Embed Size (px)
Citation preview

HEART FAILUREBy Dr. Figgins & Dr. Gausden

HEART FAILURE IS….
Clinical syndrome resulting from inadequate cardiac output for the body’s needs.
THREE COMPONENTS…
Left heart failure
Right heart failure
Congestive cardiac failure
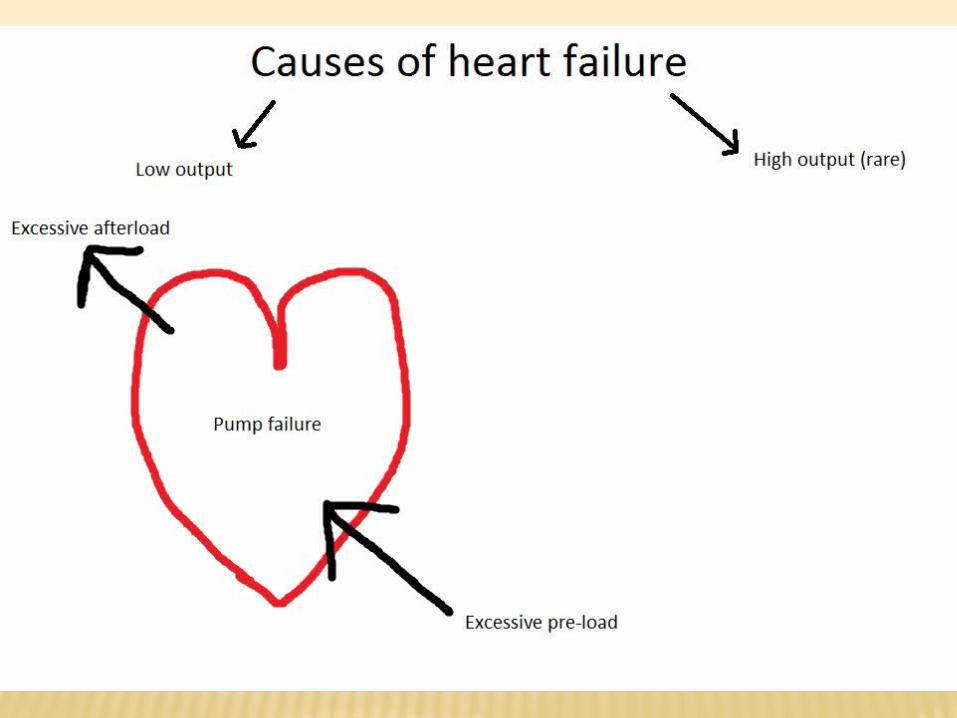

Low output
• Excessive pre-load
• Pump failure
Heart muscle disease
Restricted filling
Inadequate heart rate
Negatively inotropic drugs
• Excessive afterload
High output (rare)
Isolated RHF
PATHOPHYSIOLOGY
Inadequate CO stimulates compensatory mechanisms resembling response to hypovolaemia Initially beneficial, becoming maladaptive
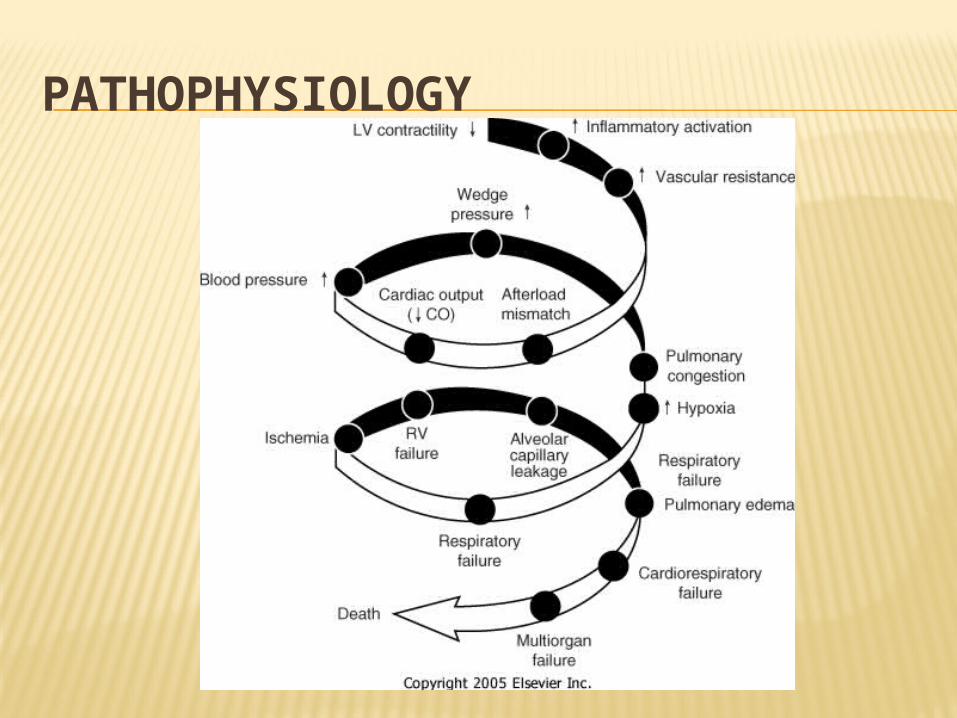
PATHOPHYSIOLOGY

DECOMPENSATE HEART FAILURE
Arrhythmias (e.g. AF) Drug issues (e.g. non-compliance) Anaemia Infection (pneumonia, UTI) Thyroid disease

LEFT HEART FAILURE
Symptoms?
Signs?
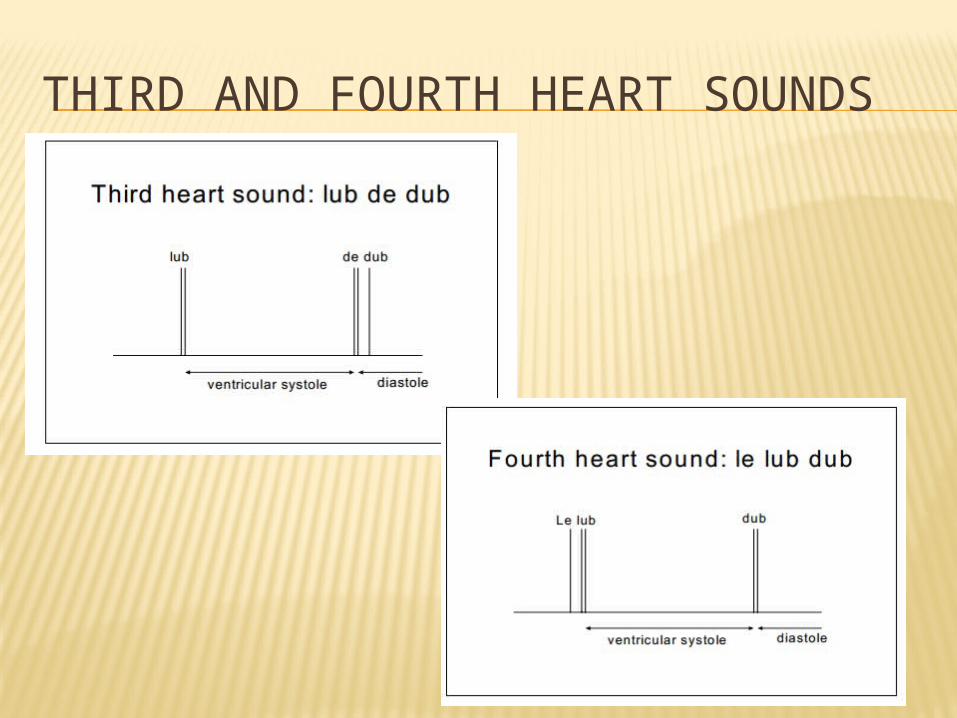
THIRD AND FOURTH HEART SOUNDS
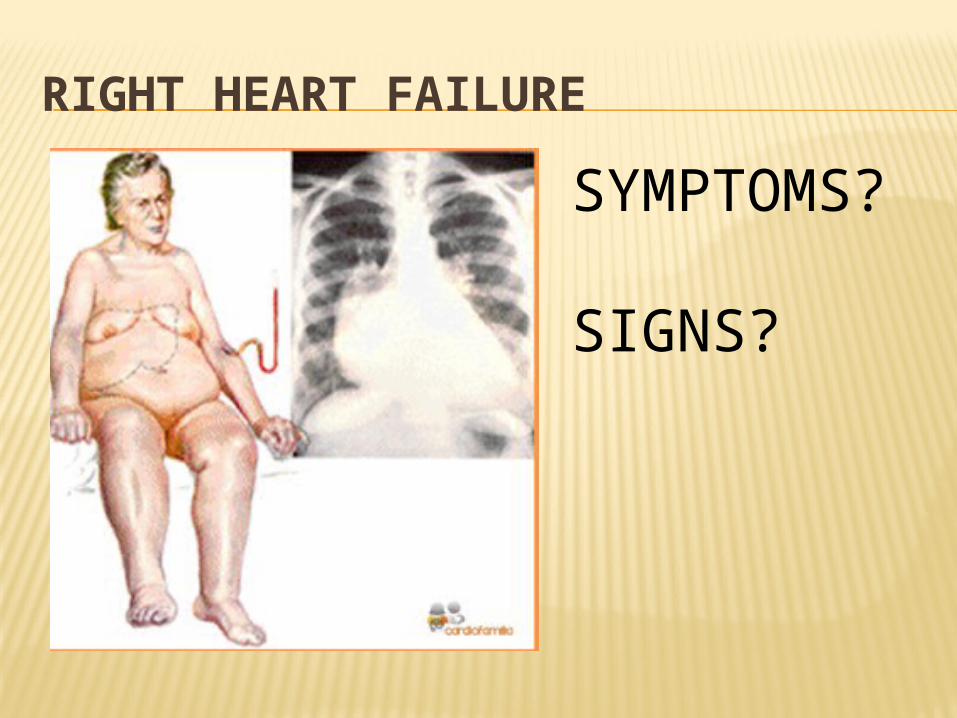
RIGHT HEART FAILURE
SYMPTOMS?
SIGNS?

New York heart failure classificationI = Cardiac disease but NO SYMPTOMS in ordinary physical activity
II = MILD SYMPTOMS and slight limitation during ordinary physical activity
III = Marked limitation in activity due to symptoms during LESS-THAN-ORDINARY ACTIVITY
IV = Severe limitations. Experiences symptoms at even AT REST
INVESTIGATIONS
BEDSIDE TESTS
BLOOD TESTS
IMAGING
SPECIAL TESTS

BNP
Protein secreted from ventricles of the heart
In response to overstretching of cardiomyocytes
High NEGATIVE predictive value (98%)
Used to RULE OUT heart failure, not rule in
Non-specific

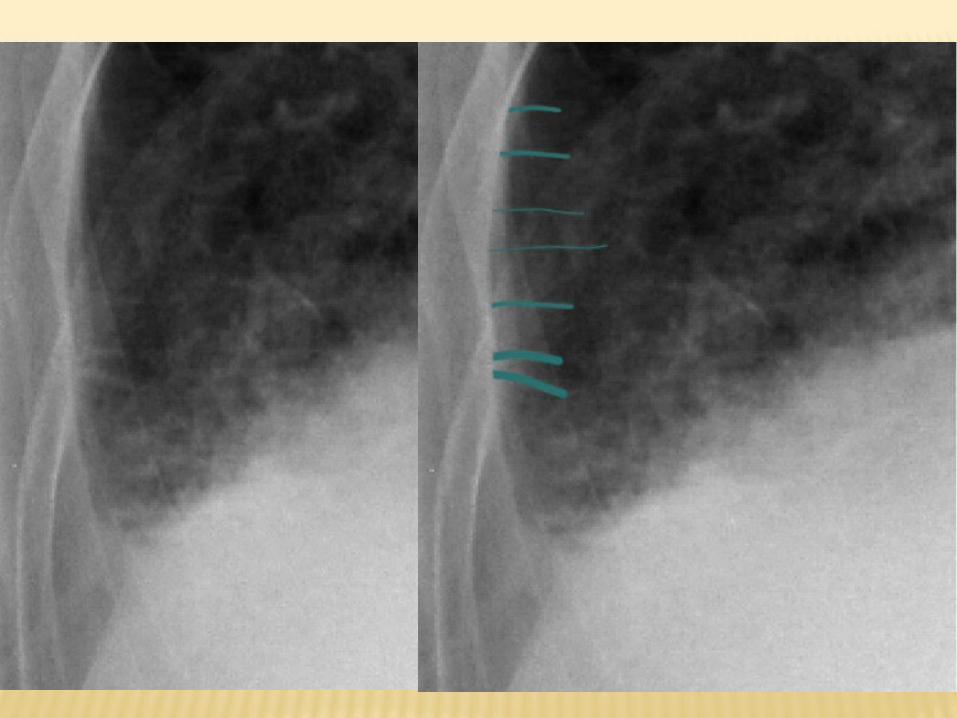

HF CXR
Alveolar oedema
Kerley B lines (interstitial oedema)
Cardiomegaly
Dilated upper lobe vessels
Effusions

ECHOCARDIOGRAM 2 types
Valves
LV systolic/diastolic Fx
Aorta
LVEF
MANAGEMENT OF ACUTE HEART FAILURE
Assess ABCDE
Loop diuretics IV - furosemide
Morphine IV - slowly
Nitrates – avoid if hypotensive
Oxygen – 100% NRBM
Position upright

MANAGEMENT OF CHRONIC HEART FAILURE CONSERVATIVE Mx
CARDIAC REHABILITATION
For pts with IHD, HF or recent cardiac surgery
Available at local hospitals Education Emotional support Physical fitness
4 stages
MEDICAL MANAGEMENT OF CHRONIC HF
Recommended by NICE if reduced ejection fraction
1st line = ACE-INHIBITORS (or ARBs) + BETA-BLOCKERS
2nd line = add in ARB or spironolactone or hydralazine
3rd line = digoxin
*patients with fluid overload should receive diuretics*
AVOID CARDIO-SELECTIVE CALCIUM CHANNEL BLOCKERS

SURGICAL MANAGEMENT OF CHRONIC HF
CLINICAL SCENARIO TIME
Mr Meldrew 61 years old 3/12 Hx of malaise,
increasing SOB and ankle swelling
Now SOB walking upstairs PMHx: HTN, MI in 2008 80 pack year smoking Hx
Any other questions?

DIFFERENTIALS??
DIFFERENTIALS??CARDIAC
Valvular heart disease Coronary artery disease Left ventricular failure
RESPIRATORY
Infection Inflammation Neoplastic Degenerative
OTHER
Anaemia Anxiety
INVESTIGATIONS?

INVESTIGATIONS?
BEDSIDE
BLOODS
IMAGING
SPECIAL

*EMERGENCY*
Mr Meldrew attends A&E severely SOB
He can hardly talk
You are the FY1 in ED sent to clerk him – what do you do?

EMERGENCY OVER…
How will you manage him long term now he is stable?

EXPLANATION STATION

REFERENCES
www.merckmanuals.com Nice Guidelines. Chronic Heart failure (2010). Patrick Davey. Medicine at a Glance (2010).
Blackwell publishing http://www.medindia.net/patients/patientinfo/C
ongestive-Heart-Failure.htm The Criteria Committee of the New York Heart
Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels. 9th ed. Boston, Mass: Little, Brown & Co; 1994:253-256.