Embed Size (px)
Citation preview

Time to Implement!Moving Forward with
Reform
By Michael Bertaut, Healthcare Economist and Exchange Coordinator
BCBSLAApril 2013

2
All information in this presentation INCLUDING THE OPINIONS OF THE PRESENTER are solely for illustrative purposes. The information is based on certain assumptions, interpretations, and calculations that are not necessarily accurate with regard to provisions of PPACA, HCERA, HIPAA, COBRA, ERISA, and other rules, regulations, guidance and all other documents issued by relevant state and federal agencies with regard to these laws and any other relevant laws. The information provided should not be considered as legal, financial, accounting, planning, or tax advice. You should consult your attorneys, accountants, and other employees or experts of this type of this type of advice based on their own interpretations, calculations, and determinations of applicable laws, rules, regulations, guidance, and any other documents and information that they determine may be relevant. The authors make guarantees or other representations as to the accuracy or completeness of the data in this presentation.
BCBSLA expressly disclaims any liability for information obtained from use of this presentation by any BCBSLA employee or by any other person. No warranty of any kind is given with regard to the contents of the presentation.
Disclaimer

What Will We Talk About?
New Requirements for Businesses
New Requirements for Health Insurance Companies
New Requirements for Individuals
Financial Impacts of the Act on all stakeholders

4
Yes. The Individual Responsibility Requirement mandates all Americans to have health insurance policy
Starts 1/1/2014 Exemptions for unaffordable
coverage (above 8% of income), certain religious groups, native Americans.
Failure to comply means confiscation of tax refund starting at $95 for first year and rising to $695 or 2.5% of income by 2017.
Do I as an Individual HAVE to have Health Insurance?

5
Exchanges ◦ An online marketplace for health insurance.
Designed to be health-neutral, gender-neutral, and very heavily subsidized by the Federal Government
Medicaid◦ Free Insurance for certain elements of the
population. Louisiana’s Medicaid expansion is still TBD
Employer◦ Employer coverage is still considered to be the
backbone of the health insurance system, albeit with many, many new rules to follow in 2014 and beyond.
Where Do I Get Insurance?

6
WHAT’S THE PLAN?◦ To create a streamlined, easy to use, consumer friendly, health
neutral, gender neutral, FEDERALLY REGULATED market for health insurance.
HOW DOES IT WORK?◦ Designed specifically to remove the 2 biggest barriers to health
insurance: Cost and Health Status, with federal subsidies and no medical questions allowed.
WHEN DOES IT OPEN?◦ 10/1/2013. Closes again on 3/31/2014◦ Subsequent years open enrollment will be about 6 weeks long.
WHAT CAN I BUY THERE?◦ Health, Dental, and Vision insurance from many major carriers.
Each state will have its own unique exchange and product selection.
What’s an Exchange?

Risk Factor
Pre-2014 Post-2014
Rate Changes by
ClassAGE OF
INSUREDRATE MAY VARY UP TO 10X BETWEEN 19 AND
64 YEAR OLD
RATE MAY VARY ONLY 3X
BETWEEN 21 YEAR OLD AND 64
YEAR OLD
YOUNGER
OLDER
GENDER WOMEN CHARGED MORE DURING
CHILDBEARING YEARS. MEN CHARGED MORE
POST AGE 55
GENDER MUST BE IGNORED FOR RATE SETTING
MEN
WOMEN
HEALTH STATUS
MEDICAL RECORDS, CLAIMS DATA,
PHARMACY RECORDS, ALL USED TO
DETERMINE RATE OR OUTRIGHT EXCLUDE
APPLICANT FROM COVERAGE
HEALTH INFORMATION CANNOT ALTER
RATES OR EXCLUDE ANYONE
HEALTHY
SICK
From this grid we can see the big winners are older women with health conditions, and the biggest losers the young, healthy males.
How Will That Insurance Be Priced?

0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60 63$100.00
$200.00
$300.00
$400.00
$500.00
$600.00
$700.00
$800.00
Age Rating Effects: Sample Current Moving to 3:1, Remove Gender
PPACA Age CurveMale CurrentFemale Current
Age of Member
Standard Premium
Dramatic decrease in
Newborn Rates (-67%)
Males Age 22-42 get
rate increases up
to 38%!
Females get rate decreases at ages 22 through 54, peaking at (-35%) at age 40.
Males get small rate decreases at ages 56-64, peaking at (-11%)
9
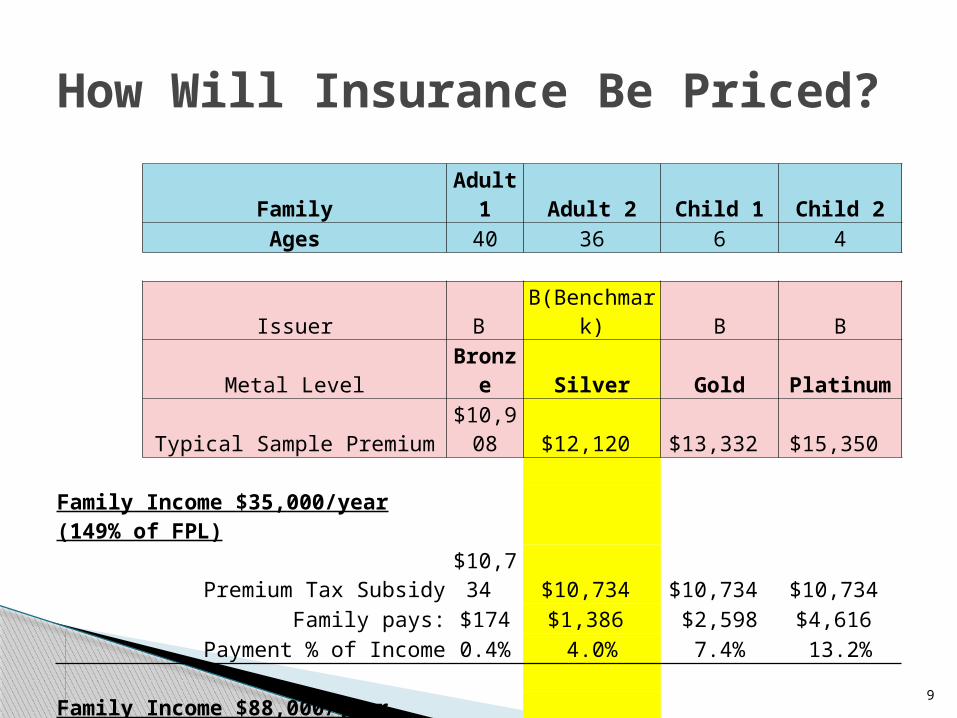
Family Adult 1 Adult 2 Child 1 Child 2Ages 40 36 6 4
Issuer B B(Benchmark) B BMetal Level Bronze Silver Gold Platinum
Typical Sample Premium $10,908 $12,120 $13,332 $15,350
Family Income $35,000/year (149% of FPL)Premium Tax Subsidy$10,734 $10,734 $10,734 $10,734
Family pays: $174 $1,386 $2,598 $4,616 Payment % of Income 0.4% 4.0% 7.4% 13.2%
Family Income $88,000/year (375% of FPL)Premium Tax Subsidy $3,760 $3,760 $3,760 $3,760
Family pays: $7,148 $8,360 $9,572 $11,590 Payment % of Income 8.1% 9.5% 10.9% 13.2%
How Will Insurance Be Priced?

Incarcerated. Income above 400% of FPL. Offered coverage at work that is affordable
and at least 60% AV. Medicaid or CHIP eligible (income <138% fpl
in states that have agreed to expand). Claimed as a dependant on someone’s taxes. Unable to attest to residency in a single
state. In the country unlawfully.
10
Who Can’t Get Help?
Once a Subsidy is Accepted, Individual MUST file Tax Return for
That year.

Children (LIH)713k58%
Blind/ Disabled, 160k13%
Pregnant Females, 196k16%
Dual Eligibles, 161k 13%
Would Add new Category of Low Income Healthy
Adults Up to 138% of FPLPotentially 550k new
What About Medicaid? Can I qualify for Free Insurance?


Who Gets Left Out?
The Healthcare Income Continuum (PPACA)
PPACA when fully enforced provides coverage and assistance for most Americans from 0 to 400% of Federal Poverty level Income
Coverage Gap
Without Medicaid expansion Louisiana will have no insurance help for citizens between 11% and 100% of FPL unless they
have employer coverage.
Around 200,000 people considered “Working Poor” will be without insurance.
0-11% Existing Medicaid
11% to 138% New Medicaid
Expansion139% to 400% Exchange
Subsidy Eligible
401% of FPL and above, you are on your own!
Federal Poverty Level Income0%

Who Pays? Small Group Rating Changes (2-50)
Minimum2x Minimum
Average Rate$300 $400$200
A$225
B$250
C$275
D$300
E$325
F$350
G$375
Today, State Law allows a 200% Rate Spread in Small Group Rates
In 2014, no Underwriting is
allowed in Groups 2-50
New MaxNew Min
+38%!
-19%!

15
15
Should Louisiana Expand Medicaid?
Yes EXPAND! No, Don’t EXPAND!
100% FMAP for First 3 years, settling at 90% FMAP going forward.
DiSH money reduced by 50% by 2016, eventually eliminated
PPACA built with expansion in mind, covers working poor.
500,000+ will get access to no-premium health insurance
Fed does not fund administration of new population
La. Budget already $1.0B in the red
90% match may not be permanent
180k+ of expansion population already has private insurance.
Another 90k will be Exchange eligible.
Medical Capacity?

How many benefit eligible Employees do I have?
Am I an Applicable Large Employer (ALE)? ALE Yes, or No, What do I do? To be or not to be Grandfathered?
As an Employer, What 4 Questions Must I Answer?

Any employee who averaged 30 hours of service per week or more in the previous look-back period (3 to 12 months.)
Any new hire who, after 90 days, is REASONABLY EXPECTED to work more than 30 hours/week
If a REASONABLY EXPECTED determination cannot be made after 90 days, then another 90 day period may be used to make the call.
If eligibility determination is made, and then hours change, coverage must continue for the LONGER of the look-back period or 6 months.
Who is benefit eligble?

FOR THE ALE COMPUTATION, the common law definition of employee must be used:
“Under common-law rules, anyone who performs services for you is your employee if you can control what will be done and how it will be done. This is so even when you give the employee freedom of action. What matters is that you have the right to control the details of how the services are performed.” (www.irs.gov)
What is a Common Law Employee?

Month Benefit Eligible
Common Law Hours
/120 FTE Total FTE AVERAGE
JAN 2013 22 3300 27.5 49.5
FEB 2013 23 2800 23.3 46.3
MAR 2013 23 3250 27.1 50.1
APR 2013 23 3450 28.8 51.8
MAY 2013 24 3105 25.9 49.9
JUNE 2013
22 3271 27.3 49.3
JULY 2013 23 3655 30.5 53.5
AUG 2013 24 3705 30.9 54.9
SEPT 2013
25 3000 25.0 50.0
OCT 2013 26 3800 31.7 57.7
NOV 2013 27 3950 32.9 59.9
DEC 2013 30 4250 35.4 65.4 53
How Do I Know if I have to Provide Coverage?Controlled Groups and Associated Groups Must
be COMBINED for this computation!!!

No obligations to provide affordable coverage
No obligations to provide valuable coverage
No obligations to offer coverage
No danger of fines under 4980H
Note: ANY GROUP may offer affordable coverage and lock their employees out of Advanced Tax Credits in the Exchange.
Ok, I’m not an ALE, what now?
21
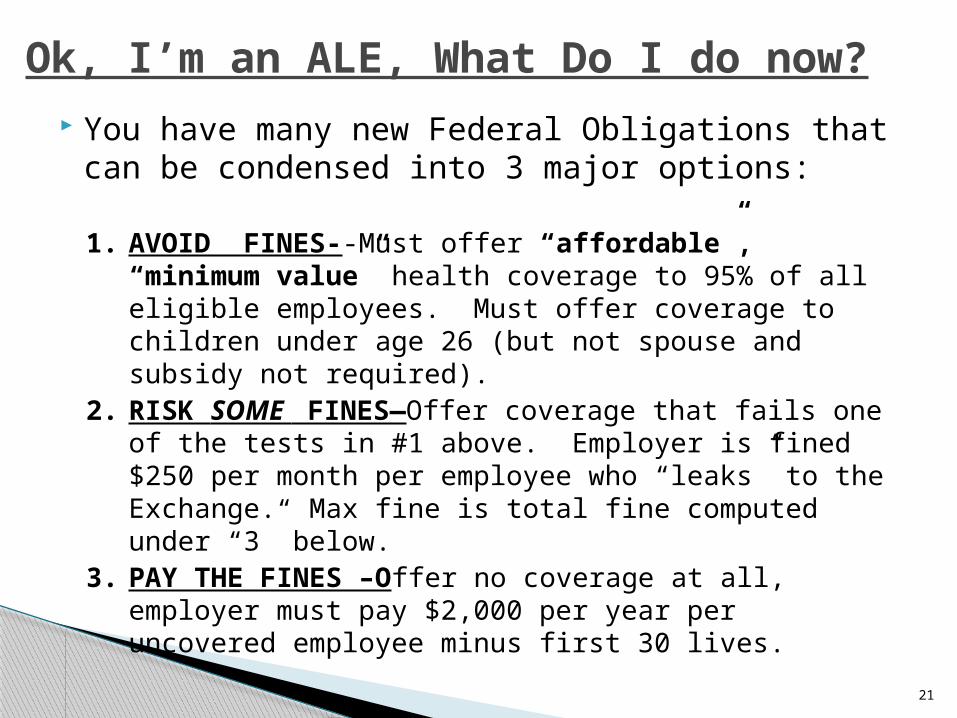
You have many new Federal Obligations that can be condensed into 3 major options:
1. AVOID FINES--Must offer “affordable”, “minimum value” health coverage to 95% of all eligible employees. Must offer coverage to children under age 26 (but not spouse and subsidy not required).
2. RISK SOME FINES—Offer coverage that fails one of the tests in #1 above. Employer is fined $250 per month per employee who “leaks” to the Exchange. Max fine is total fine computed under “3” below.
3. PAY THE FINES –Offer no coverage at all, employer must pay $2,000 per year per uncovered employee minus first 30 lives.
Ok, I’m an ALE, What Do I do now?

Federal Poverty Line:◦ Use 100% of FPL x 9.5% = affordable premium for all
employees.◦ In 2012, would be $11,170 x 9.5% = $1,061.15
Rate of Pay:◦ Use hourly rate times 130/month to determine wages x 9.5% to
compare to premium.◦ At $10/hour, $1,300/month x 12 x 9.5% = $1,482.00
9.5% of Employee Box 1 W-2 income in premiums for employee-only coverage. ◦ Determined at end of calendar year, and on an employee-by-
employee basis.◦ Partial-year adjustments allowed for new employees who work
part of a year.◦ At $20,800/year ($10/hr, 40 hrs/week) = $1,976.00
What Does “Affordable” Mean?

By 2015, the IRS will have the ability to match W-2’s issued, to taxpayers, who received Advanced Tax Credits (ATC) on the Exchange in 2014.
They can then contact employers with a list, and a bill for $250 per employee per month they received an ATC ($3,000/year!)
Employers will have just three ways to defend themselves from these fines.
Why Answer the 4 Questions?Audit Defense: 2015

Prove you are NOT AN ALE Prove the employee in
question was never benefit eligible when he worked for your firm
Prove the employee in question was offered an insurance plan that met the federal definitions of affordability, and offered at least 60% AV.
How to Defend Against Fines listed in section 4980h a) and b)!
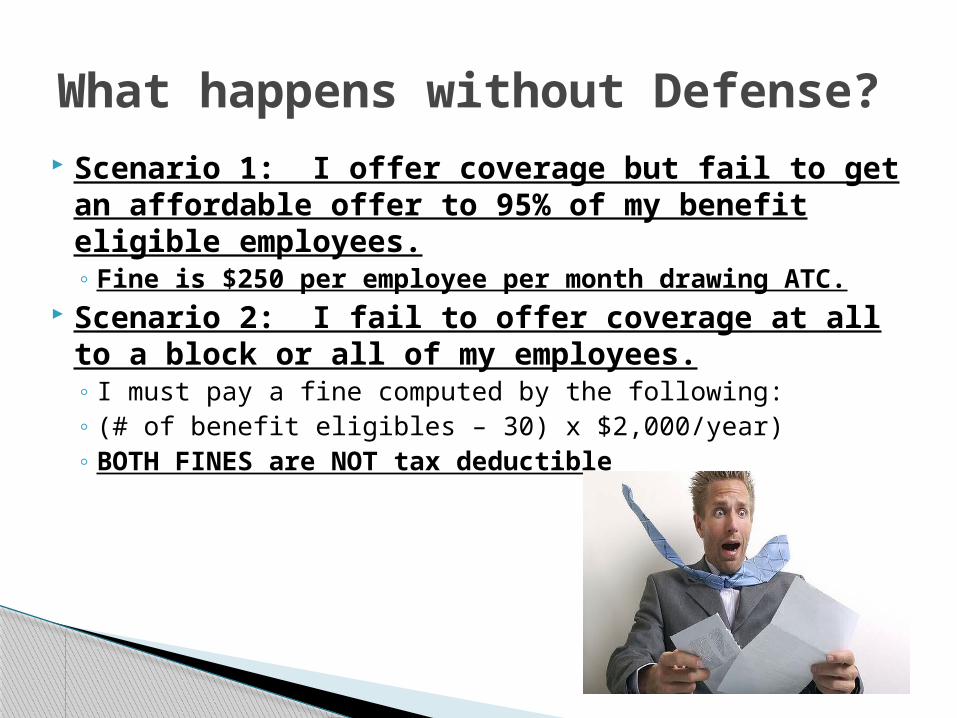
Scenario 1: I offer coverage but fail to get an affordable offer to 95% of my benefit eligible employees.◦ Fine is $250 per employee per month drawing ATC.
Scenario 2: I fail to offer coverage at all to a block or all of my employees.◦ I must pay a fine computed by the following:◦ (# of benefit eligibles – 30) x $2,000/year)◦ BOTH FINES are NOT tax deductible
What happens without Defense?

In general, an ALE must comply with the new rules or face fines by his RENEWAL DATE in 2014, not necessarily 1/1/2014
BUT……
If a group today has a fiscal year plan, and offers it to less than 33% of their employees (part timers AND full timers) or currently cover less than 25% of employees, then they MUST comply with the new ALE standards for affordability/actuarial value/offer to 95%
or fines will start on 1/1/2014, not on their renewal date.
When do ALE’s have to comply?
Grandfathering: Current Benefits to Groups
“You’re Darn Tootin’ Listen to your Grandfather!!”
• Not required to add USPTF Schedule B Tests and screenings to the Plan at zero dollar• Not required to add new women’s coverage to the Plan at zero dollar • Not required to add new coverage for FDA clinical experimental trials • Not required to reimburse ER docs at higher rates, especially out of network docs• Will not be charged transitional reinsurance fees• Will be pooled for rates (2-50) with much healthier groups • Avoid sharing cost of exchange fee on premiums.• Will not be subject to rate compression due to Age Rating, or dissolution of State UW Laws (+40% to -18%)

Invited comments on Staffing Services, rule not finalized. ALE computation paramount.
ANTI-ABUSE rules already being considered:◦ No employer-owned staffing service splits
allowed.◦ “Further guidance is forthcoming”
Staffing Services Rules (so far)

All Individual and Small Group Plans (2-50 lives) MUST match the Benchmark Essential Health Benefits Plan in breadth of coverage.
For 2014/15, in Louisiana, the Benchmark will be the coverage offered in
BLUE CROSS GROUPCARE PPO on 12/31/2011◦ This is a very rich plan. Includes pregnancy
coverage on all members, mental/nervous/ autism spectrum disorder, and a very wide formulary.
What Medical Services Must Be Covered?

Self-funded plans MUST remove all $ limits on any medical coverage considered “essential”.
Self-funded plan MUST comply with mental/nervous parity or cover no MN at all.
Self-funded plans MAY use visit limits on EHB’s to manage costs, but not $ limits
No lifetime OR annual $ limits on EHB’s and “near-EHB’s”
What Services Must Be Covered?: Self Funded

31
Applies to all Non-GF Groups save Churches Begins with renewals 8/1/2012 Services are Free to Insured Includes:
◦ FDA Approved Contraceptive Methods: “Morning After” Pill Tubal Ligation All (generic) pills, IUD’s, other methods
◦ Screening for gestational diabetes◦ HPV DNA Testing (women over 30)◦ STD counseling◦ HIV screening and counseling◦ Breastfeeding “support”, supplies, counseling◦ Domestic violence screening and counseling
Coverage Example:New Women’s Coverages
How Much is All this Going to Cost?
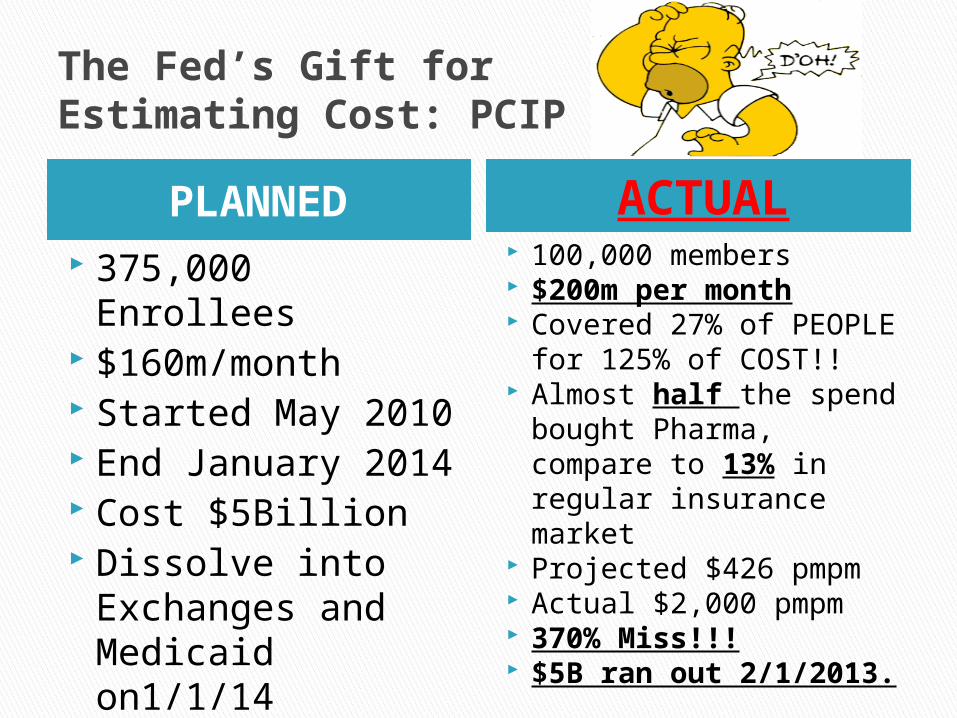
The Fed’s Gift for Estimating Cost: PCIP
PLANNED ACTUAL 375,000 Enrollees $160m/month Started May 2010 End January 2014 Cost $5Billion Dissolve into
Exchanges and Medicaid on1/1/14
100,000 members $200m per month Covered 27% of PEOPLE
for 125% of COST!! Almost half the spend
bought Pharma, compare to 13% in regular insurance market
Projected $426 pmpm Actual $2,000 pmpm 370% Miss!!! $5B ran out 2/1/2013.
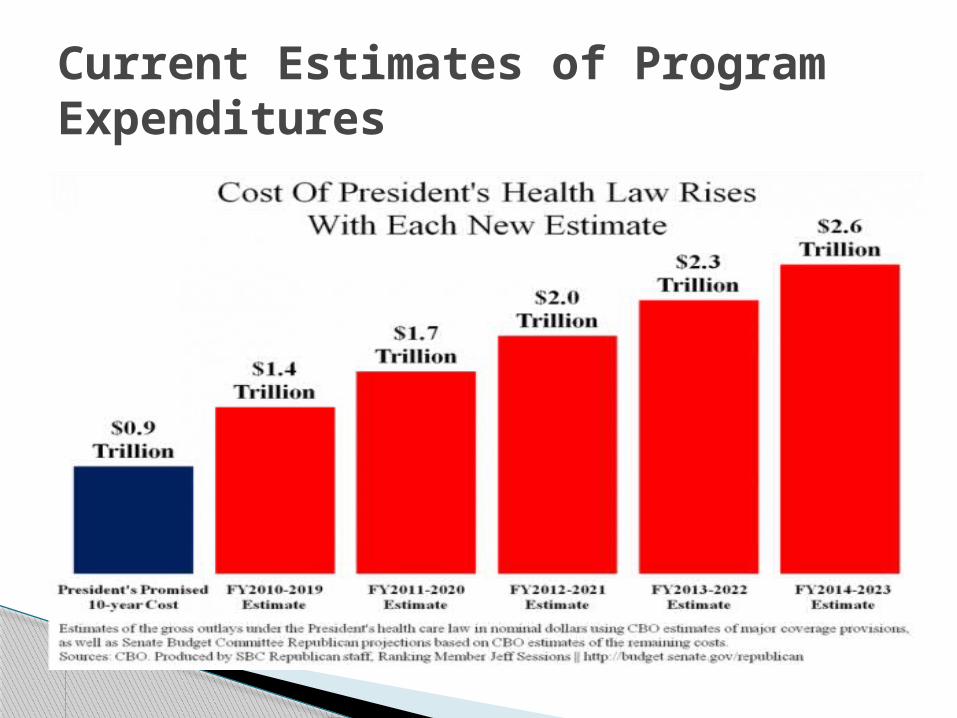
Current Estimates of Program Expenditures

PPACA requires insurance carriers and fully insured groups to make “contributions” to support subsidies on the Exchange.
Self-Funded Groups have a separate fee, $63/member/year.
Note that the effect of this new “fee” is enhanced in rates because it is not a deductible business expense.
Who Pays? The Carrier TaxYEA
RTAX($B)
BCBSLA($M)
Base Rate
Increase
2014 $8.0 $36.3 2.5%
2015 $11.3 $51.2 3.5%
2016 $11.3 $55.8 3.5%
2017 $13.9 $68.6 4.3%
2018 $14.3 $71.7 4.5%
2019
$14.3+ Premium Inflation
Plus Premium Inflation
Plus Premium Inflation

36
Who Pays? Rebates
All companies must operate three separate pools of business by state.
Each pool must hit targeted Medical Loss Ratio or higher
If Medical expenses don’t reach threshold, excess profits must be converted to cash and rebated to pool
BCBSLA Pools (6) are:◦ Individual—80%◦ Group <100--80%
◦ Group >100--85%◦ 1 Each for Blue &
HMO
Company La. Rebates
UHC $1,624,577
Humana $1,356,720
Golden Rule $884,735
Time Insurance $131,715
MEGA Life $114,249
Coventry $0
BCBSLA $0

37
NFP Carriers Already Comply with MLR Requirements
BCBSLA Audited Financial Results FY 2011National Averages From NIHCMF 2010 Update (2011)
31¢Hospital
30¢Physician
and Clinical Services
10¢Admin
Cost Including Taxes,
Commissions
13¢Prescription
Drugs
6¢Dental
Services
2¢ Other
ProfessionalServices
1¢NursingHome
2¢Home Health Care
$925M; 37%
$775M; 31%
$357M; 17%
In 2011, BCBSLA collected $2.5B in risk premiums,
broken out like this:
$425M; 15%
3¢Future Claims
Reserves/Profits
NATIONAL
AVERAGES
85% of Premiums Went to Medical in 20116% Salaries/Admin
5% Commissions
3% Reserves
1% Taxes

PPACA established Federal rate audit authority and responsibility given to CCIIO
Criteria established for “effective” process
9 states (including Louisiana) not effective today
Louisiana carriers will trigger federal audit if any pool increase reaches 10%.
Audit has no authority other than to publicize the “reasonableness” of the rate increase
Attempt to regulate rates through “bad press”
Effective Rate Review/Approval

Historically Higher Populations of the Government-Insured mean higher premiums
124%122%
118% 116% 115% 116% 117%119%
122%
129% 129%133% 131% 132%
99%104% 102% 100% 99% 98% 98%
95%92% 92% 91% 91% 92% 91%
94% 95% 96% 97% 96% 95% 96% 96%92%
90%87% 88% 88%
86%
131%
102%
87%80%
100%
120%
140%
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009*
Paym
enr-t
o-co
st R
atio
Private Payers Medicare Medicaid
39
Note: Payment-to-cost ratios indicate the degree to which payments from each payer covers the costs of treating that provider’s patients. Data are for community hospitals and cover all hospital services. Imputed values were used for missing data (about 35% of observations). Most Medicaid managed care patients are included in the private payers’ category.Source: Adapted from the American Hospital Association and Avalere Health TrendWatch Chartbook 2007: Trends Affecting Hospitals and Health Systems
Hospital Payment-to-cost Ratios for Medicare, Medicaid and Private Payers
1995-2009
Break Even (Payment = Cost)
“Our research shows 87% of hospitals nationwide either lose money or break even treating Medicare Patients. Of the 13% that don’t lose money the average profit margin is 3%.” John Whittlesey, Healthcare Management Council 2010
SGR Limits Enacted

Michael R. BertautHealthcare Economist
LINKED-IN Recommendations WELCOME!!!
Office: 225-297-2719Cell: 225-573-2092
40