Embed Size (px)
Citation preview

BY ORDER OF THE
SECRETARY OF THE AIR FORCE
AIR FORCE PAMPHLET 11-419
17 OCTOBER 2014
Operations
G AWARENESS FOR AIRCREW
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
ACCESSIBILITY: Publications and forms are available on the e-Publishing website at
www.e-Publishing.af.mil for downloading or ordering.
RELEASABILITY: There are no releasability restrictions on this publication.
OPR: AETC/A3FM
Supersedes: AFPAM11-419,
1 December 1999
Certified by: AF/A3O
(Brig Gen Giovanni K. Tuck)
Pages: 35
This pamphlet implements AFPD 11-4, Aviation Service, and AFI 11-404, Centrifuge Training
for High-G Aircrew. It provides all high-G aircrew with a source of reference for information
and techniques and covers basic physiology of high-G flight. It explains how to prevent G-
induced loss of consciousness (GLOC), describes the effects of G-forces on the body, the factors
that increase and decrease G-tolerance, and countermeasures to avoid GLOC. This publication
applies to all units assigned to or gained by major commands (MAJCOM) and HQ USAF direct
reporting units (DRU) that fly high-g aircraft and applies to high g aircrew. It also applies to the
Air Force Reserve Command (AFRC) and the Air National Guard (ANG). MAJCOMs, DRUs
and field operating agencies (FOA) may supplement this instruction. MAJCOMs, DRUs and
FOAs will coordinate their supplement to this instruction with AETC/A3FM before publication
and forward one copy to AETC/A3FM after publication. Supplements will not lessen the
requirements nor change the basic content or intent of this instruction. Refer recommended
changes and questions about this publication to the Office of Primary Responsibility (OPR)
using the AF Form 847, Recommendation for Change of Publication; route AF Form 847s from
the field through the appropriate functional chain of command. Ensure that all records created as
a result of processes prescribed in this publication are maintained in accordance with Air Force
Manual (AFMAN) 33-363, Management of Records, and disposed of in accordance with the Air
Force Records Disposition Schedule (RDS) located in the Air Force Records Information
Management System (AFRIMS). There are no requirements in this publication that may require
a waiver and no waivers will be considered.

2 AFPAM11-419 17 OCTOBER 2014
SUMMARY OF CHANGES
This document is substantially revised and must be completely reviewed. Updated
information includes new G protection technology and applications to 5th
generation fighter
aircraft. The publication format has been updated and OPR has been changed in accordance with
directives resulting from the establishment of AETC as Lead Command for the Aerospace
Physiology Training Program.
Chapter 1—PHYSICS AND PHYSIOLOGY 4
1.1. Introduction. ........................................................................................................... 4
Figure 1.1. Gravitational Axes. ................................................................................................ 4
1.2. Mishap Trends. ...................................................................................................... 4
1.3. Effects of G Stress. ................................................................................................ 5
1.4. GLOC. .................................................................................................................... 6
1.5. Physical Conditioning. ........................................................................................... 7
Chapter 2—PROTECTIVE MEASURES 9
2.1. G-Tolerance Factors. ............................................................................................. 9
2.2. Resting Tolerance. ................................................................................................. 9
2.3. Mission Preparation. .............................................................................................. 9
2.4. AGSM. ................................................................................................................... 9
2.5. G-Protection Equipment. ....................................................................................... 14
2.6. G Awareness. ......................................................................................................... 16
Chapter 3—OPTIMIZING HIGH-G MISSION PREPARATION 17
3.1. Physical Characteristics. ........................................................................................ 17
3.2. G Awareness Program History. ............................................................................. 17
3.3. Physical Conditioning. ........................................................................................... 17
3.4. Other Human Factors Affecting Our Ability to Tolerate G Stress. ....................... 20
3.5. Mission Assessment and Planning. ........................................................................ 21
3.6. Pre-flight. ............................................................................................................... 21
3.7. In-flight. ................................................................................................................. 22
3.8. Effective integration of G awareness concepts will decrease the risk of GLOC for
aircrew. .................................................................................................................. 23
Attachment 1—GLOSSARY OF REFERENCES AND SUPPORTING INFORMATION 24
Attachment 2—PHYSICAL FITNESS PROGRAM TO ENHANCE AIRCREW G-
TOLERANCE 27

AFPAM11-419 17 OCTOBER 2014 3
Attachment 3—SAMPLE WORKOUT PLANS 32

4 AFPAM11-419 17 OCTOBER 2014
Chapter 1
PHYSICS AND PHYSIOLOGY
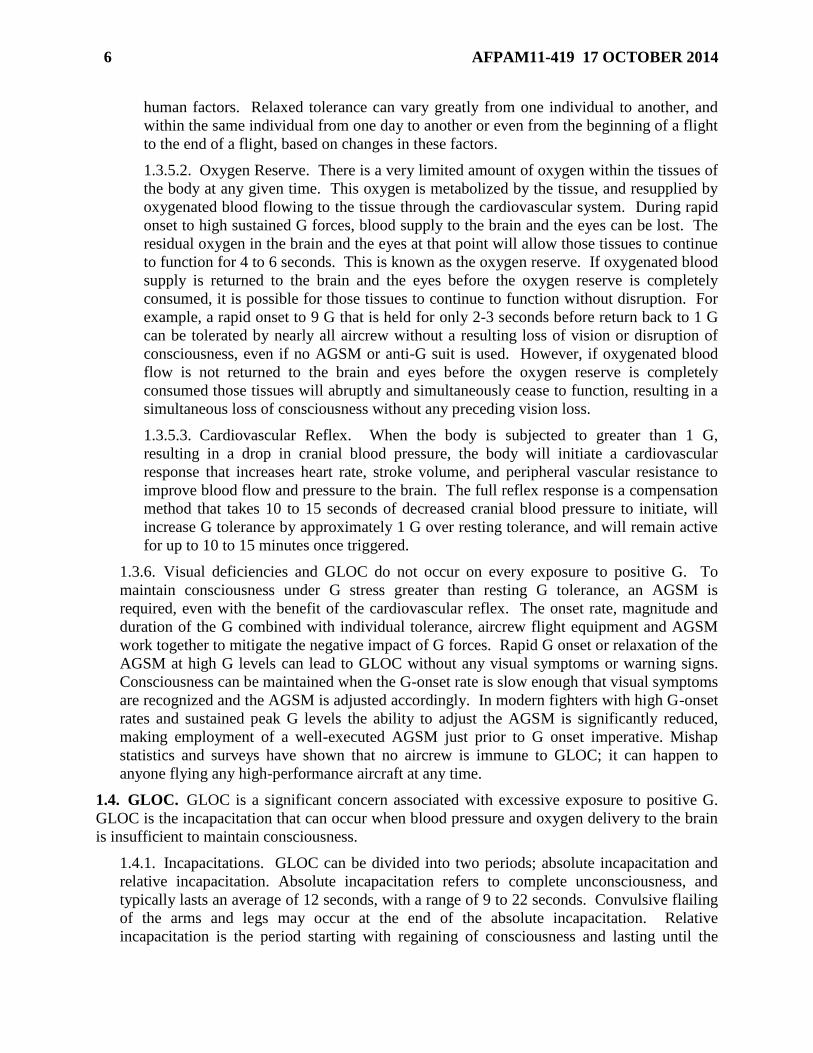
1.1. Introduction. High-G aircrew routinely experience changes in gravitational force,
abbreviated as “G,” as a result of inertial forces generated during flight. These changes in G can
be either negative (-G) or positive (+G) and will typically have direction along a specific axis--
x, y, or z. See figure 1.1 for an illustration of the three G axes. During high-G flight, G forces
can be several times greater than that of level flight. Positive changes of G along the z axis
(+Gz), or head-to-foot, can be especially challenging for aircrew. Therefore, it is imperative that
aircrew of high-G aircraft be equipped with the education, training and equipment necessary to
mitigate the risk associated with routine exposure to +Gz. For clarity, this document refers to Gz
when referencing “G.”
Figure 1.1. Gravitational Axes.
1.2. Mishap Trends. G forces continue to be a significant threat in fighter aviation. Safety data
shows that 157 G-related mishaps occurred between FY01 and FY11 with five Class As and
three fatalities costing $86.2M. Failure to understand and implement G awareness will result in
the continued average of 12 G-related mishaps per year.

AFPAM11-419 17 OCTOBER 2014 5
1.3. Effects of G Stress. An understanding of the basic physiology of G forces as they affect
the cardiovascular system (heart), cognitive function (brain), vision (eyes), and respiration
(lungs) is necessary to facilitate later discussions on factors that influence G tolerance.
1.3.1. The human body is adapted to an environment in which the constant gravitational
force exerted on it is equal to 1 G. An increase in the G forces results in reduced blood
pressure and blood flow to the brain and eyes. G forces in excess of 1 G pull blood
downward, causing it to pool in the lower body. This results in a decrease in blood returning
to the heart (venous return), and consequently diminished blood flow and blood pressure to
the head. This reduction of blood flow, and therefore oxygen delivery to the brain and the
eyes, can lead to aircrew incapacitation if not properly mitigated.
1.3.2. As blood and oxygen delivery to the brain is compromised, cognitive function will
diminish. The ability to process information decreases, reaction time can slow, judgment can
be clouded, and the ability to respond to communications or warnings can be lost. When
blood and oxygen supply to the brain falls below the level needed to maintain consciousness,
GLOC will result.
1.3.3. Unlike the brain, the eyeball has an internal pressure known as intraocular pressure
which is normally 10-20 mm Hg. Blood pressure must exceed intraocular pressure for any
oxygenated blood to enter the eye and reach the retina. The retina itself is extremely sensitive
to any reduction in available oxygen, and various impairments of vision can result. Some of
the most common visual degradations experienced by aircrew due to G forces include loss of
color vision (grey-out), loss of peripheral vision (tunneling), and complete loss of vision
(blackout). Blackout without GLOC is possible because the intraocular pressure can create a
situation where the eye experiences full loss of oxygenated blood even while the brain is still
receiving some blood flow. Aircrew must understand that any amount of vision loss during
flight due to G forces is an unacceptable risk. Aircrew must also understand that vision loss
does not always precede GLOC, see para 1.3.5.2.
1.3.4. The lungs are spongy, pliable tissue that can be extremely affected by G forces. As
positive G increases, the lungs can be compressed by the weight of the chest muscles and
other tissues pressing down on top of them. This compression of the lung tissue can result in
difficulty inhaling at high G and a feeling of air hunger, which is defined as deep, rapid, and
labored breathing caused by an increased respiratory drive due to abnormally low blood
oxygen levels. Making a preparatory inhale that is blocked off and held at the glottis prior to
the onset of G forces can mitigate this problem since the air trapped inside the lungs can’t be
compressed by the G forces. Subsequent exhales during the AGSM must be controlled to
prevent the escape of too much lung volume, which will result in lung compression,
difficulty re-inhaling the volume lost, and subsequent air hunger.
1.3.5. Three key concepts must be understood to fully comprehend an unaided human’s
ability to tolerate increased G forces. These concepts are relaxed (or resting) tolerance,
oxygen reserve, and cardiovascular reflex.
1.3.5.1. Relaxed Tolerance. Relaxed tolerance is generally defined as the number of
slow-onset Gz forces that an aircrew member can withstand without the aid of an anti-G
straining maneuver (AGSM) or any G protective equipment. This G value typically lies
in the range from 4.5-6.0 G and is a combination of several factors, such as resting blood
pressure, vertical distance from heart to brain, hydration status, and a number of other
6 AFPAM11-419 17 OCTOBER 2014
human factors. Relaxed tolerance can vary greatly from one individual to another, and
within the same individual from one day to another or even from the beginning of a flight
to the end of a flight, based on changes in these factors.
1.3.5.2. Oxygen Reserve. There is a very limited amount of oxygen within the tissues of
the body at any given time. This oxygen is metabolized by the tissue, and resupplied by
oxygenated blood flowing to the tissue through the cardiovascular system. During rapid
onset to high sustained G forces, blood supply to the brain and the eyes can be lost. The
residual oxygen in the brain and the eyes at that point will allow those tissues to continue
to function for 4 to 6 seconds. This is known as the oxygen reserve. If oxygenated blood
supply is returned to the brain and the eyes before the oxygen reserve is completely
consumed, it is possible for those tissues to continue to function without disruption. For
example, a rapid onset to 9 G that is held for only 2-3 seconds before return back to 1 G
can be tolerated by nearly all aircrew without a resulting loss of vision or disruption of
consciousness, even if no AGSM or anti-G suit is used. However, if oxygenated blood
flow is not returned to the brain and eyes before the oxygen reserve is completely
consumed those tissues will abruptly and simultaneously cease to function, resulting in a
simultaneous loss of consciousness without any preceding vision loss.
1.3.5.3. Cardiovascular Reflex. When the body is subjected to greater than 1 G,
resulting in a drop in cranial blood pressure, the body will initiate a cardiovascular
response that increases heart rate, stroke volume, and peripheral vascular resistance to
improve blood flow and pressure to the brain. The full reflex response is a compensation
method that takes 10 to 15 seconds of decreased cranial blood pressure to initiate, will
increase G tolerance by approximately 1 G over resting tolerance, and will remain active
for up to 10 to 15 minutes once triggered.
1.3.6. Visual deficiencies and GLOC do not occur on every exposure to positive G. To
maintain consciousness under G stress greater than resting G tolerance, an AGSM is
required, even with the benefit of the cardiovascular reflex. The onset rate, magnitude and
duration of the G combined with individual tolerance, aircrew flight equipment and AGSM
work together to mitigate the negative impact of G forces. Rapid G onset or relaxation of the
AGSM at high G levels can lead to GLOC without any visual symptoms or warning signs.
Consciousness can be maintained when the G-onset rate is slow enough that visual symptoms
are recognized and the AGSM is adjusted accordingly. In modern fighters with high G-onset
rates and sustained peak G levels the ability to adjust the AGSM is significantly reduced,
making employment of a well-executed AGSM just prior to G onset imperative. Mishap
statistics and surveys have shown that no aircrew is immune to GLOC; it can happen to
anyone flying any high-performance aircraft at any time.
1.4. GLOC. GLOC is a significant concern associated with excessive exposure to positive G.
GLOC is the incapacitation that can occur when blood pressure and oxygen delivery to the brain
is insufficient to maintain consciousness.
1.4.1. Incapacitations. GLOC can be divided into two periods; absolute incapacitation and
relative incapacitation. Absolute incapacitation refers to complete unconsciousness, and
typically lasts an average of 12 seconds, with a range of 9 to 22 seconds. Convulsive flailing
of the arms and legs may occur at the end of the absolute incapacitation. Relative
incapacitation is the period starting with regaining of consciousness and lasting until the

AFPAM11-419 17 OCTOBER 2014 7
aircrew has fully recovered situational awareness. Relative incapacitation also averages 12
seconds in duration, with a range of 5 to 40 seconds. Symptoms during relative
incapacitation include, but are not limited to, disorientation, confusion, stupor, apathy,
anxiety and nausea. In some instances during centrifuge training and centrifuge research
aircrew have been seen to enter into a relative incapacitation period that was not preceded by
an absolute incapacitation period (unconsciousness). Researchers have termed this
phenomenon “almost loss of consciousness (ALOC)” or “near loss of consciousness
(NLOC).” From an operational standpoint, the aircrew was incapacitated due to the G forces
and was unable to perform crew duties during this time. Therefore, ALOC, NLOC, or any
other term used to differentiate this condition from GLOC will not be used to describe G-
induced incapacitations during flight or during aircrew centrifuge training.
1.4.2. Initial Recovery. At the end of this total incapacitation period, the individual is able to
recognize where he or she is and respond to the environment. Transition from the relative
incapacitation phase to the initial recovery phase can sometimes be accelerated by using
simple, directive calls, such as “pull up,” or by using the aircrew’s name or call-sign.
1.4.3. Full recovery. The return of cognitive processing skills may require several minutes
before fully returned to normal function. During this time, flying skills and situational
awareness may be severely impaired. In addition, a sudden high-G attempt at aircraft
recovery soon after a GLOC may induce a subsequent GLOC episode. The implications of
GLOC and its immediate potential after-effects in a combat scenario are obvious. Degraded
cognitive function should be expected post-GLOC. Flight members providing assistance
should keep communications directive and extremely clear.
1.4.4. GLOC Recognition. GLOC may go unnoticed due to amnesia that can occur as a
result of impaired oxygen flow to the brain. You should suspect that GLOC may have
occurred if you cannot explain a sudden loss of altitude or have difficulty recognizing your
aircraft attitude. Tingling around the mouth or in the extremities and a sense of dreaming are
just two of the various sensations you may experience upon recovery from GLOC. It is
possible that review of your head-up display (HUD) video during debriefing may be your
first clue that you experienced an in-flight episode of GLOC. Never use visual symptoms to
gauge your current G tolerance. NOTE: Any visual impairment due to G force means
you are dangerously close to GLOC. If you experience gray-out under G, you have only
10 percent of oxygen reserve remaining and are dangerously close to a GLOC.
1.5. Physical Conditioning. The purpose of physical conditioning (PC) for fighter aircrew has
been recognized since the beginning of high-G aircrew training, as an important factor in the
protection against the stresses of G-forces in the aircraft. As one of the physiological means of
improving G-tolerance, PC is the foundation of optimal human performance in and out of the
aircraft. Analogous to an athletic event, high-G aircrew will be exposed to high levels of
external and internal stressors (e.g. physical threat of G-forces, thermal stress, hypoxia, nutrition,
circadian cycles, etc.) and one’s ability to manage these stressors and ensure peak performance is
dependent upon PC; those with higher levels of PC are capable of handling more stress. As
exemplified from the General Adaptation Syndrome, there exists a stress-adaptation response to
any stressor applied to the human body and the variables affecting the response consist of
intensity, volume, frequency, duration and mode. As a defense mechanism to the stress being
applied, the human body will attempt to accommodate the environment if the stressor is applied
for a short period of time (i.e. hours or days). However, if the period of time extends into days or

8 AFPAM11-419 17 OCTOBER 2014
weeks, then the physiological implications of the stress-adaptive response is considered
acclimatization. The physiological system will adapt to the level of stress in a process called
adaptation.
1.5.1. An effective, tailored PC program will improve any aircrew’s performance under
physical stress. For high-G aircrew, this means an improved G-tolerance. The G-force
factors that affect G-tolerance include: peak G (i.e. intensity), time-on-top of G (duration),
and onset rate of G-forces (i.e. mode). If the high-G environment, G-force factors were to be
characterized as a physical activity; it can be considered short-term, high-intensity bouts of
various activity levels interspersed with bouts of short to moderate lengths of recovery. A
Special Report prepared by the USAF School of Aerospace Medicine, USAFSAM-SR-88-1,
Physical Fitness Program to Enhance Aircrew G Tolerance, made the initial observation that
a strength and conditioning program focused on anaerobic capacity was crucial with
moderate focus on aerobic capacity. Unfortunately, inadequate research has resulted in
unqualified individuals providing advisor services without appropriate
knowledge/skills/abilities and trendy fads that may or may not be of any real physical
conditioning benefit. Take the current knowledge based upon scientific research and learn to
apply it appropriately; making updates as new, scientifically validated information becomes
available. PC programs should only be planned and implemented through qualified
personnel; recent changes to the implementation of the Fighter Aircrew Conditioning
Program (FACP) have recognized this critical need. AETC has developed an instructor
training course for FACP. Additionally, there are two reliable professional organizations
which provide credible certifications for such personalized training; 1) National Strength and
Conditioning Association (NSCA) and the American College of Sports Medicine (ACSM).

AFPAM11-419 17 OCTOBER 2014 9
Chapter 2
PROTECTIVE MEASURES
2.1. G-Tolerance Factors. G-tolerance is the ability or capacity to maintain vision,
consciousness, and effective performance when under G-stress. To do this, blood pressure and
flow must be maintained to the brain and eyes. The AGSM is the critical component of high G-
tolerance, but G awareness and “G-discipline” for high onset rates and sustained G are the
critical elements of GLOC avoidance. Factors which affect an aircrew’s G-tolerance include:
2.1.1. Aircrew physical attributes, such as resting tolerance
2.1.2. Aircrew mission preparation
2.1.3. AGSM effectiveness
2.1.4. G-protection equipment
2.1.5. G awareness and discipline
2.2. Resting Tolerance. There is no one body type that is immune to GLOC. Some aircrew are
“G naturals,” some are not; but ALL of them can significantly increase their G-tolerance. The
average aircrew resting G-tolerance is between 4.5 to 6.0 Gz. Resting tolerance is determined at
0.1 G/second onset rate. Rapid onset rate experienced in the aircraft can be up to 6.0 G/second.
Resting tolerance provides added protection in that it requires less work during the AGSM, but a
full AGSM must be initiated and maintained until max G is reached. Evidence suggests that tall
individuals are more likely to have a lower resting tolerance but may be able to compensate with
an effective anti-G strain maneuver. Resting tolerance does not protect against rapid onset rates
and an insufficient AGSM could result in significant vision loss and/or GLOC during or
immediately following the G onset.
2.3. Mission Preparation. Physical traits do not necessarily predict G-tolerance. Before every
sortie, aircrew should perform an ops check of the human weapon system. Physiological factors
such as dehydration, hypoglycemia, lack of G-specific physical fitness, or illness can adversely
affect G-tolerance and AGSM effectiveness. Adequate personal risk management is essential for
G preparation and GLOC prevention. Specifics for optimizing mission preparation are discussed
in Chapter 3. Both AF and Navy studies have shown anaerobic training improves G-tolerance.
Muscular strength and endurance training has been shown to increase strength, endurance, and
cockpit mobility during flight in the high-G environment. Moderate amounts of aerobic activity
have not demonstrated any degradation of G-tolerance. The cardiovascular fitness improvements
from aerobic exercise (aerobic capacity) will enhance the ability to recover from straining
maneuvers and shorten the recovery time between engagements and sorties. Attachment 2 of
this instruction presents a comprehensive program of strength training and aerobic training
designed to increase your G-tolerance.
2.4. AGSM. The AGSM is the best G defense measure available to aircrew. Equipment
measures (anti-G suit, COMBAT EDGE to include Positive Pressure Breathing for G (PBG),
reclined seat, etc.) were never meant to replace the AGSM, only aid it. Together, the AGSM and
G protective equipment provide over 9.0 G of protection. The current standard anti-G suit, CSU
13B/P, provides 0.3 to 0.5 G when fitted properly and 1.5 to 2.0 G of protection when fully
inflated. Aircrew must properly perform a timely and efficient AGSM in order to gain maximal

10 AFPAM11-419 17 OCTOBER 2014
benefit. It is very important that you perform the same, correct AGSM each time you anticipate
and or apply G, regardless of the amount of G. This will ensure positive feedback, and will
imprint the proper AGSM to make it an automatic response. A sound AGSM can provide
between 4.0 to 4.6 G of protection. If chest pressure is lost or the lower body strain is relaxed,
protection provided by the AGSM can be reduced significantly. Aircrew should not use G suit
inflation or visual disturbances as a cue to initiate AGSM.
2.4.1. AGSM Components. The AGSM consists of two components: lower body muscle
strain and respiratory component. Performing one without the other may significantly reduce
the effectiveness of the AGSM. The AGSM preparation should precede rapid Gz onset. It is
extremely difficult to “catch up” to a Gz load if you get behind from the start. In addition,
proficiency in performing the maneuver may decrease (decondition) when you have not
flown recently. It takes approximately 8 – 14 days for acclimation and 14 – 28 days for
deacclimitization and/or deconditioning to occur. Physical conditioning, mental
preparedness, proficiency, and currency are all keys to an effective AGSM.
2.4.1.1. Lower body Muscle Strain.
2.4.1.1.1. Purpose. The simultaneous isometric contraction of the calf, gluteal,
hamstring, quadricep, and abdominal muscles increases blood pressure and blood
flow to the heart, forces blood flow to the brain, and prevents blood from pooling in
the lower extremities. Additionally, contracting abdominal muscles prevents G-suit
from forcing air out of the lungs during rapid onset to G.
2.4.1.1.2. Execution. The most effective isometric contraction is executed with an
inward squeeze of the legs. Posture and body position are important factors in
performing an effective lower body strain. Feet should be shoulder width apart,
aligned with the knees, and knees aligned with the hips. In order to adequately
engage the gluteus and other lower body muscles, aircrew should dig their heels to
the ground and allow their pelvis to roll upward as the glutes tighten. Pushing off the
floor or rudder pedals with the legs limits the contraction of the glutes and other
lower body muscles ultimately reducing the effectiveness of the strain. The
abdominal muscle contraction should be executed with an outward push against the
G-suit bladder. The lower body muscle strain is the first defense against blood
pooling in the lower extremities and are thus an essential element of the AGSM.
They also provide the majority of the protection provided by the lower body strain.
For the lower body strain to be most effective, the initial strain must precede the G-
onset. The lower body strain should remain intact from before the G-onset until the
end of the G exposure.
2.4.1.2. Respiratory Component.
2.4.1.2.1. Purpose. The respiratory component of the AGSM is an adaptation of the
Valsalva maneuver that produces increased intra-thoracic (chest) pressure. The air
exchange interrupts the generation of chest pressure with 2.5 to 3.5 second intervals
with a rapid (<1 sec) exhale and inhale. During this brief period, intra-thoracic
pressure drops allowing for venous return and then immediately increases to return
cranial level blood pressure. The brief exchange of air also maintains lung inflation.
The air exchange is not intended to satisfy air hunger but to allow the heart to refill
with blood.

AFPAM11-419 17 OCTOBER 2014 11
2.4.1.2.2. Preparatory Breath. The respiratory component begins with a preparatory
breath prior to the G onset. The preparatory breath should approximate over half the
lung’s capacity and should not cause the chest and shoulders to rise up significantly.
The breath should be sealed off at the glottis with minimal pressure and held for
approximately 2.5 to 3.5 seconds. The preparatory breath inflates the lungs and
increases intra-thoracic pressure before the G onset.
2.4.1.2.3. Cyclic Breathing. The first rapid air exchange (exhale and inhale) should
occur approximately 3 seconds after the preparatory breath or once on top of G,
whichever occurs first. To correctly perform the air exchange, the air should be
blocked off at the glottis and a phonetic “K” should be heard on the exhale. The
exhale should be passive under G unless flying with PBG. In the case of PBG-
assisted flight, the aircrew must forcefully exhale against the pressure. Immediately
following the exhale, a quick, active inspiration should be executed. The volume of
air of the inhale should equal the volume of air of the exhale. Ideally, the exhale and
inhale process should only take about 0.5 seconds. The air exchanges should
continue every 2.5 - 3.5 seconds for the remainder of the G exposure. During G
exposure, use the shortest communications required in the tactical situation.
2.4.1.2.4. Upper Body. Upper body muscle contraction/tension should be minimal.
Chest pressure will be created during the respiratory component, but shoulders, chest
and arm muscles should not be engaged as part of the strain. Excessive chest pressure
or upper body muscle straining is very fatiguing and counterproductive to the lower
body strain.
2.4.2. Common AGSM Errors. It is imperative that aircrew develop sound AGSM
technique that is second nature and not reactive. The following paragraphs describe
execution errors in AGSM performance. A single error from the list below could cause
reduced cranial blood pressure, causing significant vision loss and/or GLOC. A combination
of errors significantly increases the risk of vision loss and/or GLOC.
2.4.2.1. Aircrew may fail to turn academic knowledge of the AGSM into practice while
performing other flying skills/duties. The mental demands of operating high-G aircraft
have proven to detract from AGSM performance; therefore all high-G aircrew must be
able to integrate proper AGSM employment with flying operations. Simply
understanding AGSM mechanics is not enough.
2.4.2.2. Aircrew may fail to tense the lower body musculature or failing to maintain the
lower body strain causes blood to pool in the extremities. Failure to adequately strain
lower body and allowing blood to pool significantly reduces blood return the brain.
2.4.2.3. Individuals may create excessive chest pressure by performing too large of a
preparatory breath, causing a significant amount of additional fatigue.
2.4.2.4. Taking in too large of an initial inhalation or bearing down with excessive chest
pressure against the closed glottis will result in decreased heart rate, blood pressure and
degradation of AGSM effectiveness. Bearing down with the chest to create excessive
pressure against the glottis will lead to overstimulation of the baroreceptors in the carotid
artery. As a result, vasodilation may occur, leading to a significant reduction in cranial

12 AFPAM11-419 17 OCTOBER 2014
blood pressure. In this case, too much force in the chest reduces blood availability to the
brain.
2.4.2.5. Failing to anticipate the G. Execution of the AGSM should begin before G is
loaded on the aircraft. Failure to anticipate G-onset will result in the aircrew either trying
to catch up on the AGSM (a very dangerous practice) or having to unload in order to buy
time to catch up.
2.4.2.6. Blocking the air exchanges off at the lips or teeth rather than the glottis.
Controlling the volume of air exchanged under G is essential to a sufficient AGSM.
Blocking the air exchanges off at the teeth or lips leads to air leaks, especially as fatigue
sets in.
2.4.2.7. Failing to maintain chest pressure, or losing air, could occur while talking or
whenever the strain is audible. As air is lost from the chest the amount of pressure
generated is reduced, directly reducing blood pressure to the brain. If air loss is
significant, as might occur with speech, the subsequent loss of blood pressure in the brain
may result in GLOC without visual loss. Air loss could also be caused from “grunting”
(letting the air escape slowly) as a result of excessive pressure against the glottis or as a
result of unequal volumes of air during the exhale and inhale.
2.4.2.8. Rapid breathing (< 2.5 seconds) leads to hyperventilation under G and can cause
significant vision loss and dizziness.
2.4.2.9. Breath holding (> 3.5 seconds) increases chest pressure and impedes return of
blood to the lungs where it is available to the heart. If blood return to the lungs is
blocked for 4 to 5 seconds the heart may run out of blood to pump.
2.4.2.10. Taking too long to complete the air exchange. Total time for each breathing
cycle should be 0.5 seconds. Slow air exchanges, extending longer than 1 second, allow
blood to pool in the lungs.
2.4.2.11. Overly aggressive AGSM. Performing a strain with the intensity necessary to
maintain vision at 9 G when the G load is only 5 G can result in early fatigue and
increase potential for GLOC in subsequent engagements. The intensity of the AGSM
should be graded in relation to the G level. It is always safer to overestimate the intensity
of the strain.
2.4.3. AGSM Checklist
2.4.3.1. Anticipate the G onset.
2.4.3.2. Simultaneously tense all lower body muscle groups to include legs, glutes, and
abdominal muscles (maintain this strain).
2.4.3.3. Execute an adequate preparatory breath sealed off at the glottis.
2.4.3.4. Once at peak G, perform air exchange every 2.5 – 3.5 seconds with equal size
exhalation/inhalation (<1 sec).
2.4.3.5. Minimize tensing of the upper body; create chest pressure sufficient to enable a
short, crisp air exchange.
2.4.3.6. Minimize communications.

AFPAM11-419 17 OCTOBER 2014 13
2.4.3.7. Don’t relax until G is unloaded to pre-strain levels.
2.4.4. AGSM Training and Proficiency. While the aircraft and personal G-protection
equipment are passive, the AGSM is active. It requires anticipation of the maneuver and is a
practiced skill which must be integrated with numerous other cockpit tasks. The efficiency
and intensity of the AGSM depends on multiple factors, including strength, endurance,
training, motivation, and proficiency. The AGSM is like other athletic skills in that it is
susceptible to deconditioning. Scientific studies indicate there is some decrease in the
endurance of the AGSM when the aircrew is not current and proficient. Tolerance to peak G
for short intervals may not be affected. NOTE: Endurance to multiple or sustained high-G
engagement may be degraded after a layoff from high G; especially if illness was the
cause.
2.4.4.1. The best time to practice the correct AGSM is during the G awareness
maneuver. This is a part of the sortie during which you can devote almost all of your
conscious attention to G and to your AGSM technique. Once the engagements start, your
attention will be directed toward the mission and practice of the AGSM will probably be
a distraction. You should use hot mic during the G awareness exercise, so you can
review your AGSM during debrief. The aircraft is not the only place to practice. The
AGSM needs to become a subconscious maneuver. The more repetitions, the more
adapted the motor units become in activating the muscles used during the AGSM.
2.4.4.2. Centrifuge training has proven to be an invaluable tool in teaching aircrew a
proper AGSM without dealing with the consequences of a GLOC in flight. The Combat
Air Forces (CAF) require that all high-performance aircraft aircrew go through centrifuge
training. Training requirements and policy are described in AFI 11-404.
2.4.5. Using HUD Video to Review AGSM.
2.4.5.1. Several requirements should be met in order to provide the best appraisal of an
individual’s AGSM through HUD video review. Squadron supervision, flight surgeons,
or aerospace and operational physiologists should perform the following during the HUD
video review:
2.4.5.2. For AGSM assessments flown dual, it is optimal if the rear cockpit remains in
cold mic during high-G segments. It is difficult to assess AGSM when multiple crew
members are on hot mic.
2.4.5.3. BFM, ACT or other higher G-load setups are ideal for AGSM review. Lower-G
sorties do not tax the aircrew’s AGSM abilities sufficiently to provide a useful AGSM
assessment. Ideally, all setups should be reviewed including the G awareness maneuver.
2.4.5.4. It is not possible to assess the quality of the lower body strain from HUD video
review. However, the importance of this aspect of the AGSM should be emphasized.
2.4.5.5. A good AGSM should begin with an audible preparatory breath just prior to G-
onset.
2.4.5.6. The first air exchange should occur 2.5-3.5 seconds after G onset or at peak G,
whichever arrives first. Listen for exhalation sounds or talking during the G-onset. This
signifies loss of air from the chest and reduced efficiency of the strain and G-tolerance.
Additionally, the aircrew is likely to be behind the G and will have trouble catching up.

14 AFPAM11-419 17 OCTOBER 2014
This may cause the aircrew to either unload some of the G or sharply increase the
intensity of the strain (usually audible). The latter may be a result of recognition of
vision loss.
2.4.5.7. Air exchanges should be short, crisp and ideally around 0.5 seconds. It should
be followed by an audible sharp inhalation. The end of the inhalation may be noted by a
sudden grunt sound or a sudden absence of breathing sounds.
2.4.5.8. If breath sounds are more rapid than 2.5 – 3.5 seconds, average chest pressure
becomes lower and G-tolerance is negatively affected. As G-tolerance is negatively
affected, the aircrew will have to work harder at any given G-load. Fatigue during the
engagement or especially in subsequent engagements will most likely become apparent.
This may be evidenced by even more rapid breathing or breathless, gasping sounds.
Observation of the G-load at these times may provide evidence that the individual is
apparently working too hard for the G-level or is unable to maintain the G necessary for
the tactical situation.
2.4.5.9. Breath exchange intervals in excess of the prescribed 2.5-3.5 second range will
tend to decrease the effectiveness of the AGSM.
2.4.5.10. During video review, it can be very difficult to determine if and when a GLOC
has occurred. Ensure appropriate reporting to squadron leadership and safety
representatives, if applicable.
2.4.5.11. Typical post-GLOC aircraft performance characteristics:
2.4.5.11.1. Aircrew will unload G upon incapacitation. Depending on the flight
control system, this may occur rapidly or over a few seconds. No further inputs will
be made until the beginning of relative incapacitation period, at which point the
aircrew may initiate aggressive control inputs in attempt to recover the aircraft.
2.4.5.11.2. The aircraft will noticeably remain in whatever attitude/power setting that
was selected prior to GLOC. These settings may result in dramatic and unusual
altitude loss and increase in airspeed after GLOC occurs.
2.4.5.12. Typical post-GLOC aircrew performance characteristics:
2.4.5.12.1. The aircrew’s respiratory component will likely cease while still under
high G. Snoring, panting or relaxed breathing may be heard.
2.4.5.12.2. Once the aircrew has regained consciousness, he/she may be noticeably
confused. Communication may be incorrect or incoherent. Basic flying skills, such
as rejoins, may be noticeably impaired. However, some individuals may recover very
quickly with little observable decrement.
2.4.5.12.3. The aircrew may be uncertain of what happened or fully believe that a
GLOC did not occur despite evidence to contrary. Multiple input sources should be
gathered (other flight members, Flight Safety representatives, flight surgeon,
squadron leadership, aerospace and operational physiologist) to assess if GLOC
occurred.
2.5. G-Protection Equipment. AFE technical manuals require periodic refitting and describe
the proper fit of both the anti-G suit and full coverage G-suit. Ensure G-suit fit is checked no

AFPAM11-419 17 OCTOBER 2014 15
less than every 120 days or if changes occur such as individual weight loss/gain or in uniform
requirements due to seasonal weather differences.
2.5.1. Anti-G Suit. The current standard 5-bladder anti-G suit, CSU 13B/P, provides about
2G of protection over the aircrew’s relaxed G-tolerance. The garment is designed to counter
G forces in high performance aircraft by providing mechanical resistance against which the
leg and abdominal muscles can push, and to reduce the available space for blood to pool,
helping increase blood pressure. The garment incorporates encased bladders over the
abdomen and each thigh and calf to protect against visual dimming, blackout,
unconsciousness, and excessive fatigue caused by centrifugal forces during aircraft
maneuvering. The garment connects to the aircraft supply (pressure source) with a quick
disconnect, typically mounted on the left side of the pilot’s seat. Raise the dust cap to allow
proper connection to the aircraft supply. If disconnected while the aircraft is pressurized, the
garment will bleed down to 1.5 PSI in 4 seconds. The manual control button, located on top
of the aircraft inflation assembly, should be used to test the system before flight and can be
used during flight to further test the system. Quick disconnects require a force between five
to twenty pounds to release, depending on disconnect type. NOTE: Ensure all anti-G
garments are clean; combustible chemicals such as jet fuel or grease will burn at
normal flash points though the nomex will not burn until a higher temperature is
reached.
2.5.2. If aircrew experience the following conditions, they should immediately notify an
Aircrew Flight Equipment (AFE) technician:
2.5.2.1. Uncommanded garment inflation during level flight.
2.5.2.2. Garment does not inflate within two to four seconds of sustained 2G.
2.5.2.3. Garment does not deflate promptly upon resuming level flight.
2.5.2.4. Garment pressure is too low or too high.
2.5.3. Full coverage G-suit (FCGS). Similar to the CSU 13B/P, the full coverage G-suit,
CSU-22P or CSU-23/P, are designed to counter G force effects such as visual dimming,
blackout, unconsciousness, and excessive fatigue experienced during high performance
aircraft maneuvers. The trousers incorporate a single bladder that provides lower body
pressure coverage excluding buttocks, crotch and feet. This bladder is not authorized for
repair if the trousers fail leak checks; the trousers must be replaced. Additionally, the
trousers incorporate secondary restraint devices to prevent the bladder from interfering with
cockpit operations in the event of fastener failure. The anti-G trousers are equipped with a
quick disconnect similar to the 5-bladder system and will bleed down to 1.5 PSI in 4 seconds
if disconnected from supply during pressurized operations. The bladder inflates
automatically via anti-G valve upon aircraft maneuvering for two or more positive Gs. The
pressure provided is proportional to the Gs experienced and will deflate when G forces drop
below 2G. The trousers should remain deflated during level flight. A manual control button
is provided on top of the aircraft anti-G valve so the system may be tested. Aircrew should
test the system before flight and pay attention to routing of the hose assembly. The assembly
should be free of twists and folds and routed as directly as possible to allow maximum
aircraft maneuverability and prevent inadvertent disconnect during flight. Disconnect force
required is 18-24 pounds. Except for the F-22, the anti-G valve is located to the left of the

16 AFPAM11-419 17 OCTOBER 2014
pilot’s seat. For F-22 operations, the anti-G valve is located to the pilot’s right. Raise the
dust cap to allow proper connection to the aircraft supply.
2.5.4. The following abnormal conditions should be reported to AFE technicians and aircraft
maintenance (to investigate for faulty anti-G valve):
2.5.4.1. Trousers inflate during level flight.
2.5.4.2. Trousers do not inflate within three to four seconds of maneuvers above 2G.
2.5.4.3. Trousers do not empty promptly when G forces drop below 2Gs.
2.5.4.4. Excessive or inadequate pressure in the trousers.
2.5.4.5. Lower extremity pain, numbness, tingling, etc, whether local or general in
distribution.
2.5.5. Pressure Breathing for G (PBG). Pressure breathing for G helps increase G
endurance by decreasing the AGSM respiratory component workload at high G-forces, but it
does not provide additional protection against the initial rapid G onset. There is no change to
AGSM performance when flying with or without PBG. An anticipatory AGSM is still
required prior to the onset of high G to protect against GLOC with this system.
2.6. G Awareness. Application of a timely and effective AGSM is the critical component of
high-G tolerance, but G awareness and G discipline (for high onset rates and sustained G) are the
critical components of GLOC avoidance. G discipline ensures effective control of the rate of
onset and the level of sustained G which should be adjusted for multiple human factor variables.
Anyone can and will GLOC if good G awareness and discipline are not employed. Ego control
and an objective assessment of one’s mindset can be a critical factor in the avoidance of a
GLOC.
2.6.1. Enhanced situational awareness includes more than just tactical and spatial awareness;
it also includes assessing one’s own physiological and psychological state throughout the
flight. You must develop a subconscious anticipation of impending G exposure or good G
situational awareness (G SA). There is no time to “think about it” with high-G onsets. Using
predictive and anticipatory skills will result in proper G discipline in the cockpit. Proper G
discipline, if employed, would have prevented nearly all our GLOC fatalities in the CAF.
KNOW YOUR LIMITS and use good G SA to maximize performance.
2.6.2. Technique. Flying technique relates to both subconscious use of the AGSM and
learned air-to-air combat methods. The proper application of G-onset rates and of sustained
G to apply combat power is something learned and enhanced through training and
experience. Resist becoming complacent with an aggressive style that disregards the human
factors that can become limiting. Consistently evaluate the effectiveness of techniques
associated with flying skill as well as AGSM application.

AFPAM11-419 17 OCTOBER 2014 17
Chapter 3
OPTIMIZING HIGH-G MISSION PREPARATION
3.1. Physical Characteristics. Safe operations in the high-G environment can be improved by
optimizing our daily habits and activities. Some natural physical characteristics are associated
with good G performance, but none are absolute guarantees of avoiding GLOC. For instance, a
person with higher blood pressure may have better G performance than a person who has lower
blood pressure. However, many physical attributes can be improved resulting in increased G
tolerance. Overall strength, particularly in those muscles utilized during the AGSM, is
associated with better G performance. For this reason, high performance aircrew should have a
comprehensive fitness routine that includes strength and endurance training. This fitness routine
should target muscles that are utilized during the AGSM, to include calf muscles (gastrocnemius
and soleus), hamstrings, quadriceps muscles, abdominal muscles, and gluteal muscles. While
there are many ways to condition for physical improvement, the emphasis should be on
mastering the AGSM during G exposure.
3.2. G Awareness Program History. As early as 19381, the stress of G-forces and GLOC from
aerial combat were recognized and the knowledge-base has continued to expand as our
technology in combat aircraft systems progresses. However, the high-G environment education
and training timeline began in 1985 with the USAF implementation of a high-G initial aircrew
program2. In 1987, the USAF established G-tolerance standards and selections for fighter
aircrew3, and further refinements of fighter aircrew high-G training occurred in 1988
4. A
broader understanding of the G-environment and the human-machine interface was introduced in
1988 by KK Gillingham5 with the summarization of the effects of high-G stress on the human
body and a systematic method for grouping G-tolerance improvements; i.e. mechanical,
educational and physiological. His research demonstrated G-tolerance improvements through
acclimatization via centrifuge training in accordance with AFI 11-404 and high-G exposures in
the aircraft, natural physical and technical abilities, a skillful and proficient AGSM, and optimal
PC to enhance fighter aircrew tolerances to the stress of a high-G environment6.
3.3. Physical Conditioning. A comprehensive program would include several components,
including cardiovascular fitness, muscular strength/endurance, balance/stability, and flexibility.
3.3.1. Cardiovascular fitness: increases blood supply to the working muscles, reducing
recovery time between engagements. It may also increase G endurance, that is, the ability to
fly multiple high-G engagements.
1 (Burton RR, Aug 1985)
2 (Lyons TJ, Apr 1997)
3 (Gillingham, G-tolerance standards for aircrew training and selection, Oct 1987)
4 (Gillingham KK, Jan 1988)
5 (Gillingham, High-G stress and orientational stress: physiologic effects of aerial maneuvering,
Nov 1988) 6 (Gillingham, High-G stress and orientational stress: physiologic effects of aerial maneuvering,
Nov 1988)

18 AFPAM11-419 17 OCTOBER 2014
3.3.2. Muscular strength: The AGSM is enabled primarily through muscular strength.
Increasing the maximal amount of force you can generate can lead to a more efficient
AGSM.
3.3.3. Muscular endurance: Increased muscular endurance improves the ability to repeatedly
perform isometric muscle tensing, thereby reducing muscle fatigue.
3.3.4. Balance/stability: exercising muscles deep within the abdomen and back attaching to
the spine or pelvis will improve cockpit stability, ultimately leading to a better AGSM.
3.3.5. Flexibility: refers to the degree to which a joint moves through a normal, pain-free
range of motion. Good flexibility may contribute to a successful AGSM and reduce the risk
for injuries.
3.3.6. When exercising for G, it’s important to target those muscles that are utilized during
the AGSM. While core and lower body muscles are most important, upper body strength and
overall cardiorespiratory endurance are also important components of proper G fitness. To
improve G performance, develop a fitness plan with cardiovascular components for a
minimum of 30 minutes, three times a week. A complete fitness plan will also have elements
to build strength and endurance in the following muscle groups: quads, glutes, abs, calf
muscles and arms. It is widely accepted that anaerobic strength is not the only fitness
component for high-G aircrew; “the endurance component of a sustained duration mission
must be coupled with good core strengthening and muscle tone.” 7 More detailed fitness
education and recommendations are located in Attachment 2.
3.3.6.1. Recent revisions to the Fighter Aircrew Conditioning Program (FACP) will
change the assessment criteria to a circuit-like rotation. This type of training may be
optimal for group PC events, such as squadron PT. The assessment emphasizes isometric
function in core and lower body large muscle groups as these are primarily used during
the AGSM. A cardiorespiratory component has been added because of the significant
impact cardiorespiratory endurance has on the ability to execute multiple AGSMs over
multiple sorties in a given day. The assessment was designed, in conjunction with last
AF fitness assessment (FA) results, to establish a baseline for trainees and to identify
areas that should be emphasized during workouts to ensure fitness for high G-flight.
3.3.6.2. FACP Assessment Basic Guidelines. Full guidance for FACP assessment
completion is incorporated into AFI 11-404, Centrifuge Training for High-G Aircrew. A
brief outline of assessment requirements is located here to illustrate PC concepts
discussed in this attachment. Students are assessed using a standard rotation of six
stations, which are located at least 25 feet apart. Trainees have 12 minutes to complete 2
full rotations of each station, and one minute to complete a minimum number of exercises
in each station. The required stations include squats, cross knee crunches, lateral lunges,
squat thrusts, push-ups, and crunches. There is no required order of completion for each
station; however, stations requiring same major muscle groups should be spaced apart.
During the assessment, form is an important part of completing repetitions, as ability to
execute the exercise cleanly is an indicator of strength.
7 (Baumgartner, 2011)

AFPAM11-419 17 OCTOBER 2014 19
3.3.7. Anaerobic Training Adaptations. Anaerobic training programs are the historical
emphasis of G-performance training programs. They consist of short-term, high intensity
exercise spaced with intermittent bouts of recovery intended to challenge the short-term
energy systems in muscle tissue. Specific anaerobic training program adaptations result in
increased capability in maximal exercise for up to three minutes and improved motor skill
performance8. Certain exercises will train specific metabolic pathways; for example, sprints
and drills under 10 seconds improve the phosphagen metabolic pathway. In order to stress
the glycolytic system, work/rest ratios can be shortened while performing short-term, high
intensity exercise sessions. With highly organized and diligently executed anaerobic training
programs the athlete can expect to see physiological adaptations such as, improved neural-
muscular recruitment and reflex potentiating, muscular alterations in fiber count
(hyperplasia) and fiber size (hypertrophy), metabolic enhancement in anaerobic muscle fiber-
type distribution (transition), and structural and mechanical alterations in connective tissue
(e.g., bones, tendons, ligaments, fascia, etc.). An important factor in planning an exercise
program with a primary focus upon anaerobic capacity will be to moderate the intensity,
volume and frequency of the aerobic training9,10
.
3.3.8. Aerobic Training Adaptations. Aerobic training challenges the muscle tissue’s ability
to use oxygen in exercise for three minutes and beyond. These programs need to encompass
both sprint and steady state work levels to account for the multitude of aerobic adaptations
from a tissue to a metabolic perspective. Similar physiological systems will be affected by
an aerobic training program and training adaptations will occur in the cardiovascular,
nervous, muscular and skeletal systems. However, the adaptive changes resulting from the
work load stress/demand during excessive aerobic training may negatively affect the
anaerobic component. The necessary steps must be taken to appropriately plan the anaerobic
and aerobic components of an exercise program11,12
.
3.3.9. Warm-up, Stretching and Flexibility. Regardless of the exercise training program’s
primary and secondary goals, a warm up/flexibility component is crucial. This component is
important for injury prevention and to improve proprioceptive/balance attenuation. A warm
up will provide faster muscle contractions/relaxations of agonist and antagonist muscles,
improve rate-of-force production and reaction times, improved muscle power and strength,
increased blood flow and oxygen delivery to enhance metabolic reactions. A general warm
up consists of 5 – 10 minutes of slow activity with an aim to increase heart rate, blood flow,
muscle temperatures, breath rates, sweat rates, and joint fluid viscosity. Another option is a
more activity-specific warm up that mimics the activity performed, lasting approximately 8 –
12 minutes in length. Flexibility as a component of a warm up or cool down will improve
performance and reduce risk of injury. It is essential the anaerobic athlete (i.e. high-G
aircrew) minimize the potential of loss of time in the aircraft through preventative measures
8 (McArdle WD, 2010)
9 (National Strength and Conditioning Association, 2008)
10 (American College of Sports Medicine, 2012)
11 (National Strength and Conditioning Association, 2008)
12 (American College of Sports Medicine, 2012)

20 AFPAM11-419 17 OCTOBER 2014
and maintain, if not improve, flexibility through stretching. Stretching can be employed post
workout or flying and as a separate session alone13,14
.
3.4. Other Human Factors Affecting Our Ability to Tolerate G Stress. While important for
G performance, a comprehensive fitness program alone will not provide adequate protection
against GLOC. G performance will be impacted by a myriad of factors on a day-to-day basis.
Those factors may include nutrition, alcohol use, self-medication, thermal burden, hydration,
rest, G-suit fit, time away from the G-environment, and situational awareness. Therefore,
properly preparing for G performance includes several factors: healthy eating, proper hydration,
plenty of rest, checking G-suit fit and function, and maintaining situational awareness at all
times. In addition to these factors, performing a proper AGSM throughout each and every
mission will ensure your success in the high +G environment.
3.4.1. Fatigue. The ability to perform an AGSM directly correlates to strength and
endurance, and these characteristics are related to rest and fatigue. Fatigue from inadequate
sleep is different than muscle fatigue. Muscle fatigue severely degrades the AGSM, whereas
inadequate sleep degrades alertness and G awareness. Either way, your G-tolerance is
compromised.
3.4.2. Heat stress degrades the body’s ability to do work and reduces G tolerance. The
combination of dehydration and blood moving to the skin for cooling significantly reduces
G-tolerance and work capacity. Studies have shown that with only 3 percent dehydration, G-
tolerance time may be reduced up to 50 percent. Always stay well hydrated, especially in hot
conditions; increase fluid intake before and during the mission.
3.4.3. Poor nutrition affects performance in the cockpit. It is important to eat regularly two
or three times a day. Optimal nutrition is based largely on vegetables, root vegetables and
tubers, natural meat protein sources, unrefined fats, unrefined fruits and possibly dairy (if
well-tolerated). Grains and grain products, sweeteners of all types, and refined oils should be
minimized if not eliminated. Avoid high sugar “coke and candy bar” snacks when unable to
eat regularly. G-tolerance is reduced if your blood sugar drops below normal ranges. To
minimize this potential problem, avoid “substitute” snacks high in sugar content. Poor
nutrition has been a strong contributor to GLOC events. Recent mishap reviews discuss
aircrew who have only consumed potato chips or a niacin supplement as their entire daily
intake have experienced GLOC episodes.
3.4.4. It has been well documented that alcohol and its hangover effect have a significant
negative effect on G tolerance. Alcohol degrades sleep quality, causes dehydration and salt
loss, and depletes body sugar stores. It also tends to dilate blood vessels. All these factors
have a negative effect on the body’s ability to tolerate G-stress and will result in GLOC if
dehydration effects are not countered.
3.4.5. Illness or infection also degrades G tolerance. Although the amount of degradation is
unknown, some GLOC mishaps have occurred just after aircrew have returned to flying after
being ill. Performance may be reduced after a recent illness when the body is probably not
ready to support the intense effort for an aggressive BFM or ACM sortie. When coming
back on status, energy level and muscular strength may be lower and the cardiovascular
13
(National Strength and Conditioning Association, 2008) 14
(American College of Sports Medicine, 2012)

AFPAM11-419 17 OCTOBER 2014 21
system may be “detuned” and detrained (slower and less intense response). The use of
medication can potentially further degrade G-tolerance and performance. Together, these
effects can reduce aircrew’s ability to tolerate G stress. Studies have shown that two weeks
of non-flying has results in lower G-tolerance resulting from detraining effects; this effect is
increased by illness.
3.5. Mission Assessment and Planning. Personal G-tolerance abilities should be considered
during mission planning. Have Gs ever been a problem? Are there any current red flags to less
than optimal G performance? Is this a particularly demanding upgrade sortie or a uniquely
demanding sortie for some other reason? Is aircraft configuration such that extremely high-G
loads are likely? These, among others, are good questions to ask at the mission planning stage.
3.5.1. Consider how long it has been since the last high-G sortie flown. If aircrew are
returning from a break from high-G missions, plan G-maneuvering on the assumption that G-
proficiency and G-tolerance will be low. Decide what onset rates are acceptable and what G
levels should be used. Have a game plan to prudently react to any indications of sub-par G-
tolerance both individual aircrew and flight members.
3.5.2. High-G flight requires a physiological system that is operating as close to 100-percent
as possible. Proper sleep, nutrition & hydration must be emphasized. There will be days
when the right answer is to not fly or fly a less demanding sortie. Practice good nutrition and
good sleep discipline. Fly nourished and rested to the maximum extent possible. Don’t fly
when ill, fatigued, dehydrated, or while on medications. Regular exercise, good nutrition,
and regular sleep allow aircrew to fly at peak condition (peak G capacity).
3.5.3. Proper hydration is critical for normal G-tolerance. Don’t wait until a feeling of thirst.
Proper hydration starts days, not minutes, before step. Plan to bring sufficient water to the
aircraft to meets the demands of unanticipated extended ground ops or high heat conditions.
3.5.4. Ensure physical training is deconflicted from high-G sorties. If muscles used during
the AGSM are sore or exhausted, the ability to execute a proper AGSM will be impaired.
Avoid any strenuous activities the day of a high-G sortie.
3.6. Pre-flight.
3.6.1. Ensure G-suit is properly fitted and that comfort zippers are engaged. A loose fitting
G-suit may be more comfortable, but will not provide the rated G-protection.
3.6.2. Conduct a good pre-flight warm-up during the walk-around and when in the seat.
Lower body musculature as well as trunk/neck rotational movements should be employed.
Light stretching is acceptable but range-of-motion and dynamic light load-bearing
movements are optimal.
3.6.3. In the cockpit, perform positive checks of all equipment and perform a G-suit inflation
check.
3.6.4. Review the plan once again: what anticipated high-G maneuvering will be employed
in this mission, and how do flight members intend to monitor G-performance? What high-G
maneuvers are not acceptable during this flight?
3.6.5. Passenger Briefing Requirements. AFI 11-202 Vol. 3, General Flight Rules, directs
passenger briefing requirements. Required aeromedical topics, including preventing fatal
misunderstanding of regulator use, is further clarified in AFI 11-403, Aerospace

22 AFPAM11-419 17 OCTOBER 2014
Physiological Training Program. To meet the requirement that passengers are briefed on
items affecting safety or mission completion, brief passengers and other aircrew who do not
normally fly high-G aircraft on the aspects of high-G flight. Discuss the following topics:
3.6.5.1. How to execute an effective AGSM
3.6.5.2. How to operate the G-suit
3.6.5.3. Mission parameters, communications, and other means to indicate the need to
execute an AGSM
3.6.5.4. Importance of hydration, nutrition, and properly preparing for high-G flight
3.6.5.5. Individual problems that must be communicated to the aircrew
3.7. In-flight.
3.7.1. Performing a G Awareness Maneuver provides the following benefits:
3.7.1.1. Provides the opportunity to assess G-tolerance and allow for rehearsal of the
AGSM in a low-threat environment.
3.7.1.2. Allows opportunity to check the G-suit (and COMBAT EDGE if applicable)
connections and operation.
3.7.1.3. Recalibrates feel for application (onset) and control (peak level) aircraft G.
3.7.1.4. Provides an exposure to the cardiovascular system to activate the reflex response
to a drop in blood pressure. A maneuver of 3 to 5G for at least 10 seconds is required to
fully develop this reflex response.
3.7.2. Stay ahead of the Gs by employing an AGSM aggressive enough to match anticipated
G- load. Do not wait for signs that an AGSM is not meeting demands. No noted visual
impairment prior to GLOC is common at high G-loads/G-onset rates. There may be little to
no indication that the aircraft is outperforming the AGSM being performed as a
countermeasure.
3.7.3. During engagements, maintain energy state awareness and potential for impending
high-G. Intentionally plan to keep AGSM ahead of the Gs and recognize when it may be
lagging.
3.7.4. Intra-sortie fatigue is likely one of the most significant hazards (or fight-pit/tank-fight
scenarios). As the fatiguing effects of multiple high-effort AGSM bouts build, AGSM
performance will likely erode. This creates an increasingly hazardous condition as the sortie
continues. Be especially mindful of degraded G-performance late in the sortie.
3.7.5. Post Flight. Assess flight members’ G-performance with a candid assessment of
AGSM performance as well as assessment of how well the G-load was anticipated.
3.7.5.1. Any significant problems with G-performance noted in debrief should be
brought to the attention of squadron leadership. AFE personnel and maintenance should
also be notified to rule out any mechanical or equipment related causes.
3.7.5.2. Objectively review the mission; analyze G-discipline and AGSM effectiveness.
Were AGSM mechanics correct? Did preflight G-tolerance assessment match actual G-

AFPAM11-419 17 OCTOBER 2014 23
performance? Note any opportunities to perfect AGSM employment and improve
aircrew abilities to mitigate the effects of high-G flight.
3.8. Effective integration of G awareness concepts will decrease the risk of GLOC for
aircrew. This pamphlet provides a foundation. Experts such as squadron and operational
leadership, flight surgeons, aerospace and operational physiology personnel, exercise specialists,
and aircrew flight equipment personnel should also be consulted with additional questions on
GLOC prevention.
BURTON M. FIELD, Lt Gen, USAF
DCS, Operations, Plans and Requirements

24 AFPAM11-419 17 OCTOBER 2014
Attachment 1
GLOSSARY OF REFERENCES AND SUPPORTING INFORMATION
References
AFPD 11-4, Aviation Service, 1 Sep 2004
AFI 11-202 Volume 1, Aircrew Training, 22 Nov 2010
AFI 36-2251, Management of Air Force Training Systems, 5 Jun 09
AFI 91-204, Safety Investigations and Reports, 24 Sep 08
AFI 11-301, Aircrew Flight Equipment (AFE) Program, 25 Feb 09
AFI 11-202 Volume 3, General Flight Rules, 22 Oct 10
AFI 11-403, Aerospace Physiological Training Program, 30 Nov 12
AFI 11-404, Centrifuge Training for High-G Aircrew, 28 Oct 05
AFI 33-360, Publications and Forms Management, 7 Feb 13
AFRL-SA-WP-SR-2011-0003. July 2011. Handbook of Aerospace and Operational Physiology.
Woodrow AD, Webb JT.
American College of Sports Medicine. ACSM’s Foundations of Strength and Conditioning,
2012. Ratamess N.
Aviation, Space, and Environmental Medicine. 1985 Aug;56(8):812-7. Operational G-induced
loss of consciousness: something old; something new. Burton RR, Whinnery JE.
Aviation, Space, and Environmental Medicine. 1997 Apr;68(4):322-4. Assessment of the anti-G
straining maneuver (AGSM) skill performance and reinforcement program. Lyons TJ, Marlowe
BL, Michaud VJ, McGowan DJ.
Aviation, Space, and Environmental Medicine. 1987 Oct;58(10):1024-6. G-tolerance standards
for aircrew training and selection. Gillingham KK.
Aviation, Space, and Environmental Medicine. 1988 Jan;59(1):12-9. High-G training for fighter
aircrew. Gillingham KK, Fosdick JP.
Aviation, Space, and Environmental Medicine. 1988 Nov;59(11 Pt 2):A10-20. High-G stress and
orientational stress: physiologic effects of aerial maneuvering. Gillingham KK.
Aviation, Space, and Environmental Medicine. 2006 Jun;77(6):573-80. Physical conditioning to
enhance +Gz tolerance: issues and current understanding. Bateman WA, Jacobs I, Buick F.
Exercise Physiology, Nutrition, Energy, and Human Performance, 7th
edition. Lippincott,
Williams, and Wilkins; Baltimore, MD: 2010. McArdle WD, Katch FI, Katch VL.
Fundamentals of Aerospace Medicine, 3rd
edition. Lippincott, Williams, and Wilkins; Baltimore,
MD: 2002. DeHart RL, Davis, JR.
Journal of Strength & Conditioning Research. 2012 May; doi: 10.1519/JSC.0b013e31825d8263
Original Investigation: PDF Only. Strength Training for the Warfighter. Kraemer, William J.;
Szivak, Tunde K.

AFPAM11-419 17 OCTOBER 2014 25
National Strength and Conditioning Association, Essentials of Strength Training and
Conditioning. 3rd
Ed: 2008. Baechle TR, Earle RW.
Technical Manual 14P3-6-121. Anti-G Cutaway Garment Type CSU-13B/P. 31 October 1998,
incorporating Change 25, 24 Sep 12.
Technical Manual 14P3-6-141. Anti-G, Trousers, Pneumatic Type CSU-22/P and CSU-23/P. 30
January 2003, incorporating Change 5, 1 Jun 12.
USAFSAM-SR-88-1. March 1988. Physical Fitness To Enhance Aircrew G Tolerance. Burton
RR, Crisman RP.
Adopted Forms
AF Form 847, Recommendation for Change of Publication
AF Form 1274, Physiological Training
Abbreviations and Acronyms
AP—Aerospace Physiology
AETC—Air Education and Training Command
AFI—Air Force Instruction
AFMS—Air Force Medical Service
AFPD—Air Force Policy Directive
AFRL—Air Force Research Laboratory
AGSM—Anti-G Straining Maneuver
ANG—Air National Guard
AOP—Aerospace and Operational Physiology
AOPTU—Aerospace and Operational Physiology Training Unit
ARC—Air Reserve Component
CC—Commander
CONOPS—Concept of Operations
DNIF—Duty Not Involving Flying
DV—Distinguished Visitor
ETCA—Education and Training Course Announcement
FACP—Fighter Aircrew Conditioning Program
FS—Flight Surgeon
FTU—Formal Training Unit
HQ—Headquarters
IFF—Introduction to Fighter Fundamentals

26 AFPAM11-419 17 OCTOBER 2014
MAJCOM—Major Command
MDS—Mission Design Series
NVG—Night Vision Goggles
OG—Operations Group
OPR—Office of Primary Responsibility
PC—Physical Conditioning
PCS—Permanent Change of Station
SA—Situational Awareness
SD—Spatial Disorientation
UFT—Undergraduate Flying Training
WG—Wing

AFPAM11-419 17 OCTOBER 2014 27
Attachment 2
PHYSICAL FITNESS PROGRAM TO ENHANCE AIRCREW G-TOLERANCE
A2.1. Introduction. Physical fitness is an integral part of successfully flying high-G aircraft.
This attachment contains recommendations to improve G-tolerance by effective PC.
A2.1.1. Purpose of a PC Program. Successful control of today’s modern fighters depends
on your ability to overcome the high G-forces generated by increasingly capable aircraft.
This attachment contains general recommendations for establishing a personal PC program to
enhance your G-tolerance and general physical performance under G. There isn’t one perfect
program for every high-G aircrew. Yet there are some general principles recognized by
strength and conditioning authorities that may improve performance in the high-G realm.
Foundational abilities in full-body strength, power, endurance and mobility will serve high-G
aircrew well. Additionally, there are specific attributes related to AGSM performance that
can be trained. For example, high-intensity lower body/core activities executed in an interval
training pattern mimic the demands imposed by multiple high-G engagements.
A2.2. PC to Improve G-Tolerance. Being in good physical condition holds definite
advantages for performance in the cockpit, especially G-tolerance. Increased muscular strength
and endurance allow aircrew to efficiently perform the AGSM with less relative muscular effort,
therefore less “mental” effort is required. The AGSM expends energy at a rate similar to
sprinting or weight lifting. Some research suggests that high intensity strength training increases
the ability to withstand high G-forces for a longer duration with less fatigue. Additionally, well-
developed aerobic capacity and muscular endurance has been shown to decrease the recovery
time needed between centrifuge training runs. This capacity to recover between engagements is
critical to maintaining an effective AGSM. Additionally, exhaustion of the respiratory muscles
often erodes an individual’s AGSM performance. A well-rounded G-training program will
incorporate elements of strength, power, endurance, work capacity, mobility and flexibility.
A2.3. General Guidelines: Any type of physical training must be preceded by a thorough
warm-up. The goals of the warm-up are to increase the temperature of the muscles and
connective tissues, work the muscles/joints through the range of motion anticipated for the
activity and to prepare the neurological pathways for the impending activity. Proper form can
also be reinforced at this stage. Light load bearing activities such as air squats, push-ups, light
dumb bell shoulder presses, jogging, etc. are advised. Focus on the shoulders, low back and
knees and the muscle groups crossing these joints, as these are the most likely casualties of
insufficient warm-up activities. The minimum time to devote to a proper warm-up is
approximately 5-10 minutes. At least 2-3 warm-up sets are advisable for strength and power
movements and perhaps more if working near 1 repetition max (RM) loads. Post-workout static
stretching of all major muscle groups and joints is advised.
A2.3.1. Strength Training Elements. For the larger, multi-joint exercises such as squat,
dead lift, power clean and bench press, working near 1RM will tend to develop the
neurological adaptations that may produce a more effective AGSM. This also tends to
produce general physical improvements many individuals seek. Strength training intensity is
commonly expressed as a percentage of an individual’s 1RM. For example: 6 sets of 3
repetitions at 90% of 1RM. The percentage is largely utilized to track progress and have an
objective way to track workout loads. For most strength-related training, loads from 70%-

28 AFPAM11-419 17 OCTOBER 2014
100% of 1RM are appropriate. Longer rest periods between sets, on the order of 1 to 5
minutes, are appropriate for strength training activities. At least 48-72 hours recovery is
required between similar types of movements at high loads.
A2.3.2. Power Elements. Exercises executed for power development normally strive to
move moderately-heavy weights in explosive movement patterns. Examples of such
exercises include the Olympic lifts such as the snatch, clean and jerk, power cleans,
plyometrics, etc. They are worthy elements for the high-G aircrews’ workout routine, but
should only be pursued under close supervision of a trained strength and conditioning
professional. Executed with proper form and care, these types of movements are very safe
and will improve overall athleticism and cockpit mobility under G.
A2.3.3. Cardiovascular Training Elements. Cardiovascular training will tax the body’s
ability to uptake oxygen and produce work over an extended period, from approximately 3
minutes to indefinitely. Cardiovascular fitness is commonly described using maximal
oxygen consumption, or VO2 max, which is defined as the maximum amount of oxygen
consumed during each minute of near maximal exercise. Intensity in cardiovascular training
increases VO2 max, or the body’s ability to efficiently transport oxygen to the site of muscular
activity and maximally use cellular machinery to produce physical work. In general, the
higher the intensity, the less time that activity can be maintained. Consider the difference in
run rate between a 1.5 mile max effort pace and a 10 mile run pace. There is a lot of current
evidence to suggest that short duration, high intensity, interval types of training produce most
of the positive adaptations from cardiovascular training without the enormous wear and tear
that longer duration, low intensity cardiovascular training tends to produce. Often, this
method is also more time efficient. Examples could include one type of activity with
programmed short rest periods, like 400m sprints with 1 min between sets. Or circuit
training activities executed over a specified time period or a prescribed number of repetitions
with minimal/no rest periods. These higher intensity, shorter duration activities with short
rest periods are likely very beneficial for AGSM performance. Longer, slower, lower
intensity activities such as long runs, bike rides, sports etc. are fine occasionally or a couple
times per week. But excessive pursuance of this element will definitely impede strength and
power gains.
A2.3.4. High Intensity Circuit Elements. There is a nearly infinite number of ways to
combine exercises in a high intensity circuit fashion, lasting anywhere from a few minutes to
perhaps 45 minutes. Once a solid strength & conditioning foundation is set, the high-G
aircrew is advised to incorporate these types of workouts 2-3 times per week. However, they
can be highly taxing on the body and great care should be given when using them. High rep
counts of moderate loads can be especially taxing. Additionally, technique can tend to get
sloppy when complex exercises are completed in a fatigued state. Use caution and never
continue to perform movements if proper technique cannot be maintained.
A2.3.5. Evaluating 1 RM. 1RM assessment is a good method to calculate and monitor
strength/power loads for workouts and is usually most appropriate for multi-joint movements
like squat, bench press or dead lift. 1RM is a load that can be completed once with proper
technique and full range of motion. 1RM should occasionally be assessed to track progress.
1RM assessment should only be pursued under the supervision of trained personnel, as
improper form or technique can increase the risk of injury. If training experience is very low,
1RM testing is likely ill-advised. There are methods to estimate 1RM by conducting 5-

AFPAM11-419 17 OCTOBER 2014 29
10RM assessments. Again, a trained professional can aid in this calculation. Once loads
become noticeably lighter or additional reps can be achieved compared to previous results,
addition of 5-10 pounds for upper body movements and 10-20 pounds for lower body
movements is appropriate.
A2.4. Specific Exercises. There are several broad groups of exercises to include in a prudent
high-G training program. Additionally, there are many variations as well as a lot of creative
movements to add variety and reduce boredom during training. In general, the best game plan is
to train for movements, not specific muscles. The human system rarely operates via single joint
movements, i.e. bar bell curls. It is also better to rely on free weights and body-weight types of
movements over exercise machines. Below are some examples of good fundamental movements
to include in a program, but this list should not be considered comprehensive. For new or
complex movements, seek guidance from strength and conditioning professionals. Exercise
physiologists, certified personal trainers, and Aerospace & Operational Physiologists are good
starting points.
A2.4.1. Legs/core/low back: Back squats, front squats, overhead squats, dead lifts, step ups,
lunges, back extensions.
A2.4.2. Upper body extension: Overhead presses, pushups, bench press, ring dips, ring
pushups.
A2.4.3. Abdominals: Sit-ups, crunches, planks, GHD (Glute-Hamstring Developer)
A2.4.4. Upper body flexion: Pull-ups, rows, shrugs, power cleans, rope climbs.
A2.4.5. Power movements: Power-cleans, snatches, squat cleans, plyometrics such as box
jumps and jumping rope.
A2.4.6. Neck: Shrugs and upright rows, 4-way neck machine, light resistance bands for neck
flexion, extension and rotation.
A2.5. Cardiovascular Conditioning. Many options exist for cardiovascular training. All the
classic options such as running, biking, swimming, rower machine, stair climbing and jumping
rope are fantastic options alone or when combined in a high intensity circuit workout.
A2.6. Building Exercise Programs. This pamphlet cannot provide the full education needed to
design effective exercise programs. Aircrew interested in a personalized fitness program should
work with experts certified in exercise training. This paragraph provides supplementary
information to aid aircrew members in working with experts to develop personalized programs.
An exercise program is considered comprehensive when it encompasses both the anaerobic and
aerobic needs of the individual as the program pertains to the improvement in their respective
activity performance. Programs should implement specificity, overload, and progression.
Specificity, defines the foundation of the training by determining what type of physical demand
should be imposed, when and how to impose the demand and what the expected resultant
physiological effect of the imposed stress/demand will be. Overload refers to imposing greater
intensity of stressors/demands on the body in an effort to allow the body to build up stress-
adaptive responses of accommodation, then acclimatization. If overload is to be effective, then
progression, a systematic and gradual approach of the application of stress/demand, must be
applied with the goal of increasing long-term adaptations. Programs should be properly
developed using the following step-by-step process.

30 AFPAM11-419 17 OCTOBER 2014
A2.6.1. Step 1 Needs Analysis: determination of the unique characteristic of the physical
activity through biomechanical, physiological, and injury analyses. Other variables to
evaluate are current and projected training status, physical evaluation methods, and primary
and secondary training goals with defined objectives.
A2.6.1.1. Biomechanical analysis refers to muscular, skeletal and motor skill patterns
A2.6.1.2. Physiological analysis refers to anaerobic and aerobic component prioritization
A2.6.1.3. Injury analysis refers to identification of common musculoskeletal injury sites
with the intent of risk reduction and injury prevention.
A2.6.2. Step 2 Exercise Selection: In order to select appropriate exercises to compliment the
physical activity the nature of the exercises, the musculoskeletal demands of the activity, the
technical training experience of the occupational athlete, the available facilities and schedule
time, all must be understood. Establish core exercises (e.g. multi-joint, multi-muscle, large
primary muscles) as the primary priority with assistive exercise (e.g. single-joint, small-
muscle, smaller stabilization muscles) as secondary importance; consider the movement of
the activity and determine the exercise-specificity of the exercises selected with a balance
placed upon agonist and antagonist movements for muscle balance.
A2.6.3. Step 3 Training Frequency: Common training frequency is a week period when
creating an exercise program. Factors that affect the frequency of training consist of the
athlete’s current training status, exercise loads and type of exercises, and other schedule
variables (e.g. flying, education & training, etc.).
A2.6.4. Step 4 Exercise Order: The sequence of a training program’s exercises for a daily
workout start with the athlete’s maximal, most forceful or exhaustive exercises for that
workout. Four common methods for exercise selection can be used; 1) Power, other core,
then assistive exercises, 2)upper/lower body alternation, 3) push/pull alternation, and 4)
superset & compound sets.
A2.6.5. Step 5 Training Load & Repetitions: Generally, mechanical work is the quantified
product of the load of work multiplied by the repetition of work performed. Load can be
determined by multiplying a percentage of a maximal effort/established personal best weight
or time. There exist two common methods for the determination of an individual’s load
maximum; 1-Repetition Maximum (1RM) and Multiple Repetition Maximum (MRM).
Aircrews should use the MRM method to establish training loads due to specificity of
activity and safety/risk assessment.
A2.6.6. Step 6 Volume: Training volume can be calculated from load by multiplying the
amount of sets the load is performed and how many repetitions will be performed within
each set.
A2.6.7. Step 7 Rest Periods: Periods of time between sets and exercises within a workout
session will constitute rest periods or inter-set periods and can provide parameters for
workout work-to-rest (work/rest) ratios. Higher intensity sets or sessions require longer
work/rest periods. As the exercise intensity lowers, the rest period ratio should also decrease
during circuit training workout sessions. As stated previously, an exercise programs must
take a scientifically based, methodological/systematic approach to applying the demands of
physical training to the athlete in order for them to reap the positive benefits of an enhanced

AFPAM11-419 17 OCTOBER 2014 31
human performance for their respective activity. For high-G aircrew, the demand of the
AGSM is short-term, high-intensity anaerobic bout of physical effort interspersed with lower
intensity, moderate times of rest periods. The strength and conditioning specialist will need
to use the aforementioned fact as the foundation in the creation of exercise programs that
consists of anaerobic and aerobic components.

Attachment 3
SAMPLE WORKOUT PLANS
A3.1. Sample Workout Plan #1. Weight loads not prescribed, based on individual ability. This would be an advanced routine,
appropriate for someone in very good condition and having mastered all technically complex movements.

AFPAM11-419 17 OCTOBER 2014 33
Figure A3.1. Sample Workout Plan #1.

34 AFPAM11-419 17 OCTOBER 2014
Figure A3.2. Sample Workout #2 Training Legend.

AFPAM11-419 17 OCTOBER 2014 35
Figure A3.3. Sample Workout Plan #2 (use legend at Figure A3.2).





























