Embed Size (px)
Citation preview

By Nicole Stevens

Human fetal circulation works differently to extrauterine circulation, and there are 3 key differences:The presence of a placenta in the “circuit”
Blood flowing through the foramen ovale between the right atrium and the left atrium
Blood bypassing through the ductus arteriosus from the pulmonary artery to the aorta
There are also many other embryonic circulatory vessels; these are slowly obliterated and remain in the adult only as fibrous remants

ROLES OF THE PLACENTA: Secretes endocrine hormones which increase
through the pregnancy, causing progressive changes in maternal metabolism.; this creates an increase in the maternal glucose and amino acids available to the foetus
Facilitates the transfer of these (and other) essential nutrients from the maternal to the fetal circulation, and conversely, of metabolic wastes from the fetal to the maternal system
Adequate maternal and fetal blood flow through the placenta is vital through the pregnancy to maintain healthy growth and development of the fetus

ROLES OF THE PLACENTA cont..: Exchange of CO2 and O2 also occurs in the placenta The maternal and fetal circulations are not joined,
instead, the respiratory gases, carbohydrates, lipids, vitamins, minerals and amino acids diffuse across the placental membrane
The placenta is a low resistant component of fetal circulation
The fetal heart generates the force to pump blood through the umbilical arteries (2) to the placenta
Blood returns from the placenta to the fetus via the umbilical vein

FORAMEN OVALE (FO): Connects the right atrium to the left atrium; it
permits oxygenated blood to bypass the right ventricle and pulmonary circuit and go directly to the left atrium
A “flap” known as the septum primum is located on the left side of the atrial septum, it is pushed open by blood flow going from right to left, but any flow going from left to right will push it closed (this prevents blood flowing in the wrong direction)

DUCTUS ARTERIOSUS: Connects the pulmonary trunk to the descending
aorta Allows bypassing of the non-functioning lungs Returns blood to the placenta for oxygenation Systemic circulation returning to the heart goes
into the right atrium then the right ventricle, this is pumped into the pulmonary artery; blood wants to travel on the path of least resistence, there is high resistence in the lungs of the fetus and low resistence in systemic circulation, the blood will prefer to flow across the ductus arteriosus into the aorta, rather than down the right and left pulmonary arteries to the lungs.

THE PATH: (may help to track it on your heart drawings)
Deoxygenated fetal blood is carried to the placenta by the two umbilical arteries; these arise from the internal iliac arteries
Gas exchange occurs in the placenta Oxygenated blood travels from the placenta via
the umbilical vein and enters the IVC About 50% of this passes through the liver and
the rest bypasses the liver via the ductus venosus; the IVC also drains blood returning from the lower part of the body

THE PATH cont.. On reaching the heart at the right atrium the blood
is divided into 2 streams (of unequal sizes); the larger stream is shunted to the left atrium through the FO,the smaller stream joins the flow of blood returning from the SVC (returning from the myocardium and upper body)
The blood that goes through the FO ends up in the left ventricle and is ejected into the aorta
The blood that goes into the right ventricle is pumped into the pulmonary artery but most will go across the DA and end up in the aorta as well

Most of the relatively O2 rich blood that comes up the ascending aorta from the left ventricle will end up at the head and upper extremeties (the vessels feeding these areas come off the aorta prior to the DA union point)
The patency of the DA is maintained by the relatively low O2 tension and the vasodilating effects of prostaglandin E2 (maternal hormone coming through the placenta)

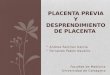
FETAL CIRCULATION

At birth, the circulation of fetal blood through the placenta ceases; the umbilical vessels are obliterated when the cord is clamped externally
There is a reduction in blood flow through the IVC and the ductus venosus (this will close within 3 – 10 days)
There is a dramatic fall in PVR with lung expansion (opening up of pulmonary vessels)
A reduction in hypoxic pulmonary vaso-constriction and stimulation of pulmonary stretch receptors contribute to this process

The rise in pulmonary blood flow leads to an increase in blood returning to the left atrium; the left atrial pressure therefore exceeds the right atrial pressure; this reversal of pressure causes the flap of the FO to be pushed closed (the initial closure occurs within minutes, anatomical closure takes several days
The ductus arteriosus consticts due to the high partial pressure of oxygen; this process is usually complete 2 days after birth (we will discuss the failure of this to occur later)

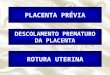
NEONATALCIRCULATION

In some circumstances a neonates circulation may revert back to be fetal-like; this state is known as persistent foetal circulation (PFC)
A neonates pulmonary arterioles remain very reactive and will constrict in response to: hypoxia, hypercarbia, acidosis and cold; this can lead to an increase in PVR, which favours right to left shunting through the FO and ductus arteriosus
The result of this is the neonate reverting to PFC, with one major difference – there is no placenta to provide oxygenation; a vicious cycle of worsening hypoxia and acidosis is then set in motion.

The management of this requires treatment of the underlying causes:
Such as, escalating respiratory support to provide better ventilation
Use of nitric oxide if there is pulmonary hypertension, to aid in dilating the pulmonary vessels
Management of infection with antibiotics Management of thermoregulation

BY: NICOLE STEVENS

Patent Ductus Arteriosus is a functional connection between the pulmonary artery and the descending aorta.
In the fetus the DA allows blood to be diverted away from the pulmonary artery (the high resistance pulmonary circulation) to the descending aorta (the low resistance systemic circulation)
The duct remains open due to the prostaglandin supply coming from the placenta.
The DA protects the lungs from circulatory overload.

After the birth the baby’s lungs expand as they begin to take breaths.
Pulmonary resistance decreases and the oxygen levels in the blood rise causing the DA to constrict.
Sometimes the DA doesn’t constrict and the baby is left with a PDA.
This can be due to lack of oxygen or an increase in the amounts of prostaglandin.
Sometimes the PDA will functionally close but will reopen in response to certain stimuli such as hypercarbia, acidosis, infection, hypoxia and cold

It is approximately 10mm in diameter
Functional closure occurs between 12 hours and 4 days of age in healthy term babies
Structural closure takes between 2 to 6 weeks

It is common in premature infants
Serious concern as the pulmonary artery is not getting enough blood for the lungs to function effectively
It can cause worsening RDS and an escalation in the respiratory support that is required
Diagnosed on ECHO
Treated with Indomethacin and sometimes may require surgical closure (called a PDA ligation)

PDA in the preterm infant: There is nothing wrong with the heart, the PDA just
doesn’t close and usually causes a left to right shunt The tissue is immature; the fetal haemoglobin has a
higher affinity for oxygen (doesn’t release it as easily) The lower the gestational age the greater the risk of
PDA VLBW infants will have up to 50 – 60% chance of a PDA The immature ductal tissue is much less reactive to
oxygen, therefore less likely to readily close in response to the increase in partial pressure of oxygen that occurs after birth

PDA in the term infant: If there is pulmonary hypertension (numerous
causes for this, eg. meconium aspiration, infection) the blood shunts right to left through the PDA
Deoxygenated blood that should be going to the lungs goes back to the body, this causes hypoxia and acidosis, which causes vascular smooth muscle to constrict, and the end result can be persistent fetal circulation (without the presence of placenta for oxygenation)

When trying to determine if shunting of blood is occuring across a PDA you may be asked to measure pre and post ductal oxygen saturations
Pre ductal SaO2 are measured on the right hand/wrist, and post ductal SaO2 can be measured on any of the other limbs, usually a difference of 10% or more is considered significant and may be caused by shunting of blood across a PDA
The arteries that supply part of the brain, and right arm, branch off the aorta prior to where the duct joins it, and the arteries that supply the other limbs branch off after the point where the PDA joins the aorta – hence, the reason we can measure pre and post ductal SaO2 at these points.

Pulmonary oedema Poor perfusion Bounding pulses Swinging saturations Desaturations Renal compromise Heart murmur Congestive cardiac failure Mottled or pale

If a neonate is symptomatic of an existing PDA they may require treatment
Chemical treatment: Indomethacin (usually given IV but oral route can be used, although thought to be not as effective)
(Note: there is currently a world-wide shortage of indomethacin as its production has stopped, in the near future an alternate drug may be used)
If chemical treatment fails surgical treatment may be used: PDA ligation

First line treatment Urea & Creatinine are checked before
commencing Indomethacin to ensure normal renal function before commencement of the drug.
Platelets are also checked to ensure normal range
3 daily doses of 200mcg/kg at 2200hrs Side Effects include impairment of renal
function, reduce platelet aggregation, GI tract bleeding, hypoglycaemia, hyponatreamia, hyperkaleamia and can mask infection.

Monitor urine output Daily Urinalysis BP monitoring Observe for bleeding and or NEC Contraindicated in infants with recent IVH
and NEC

Some cardiac abnormalities are considered “duct-dependent”; these can be cyanotic or acyanotic
Duct-dependent defects can be related to pulmonary flow (for example pulmonary stenosis or pulmonary atresia); or related to systemic flow (for example hyperplastic left heart or transposition of the greater arteries)
If there is a definite or suspected diagnosis of a cardiac abnormality, that is duct dependent, a prostaglandin infusion is the treatment of choice (a synthetic version of the hormone that keeps it open inutero); the use of prostaglandin before further investigations and/or surgery has improved the mortality and morbidity outcomes for these neonates