].
ferent developmental stages of osteoblasts on bone remod-elling. For this purpose, we include a transient-amplifying(i.e. proliferating) stage in the osteoblastic lineage in thebone cell population model of Pivonka et al. [1]. Themotivation for this inclusion is twofold:
1. It is known that the density of MSCs in bone marrowis very low, and though MSCs are recruited to the BMU
site by TGFβ [37], it is likely the models of Refs [1,13]rely on an unphysiological recruitment of a sufficientnumber of pre-osteoblasts for the stimulation of asustained formative response. The fast increase inosteoblast population required in a BMU remodellingevent is believed to involve proliferative cells (under-going symmetric cell division), i.e., so-called transient-amplifying osteoblast progenitors [38].
2. Hormones and cytokines regulate stages of osteoblastdevelopment differently. The transient-amplifyingstage of osteoblasts is known to be strongly depen-dent on various hormones, growth factors and othermolecules, such as Wnt, insulin-like growth factor(IGF), prostaglandin E2 (PGE2) and estrogen [38–40].The anabolic effect of intermittent PTH is believed tooperate through multifactorial regulation of osteoblastgeneration at several developmental stages [23]. Also,in some bone diseases, signalling by these hormonesand growth factors is disrupted, leading to an ab-normal population of osteoblasts and a subsequentimbalance of bone during remodelling. For thesereasons, a more accurate account of the transient-amplifying stage of osteoblasts is essential for therealistic modelling of such diseases.
However, we find that the inclusion of OBp proliferationproposed in this paper has to be treated with some careas it can lead both to an unstable dynamic system (notconverging to a steady state with finite cell densities) and topotentially unphysiological system behaviour, for examplean anabolic response to continuous PTH administration,which is experimentally known to be catabolic. Theseissues are addressed in detail in this paper.
3 Description of the model
For simplicity, osteoblast progenitors and pre-osteoblastsare pooled into a single proliferative cell type in ourmodel, which we call pre-osteoblast and denote by OBp.Three stages of osteoblast development and two stages ofosteoclast development are included in the cell populationmodel.
Osteoclasts. Pre-osteoclasts (OCps) represent circulatingcells of hematopoietic origin. Pre-osteoclasts are assumedto mature into active osteoclasts (OCas) upon activation oftheir RANK receptor by the ligand RANKL. Active osteoclastsare cells that resorb bone matrix at a rate kres assumedconstant (in volume per unit time). In the model, OCas areassumed to undergo apoptosis at a rate enhanced by thepresence of TGFβ [1, 9, 15]. Thus, osteoclast developmentcan be summed up schematically as:
OCpRANKL+−→ OCa
TGFβ+−→ ;. (1)
Osteoblasts. Uncommitted osteoblast progenitors (OBus)represent a pool of MSCs. These MSCs are assumed to com-mit to the osteoblastic lineage by becoming pre-osteoblasts(OBps) through activation of TGFβ signalling. In the model,OBps represent transient-amplifying osteoblast progenitorsand they are therefore assumed to proliferate. Theirmaturation into active osteoblasts (OBas) is assumed to bedownregulated by TGFβ. Active osteoblasts are cells thatform bone matrix at a rate kform assumed constant (involume per unit time). The fate of active osteoblasts iseither (i) to be buried in osteoid and become osteocytes;(ii) to undergo apoptosis; or (iii) to become bone-liningcells covering the surface of newly-formed bone. In ourmodel, the elimination of an OBa depletes the pool ofmatrix-synthesising cells and thereby includes all threepossibilities. Thus, osteoblast development can be summedup schematically as:
OBuTGFβ+−→ OBp
�
TGFβ−−→ OBa −→ ... (2)
Regulatory factors. System-level coupling between theosteoclasts and osteoblasts occurs because the concentra-tions of the coupling signalling molecules TGFβ and of
3

RANKL are themselves influenced by cellular actions. Thegrowth factor TGFβ is assumed to be stored in the bonematrix and released into the microenvironment in activeform by the resorbing OCas [9,37,41]. The ligand RANKL isassumed to be expressed on the surface of OBps. Howeverthis expression can be blocked by binding to OPG, whichin turn is assumed to be produced in soluble form byOBas [10, 42]. The generation of RANKL and of OPG byosteoblasts is respectively upregulated and downregulatedby the systemic hormone PTH.
Governing equations. The osteoclast and osteoblast de-velopment pathways (1)–(2) are transcribed mathemati-cally as so-called ‘rate equations’ involving OCp, OCa, OBu,OBp and OBa cell densities (number of cells per unit vol-ume) [1,15]:
∂
∂ tOCa = DOCp
OCp −AOCaOCa, (3)
∂
∂ tOBp = DOBu
OBu −DOBpOBp +POBp
OBp, (4)∂
∂ tOBa = DOBp
OBp −AOBaOBa, (5)
where
DOCp(t) = DOCp
πact�RANKL(t)/kRANKLOCp
�
, (6)
AOCa(t) = AOCa
πact�TGFβ(t)/kTGFβOCa
�
, (7)
DOBu(t) = DOBu
πact�TGFβ(t)/kTGFβOBu
�
, (8)
DOBp(t) = DOBp
πrep�TGFβ(t)/kTGFβOBp
�
. (9)
In Eqs (3)–(5), source and sink terms are specified accord-ing to transformation rates between cell types with firstorder reaction rates to account for the effect of populationsizes. DOCp
(t) is the differentiation rate of OCps intoOCas activated by RANKL, AOCa
(t) is the apoptosis rate ofOCas activated by TGFβ, DOBu
(t) is the differentiation rateof OBus into OBas activated by TGFβ, and DOBp
(t) is thedifferentiation rate of OBps into OBas repressed by TGFβ.The elimination rate of active osteoblasts,AOBa
, is assumedunregulated and constant: AOBa
(t) ≡ AOBa. Activation and
repression of these rates by RANKL or TGFβ is expressed inEqs. (6)–(9) in terms of the dimensionless functions
πact(ξ) =ξ
1+ ξ, πrep(ξ) = 1−πact(ξ) =
1
1+ ξ. (10)
These functional forms of πact and πrep are based on thefollowing assumptions. Ligands such as RANKL and TGFβ
modulate cell behaviours by binding to specific receptors onthe cells and triggering intracellular signalling pathways.Following Refs [1, 13, 15], we assume that the signalreceived by a cell corresponds to the fraction of occupiedreceptors on the cell. This fraction is equal to πact(L/k),where L is the extracellular ligand concentration and ka binding parameter (dissociation binding constant) [43].We do not model intracellular pathways explicitly butrelate a cell’s response to its input signal by assuminga phenomenological relationship. Here, we assume thata cell responds in proportion to receptor occupancy, i.e.either in proportion to πact (for activation) or to πrep
(for repression).1 Note that since receptor occupancy isa nonlinear function of the free ligand concentration, theoverall relationship between concentration of extracellularligand L and cell response in Eqs (6)–(9) is nonlinear.
The rate equations governing the concentrations of TGFβ,RANK, RANKL, OPG and PTH are solved under the approxima-tion that receptor–ligand binding reactions occur on a fasttimescale compared to cell responses. These equations arepresented in Appendix A.
The proliferation termPOBpOBp in Eq. (4) has been added
to the original system of equations of Ref. [1] to accountfor the transient-amplifying stage of osteoblasts. This terminvolves the proliferation rate POBp
(t), which is related to
the average cell cycle period of pre-osteoblasts, τmitosisOBp
, by
POBp(t) = ln(2)/τmitosis
OBp(t). The proliferation rate POBp
(t) iscontrolled by a feedback mechanism and is therefore timedependent (see Regulation of OBp proliferation below).
Finally, the matrix-resorptive activity of OCas and matrix-synthesising activity of OBas influence the overall amountof bone according to:
∂
∂ tBV =−kresOCa + kformOBa, (11)
where BV stands for the volume fraction of bone matrixin a representative volume element at the tissue scale.2
The quantity kresOCa represents the resorption rate (bonevolume fraction resorbed per unit time) and the quantitykformOBa represents the formation rate (bone volume frac-tion formed per unit time). All the parameter values of themodel are listed in Appendix B (Table 1).
The system of ODEs (3)–(5) together with Eqs. (27)–(31) form a closed system that can be solved for the timeevolution of the three state variables OBp, OBa and OCa froman initial condition. Eq. (11) can then be integrated toprovide the time evolution of the bone volume fraction.Clearly, BV(t) is not a function of the current state only asit depends on the integrated history of OCa(t) and OBa(t).However, the bone volume fraction change rate ∂
∂ tBV is a
function of the current state and will be a major modeloutput followed in this paper.
Regulation of OBp proliferation. In a single BMU, thou-sands of active osteoblasts refill the cavity created by theosteoclasts [3, 5]. Their continual recruitment from pre-osteoblasts occurs at a rate that varies with the rate ofresorption. For a BMU that advances in bone at 40 µm/day,an estimated rate of 120 active osteoblasts per day isnecessary to ensure that the whole perimeter of the BMU
cavity is covered by the bone refilling cells [3]. Thisrequired recruitment rate of active osteoblasts is achievedby a combination of differentiation from mesenchymalstem cells near the tip of the blood vessel, and proliferationof pre-osteoblasts between the blood vessel and cavitywalls [30, 32, 44]. Active osteoblasts in BMUs usually form
1Such a relationship has been shown to hold experimentally forexample in the context of human fibroblasts stimulated by epidermalgrowth factor (EGF): the mitogenic response of these fibroblasts is linearlydependent on the fraction of occupied EGF receptors [43, Fig. 6-7, p.249].
2The volume fraction of bone matrix is also equal to 1−Φ where Φ isthe ‘bone porosity’, i.e., the volume fraction of soft tissues (marrow, cells,stroma) (compare with Ref. [3, Eq. (3.7)]).
4

a single layer of cells [45], and so are limited in numberby the available bone surface area. It is likely that feedbackcontrol mechanisms regulate pre-osteoblast proliferation tolimit the generation of active osteoblasts. We model thiscontrol of cell population by limiting the proliferation rateof pre-osteoblasts with the density of pre-osteoblasts, i.e.:
POBp(t) =
POBp(t)�
1− OBp(t)
OBsatp
�
, if OBp(t)< OBsatp ,
0, if OBp(t)≥ OBsatp .
(12)
In Eq. (12), OBsatp is a critical density above which prolifera-
tion is entirely suppressed. The control of the proliferationrate by the density of OBps may represent ‘contact inhibi-tion’ or ‘pressure inhibition’ of proliferation and/or nutrientor space restrictions in the BMU cavity. It may representa feedback control from newly-formed active osteoblastsnear the reversal zone. Indeed, pre-osteoblasts representthe last stage of osteoblast development before maturationinto active osteoblasts. The density of pre-osteoblasts at agiven time used in Eq. (12) is thus approximately propor-tional to the density of newly-formed active osteoblasts.
In Eq. (12), the remaining factor POBp(t) stands for
additional negative and/or positive regulations of theproliferation of OBps as due to, e.g., Wnt signalling, PTH
administration, and other hormones and growth factorsthat may play a role in mechanosensing [4, 46] or in thedevelopment of osteoporosis, viz.
POBp(t)≡ POBp
(Wnt(t), PTH(t), estrogen(t), IGF(t), TGFβ(t), ...).(13)
Including all these regulations is beyond the scope of thepresent work, but provides a clear direction for futureresearch. Here we will assume that in normal bone home-ostasis, systemic levels of these signalling molecules leadto a specific value of POBp
and we will first investigate howPOBp
as a parameter affects the remodelling behaviour ofthe system. In Section 5, the model is applied to a complexdisease, and in this case, POBp
is made dependent on Wnt
produced by metastatic prostate cancer cells.We note that a time-dependent regulation of the pro-
liferation rate POBp(t) is essential to allow OBp cells to
(i) rapidly proliferate in early stages of osteoblastogene-sis (when the density of pre-osteoblasts is low) and (ii)reach a controlled steady state. Mathematically, a rapid,exponential-like increase in the OBp population may occurfrom Eq. (4) whenever POBp
(t)−DOBp(t) is positive and
does not decrease too fast in time.3 On the other hand,one sees from Eq. (4) that a necessary condition for theOBp population to stay bounded and to converge to ameaningful steady-state (with finite, positive cell densities)is that
POBp(t)−DOBp
(t)< 0, t →∞. (14)
The regulation of proliferation given in Eq. (12) enables usto fulfill both requirements (i) and (ii).
3The density of OBps at time t has a contribution proportional to
exp�
∫ t
0dt ′ (POBp
−DOBp)(t ′)
. This contribution increases faster thanany power law in time (exponential-like increase) provided that (POBp
−DOBp
)(t) is positive and does not decrease faster than or as fast as O(1/t).
Pre-osteoblasts generation: differentiation vs prolifera-tion. Differentiation from MSCs and proliferation of pre-osteoblasts are two different biological mechanisms thatenable the population of osteoblasts to reach the sizerequired in a BMU for functional remodelling. The relativeproportion of these two mechanisms in vivo has not beenquantified experimentally. Proliferation is a mechanismthat exponentially inflates any deviation in the originalpopulation size. Proliferation thus provides a sensitivecontrol of the population and the potential for a quickresponse. Of course if this is the dominant mechanismfor increasing the size of the OBp cell population, a smallchange in proliferation rate may lead to a very large changein the OBp cell population. We observe here that themore proliferation becomes dominant, the more difficult itbecomes for the final cell population to be well-controlled,as a small change in the rate of proliferation leads to a largechange in cell population. By contrast, differentiation ofMSCs is a mechanism that influences the initial populationof pre-osteoblasts. This provides a more stable mechanismfor controlling OBp cell population, but this has the poten-tial disadvantage of requiring the recruitment and mainte-nance of large numbers of MSCs. Clearly, if differentiationis large, then proliferation needs to be limited to reach thesame population size.
For these reasons, it is helpful in the model to introducethe relative proportion of OBu differentiation and OBp pro-liferation as a parameter. We introduce the fraction ν suchthat the generation of OBps in the steady state is achievedwith a fraction ν by OBp proliferation and with a fraction1−ν by OBu differentiation. Denoting steady-state valuesby an overline, the total generation rate of OBps in thesteady state is given by σOBp
= DOBuOBu + P OBp
OBp (seeEq. (4)). The first term represents the contribution of OBudifferentiation and should thus account for a fraction 1−νof σOBp
. The second term represents the contribution of OBpproliferation and should thus account for a fraction ν ofσOBp
. To determine the values of POBpand DOBu
that satisfythis, we impose
P OBpOBp = ν σOBp
, DOBuOBu = (1−ν) σOBp
, (15)
and use the fact that σOBp= DOBp
OBp in the steady state.With Eqs. (8),(9),(12), one then has from Eq. (15):
POBp(ν , OBsat
p ) = ν DOBpπrep
�
TGFβ
kTGFβOBp
��
1− OBp
OBsatp
�−1, (16)
DOBu(ν , OBsat
p ) = (1−ν) DOBp
πrep�
TGFβ
kTGFβOBp
�
πact�
TGFβ
kTGFβOBu
�
OBp
OBu. (17)
Therefore, provided that POBp= POBp
(ν , OBsatp ) and DOBu
=DOBu(ν , OBsat
p ) in Eqs. (12) and (8), the system reachesfor any value of ν a steady state characterised by thesame cell densities OBp, OBa and OCa and regulatory factorconcentrations TGFβ, RANKL, etc. as in Ref. [1] (despite theadditional proliferation term in Eq. (4)).4
The parameter ν enables us to investigate how the rela-tive occurrence of OBp proliferation vs OBu differentiation in
4For ν = 0, the model of Ref. [1] is retrieved, except for a correction inthe production rate of RANKL, see Appendix A.
5

osteoblastogenesis affects bone remodelling with a modelcalibrated against the same healthy-state properties. Tounderstand how a dysregulation of OBp proliferation affectsbone remodelling in an anabolic disease, we will set inSection 4
POBp= POBp
(ν , OBsatp ) +∆POBp
, (18)
DOBu= DOBu
(ν , OBsatp ), (19)
and study the effects of ν , OBsatp and of the proliferation
rate ‘offset’ ∆POBp(which accounts for dysregulation) on
the steady state of the system.
4 Properties of the model
The steady-state cell densities represented by the modelcorrespond to physiological cell densities (averaged at thetissue level) of a normal, healthy adult whose skeletonundergoes remodelling. While a baseline of mesenchy-mal stem cells and hematopoetic stem cells is implicitlyassumed, a bone remodelling event is not necessarily in-duced. Indeed, the system of ODEs (3)–(5) governingthe evolution of OBp(t), OBa(t), and OCa(t) always admitsvanishing bone cell densities as a solution, whatever thedensity of OBus and of OCps.
Specific signalling is required to commit these stem cellsto the osteoblastic and osteoclastic lineage. The inductionof a bone remodelling event appears to be a complicatedand poorly-understood process, that first requires bone lin-ing cells retracting from the bone surface, and is followedby the recruitment of osteoclasts on site. Our model isnot capable of modelling this induction process. However,the specific signalling between osteoblasts and osteoclastsmediated by RANKL and TGFβ forms a positive feedback loopthat leads any initial population of pre-osteoblasts or activeosteoclasts to a steady state characterised by positive celldensitites OBp, OBa, OCa [1,15].
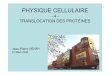
Anabolic potential of pre-osteoblast proliferation. Ourprevious investigations of the bone remodelling model ofRef. [1] have revealed that the RANK–RANKL–OPG pathwayis effective at inducing catabolic behaviour in response toan increase in the RANKL/OPG ratio, but not effective atinducing anabolic behaviour in response to a decrease inthe RANKL/OPG ratio [19]. By contrast, Figure 2 showsthat increasing POBp
from a normal state with steady bonevolume is very effective at inducing an anabolic behaviourof bone remodelling. But decreasing POBp
from this stateis not effective at inducing a catabolic behaviour of boneremodelling, even at high fractions ν .
The strong anabolic potential of pre-osteoblast prolifera-tion occurs despite pre-osteoblasts expressing RANKL, whichby binding to the RANK receptor of osteoclasts promotesosteoclast activation. This is similar to the bone formativetherapeutic strategy investigated by Lemaire et al. [13].In fact, the dynamics shows that active osteoclasts areonly transiently increased by an increase in pre-osteoblastdensity. The increase in OBps (which promotes osteoclasto-genesis by increasing RANKL signalling to OCps) is followedby a delayed increase in OBas. The latter cells produce
00.250.50.750.95
fractions Ν HProlif�differL:
0.00 0.02 0.04 0.06 0.08 0.10 0.12 0.14
0.00
0.05
0.10
0.15
0.20
OBp proliferation rate HPOBpL @1�dayD
Bon
evo
lum
ech
ange
rate
H¶ tB
VL@
%�da
yD
Figure 2 – Steady-state value of bone volume change rate (in percentvolume fraction/day) plotted against POBp
= POBp(ν , OBsat
p ) + ∆POBpfor
different fractions ν and a common value of OBsatp = 0.04 pM. Each curve’s
zero is marked by a dot and represent the value POBp(ν , OBsat
p ) at whichbone volume is steady (see Eq. (18)). The vertical dashed line representsthe upper bound POBp
(1, OBsatp ).
OPG, which binds competitively to RANKL. This reducesthe initial increase in RANKL signalling back to near-normallevels. Another limiting factor for osteoclastogenesis byRANKL signalling is the limited number of RANK receptorson OCps. The generation rate of active osteoclasts saturateswhen all RANK receptors on OCps are bound to RANKL.
It is noteworthy that the RANK–RANKL–OPG signallingpatway exhibits a pronounced ‘catabolic bias’ in the boneremodelling models developed by Lemaire et al. [13] andby Pivonka et al. [1, 19], while pre-osteoblast proliferationexhibit a “complementary” ‘anabolic bias’ in the presentmodel. We emphasise that depending on the individual,such biases may not be as pronounced in practice as themodels suggest. In the models, these biases can be partiallyexplained by the rapid saturation of the receptor–ligandbinding reaction rates (similarly to Michaelis–Menten en-zyme kinetics) that limit the cells’ response to extracellularligands (via the ‘activator’ and ‘repressor’ functions πact andπrep). As a consequence, cell behaviour is asymmetrical inresponse to an increase or to a decrease of extracellularligands. The strength of this asymmetry depends on whereon the curves πact and πrep the normal state is assumedto be. Normal ligand concentrations are likely to differacross indivuals. In some individuals, this normal ligandconcentration may lie closer to the initial linear part, orfinal saturated part of the functions πact, πrep than in otherindividuals, and in this way, lead to a less pronouncedasymmetry of the cell’s response.
Response to ‘continuous’ PTH administration. The in-clusion of OBp proliferation into the model introduces anadditional mechanism for osteoblastogenesis. The relativeimportance of this additional mechanism is represented bythe parameter ν introduced in Section 3. High fractions νemphasise proliferation, which makes the model sensitiveto small variations in the initial populations. Depending onthe value of ν , different system behaviours may arise, asillustrated in the following.
While an increase in pre-osteoblast proliferation isobserved to induce a strong anabolic response for a
6

broad range of fractions ν (Figure 2), the magnitude ofthe catabolic response to ‘continuous’ PTH administration(which increases the RANKL/OPG ratio), is strongly depen-dent on the choice of ν and OBsat
p . Figure 3 shows thesteady-state resorption and formation rates reached by themodel for four combinations of (ν , OBsat
p ) (Fig. 3(a)–(d))under two externally-driven influences:
(i) An altered value of the OBp proliferation rate parame-ter POBp
(blue curve).
(ii) A continuous administration of PTH at rate PextPTH
(seeEq. (31)) (red curves);
In Figure 3, the alteration of OBp proliferation may rep-resents an alteration in the Wnt pathway. Continuous PTH
administration increases the concentration of PTH and thusincreases the RANKL/OPG ratio (see Eqs. (28), (30)), whichpromotes osteoclastogenesis. It is well-known that con-tinuous PTH administration leads to a catabolic response.Strikingly, Figure 3(b) and (c) exhibit two examples of pairs(ν , OBsat
p ) that lead to an (as far as the authors are aware;unphysiological) anabolic behaviour in response to an in-crease in the RANKL/OPG ratio from the normal state. De-creasing OBsat
p and/or ν can restore the expected catabolicbehaviour. This is seen by comparing Figure 3(b)→(a)(decrease in OBsat
p ) and Figure 3(c)→(d) (decrease in ν).
The possibility for such unphysiological anabolic be-haviour is new compared to the models by Lemaire etal. [13] and Pivonka et al. [1]. However, this variabilitymay be advantageous, allowing the system to be adjustedto specific patients or patient groups responding differentlyto increased PTH. The anabolic or catabolic behaviour ofthe model in response to increased RANKL/OPG ratio canbe measured in Figure 3 by the angle that the PTH curvemakes with the diagonal (corresponding to BV homeostasis)at the point corresponding to the normal state. This angleis shown in Figure 3(c) as ‘α’ and is plotted against νand OBsat
p in Figure 4. Only the region corresponding tonegative angles (bottom-left region, in red, in Figure 4)corresponds to a catabolic response to increased PTH. Aphysiologic estimate of this angle constrains (ν , OBsat
p ) to beon the contour line corresponding to this angle in Figure 4,leaving one degree of freedom. To retrieve the samecatabolic behaviour to continuous PTH administration nearthe normal state for normal individuals as in Refs [1, 19],we choose this angle to be ≈ −4.5◦. We note, however,that the catabolic response to continuous PTH in the presentmodel is stronger at larger values of PTH administrationrates (not shown).
While continuous PTH administration (infusion) does notinduce an anabolic response, it is known that intermittentPTH administration (daily injections) does lead to an an-abolic response. This dual catabolic–anabolic mode of ac-tion of PTH remains poorly understood [23]. It is instructiveto understand within our model how an anabolic responseto continuous PTH administration is obtained in Figure 3(b)and (c). This anabolic response of the model occurs whenν or OBsat
p is large, i.e. when OBp proliferation is significant.Increasing PTH increases RANKL/OPG and promotes osteo-clastogenesis, which frees TGFβ in the microenvironment
and increases the OBp population. If OBp proliferationis significant, this increase in OBp is amplified stronglyand eventually overcomes PTH-induced osteoclastogenesis,which leads to an anabolic behaviour. As this behaviouris not observed in vivo for continuous PTH administration,it can be expected that the proliferative potential of pre-osteoblasts is normally limited to the negative angle regionin Figure 4. We estimate that the balance between OBu dif-ferentiation and OBp proliferation is probably somewherein the range 0.4 ® ν ® 0.6. This imposes a strong upperlimit to the parameter OBsat
p (see Figure 4). For an angle≈−4.5◦, one has OBsat
p ® 0.005 pM.Finally, we note that intermittent PTH administration may
exert an action on a variety of regulatory pathways of boneremodelling [23]. An overall anabolic response may beobtained as a combined effects of anabolic and catabolicdisruptions of bone remodelling. This is the case forexample of point D in Figure 3(a), where the superpositionof an upregulation of pre-osteoblast proliferation and acatabolic response to PTH administration still leads to anoverall anabolic response.
5 Application to prostate cancermetastasis
Many bone pathologies are due to an altered bone balanceand an altered bone turnover rate during remodelling.Bone imbalance is associated with under-refilling (boneloss) or over-refilling (bone gain) in BMUs. Bone turnoverrate is associated with the number of active BMUs andindicates how fast bone may be lost, gained, and/or turnedover. Our computational model represents bone remod-elling at the tissue scale, where BMU quantities are spatiallyaveraged. At this scale, bone imbalance and abnormalturnover rates are characterised by altered overall rates ofbone resorption kresOCa and bone formation kformOBa in therepresentative volume element [6].
Prostate cancer develops metastases primarily to trabec-ular bone of the pelvis, femur and vertebral bodies [47].Several regulatory factors produced by the metastasisingprostate cancer cells (PCa) interfere with the normal regula-tion of bone remodelling, leading to osteoblastic (anabolic)lesions with underlying osteolytic (catabolic) areas [25,48,49]. The molecules Wnt in particular, are believed to beparticularly important in establishing osteoblastogenesis inthese lesions [50]. Hall et al. [26] suggest that inhibitionof Wnt by Dkk1 at an early stage of PCa metastasis leadsto osteolytic lesions (due to expression of e.g. PTHrP orRANKL by the PCa cells). These lesions help the PCa cells toestablish in the bone microenvironment. At a later stage,PCa cells progressively increase the Wnt/Dkk1 ratio, resultingin an increased osteoblastic response. Prostate cancer cellsalso produce PSA, which cleaves PTHrP after amino acid23 [48, 49, 51, 52]. The cleaved form PTHrP[1–23] fails toactivate the PTH receptor on osteoblasts, but is thought topromote osteoblastogenesis [49].
The above time course of metastatic bone lesions canbe simulated in the model by prescribing an assumedtime course for the population of PCa cells and for their
7

(a) ν = 0.75, OBsatp = 0.005 pM (b) ν = 0.75, OBsat
p = 0.01 pM
0%�da
y0.02%
�day
-0.0
2%�da
y
normal
A
B
C
DE
OBp prolif.
RANKL�OPG
0.00 0.02 0.04 0.06 0.08 0.100.00
0.02
0.04
0.06
0.08
0.10
Form
atio
nra
teHk f
orm
OB
aL@
%�da
yD 0%�d
ay0.02%
�day
-0.0
2%�d
ay
normal
A
B
C
D
E
E'
0.00 0.02 0.04 0.06 0.08 0.100.00
0.02
0.04
0.06
0.08
0.10
(c) ν = 0.75, OBsatp = 0.03 pM (d) ν = 0.25, OBsat
p = 0.03 pM
0%�da
y0.02%
�day
-0.0
2%�da
y
normal
A
C
Α
0.00 0.02 0.04 0.06 0.08 0.100.00
0.02
0.04
0.06
0.08
0.10
Resorption rate HkresOCaL @%�dayD
Form
atio
nra
teHk f
orm
OB
aL@
%�da
yD
0%�da
y0.02%
�day
-0.0
2%�da
y
normal
A
BC
D
0.00 0.02 0.04 0.06 0.08 0.100.00
0.02
0.04
0.06
0.08
0.10
Resorption rate HkresOCaL @%�dayD
Figure 3 – Formation rate vs. resorption rate in the steady states obtained by varying OBp proliferation rates POBp(blue curve) and by varying RANKL/OPG
ratios (via continuous PTH administrations PextPTH
) (red curves). The various labelled points correspond to the following pairs (POBp, Pext
PTH): normal
≡�
POBp(ν , OBsat
p ), 0�
; A ≡ (0, 0); B ≡�
2POBp(ν , OBsat
p ), 0�
; C ≡�
POBp(ν , OBsat
p ), 400/day�
; and D ≡�
2POBp(ν , OBsat
p ), 200/day�
; Points E in (a), (b) and E’in (b) correspond to states with no bone gain nor loss, but higher turnover rate.
expression of regulatory factors. To simplify, we assumethat a PCa tumour implants itself in trabecular bone andlocally grows over a characteristic time τPCa to a maximumdensity PCamax:
PCa(t) = PCamax�1− exp(−t/τPCa)�
. (20)
The PCa cells are assumed to produce PTHrP at a constantrate βPTHrP, and PSA at a slowly increasing rate βPSA(t):
βPSA(t) = βmaxPSA
�
1− exp(−t/τPSA)�
, (21)
The production rate of Wnt, βWnt(t), is assumed low initially
(or inhibited by Dkk1), but increases at later times:
βWnt(t) = βmaxWnt
e(t−tWnt)/τWnt + βminWnt /β
maxWnt
e(t−tWnt)/τWnt + 1. (22)
In Eq. (22), βminWnt is the minimum production rate, βmax
Wnt isthe maximum production rate, tWnt is the time at which theproduction rate increases and τWnt measures the durationof that increase.
Both the catabolic influence of PTHrP and the anabolicinfluence of Wnt produced by the PCa cells are taken intoaccount in the bone remodelling model. Cleavage of PTHrP
by PSA is taken into account, but not a potential anabolic
8

Figure 4 – Angle between the continuous PTH administration responsecurve and the diagonal at the point corresponding to the normal state inFigure 3. Positive (negative) angles represent a response to increase inPTH directed towards anabolic (catabolic) states. The four situations (a)–(d) of Figures 3 are also represented. Only negative angles (red region)represent the physiologically expected catabolic response to continuousPTH administration. The grey region is not part of the allowable parameterspace as it corresponds to OBsat
p < OBp.
influence of PTHrP[1–23]. Binding properties of PTHrP onosteoblasts are assumed identical to those of wPTH, andso the concentration of PTHrP is added to that of PTH inEqs. (28),(30). The Wnt produced by the PCa cells isassumed to promote OBp proliferation according to:
POBp= POBp
(ν , OBsatp )h
1+αWntOBpπact�Wnt(t)/kWnt
OBp
�
i
. (23)
As for the regulatory factors of bone remodelling, weassume that the binding reactions involving PTHrP, PSA andWnt are fast. The concentration of these molecules quicklyreaches a quasi-steady state equal to the production ratedivided by the degradation rate [1, Eq. (25)]. We thushave:
PTHrP(t) =βPTHrP PCa(t)
DPTHrP + kPSAPTHrP
PSA(t)(24)
PSA(t) =βPSA(t)PCa(t)
DPSA
(25)
Wnt(t) =βWnt(t)PCa(t)
DWnt
, (26)
where DPTHrP, DPSA and DWnt are degradation rates. Table 2in Appendix B lists the parameter values associated toEqs. (20)–(26).
The time course of the concentrations PTHrP(t) andWnt(t) in the bone microenvironment, and their effect onthe local bone volume fraction, are shown in Figure 5. Ithas to be emphasised that BV(t) does not represent the timecourse of the whole skeleton, but rather the evolution of asmall part of trabecular bone within a tissue sample. Otherregions of the bone might follow the same trend but have
PCaHtL�PCamax
ΒPSAHtL� ΒPSAmax
ΒWntHtL� ΒWntmax
0 50 100 150 200 250 300 3500.0
0.2
0.4
0.6
0.8
1.0
PCa
quan
titie
sHno
rmal
ised
L
PTHrP
PTH
0 50 100 150 200 250 300 3500
1
2
3
4
5
6
PTH
rP&
PTH
@pM
D
PSA
Wnt
0 50 100 150 200 250 300 3500
5
10
15
20
25
Wnt
&PS
A@p
MD
0 50 100 150 200 250 300 35098
100
102
104
106
t @daysD
BV
@%D
Figure 5 – Time courses of prostate-cancer-induced PTHrP(t), PSA(t) andWnt(t), and their effect on the local bone volume fraction. The assumedevolution of the tumour and the rate of PSA and Wnt expression per PCacell is seen in the topmost plot. The metastatic lesions transition fromosteolytic to osteoblastic due to Wnt upregulating OBp proliferation.
a different time course. This hypothesis is supported byhistological evidence by Roudier et al. [27] in patients whodied with multiple bone metastases. This study shows thatboth regions of osteolytic lesions and regions of osteoblasticlesions are often found in the same individual.
9

0%�da
y0.02%
�day
-0.0
2%�da
y
Ν=0.5
OBpsat=0.005 pM
normal
PCa
PCa evolution
0.00 0.02 0.04 0.06 0.08 0.100.00
0.02
0.04
0.06
0.08
0.10
Resorption rate HkresOCaL @%�dayD
Form
atio
nra
teHk f
orm
OB
aL@
%�da
yD
Figure 6 – Simulated resorption rate and formation rate due to prostatecancer metastases to a tissue-scale portion of trabecular bone (blue line).The dots on the line mark the elapsed weeks. The metastatic lesiontransitions from osteolytic to osteoblastic with increased turnover.
The joint evolution of the resorption rate and formationrate of this simulated disease are displayed in Figure 6. Onesees that while the cancer develops osteoblastic lesions,turnover rate is higher than normal, and so resorption rateis also higher than normal. This is also consistent with thedescription by Clarke and Fleisch [25] of prostate cancerlesions to bone being often a combination of both an in-crease in resorption and in formation at a same site. Here,we have driven the transition between osteolytic lesionsand osteoblastic lesions by an increase in Wnt productionaround tWnt. While several other factors are known toinfluence the co-evolution of prostate cancer metastasesand bone lesions, this sequence of events may alreadycapture an aspect of metastatic lesions to bone, namely,that the interference of cancer-cell-produced cytokines withthe normal biochemistry of bone remodelling can disruptnormal remodelling signals and drive it to either catabolicand anabolic imbalances.
6 Conclusions
Recent experimental evidence suggests that osteoblast pro-liferation plays an important role in the regulation ofbone remodelling. In this paper, we have developed anovel computational model of bone cell interactions thatincludes osteoblast proliferation. This model takes intoaccount a catabolic regulatory mechanism of bone remod-elling, mediated by the RANK–RANKL–OPG pathway, and anew anabolic regulatory mechanism of bone remodelling,driven by osteoblast proliferation. From our numericalsimulations the following observations have been made:
• Preosteoblast proliferation has the potential for astrong anabolic bone response. Such a response couldbe mediated by a variety of signalling molecules in-cluding Wnt. The strong anabolic response of prolif-
eration complements the strong catabolic response ofRANKL observed in our model;
• To obtain physiologically meaningful results and amanageable control of osteoblastogenesis, a balancebetween osteoblast differentiation and proliferation isessential, as well as a feedback regulation of prolifer-ation. This feedback regulation probably originates inthe limited spatial and metabolic resources within theconfines of the BMU;
• Combining different strengths of pre-osteoblast prolif-eration with continuous PTH administration broadensthe range of physiological bone responses that themodel can represent. This may enable a better repre-sentation by the model of variability in the physiologyof individuals.
• The example of prostate cancer metastasis to boneshows that the proposed catabolic and anabolic regu-latory mechanisms of the model are able to simulatethe progression of a complex bone disease rangingfrom catabolic to anabolic bone responses.
The numerical results indicate that the new model isimproved and able to capture essential features of boneremodelling. Nevertheless, several aspects of the modelcan be further improved. In particular the phenomeno-logical description of Wnt regulation of osteoblast prolifer-ation could include biochemical binding reactions betweendifferent molecules regulating the binding properties ofWnt to its receptor LRP5/6, such as sclerostin and Dkk1.Most interestingly, the variability of the bone responseto a combination of continuous PTH administration andperturbation of osteoblast proliferation suggests that futuredevelopments of the model could shed light on the mech-anisms underlying the difference between continuous PTH
administration and intermittent PTH administration.
Appendix A Rate equations of theregulatory factors
The regulatory factor concentrations are governed by masskinetics rate equations. Ligand–receptor binding reactionsoccur on a time scale much faster than the characteristictimes of cellular response (such as differentiation, apop-tosis). The rate equations for the regulatory factors cantherefore be taken in their steady state (see Refs. [1, 15]
10

for details). This gives:
TGFβ(t) =�
PextTGFβ(t) + nbone
TGFβkresOCa(t)
�
/DTGFβ (27)
RANKL(t) =Pext
RANKL(t) + β RANKL
OBpOBp(t)
1+ kRANKLRANK
RANK+ kRANKLOPG
OPG(t)
ר
DRANKL +β RANKL
OBpOBp(t)
N RANKLOBp
OBp(t)πact�
PTH(t)/kPTHOB,act
�
«−1
(28)
RANK = N RANKOCp
OCp, (29)
OPG(t) =Pext
OPG(t) + βOPG
OBaOBa(t)πrep�PTH(t)/kPTH
OB,rep
�
βOPGOBa
OBa(t)πrep�
PTH(t)/kPTHOB,rep
�
/OPGsat + DOPG
(30)
PTH(t) =�
PextPTH(t) + βPTH
�
/DPTH (31)
In these equations, external production rates PextL (t) rep-
resent external sources (or sinks) of the protein L and areassumed given. We provide in Table 1 the description andvalues of the parameters of the model.
A slight change in the expression for RANKL in Eq. (28)has been made compared to Ref. [1]. The production ofRANKL is now correctly proportional to the number of cellsthat express RANKL. We have replaced βRANKL in Ref. [1, Eq.(36)] by β RANKL
OBpOBp(t).5 To ensure that the normal steady
state is unchanged by this correction, we take β RANKLOBp
=βRANKL/OBp. We note that the same inconsistency of havinga production rate of RANKL not scaled by the number ofosteoblasts is present in Ref. [13]. While many behavioursof the model are marginally affected by this correction,some inconsistent behaviours have been corrected. Inparticular, increasing the number of pre-osteoblasts in ourmodel now increases the total number of RANKL (boundand unbound) accordingly, and transiently increases thenumber of active osteoclasts (until OPG, produced by OBas,inhibits RANKL-activation of RANK). Previously, a decreasein the number of active osteoclasts was observed in thissituation.
Appendix B Model parameters
The parameters of the bone remodelling model are listedin Table 1. The additional parameters introduced for theexample of prostate cancer metastasis are listed in Table 2.
5We assume Model Structure 2 of Ref. [1], in which RANKL is onlyexpressed by OBps and OPG is only expressed by OBas.
11

Table 1 – Model parameters
Symbol Value Description
OCp 1 · 10−3 pM pre-osteoclast densityOCa 1 · 10−4 pM steady-state density of active osteoclatsOBu 1 · 10−3 pM uncommitted osteoblast progenitors (MSC) densityOBp 1 · 10−3 pM steady-state density of pre-osteoblastsOBa 5 · 10−4 pM steady-state density of active osteoblatsnbone
TGFβ1 · 10−2 pM density of TGFβ stored in the bone matrix
kres 200 pM−1day−1 daily volume of bone matrix resorbed per osteoclastkform 40 pM−1day−1 daily volume of bone matrix formed per osteoblast
DOCp2.1/day OCp→ OCa differentiation rate parameter
AOCa5.65/day OCa apoptosis rate parameter
DOBu0.7/day OBu→ OBp differentiation rate parameter, value for ν = 0.5; Eq. (19)
DOBp0.166/day OBp→ OBa differentiation rate parameter
POBp0.054/day OBp proliferation rate parameter, value for ν = 0.5; Eq. (18)
AOBa0.211/day OBa apoptosis rate
kRANKLOCp
16.65 pM parameter for RANKL binding on OCp
kTGFβOCa
5.63 · 10−4 pM parameter for TGFβ binding on OCa
kTGFβOBu
5.63 · 10−4 pM parameter for TGFβ binding on OBu
kTGFβOBp
1.75 · 10−4 pM parameter for TGFβ binding on OBp
kPTHOB,act 150 pM parameter for PTH binding on OB (for πact)
kPTHOB,rep 0.222 pM parameter for PTH binding on OB (for πrep)
kRANKLRANK
0.034/pM association binding constant for RANKL and RANK
kRANKLOPG
0.001/pM association binding constant for RANKL and OPG
β RANKLOBp
1.68 · 105/day production rate of RANKL per OBp
β OPGOBa
1.63 · 108/day production rate of OPG per OBa
βPTH 250pM/day production rate of systemic PTH
N RANKLOBp
2.7 · 106 maximum number of RANKL per OBp
N RANKOCp
1 · 104 number of RANK receptors per OCp
OPGsat 2 · 108 pM OPG density at which endogeneous production stopsnbone
TGFβ0.01pM density of TGFβ stored in the bone matrix
DTGFβ 2/day degradation rate of TGFβ
DRANKL 10/day degradation rate of RANKL
DOPG 0.35/day degradation rate of OPG
DPTH 86/day degradation rate of PTH
ν 0.5 fraction of OBp proliferation over OBu differentiation involved in the steady-statedensity OBp
OBsatp 0.005 pM OBp density at which proliferation stops
Table 2 – PCa-specific parameters
Symbol Value Description
PCamax 5 · 10−3 pM maximum PCa density
τPCa 10 days duration of local PCa growthτPSA 200 days duration of increase in PSA productionτWnt 50 days duration of increase in Wnt production
tWnt 200 days time of increase in Wnt production
βPTHrP 2 · 105/day production rate of PTHrP per PCa
βmaxPSA
1 · 104/day final production rate of PSA per PCa
βminWnt
5 · 102/day minimum production rate of Wnt per PCa
βmaxWnt
1 · 104/day maximum production rate of Wnt per PCa
DPTHrP 86/day degradation rate of PTHrP
DPSA 4/day degradation rate of PSA
DWnt 2/day degradation rate of Wnt
kPSAPTHrP
60 pM−1day−1 parameter for PSA cleaving PTHrP
kWntOBp
2 pM parameter for Wnt binding on OBp
αWntOBp
2 amplification factor of PCa-induced OBp proliferation
12

References
[1] Pivonka P, Zimak J, Smith DW, Gardiner BS, Dunstan CR,Sims NA, Martin TJ and Mundy GR (2008). Model structureand the control of bone remodeling: A theoretical study.Bone 43:249
[2] Parfitt AM (2002). Targeted and nontargeted bone remod-eling: relationship to basic multicellular unit originationand progression. Bone 30:5
[3] Martin RB, Burr DB and Sharkey NA (1998). Skeletal TissueMechanics (New York: Springer)
[4] Bonewald LF and Johnson ML (2008). Osteocytes,mechanosensing and Wnt signaling. Bone 42:606
[5] Parfitt AM (1994). Osteonal and hemi-osteonal remodeling:The spatial and temporal framework for signal traffic inadult human bone, J. Cell. Biochem. 55:273–286
[6] Parfitt AM (1983). The physiological and clinical signifi-cance of bone histomorphometric data. In Recker RR (Ed.),Bone histomorphometry: Techniques and interpretation. CRCPress, Boca Raton, pp. 143–223.
[7] Ma YL, Cain RL, Halladay DL, Yang X, Zeng Q, Miles RR,Chandrasekhar S, Martin TJ, Onyia JE (2001). Cataboliceffects of continuous human PTH (1–38) in vivo is associ-ated with sustained stimulation of RANKL and inhibitionof osteoprotegerin and gene-associated bone formation.Endocrinology 142:4047–4054
[8] Martin TJ (2004). Paracrine regulation of osteoclast forma-tion and activity: Milestones in discovery. J. Musculoskel.Neuron. Interact. 4:243–253
[9] Roodman G D (1999). Cell biology of the osteoclast. Exp.Hematology 27:1229–1241
[10] Gori F, Hofbauer L C, Dunstan C R, Spelsberg T C, KholsaS and Riggs B L (2000). The expression of osteoprotegerinand RANK ligand and the support of osteoclast formationby stromal-osteoblast lineage cells is developmentally reg-ulated. Endocrinology 141:4768–4776
[11] Pivonka P and Komarova SV (2010). Mathematical model-ing in bone biology: From intracellular signalling to tissuemechanics. Bone 47:181–189
[12] Komarova S V, Smith R J, Dixon S J, Sims S M and WahlL M (2003). Mathematical model predicts a critical rolefor osteoclast autocrine regulation in the control of boneremodeling. J. Theor. Biol. 229:293–309
[13] Lemaire V, Tobin FL, Greller LD, Cho CR, Suva LJ (2004).Modeling the interactions between osteoblast and osteo-clast activities in bone remodeling. J. Theor. Biol. 229:293–309
[14] Ryser M D, Nigam N and Komarova S V (2009). Mathemat-ical modeling of spatio-temporal dynamics of a single bonemulticellular unit. J. Bone Miner. Res. 24:860–870
[15] Buenzli PR, Pivonka P, Smith DW (2011). Spatio-temporalstructure of cell distribution in Bone Multicellular Units: Amathematical model. Bone 48:918–926
[16] Ji B, Genever PG, Patton RJ, Putra D and Fagan MJ (2012)A novel mathematical model of bone remodelling cyclesfor trabecular bone at the cellular level. In press. Biomech.Model. Mechanobiol. DOI: 10.1007/s10237-011-0366-3
[17] van Oers R F M, Ruimerman R, Tanck E, Hilbers P A J andHuiskes R (2008). A unified theory for osteonal and hemi-osteonal remodeling. Bone 42:250–259
[18] Buenzli PR, Jeon J, Pivonka P, Smith DW, Cummings PT(2012). Investigation of bone resorption within a corticalbasic multicellular unit using a lattice-based computationalmodel, Bone 50:378–389
[19] Pivonka P, Zimak J, Smith DW, Gardiner BS, Dunstan CR,Sims NA, Martin TJ and Mundy GR (2010). Theoreticalinvestigation of the role of the RANK–RANKL–OPG system inbone remodeling. J. Theor. Biol. 262:306–316
[20] Scheiner S, Pivonka P, Smith DW, Dunstan CR (2011)Mathematical modeling of the pathophysiology of post-menopausal osteoporosis and treatment by the anti-catabolic drug denosumab. Preprint.
[21] Wang Y, Pivonka P, Buenzli PR and Smith DW (2011). PLoSOne 6:e27494, pp 1–21
[22] Henriksen K, Neutzsky-Wulff AV, Bonewald LF and KarsdalMA (2009). Local communication on and within bonecontrols bone remodeling. Bone 44:1026–1033
[23] Jilka RL (2007). Molecular and cellular mechanisms of theanabolic effect of intermittent PTH. Bone 40:1434–1446
[24] Hodsman AB, Bauer DC, Dempster DW, Dian L, Hanley DA,Harris ST, Kendler DL, McClung MR, Miller PD, OlszynskiWP, Orwoll E, and Yuen CK (2005). Parathyroid hormoneand teriparatide for the treatment of osteoporosis: A reviewof the evidence and suggested guidelines for its use. Endocr.Rev. 26:688–703
[25] Clarke NW and Fleisch HA (2008). The biology of bonemetastases from prostate cancer and the role of bisphos-phonates. In Ablin RJ and Mason MD (Eds.), Metastasis ofprostate cancer, Springer, pp. 253–281
[26] Hall ChL, Kang S, MacDougald OA, Keller ET (2006). Therole of Wnt in prostate cancer bone metastases. J. Cell.Biochem. 97:661–672
[27] Roudier MP, Morrissey C, True LD, Higano CS, Vessella RLand Ott SM (2008). Histopathologic assessment of prostatecancer bone “osteoblastic” metastases. J. Urol. 180:1154–1160
[28] Khosla S, Westendorf JJ, Oursler MJ (2008). Building boneto reverse osteoporosis and repair fractures. J. Clin. Invest118:421–428
[29] Kimmel DB and Jee WSS (1980). Bone cell kinetics duringlongitudinal bone growth in the rat. Calcif. Tissue Int.32:123–133
[30] Roberts WE, Mozsary PG and Klinger E (1982). Nuclear sizeas a cell-kinetic marker for osteoblast differentiation. Am. J.Anat. 165:373–384
[31] McCulloch CAG and Melcher AH (1983). Cell density andcell generation in the periondontal ligament of mice. Am. J.Anat. 167:43–58
[32] Aubin JE. (2008). Mesenchymal stem cells and osteoblastdifferentiation. In Bilezikian JP, Raisz LG and Martin TJ(Eds), Principles of bone biology, volume 1, pages 85–107.Academic Press, San Diego, 3 edition.
[33] Liu F, Malaval L and Aubin JE (2003). Global amplifica-tion polymerase chain reaction reveals novel transitionalstages during osteoprogenitor differentiation. J. Cell Sci.116:1787–1796
[34] Fuerer Ch, Nusse R and ten Berge D (2006), EMBO Rep9:134
[35] Uitterlinden AG et al. (2004). Am. J. Human Genetics75:1032
[36] Krishnan V, Bryant HU and MacDougald OA (2006). Reg-ulation of bone mass by Wnt signalling. J. Clin. Invest.116:1202–1209
[37] Tang Y et al. (2009). TGFβ1-induced migration of bonemesenchymal stem cells couples bone resorption with for-mation. Nat. Med. 15:757–766
[38] Manolagas SC, Kousteni K and Jilka RL (2002). Sex steroidsand bone. Recent Progress in Hormone Research 57:385–409
13

[39] Di Gregorio GB, Yamamoto M, Ali AA, Abe E, Roberson P,Manolagas SC, Jilka RL, Attenuation of the self-renewalof transit-amplifying osteoblast progenitors in the murinebone marrow by 17β-estradiol, The Journal of ClinicalInvestigation 107:803–812
[40] Ogita M, Rached MT, Dworakowski E, Bilezikian JP,Kousteni S (2008). Differentiation and proliferation of pe-riosteal osteoblasts progenitors are differentially regulatedby estrogens and intermittent parathyroid hormone admin-istration. Endocrinol. 149:5713–5723
[41] Iqbal J, Sun L and Zaidi M (2009). Coupling bone degrada-tion to formation. Nat. Med. 15:729–731
[42] Thomas GP, Baker SU, Eisman JA and Gardiner EM (2001).Changing RANKL/OPG mRNA expression in differentiatingmurine primary osteoblasts. J. Endocrinol. 170:451–460
[43] Lauffenburger DA and Linderman JJ (1993). Receptors:models for binding, trafficking, and signaling. (New York:Oxford Univ. Press)
[44] Jaworski Z F G and Hooper C (1980). Study of cell kineticswithin evolving secondary haversian systems. J. Anat. Lon-don 131:91–102
[45] Marotti G, Zambonin Zalone A and Ledda M. Number,size and arrangement of osteoblasts in osteons at differentstages of formation. Calcif. Tissue Int. 21:96–101.
[46] Scheiner S, Pivonka P, Hellmich C and Smith DW (2011).Computational simulation of bone remodeling by meansof a coupled systems biology-micromechanical approach.Preprint.
[47] Bubendorf L, Schöpfer A, Wagner U, Sauter G, Moch H,Willi N, Gasser ThC and Mihatsch MJ (2000). Metastaticpattern of prostate cancer: An autopsy study of 1589patients. Human pathology 31:578–583
[48] Keller ET, Zhang J, Cooper CR, Smith PC, McCauley LK,Pienta KJ and Taichman RS (2001) Prostate carcinomaskeletal metastases: Cross-talk between tumor and bone.Cancer and Metastasis Reviews 20:333–349.
[49] Chirgwin JM and Guise ThA (2003) Cancer metastasis tobone. Science & Medecine 9:140–151.
[50] Hall ChL, Bafico A, Dai J, Aaronson SA, Keller ET (2006).Prostate cancer cells promote osteoblastic bone metastasesthrough Wnts. Cancer Res. 65:7554–7560
[51] Cramer SD, Chen Z and Peehl DM (1996) Prostate specificantigen cleaves parathyroid homrone-related protein in thePTH-like domain: Inactivation of PTHrP-stimulated cAMPaccumulation in mouse osteoblasts. J. Urol. 156:526–531
[52] Logothetis ChJ, Lin S-H (2005). Osteoblasts in prostatecancer metastasis to bone. Nat. Rev. Cancer 5:21–28
14