Embed Size (px)
Citation preview

Editorial BoardDrozdstoj Stoyanov (Editor-in-chief)Damianka Getova-Spassova(Managing Editor)Ivan Kindekov (Scientific secretary)Boyan LozanovDobrin SvinarovGrigor VelevJanet Grudeva-PopovaMargarita KamenovaMihail BoyanovNadka Bojadjieva
International Advisory BoardAndrew Miles – London, U.K.Ashok Agraval – Clivelandq Phio, USAJuan E. Mezzich – New York, USAJan Kiselovic – Bratislava, SlovakiaKenneth William Fulford – Oxford, U.K.Miroljub Popovic – Murcia, SpainSamuel Refetoff – Chicagp, Illinois, USAStanley B. Prusiner – Nobel Laureate, San Francisco, USA
BULGARIAN MEDICINE ISSN 1314-3387
Редакционна колегияДроздстой Стоянов
(главен редактор) Дамянка Гетова-Спасова
(изпълнителен редактор)Иван Киндеков
(научен секретар)Боян Лозанов
Добрин СвинаровГригор Велев
Жанет Грудева-ПоповаМаргарита Каменова
Михаил БояновНадка Бояджиева
Международен редакционен съвет
Андрю Майлс – Лондон, Великобритания
Ашок Агравал – Кливланд, САЩХуан Месич – Ню Йорк, САЩ
Ян Киселович – Братислава, Словакия
Кенет Уилиям Фулфорд – Оксфорд, Великобритания
Миролюб Попович – Мурсия, Испания
Самуел Рефетоф – Чикаго, САЩ
Стенли Прузиър – Нобелов лауреат, Сан Франциско, САЩ

Съдържание
Христо Давидов, Златослав АрабаджиевНевроцистицеркоза: Обзор върху
психиатричната симптоматика ............................... 4
Райчева Г., Грудева-Попова Ж., Попов В., Влайкова М., Вълчева M.Множествени първични малигнени неоплазми..... 9
Сарачева К., Гетова Д.Ефекти на триптани второ поколение –
фроватриптан и алмотриптан върху локомоторната
активност при експериментален модел
на мигрена................................................................17
Гетова Д., Димитрова Д., Тополов М.Сравняване на телесното тегло, BMI, нивата на
глюкоза, кръвното налягане и пулсовата честота
на различни възрастови групи пациенти включени
в проекта НИРДИАБО от Пловдив...........................23
В. Попов, И. Михайлова, Ж. Грудева-ПоповаПерсонализирана радиационна
онкология - концепция,
реални клинични възможности..............................30
Желязкова М., Тодоров П., Попова В., Каралилова Р., Баталов А.Вътреставни апликации с тромбоцит богата плазма
за лечение на колянна остеоартроза.....................36
Author’s guidelines .............................45
Обзори
Оригинални статии
Бъ
лгар
ска м
ед
иц
ин
а
Българска медицина се реферира в международната база данни Index Copernicus International.

Content
Hristo Davidov, Zlatoslav ArabadzievNeurocysticercosis: Review of its
Psychiatric manifestations ......................................... 4
Raycheva G., Grudeva-Popova Zh., Popov V., Vlajkova M., Valcheva M.Multiple primary malignant neoplasms...................... 9
Saracheva K., Getova D.Effects of second generation triptans -
frovatriptan and almotriptan on locomotor activity
in an experimental model of migraine......................17
Getova D., Dimitrova D., Topolov M.Comparison of body weight, BMI, glucose level, blood
pressure and heart rate in different groups of patients
included in NIRDIABO project from Plovdiv.............23
V. Popov, I. Mihaylova, Zh. Grudeva-PopovaPersonalized radiation oncology -
concepts, real clinical possibilities ...........................30
Zhelyazkova M., Todorov P., Popova V., Karalilova R., Batalov A.Intra-articular platelet rich plasma injections for Knee
Osteoarthritis.............................................................36
Author’s guidelines .............................47
Reviews
Original articles
Bu
lgaria
nm
ed
icin
e
Bulgarian medicine is included inIndex Copernicus International database.
4 Bulgarian medicine vol. 7 № 1/2017
Невроцистицеркоза: Обзор върху психиатричната симптоматика Христо Давидов1, Златослав Арабаджиев2
1Медицински факултет, Медицнски университет – Пловдив
2Катедра по Психиатрия и Медицинска психология,
Медицински университет - Пловдив
Neurocysticercosis: Review of its Psychiatric manifestations
Hristo Davidov1, Zlatoslav Arabadziev2
1Faculty of Medicine, Medical University of Plovdiv, Bulgaria
2Department of Psychiatry and Medical Psychology,
Medical University of Plovdiv, Bulgaria
Reviews
РЕЗЮМЕ:
Невроцистицеркозата е паразитнозаболяване на Централната нервна систе-ма, причинено от ларвовата форма насвинската тения, Taenia solium. При цере-бералната цистицеркоза обикновено имаизява на психиатрична симптоматика. Идвете заболявания могат да бъдат комор-бидни на други неврологични синдроми,или да се проявяват самостоятелно. Тезиабнормности са били предмет на широкомащабни проучвания провеждани от пси-хиатри и невролози в началото на 20 век,полагащи основите за по–доброто разби-ране на органичните психични разстрой-ства.
Ключови думи: Taenia solium, невро-цистицеркоза, клинична картина, психиа-трична коморбидност
ABSTRACT
Neurocysticercosis is a medical condition ofparasites investing the central nervous sys-tem. It is caused by the larval form of the porktapeworm Taenia solium. Psychiatric distur-bances are typically present as clinical symp-toms of cerebral cysticercosis, both in comor-bidity with other neurological syndromes or asa dominant feature. These kinds of abnormal-ities were a subject of extensive studies bypsychiatrists and neurologists at the begin-ning of the 20th century, providing key pre-liminary insights into organic mental diseases.
Key words: Taenia solium, neurocysticer-cosis, clinical manifestations, psychiatriccomorbidity

Bulgarian medicine vol. 7 № 1/2017 5
INTRoDuCTIoN
Neurocysticercosis (NCC), a condition cau-sed by the pork tapeworm T. solium, is themost common parasitic infection of the CNS(5). Nevertheless, its natural history hasn’tbeen well documented. As regards the epide-miology of NCC, the disease is widely endemicin underdeveloped countries in Central andSouth America, Asia, and Africa. According tostatistical data, more than 400,000 people inLatin America (1,11) and 10% of those pre-senting neurologic signs in developing countri-es (10) have NCC. NCC accounts for up to 2%of neurologic and neurosurgical admissions insouthern California (15) and for more than1000 cases per year in the United States (23).It mostly affects adults in their 30s or 40swhile the infection is quite uncommon in theelderly and in children younger than 2 yearsowing to the long incubation period of T. soli-um (19).
LIFE CyCLE oF TAENIA SoLIuM
It takes approximately 2 months for thelarva to evolve into a mature adult tapewormat is capable of producing eggs (18). The fully-grown tapeworm lives in the human smallintestines and consists of a scolex and strobi-la. The strobila consists of proglottids thatcontain approximately 40,000 eggs. T. soliumcan shed up to 300,000 eggs daily into thefeces. Afterwards, the eggs are disseminatedinto the environment. Free-ranging pigs nor-mally feed on human feces that are contami-nated with eggs, which later develop into cys-ticerci (scolex containing cysts). The ingestionof undercooked infected pork containing cys-ticerci, whereby ingestion of T.solium eggsoccurs, and the contact with carriers or conta-minated food infects humans with NCC.Ingested eggs hatch in the stomach and theintestine and the then-formed oncospherescirculate in the blood and get access to varioustissues. Thus cysticerci often develop in sub-cutaneous tissue, skeletal muscle, the brain,the eyes, heart, liver and lungs. Actually,developing cysticerci cause little host reaction.Usually only after several years, when cysti-cerci denigrate, inflammation develops.Ultimately, the cysts undergo necrosis andmay become calcified. These calcified or dead
cysts are antigenic and upon being recognizedby the host, may induce an inflammatoryreaction (17). The survival of the eggs isadversely affected by extreme temperatureand desiccation, whereas humidity, tempera-tures ranging between 10°F and room tempe-rature favor egg survival. It should be takeninto consideration that wind, water, and birdshelp dispersing the eggs (19).
CLASSIFICATIoN AND PRoGNoSIS
NCC is categorized according to the viabili-ty and location of the parasite in the host CNS.The classification is divided into active (vesicu-lar), transitional (inflammatory, degenerating,or colloidal), granular nodular (healing), andinactive (calcified) stages (4). Each viabilitycriterion is further subdivided into extraparen-chymal and parenchymal. Parenchymal formsof NCC have good prognosis in terms ofremission of clinical signs (7). On the otherhand, the prognosis for extraparenchymalforms is unfavorable, especially in patientswith hydrocephalus due to arachnoiditis (7).The viability criterion allows analysis of theparasite`s natural history and production ofpathophysiologic changes in the hosts CNS.This is of prime importance as clinical mani-festations and therefore therapeutic procedu-res vary depending on the classification (19).
DISEASE MANIFESTATIoNS
The presentation of NCC in accordance withthe stage, location, and amount of thecysts.11 The clinical manifestations developupon an inflammatory response around a cys-ticercus that is degenerating. What triggerssuch degeneration hasn’t been established,but the cyst seems to lose its ability to regu-late the host immune response. It has beenestimated that peak presentation occurs in 3to 5 years post infection, but it might take lon-ger than 30 years. After degenerating, thecysts become calcified and inactive. At thisstage, they may no longer cause symptoms ormay serve as a core for epileptic activity.Parenchymal NCC is the most common type ofNCC. As a great number of cysts invade thebrain parenchyma, clinical manifestationsinclude seizures (focal or generalized), focalencephalitis, edema, and vasculitis. Any focal

6 Bulgarian medicine vol. 7 № 1/2017
neurologic deficits are usually transient, withremissions and relapses. Patients may sufferfrom headaches and signs of increased intrac-ranial pressure in both the parenchymal andextraparenchymal forms. Patients having ext-raparenchymal disease usually develop sym-ptoms of hydrocephalus owing to intraventri-cular cysts. Subarachnoid cysts may lead tovisual field defects and cranial nerve palsies.Spinal cord cysticer-cosis is rare. When thespine is affected, the thoracic region is themost common location. Spinal cord cysticer-cosis can in turn lead to radiculopathy, parest-hesias, and sphincter disturbances. Cysticercimay also develop in the eyes, heart, muscle,or subcutaneous tissue. Ocular cysticercosis isusually asymptomatic. Chorioretinitis, retinaldetachment, or vasculitis may result in inflam-mation that occurs around degenerating cys-ticerci. When the heart is affected, conductiondefects and arrhythmias may ensue.Subcutaneous tissue and muscle involvementwill result in subcutaneous nodules and myo-pathy (19).
PREVALENCE oF PSyChIATRIC DISoRDERS
Most of the psychiatric knowledge on NCChas been gathered from studies carried out inmental institutions in the late 1800s and theearly 1900s. These sources have provided uswith detailed descriptive accountss of the pati-ents’ psychopathology. In many cases it wouldmimic major psychiatric syndromes such asschizophrenia and bipolar disorder (12,13,24).
The occurence of NCC was presumed to behigh in psychiatric institutions not only due toa causal relationship between the two medicalconditions, but also because patients withsevere forms of psychosis and dementia wereprone to become secondarily infected as aconsequence of poor hygiene and copropha-gia.A number of psychiatric syndromes havebeen so far attributed to NCC. In early papersof classic research on this subject, one cancome across accounts that are indistinguis-hable from dementia praecox, paranoia,neurosyphilis, Korsakoff’s psychosis anddementia (22,27). Chronic delusions and hal-lucinations, as well as mood variations compa-tible with the diagnoses of major depressive
disorder and bipolar disorder were also repor-ted (2,21). As the etiology of these cases wasseldom established in life, clinical findingswere retrospectively correlated to neuropat-hological observations of signs of the parasiticinfection. Leukart (1886), for instance, sug-gested that cysticerci that are located in theventricles and basal ganglia were more liableto induce mental abnormalities than corticallesions (14). In the majority of these cases,neuropsychiatric findings were compatiblewith major cognitive impairments such asdelirium and dementia (14, 24).
In Europe, further interest in NCC was rai-sed after the evaluation of cysticercosis in 450British ex-servicemen who had acquired thedisease during military placements in pre-1947 colonial India (6). 39 of these patients(8.7%) manifested mental disorders as a pro-minent feature – there were cases of organicdeterioration, affective disorders and schi-zophrenia. Excluding the former cases of une-quivocal organic mental disease, medicalrecords showed divergence on the etiologicalrelationship between the psychiatric conditionand cysticercosis.
Clinicians from Brazil, Chile, Mexico, Chinaand other countries where prevalence of thedisease was high have also made importantcontributions to this field of scientific knowled-ge.
In a cross-sectional study of 38 cases at aneurology outpatient clinic in Brazil, depressi-on was the commonest psychiatric manifesta-tion, as shown by the Present StateExamination and the Schedule for AffectiveDisorders and Schizophrenia – LifetimeVersion semi-structured interviews (9,25,28).Signs of psychosis were observed in five pati-ents although none had a clear-cut schizoph-renic or bipolar presentation. Only 13 patients(34.2%) were classified as mentally healthyby the aforementioned psychometric met-hods. Thirty-two patients were assessed bythe Mini-Mental State Examination and theStrub and Black’s Mental Status Examination(8,26), whereby neuropsychological dysfun-ction was identified in the majority of thecases (87.5%). Yet, severe cognitive abnor-malities were less frequent (15.6%) (9, 24).Attention deficits were detected in all the pati-ents assessed, which has probably been influ-

Bulgarian medicine vol. 7 № 1/2017 7
enced by the effect of antiepileptic drugs(car-bamazepine and barbiturates). 59.4% hadmild to moderate and 40.6% manifestedsevere attention disturbance. Memory andlanguage were affected in 78% of the patientsand higher cognitive functions were impactedin 87.5%.Other deficits included disorders ofpraxis and motor functions (50%). Readingand writing skills were not so commonlyimpacted (28% and 0.6% of patients, respec-tively). There was no clear pattern of localiza-tion for the neuropsychological dysfunction inthe patients. Despite the clinical heterogeneityof the test group, there was only a mild corre-lation between the manifestation of depressi-on and laboratory signs of active disease(defined by the presence of parenchymalcysts, not just calcifications , as shown bycomputed tomography(CT) and magneticresonance imaging(MRI) scans, and/orinflammatory cerebrospinalfluid (CSF)) (P =0.04), and modest correlation with the occur-rence of intracranial hypertension (P = 0.1).Psychosis also possibly correlated with intrac-ranial hypertension (P =0.06) but not withdisease activity (P = 0.5). No association wasfound between the psychiatric manifestationsand the occurrence of epilepsy (P = 0.63),even when the epidemiological group of activeepilepsy 29 was considered (P =0.72), norwith the current use of steroids (P =1).Previous history of depressive episodes swasstrongly associated with current depression (P= 0.006) and psychosis (P = 0.04) (9).Thesefindings come in accordance with severalother studies that have addressed the etiologyof organic mood disorders. Family history ofdepression and history of depression before
the onset of the organic disease are regardedas risk factors for developing depression inpatients with cerebrovascular disease andmultiple sclerosis due to greater biological vul-nerability (3,20). Disease activity, i.e. diffuseor localized central nervoussystem inflamma-tion, is temporally related to organic mooddisorders, as shown in other medical andneurological conditions like systemic lupuserythematosus and multiple sclerosis (16,24).
CoNCLuSIoNS
The assessed mental abnormalities andcognitive dysfunctions in respectively 65.8%and 87.5%, of a cross-section of neurologicaloutpatients with NCC presents an estimate ofthe high prevalence of psychiatric morbidity inthe given setting. Samples of psychiatric inpa-tients might assist with a different profile ofpsychiatric findings of more severe or evenspecific forms of mental diseases. That isthanks to psychiatric surveys based on pati-ents from mental institutions in the first half ofthe 20th century reporting up to 75% of seve-re mental diseases in association with cysti-cercosis. Such a high rate might be accountedfor by a long period of the untreated underly-ing organic disease, since many of the afore-mentioned patients had previous history ofneurological syndromes prior to psychiatricadmission, as written in their medical records.It is possible therefore that mental diseaserepresents one of the consequences of a dete-riorating organic illness, in the setting of noeffective therapeutic strategies for the parasi-tic infection at that time.
REFERENCES:
1. Bern C, Garcia HH, Evans C, et al. Magnitude ofthe disease burden from neurocysticercosis in adeveloping country, Clin Infect Dis,1999;29:1203-9
2. Brinck, G., Beca, F. Contribución al estudio de lacisticercosis cerebral. Revista Medica de Chile(Santiago) 1936, 64, 348–392.
3. Brumback, R.A. Is depression a neurologic dis-ease? Behavioural Neurology 1993, 11, 79–104.
4. Carpio A, Placencia M, Santillan F, Escobar A. Aproposal for classification of neurocysticercosis.Can J Neurol Sci , 1994; 21:43-7
5. Del Brutto OH, Rajshekhar V, White AC Jr, et al.Proposed diagnostic criteria for neurocysticerco-sis. Neurology, 2001;57:177-83
6. Dixon, H.B.F., Lipscomb, F.M. Cysticercosis: anAnalysis and Follow-up of 450 Cases. F. Mildnerand Sons, London, 1961.
7. Estanol B. Medical treatment of cerebral cysticer-cosis. Eur Neurol 1997;37:125-126
8. Folstein, M.F., Folstein, S.E., Mchugh, P.R.H. Mini-Mental State: A practical method for grading thecognitive state of patients for the clinician.Journal of Psychiatric Research 1975, 12, 189–198.
9. Forlenza, O.V., Vieira, A.H.G., Gouveia, M.F., et al.Psychiatric morbidity of cerebral cysticercosis: a
8 Bulgarian medicine vol. 7 № 1/2017
Адрес за кореспонденция:
ХРИСТО ДАВИДОВ,
студент по медицина в Медицински университет в Пловдив
Email: [email protected]: 0897767938
Corresponding author:
hRISTo DAVIDoV,
student of Medicine in Medicaluniversity of Plovdiv, BulgariaEmail: [email protected]
Mobile: 0897767938
study of 38 patients from a neurology clinic inSão Paulo. Journal of Neurology, Neurosurgeryand Psychiatry, 1997, 62, 612–616.
10. Garcia HH, Gilman RH, Tovar MA, et al. Factorsassociated with Taenia solium cysticercosis:analysis of nine hundred forty-six Peruvian neu-rologic patients. Cysticercosis Working Group inPeru (CWG). Am J Trop Med hyg, 1995;52:145-8
11. Garcia HH, Pretell EJ, Gilman RH, et al. A trial ofantiparasitic treatment to reduce the rate ofseizures due to cerebral cysticercosis.Cysticercosis Working Group in Peru. N EnglJMed , 2004;350:249-58.
12. Griesinger, W. Cysticerken und ihre Diagnose.In: Psychiatrische und NervenpathologisheAbhandlungen. Gesammelte Abhandlungen.Verlag von August Hirschwald, Berlin, 1872,399–443.
13. Küchenmeister, F. On Animal and VegetableParasites of the Human Body. A Manual of TheirNatural History, Diagnosis and Treatment. TheSyndenham Society, London, 1857.
14. Leukart, R. The Parasites of Man, and TheDiseases Which Proceed From Them. A Textbookfor Students and Practitioners. Young J.Pentland, Edinburgh, UK, 1886, 488–551.
15. McCormick GF. Cysticercosis – review of 230patients. Bull Clin Neurosci 1985;50:76-101
16. Miguel, E.C., Pereira, R.M.R., Pereira, C.A.B., etal. Psychiatric manifestations of systemic lupuserythematosus: clinical features, symptoms, andsigns of central nervous system activity in 43patients. Medicine 1994, 73, 224 – 232.
17. Nash TE, Patronas NJ. Edema associated withcalcified lesions in neurocysticercosis. Neurology,1999, 53:777-81.
18. Pawlowski ZS. Taeniasis and cysticercosis. In:Hui YH, Gorham JR, Murrel KD, editors.Foodborne disease handbook. New York: MarcelDekker; 1994, 199-254.
19. Pinto, S. et. Al, Neurocysticercosis: An unusualcase of epileptic seizures, Hospital physician,2005, 40-44
20. Popkin, M.K., Tucker, G.J. ‘Secondary’ and drug-induced mood, anxiety, psychotic, catatonic, andpersonality disorders: a review of the literature.Journal of Neuropsychiatry and ClinicalNeuroscience, 1992, 4, 369–385.
21. Pupo, P.P., Cardoso, W., Reis, J.B., et al. Sobre acisticercose encefálica.
Estudo clínico, anátomo-patológico, radiológico e doliquido céfalo-raqueano. Archivos da Assistênciaaos Psicopatas de São Paulo, 1946, 10–11, 3–123.
22. Ribas, J.C. Psicoses por lesões cerebrais. Revistade Medicina 1934, 27, 31–39.
23. Shandera WX, White AC Jr, Chen JC, et al.Neurocysticercosis in Houston, Texas. A report of112 cases.Medicine (Baltimore) 1994;73:37-52
24. Singh G., Probhakar S, Taenia soliumCysticercosis: From Basic to Clinical Science,Cabi, 2002, 263-268
25. Spitzer, R.L., Endicott, J. Roteiro para distúrbiosafetivos e esquizofrenia – versão para a vidatoda – SADS-L, Trad. de Valentim Gentil Filho.São Paulo: Departamento de Psiquiatria daFaculdade de Medicina da Universidade de SãoPaulo, 1978–1979. [Mimeo]. Translated from:Spitzer, R.L., Endicott, J. Schedule for AffectiveDisorders and Schizophrenia (Life-time) – SADS-L. 3rd edn. Clinical Research BranchCollaborative Program on the Psychobiology ofDepression, NIMH, Bethesda, USA. May, 1978 –September, 1979.
26. Strub, R., Black, F.W. Mental Status Examinationin Neurology, 2nd edn. FA Davis Company,Philadelphia, USA, 1984.
27. Tretiakoff, C., Pacheco, E., Silva, A.C.Contribuição para o estudo da cysticercóse cere-bral e em particular das lesões cerebraes toxicasá distancia n’esta affecção. Memórias do Hospíciode Juqueri 1,1924, 37–66.
28. Wing, J.K., Cooper, J.E., Sartorius, N., TheMeasurement and Classification of PsychiatricSymptoms. An Instruction Manual for ThePresent State Examination and CATEGOProgram. Cambridge University Press,Cambridge, UK, 1974.
Bulgarian medicine vol. 7 № 1/2017 9
Множествени първичнималигнени неоплазмиРайчева Г., Грудева-Попова Ж., Попов В., Влайкова М., Вълчева M.Катедра по Клинична Онкология Медицински Факултет,
Медицински Университет – Пловдив;
Университетска Болница „Св. Георги” – Пловдив
Multiple primarymalignant neoplasms
Raycheva G., Grudeva-Popova Zh., Popov V., Vlajkova M., Valcheva M.Мedical University, Faculty of Medicine – Plovdiv
Department of Clinical Oncology
University Hospital „Sv. Georgi” – Plovdiv
РЕЗЮМЕ:
В последното десетилетие честотата напациентите с множествени първичнималигнени заболявания нарастна значи-телно както поради подобрените диагнос-тични възможности, така и поради удълже-ната преживяемост. Подобен случай е опи-сан за първи път от Whipham (1878) припациент с левкемия и карцином на пан-креаса. Billroth (1889) формулира първитетри критерия, характеризиращи подобнитумори: всеки тумор е с различен хистоло-гичен произход; имат различна локализа-ция (добре диференцирани макро, -мик-роскопски); всяка лезия има свои метас-тази. Warren and Gates(1932) предлагатактуални критерии: всеки тумор трябва дабъде злокачествен; да бъде категоричноразличен от другия; възможността единиятда бъде метастатична лезия на другия сеизключва. Огромното разнообразие и въз-можности за комбиниране на тези тумориправи невъзможно създаването на една
ABSTRACT
In recent years, the incidence of patientswith multiple primary malignant tumors hasincreased considerably - due to the increaseddiagnostic capacity and prolonged survival ofthese patients. For the first time, such a casedescribed by Whipham (1878) of a patientwith leukemia and pancreatic carcinoma. FirstBillroth (1889) formulates three primary crite-ria for distinguishing these tumors: eachtumor must have a different histologicalappearance; the tumors must arise in variouslocations (i.e., clearly differentiated macro-and microscopically); each lesion must pro-duce its metastasis. Warren and Gates (1932)offered broader criteria: each of the tumorshas a clear picture of malignancy; each mustbe distinct; the possibility of one being ametastatic lesion of the other must be exclud-ed. The huge diversity and countless possibil-ities for combinations of these tumors make itimpossible to structure them into a singleclassification. That is why we divide them into

10 Bulgarian medicine vol. 7 № 1/2017
класификация. Ето защо те са разделят вдве групи: синхронни (две или повеченеоплазми се развиват едновременно впериод до 6 месеца) и метахронни (втори-ят карцином се появява повече от 6 месецаслед първия). Според статистическитеданни 5-годишната онкологична прежи-вяемост е нарастнала до 60%. Даннитепоказват, че броят пациенти с множестве-ни първични малигнени заболявания щенараства.
Kлючови думи: синхронни неоплазми,метахронни неоплазми
two groups: synchronous (two or more neo-plasias develop simultaneously within a periodof up to 6 months and metachronous (thesecond carcinoma develops after 6 monthscompared to the first). By statistical data, 5-year oncology survival rate increased to 60%.Data show that the number of patients withmultiple primary malignant neoplasias willincrease.
Key words: synchronous neoplasms,metachronous neoplasms
INTRoDuCTIoN
In recent years, the incidence of patientswith multiple primary malignant tumors hasincreased considerably - due to the increaseddiagnostic capacity and prolonged survival ofthese patients. Patients survived a malignancyhave a 20% higher risk of developing a secondprimary neoplasia in the same or another organcompared to the general population.Publications in this area were recognized sincethe late nineteenth century.
In 1888 Fenger [5] published the first reporton synchronous colorectal carcinomas. Later, in1889 Billroth [1] reported a series of cases ofmultiple primary breast carcinomas. Until theend of the 19th century, there was a lack of inte-rest in the scientific circles of these isolatedcases of patients with multiple neoplasias. Atthe beginning of the 20th century, however, it isnoticeable that not only the incidence of patientsprogress but also the number of cases describedin the scientific literature. In 1932, Warren andGates [19] summarized 1259 cases from theworldwide publications. In the following years,over 10,000 cases have been reported globally.
In the period 1926-1931 Warren [18] and col-leagues observed cases of autopsy patients withmalignancies, 3.7% of all had multiple primarylesions. From the period 1932-1943 6.8 % havebeen demonstrated with multiple primary malig-nancies. Hurt and Borders [6] reported 3.3% pri-mary malignant lesions among surgical patientsat the Mayo Clinic in 1929. In 1937 Stalker [14]and associates confirm 4.5% of primary malig-nant neoplasia among surgical interventions inthe same clinic.
It is noteworthy that the number of thesepatients has increased significantly over theyears and they are no longer isolated cases.Due to improved treatment methods, patientswho have overcome a malignant disease livelong enough to have the risk of developing asecond illness.
CRITERIA FoR DIAGNoSIS
At the beginning of the 20th century, it waswrongly believed that the presence of a malig-nant neoplasia suppressed the development ofanother. Hurt and Broders [6], however, noticeda trend among 71 cases that the occurrence ofa second neoplasia is more likely to occur in thesame organ or system as the first. Taylor, 1931reported 18 breast cancer patients who develo-ped a second malignancy in the genital tract[15]. A little later, other scientists (Pierce andSlaughter, Huber) sought an explanation for therelationship between estrogen-dependentorgans and the occurrence of a second neopla-sia. However, there is no clear evidence to sup-port these two hypotheses [13].
All this requires the establishment of clearcriteria for the diagnosis of multiple primarymalignancies. Due to the specificity, variety, andunpredictability of these neoplasias, it’s hard tobe absolute. Multiple primary malignancies aretwo or more tumors that are found in the sameindividual at the same time or consecutivelyover a given period, i. e. occur synchronously ormetachronically in one or different organs.
First Billroth [1] formulates three primary cri-teria for distinguishing these tumors:
Bulgarian medicine vol. 7 № 1/2017 11
l Each tumor must have a different histologicalappearance
l The tumors must arise in various locations(i.e., clearly differentiated macro- and mic-roscopically)
l Each lesion must produce its metastasis.Subsequently, it became apparent that due
to these strict requirements, a low incidence ofmultiple primary malignant neoplasias wasreported. This is not real because it is entirelypossible that two carcinomas, independently ofeach other, with a similar histological characte-ristic, occur. In 1932, Warren and Gates [19]offered broader criteria:l Each of the tumors has a clear picture of
malignancyl Each must be distinctl The possibility of one being a metastatic lesi-
on of the other must be excluded.
CLASSIFICATIoN
The huge diversity and countless possibiliti-es for combinations of these tumors make itimpossible to structure them into a single clas-sification. That is why we divide them into twogroups [12]: 1. Synchronous - when two or more neoplasias
develop simultaneously within a period ofup to 6 months.
2. Metachronous - when the second carcinomadevelops after 6 months compared to thefirst. This division is somewhat conditional.Synchronic tumors are not relevant to theprognosis if they are diagnosed on time. Butif their presence is missed, they later mani-fest themselves as the so-called an advan-ced metachronous tumor at an advancedstage.Patients with primary malignancy had a
1.29-fold higher risk of developing a secondmalignant tumor with the same localization(Schoenberg) as compared to the generalpopulation. In general, we distinguish the fol-lowing risk factors: genetic predisposition,exposure to environmental carcinogenic fac-tors, prior therapy for first malignant neoplasia(chemotherapy, radiotherapy), immunocom-promised status. Most likely, the etiology of asecond primary malignant tumor is multifacto-
rial (table 1). Other determinants includeimproved diagnostic tests, complicated, com-plex treatment, a presence of screening pro-grams (for breast cancer, colorectal cancer,prostate cancer, etc.).
CASE STuDIES IN DIFFERENT CouNTRIES
The scientific literature has many retros-pective studies evaluating the incidence ofmultiple primary neoplasias. Due to theadvanced diagnostic methods, it ranges from0.4% to 21% in different countries.
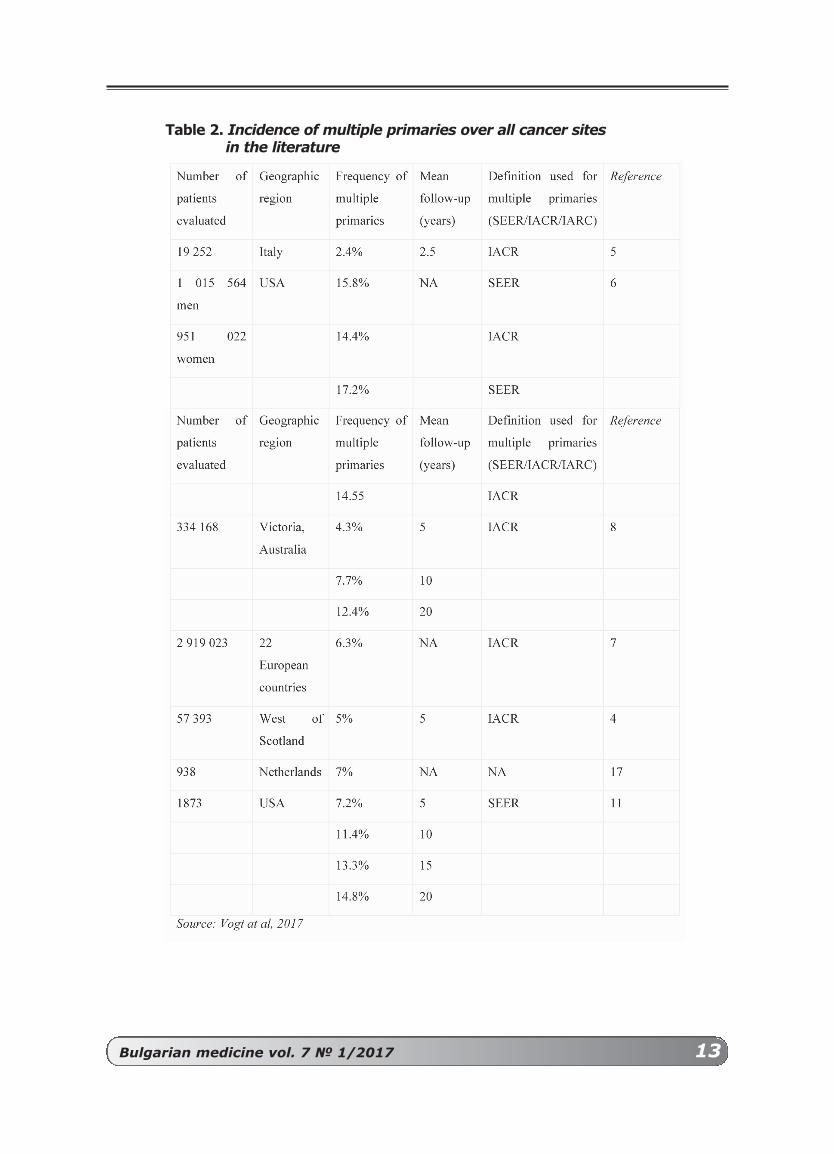
In a 10-year study (1944-1953) in MayoClinic, USA, involving 37,580 patients, 1,909cases of histologically verified multiple prima-ry malignancies were reported, or 5.1%. Thispercentage increased after 309 autopsycases demonstrating the presence of morethan one tumor left asymptomatic during thelifetime [9]. A Swedish study of 808 522oncologists over 30 years confirms 11% ofcases with second primary malignancy(Table 2).
SuMMARy
By statistical data, 5-year oncology survi-val rate increased to 60%. According to theWorld Cancer Registry for 2012, there are14.1 million cancer patients, of which 8.2 mil-lion have died. The prognosis for 2030 sho-wed 21.7 million cases of malignancies, ofwhich 13 million will end fatally. Data showthat the number of patients with multiple pri-mary malignant neoplasias will increase. Thispatient pool is of interest not only because ofthe increasing incidence but also because ofthe therapeutic challenges, especially whencombining a solid tumor with an on-hemato-logic disease. In daily clinical practice, thesepatients should be individually refined.
CASE STuDIES IN DIFFERENT CouNTRIES
The scientific literature has many retro-spective studies evaluating the incidence ofmultiple primary neoplasias. Due to theadvanced diagnostic methods, it ranges from0.4% to 21% in different countries.

12 Bulgarian medicine vol. 7 № 1/2017
Table 1. Epidemiological factors of multiple primary tumors
In a 10-year study (1944-1953) in MayoClinic, USA, involving 37,580 patients, 1,909cases of histologically verified multiple primarymalignancies were reported, or 5.1%. Thispercentage increased after 309 autopsy cases
demonstrating the presence of more than onetumor left asymptomatic during the lifetime[9]. A Swedish study of 808 522 oncologistsover 30 years confirms 11% of cases with sec-ond primary malignancy (Table 2).
Bulgarian medicine vol. 7 № 1/2017 13
Table 2. Incidence of multiple primaries over all cancer sites in the literature

14 Bulgarian medicine vol. 7 № 1/2017
Table 3. Second tumor appearance depending on location
In a retrospective study in China for theperiod 01.2010-12.2013 involving 15,398cancer patients, reported 0.99% of cases ofmultiple primary malignant neoplasias [8].They report that patients with primary head-neck and urinary tract malignancies weremost at-risk of developing a second tumor,50% of them were having no prior radiationor chemotherapy (Table 3).
Most studies show that male gender ismore affected [8]. Patients with multipletumors are older than those with onlytumors - between 50 and 70 years of age.Most commonly, the combinations reportedin men are the prostate-colorectal carcino-ma, prostate-lung, prostate-chronic lym-phocytic leukemia. In women: breast cancerwith contralateral breast cancer or breast
cancer in conjunction with hematologicalmalignancy (Table 4).
SuMMARy
By statistical data, 5-year oncology survivalrate increased to 60%. According to the WorldCancer Registry for 2012, there are 14.1 millioncancer patients, of which 8.2 million have died.The prognosis for 2030 showed 21.7 millioncases of malignancies, of which 13 million will endfatally. Data show that the number of patientswith multiple primary malignant neoplasias willincrease. This patient pool is of interest not onlybecause of the increasing incidence but alsobecause of the therapeutic challenges, especiallywhen combining a solid tumor with an on-hema-tologic disease. In daily clinical practice, thesepatients should be individually refined.

Bulgarian medicine vol. 7 № 1/2017 15
Тable 4. Common risk factors for multiple primaries in women with breast cancer (adapted from Wood et al. 2012)
REFERENCES
1. Billroth T. Die Allgemeine ChirurgischePathologie and Therapie in 51 Vorlesungen. In:Handbuch fur Studierende and Artze. Berlin1889; 14, p. 908
2. Billroth H.: Quoted by Hojman D, Garriz RA,Markman(35 Hojman D, Garriz RA, Markman I.Multiple malignant tumors of the colon and rec-tum. Dis Colon Rectum 1966; 9:121–6
3. Billroth T: Quoted by CORNES JS (17 CornesJS). Multiple primary cancers: primary malig-nant lymphomas and carcinomas of the intes-tinal tract in the same patient; doi:10.1136/jcp.13.6.483. J Clin Pathol 1960; 13:483-489
4. Demandante C, Troyer D, Miles T. Multiple pri-mary malignant neoplasms. Case Report and aComprehensive Review of the Literature. Am JClin Oncol (CCT) 2003; 26(1):79-83
5. Fenger C. Double carcinoma of the colon. J AmMed Assoc 1888;11:606–8
6. Hurt,H, Brodersa C. Multiple primary malignant
neoplasms. J Lab Clin Med 1933; 18:765-7777. Huber H. Genitalkarzinom und Mammakarzinom
als Multiplizitatstumoren. Strahlen-therapie1953; 92:130-140
8. Liu Z, Liu C, Guo W, et al. Clinical analysis of152 cases of multiple primary malignanttumors in 15,398 patients with malignanttumors. doi: 10.1371/journal.pone.0125754.eCollection 2015
9. Moertel C., Dockerty M, Baggenstoss A. Multipleprimary malignant neoplasms. Introduction andPresentation of Data. Cancer March- April,1961; 14:221- 230
10. Moertel C, Dockerty M, Baggenstoss A. Multipleprimary malignant neoplasms, Tumors ofDifferent Tissues or Organs. Cancer March-April 1961; 14:231- 237
11. Moertel C, Dockerty M, Baggenstoss A. Multipleprimary malignant neoplasms, Tumors ofMulticentric Origin, Cancer March-April, 1961;14:238- 248
12. Pavlov V. Colorectal carcinoma in the contextof multiple primary malignancy - diagnosis,

16 Bulgarian medicine vol. 7 № 1/2017
operative treatment and prognosis. Phd Thesis2015; 3-12
13. Pifrcev. K, Slaughter P. Association of breastand pelvic disease. Cancer 1: 468-471, 1948
14. Stalkerl K, Philips R Pemberton, J. Multiple pri-mary malignant lesions. Surg Gynec Q Obst1939; 68:595-602
15. Taylor, H. Coincidence of primary breast anduterine cancer. Am J Cancer 1931; 15:277-279
16. Vogt A, Schmid S, Heinimann K, et al. Multipleprimary tumours: challenges and approaches,a review. 2017; 10.1136/esmoopen-2017-000172
17. Warren S, Ehrenreich T. Multiple primarymalignant tumors and susceptibility to cancer.Cancer Res 1988; 4:744
18. Warren S, Ehrenreich T. Multiple primarymalignant tumors and suspectibility to cancer.Cancer Res 1944; 4:554-570
19. Warren S, Gates O. Multiple primary malignanttumors: a survey of the literature and a statis-tical study. Am J Cancer 1932; 16:1358–414
20. Whipham T; Quoted by CORNES JS (CornesJS). Multiple primary cancers: primary malig-nant lymphomas and carcinomas of the intes-tinal tract in the same patient. J Clin Pathol1960; 13:483-489 doi:10.1136/jcp.13.6.483
21. Wood M , Vogel V, Ng A et al . Second malig-nant neoplasms: assessment and strategies forrisk reduction. J Clin Oncol 2012; 30:3734–4doi:10.1200/JCO.2012.41.8681
Адрес за кореспонденция:
Д-Р ГАБРИЕЛА РАйчЕВА
Катедра Клинична ОнкологияМедицински Университет –
ПловдивКлиника по Медицинска ОнкологияУМБАЛ „Св. Георги” - ЕАД, Пловдив
Tel /fax + 359 32 602 880; +359 899 267 946
E-mail: [email protected]
Corresponding author:
GABRIELA RAyChEVA, MD
Department of Clinical Oncology Мedical University, Faculty
of Medicine – PlovdivUniversity Hospital
„Sv. Georgi” – PlovdivClinic of Medical Oncology
Tel /fax + 359 32 602 880;+359 899 267 946
E-mail: [email protected]

Bulgarian medicine vol. 7 № 1/2017 17
Original articles
Ефекти на триптани второ поколение – фроватриптан и алмотриптан върху локомоторната активност при експериментален модел на мигренаСарачева К.1, Гетова Д.2
1Катедра по Фармакология и лекарствена токсикология, Фармацевтичен факултет, Медицински Университет Пловдив
2Лаборатория по експериментална невропсихофармакология,Технологичен център по спешна медицина, Пловдив, България
Effects of second generation triptans - frovatriptan and almotriptan on locomotor
activity in an experimental model of migraine. Saracheva K.1, Getova D.2
1Department of Pharmacology and Drug Toxicology, Faculty of Pharmacy, Medical University Plovdiv, Plovdiv, Bulgaria
2Laboratory of experimental neuropshychopharmacology, Technological center of emergency medicine, Plovdiv, Bulgaria
РЕЗЮМЕ:
Целта на настоящето проучване е да сеустановят ефектите на фроватриптан иалмотриптан върху локомоторната актив-ност на мъжки и женски плъхове с моделна мигрена. Материали и методи: Бяхаизползвани бели мъжки и женски плъховепорода Wistar (12 групи: 6 – мъжки и 6 –женски, n=8) третирани с : Контрола (физ.разтвор) субкутанно; Нитроглицерин 10мг/кг интраперитонеално (НТГ); НТГ +Фроватриптан 2,5 мг/кг субкутанно; НТГ +Фроватриптан 5 мг/кг субкутанно; НТГ +Алмотриптан 3 мг/кг субкутанно; НТГ +Алмотриптан 6 мг/кг субкутанно. В апарата
ABSTRACT
The aim of this experiment was to evalu-ate effects of frovatriptan and almotriptan onlocomotion in male and female rats withexperimental model of migraine. Materialsand methods: Male and female Wistar ratswere used (12 groups: 6 – male, 6- female,n= 8) treated with: Control (saline) s.c;Nitroglycerin (NTG) 10 mg/kg i.p; NTG +Frovatriptan 2,5 mg/kg s.c; NTG +Frovatriptan 5 mg/kg s.c; NTG + Almotriptan3 mg/kg s.c; NTG + Almotriptan 6 mg/kg s.c.In Activity Cage apparatus was registeredhorizontal and vertical activity of each rat for5 minutes. The statistic evaluation was done

18 Bulgarian medicine vol. 7 № 1/2017
INTRoDuCTIoN
Serotonin (5-HT) is very important monoa-mine neurotransmitter and plays a significantrole in modulating locomotor activity.Moreover, different subtypes of 5-HT recep-tors modulate motor functions in rodents,including 5-HT1A, 5-HT1B, 5-HT1D [5].
The key mechanism of frovatriptan andalmotriptan action in migraine is their agonistactivity on 5-HT1B/1D receptors and moderateaffinity to 5-HT1A receptors [3,6].
Different neuronal pathways participate inthe regulation of locomotor activity - glutama-tergic, noradrenergic, dopaminergic and sero-toninergic. Most of the receptor subtypes(including 5-HT1A/B/D) are expressed in moto-neurons. [9].
The aim of this experiment was to evalua-
te some effects of frovatriptan and almotri-ptan on locomotion in male and female ratswith experimental model of migraine.
MATERIALS AND METhoDS
AnimalsWe used male and female Wistar rats with
initial body weight 200-220g. The rats werehoused in standard laboratory conditions (23-25°C, 50-55% humidity and 12/2h light/darkcycle) and fed with standard commercial foodand given water ad libitum.
Experimental migraine model was inducedvia intraperitoneal (i.p.) injections with nitrog-lycerin 10 mg/kg (NTG). 130 h after NTG admi-nistration, rats were treated subcutaneously(s.c.) with triptans. The rats were divided intotwelve groups (6 male and 6 female groups,
„Activity Cage” се регистрираха броя хори-зонтални и вертикални движения на всякоживотно еднократно за 5 минути.Статистическата обработка на данните бенаправена чрез програмата SPSS (17.0).За всяка група бе изчислено средната ѝстойност (mean) и стандартната ѝ грешка(SEM). Резултати: Женските плъхове тре-тирани с фроватриптан и в двете дози, ста-тистически значимо завишиха хоризонтал-ната активност спрямо групата третиранасамо с модел, докато ниската доза фрова-триптан завиши само вертикалната актив-ност. Женските плъхове третирани с алмо-триптан и в двете дози не променихацялостната локомоторика. Мъжките групиплъхове третирани с фроватриптан 2,5мг/кг достоверно завишиха хоризонтална-та и вертикална активност спрямо модел-ната група с нитроглицерин. Групата салмотриптан 6 мг/кг значимо занижи хори-зонталната активност, а вертикалната небе променена. Заключение: Нашитерезултати ни позволяват да предположим,че повишената експлораторна активностпри мъжките плъхове с фроватриптан седължи на пресинаптична регулация чрез5-HT1A, 5-HT1B рецепторите локализира-ни върху мотоневроните.
Ключови думи: локомоторика, фрова-триптан, алмотриптан, плъхове, модел намигрена
by SPSS (17.0) by calculating mean and SEMfor each group. Results: Female rats treatedwith frovatriptan in both doses, significantlyincreased the horizontal activity compared tothe group treated only with NTG. The lowdosage of frovatriptan increased only the ver-tical activity. Female groups of rats treatedwith almotriptan in both doses did not showsignificant changes in total motor activity.Male rats injected with low dosage frovatrip-tan increased significantly horizontal activitycompared to the group treated only with NTG.Frovatriptan in both doses, applied in malerats significantly increased the vertical activitycompared to the model group. Male ratstreated with the high dosage almotriptan sig-nificantly decreased the horizontal activity,while vertical activity was not changed.Conclusion: Our results permitted to suggestthat the increased exploring activity in bothrat sexes, treated with frovatriptan is due tosome presynaptic regulation that comesdirectly from both 5-HT1A, 5-HT1B receptors,localized on motoneurons.
Key words: locomotion, frovatriptan,almotriptan, rats, migraine model
Bulgarian medicine vol. 7 № 1/2017 19
n=8) as it follows: Control group – treatedwith saline 0.1 ml/100g s.c. Second group,treated only with NTG 10 mg/kg i.p. Thirdgroup, treated with NTG 10 mg/kg i.p andFrovatriptan 2.5 mg/kg s.c. Fourth group,treated with NTG 10 mg/kg i.p andFrovatriptan 5 mg/kg s.c. Fifth group, treatedwith NTG 10 mg/kg i.p and Almotriptan 3mg/kg s.c. and sixth group, treated with NTG10 mg/kg i.p and Almotriptan 6 mg/kg s.c.
All experiments were carried out accordingto the guidelines of laboratory animals in EU-guidelines/EEC Directive of 1986.
SubstancesSodium chloride solution 0.9% (saline) was
purchased from B.Braun Medical EOOD (Sofia,Bulgaria). Both triptans were purchased as puresubstances Frovatriptan succinate monohydrateand Almotriptan malate from Sigma-Aldrich(USA), and NTG was purchased as Nitronalsolution. (G. Pohl-Boskamp GmbH & Co).
Locomotor activity test The original automatic activity cage (Ugo
Basile, Italy) with UV detector for horizontaland vertical movements was used. The ratswere tested 40 min after the administration(s.c.) of triptans. Each rat had single test for 5min. The horizontal and vertical movementswere measured in relative units.
STATISTICAL EVALuATIoN
Data management was performed in SPSS17.0 statistical software. All observed para-
meters were expressed as mean ± S.E.M foreach group. A value of P<0.05 was consideredrepresentative of a significant difference.
RESuLTS
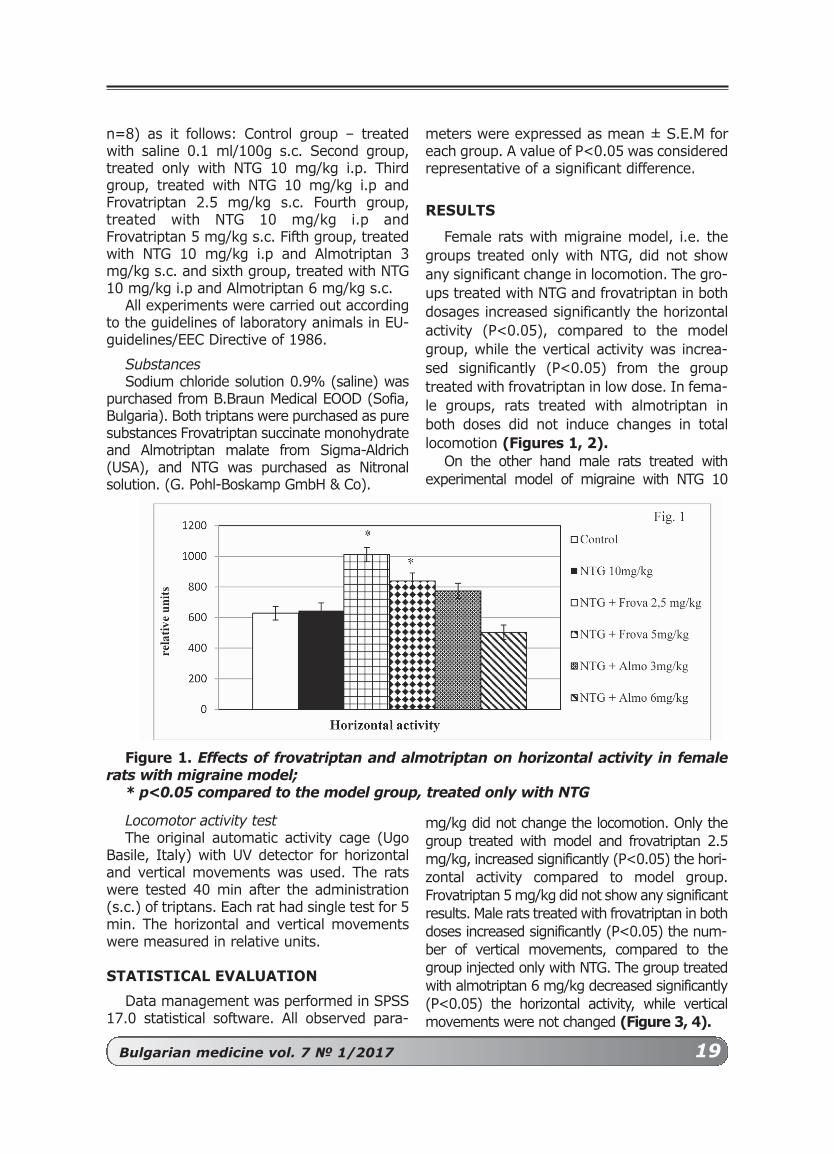
Female rats with migraine model, i.e. thegroups treated only with NTG, did not showany significant change in locomotion. The gro-ups treated with NTG and frovatriptan in bothdosages increased significantly the horizontalactivity (P<0.05), compared to the modelgroup, while the vertical activity was increa-sed significantly (P<0.05) from the grouptreated with frovatriptan in low dose. In fema-le groups, rats treated with almotriptan inboth doses did not induce changes in totallocomotion (Figures 1, 2).
On the other hand male rats treated withexperimental model of migraine with NTG 10
mg/kg did not change the locomotion. Only thegroup treated with model and frovatriptan 2.5mg/kg, increased significantly (P<0.05) the hori-zontal activity compared to model group.Frovatriptan 5 mg/kg did not show any significantresults. Male rats treated with frovatriptan in bothdoses increased significantly (P<0.05) the num-ber of vertical movements, compared to thegroup injected only with NTG. The group treatedwith almotriptan 6 mg/kg decreased significantly(P<0.05) the horizontal activity, while verticalmovements were not changed (Figure 3, 4).
Figure 1. Effects of frovatriptan and almotriptan on horizontal activity in femalerats with migraine model;
* p<0.05 compared to the model group, treated only with NTG

20 Bulgarian medicine vol. 7 № 1/2017
DISCuSSIoN
The abundance of 5HT1B/1D receptors insome subcortical brain regions – caudateputamen, n. accumbens, hypothalamus andalso in the frontal cortex in mice, rats and gui-nea pigs, suggests their participation in modu-lating locomotor activity [10].
Other authors describe the possibility 5-HT1A, 5-HT1B, 5-HT2A, 5-HT2C and 5-HT3receptors to regulate dopaminergic activation,GABA neurons and serotonin projections tostriatum, which in their turn, perform presy-naptic serotonin regulation on dopaminerelease [1].
Our experiments showed that female ratstreated with the NTG migraine model and fro-vatriptan increased the total locomotion.Frovatriptan possesses high agonist activity to5-HT1B receptors (pKi = 8.6). The specificlocation of these receptors on GABA neuronsin the ventral tegmentum and their influencefrom frovatriptan indirectly leads to increaseddopaminergic transmission in these areas,respectively, and dopamine levels [11].
The above mentioned suggests that frova-triptan’s high affinity to 5-HT1B receptor couldinfluence locomotor activity in male and fema-le rats. In an experimental study Borycz et al.
Figure 2. Effects of frovatriptan and almotriptan on vertical activity in female ratswith migraine model;
* p<0.05 compared to the model group, treated only with NTG
Figure 3. Effects of frovatriptan and almotriptan on horizontal activity in male ratswith migraine model;
*p<0.05 compared to the model group, treated only with NTG

Bulgarian medicine vol. 7 № 1/2017 21
(2008) explored 5HT1B/1D receptor agonistSKF99101H activity and detected hyperloco-motive activity in guinea pigs, which is anot-her proof of the participation of 5-HT1B recep-tors in the motor activity at all [4].Frovatriptan is a full agonist with moderateaffinity to 5-HT7 receptors (pKi/IC50 =6.7)[2]. A large number of immunohystochemicalstudies prove the location of this receptor inthalamus, hypothalamus and hippocampus.All these structures are also proven to beinvolved in motor activity in rodents whichgives us the reason to suggest that 5-HT7receptors do not play a minor role in the exp-loratory activity in male and female rats [8].
Decreased horizontal activity in male ratstreated with almotriptan 6 mg/kg probablycould be due to almotriptan’s agonist activityto 5-HT1A receptors (pKi/IC50 =7.4), forwhich scientific data describes a possible sup-pressive role on locomotion in male rats, trea-ted with NTG migraine model [7].
CoNCLuSIoN
Frovatriptan showed better results in the„open field” test in both rat sexes, while thesuppressed motor activity in the rats treatedwith almotriptan is a consequence of its ago-nist activity to 5-HT1A receptors.
Figure 4. Effects of frovatriptan and almotriptan on vertical activity in male ratswith migraine model;
*p<0.05 p<0.05 compared to the model group, treated only with NTG
REFERENCES:
[1] Alex KD, Pehek EA. Pharmacologic mecha-nisms of serotonergic regulation of dopamineneurotransmission. Pharmacol.Ther. 2007;113:296–320.
[2] Balbisi EA. Frovatriptan: a review of pharma-cology, pharmacokinetics and clinical potentialin the treatment of menstrual migraine. TherClin Risk Manag. 2006; 2(3):303-8.
[3] Bookshire BR, Jones SR. Direct and indirect 5-HT receptor agonists produse gender specificeffects on locomotor and vertical activities inC57 BL/6J mice. Pharmacol. Biochem. Behav.2009; 94(1):194-203.
[4] Borycz J, Zapata A, Quiroz C et al. 5-HT 1Breceptor-mediated serotoninergic modulation ofmethylphenidate-induced locomotor activation
in rats. Neuropsychopharmacology. 2008;33:619–626.
[5] Ghosh M, Pearse D. The role of the serotonin-ergic system in locomotor recovery after spinalcord injury. Frontiers in neural circuits. 2015;8:1-14.
[6] Godinez-Chaparro B, Lopez- Santillian FJ,Arguelles CF et al. Role of 5-HT1B/1D receptorsin the reduction of formalin- induced nocicep-tion and secondary allodynia/ hyperalgesia pro-duced by antimigraine drugs in rats. LifeSciences. 2013; 92(22):1046-54.
[7] Gras J, Llenas J, Jansat JM et al. Almotriptan,a new anti-migraine agent: a review. CNSDrug Rev. 2002; 8(3):217-34.
[8] Hedlund PB, Sutcliffe JG. Functional, molecu-lar and pharmacological advances in 5-HT7receptor research. Trends Pharmacol Sci. 2004;

22 Bulgarian medicine vol. 7 № 1/2017
25(9):481-6.[9] Humphreys JM, Whelan PJ. Dopamine exerts
activation-dependent modulation of spinal loco-motor circuits in the neonatal mouse. JNeurophysiol. 2012; 108(12):3370-81.
[10] O’Neill MF, Fernandez AG, Palacios JM.Activation of central 5-HT1B receptors
increases locomotor activity in mice. Hum.Psychopharmacol. 1997; 12:431–435.
[11] O'Dell LE, Parsons LH. Serotonin1B receptorsin the ventral tegmental area modulatecocaine-induced increases in nucleus accum-bens dopamine levels. J.Pharmacol.Exp.Ther.2004; 311:711–19.
Адрес за кореспонденция:
КРЕМЕНА САРАчЕВА,магистър фармацевт
Катедра по фармакология и лекарствена токсикология,
Факултет по фармация, Медицински университет - Пловдив
E-mail:[email protected]
Corresponding author:
KREMENA SARAChEVA,MPhARM,
Department of Pharmacology and Drug Toxicology, Faculty
of Pharmacy, Medical University of Plovdiv, Bulgaria
E-mail: [email protected]
Bulgarian medicine vol. 7 № 1/2017 23
Comparison of body weight, BMI, glucoselevel, blood pressure and heart rate
in different groups of patients included in NIRDIABo project from Plovdiv
Getova D.1, Dimitrova D.1,2, Topolov M.1,3
1Laboratory of Neuropsychopharmacology, High Technological Center for Emergency Medicine Plovdiv;
2Departmet of Pharmacology and Clinical Pharmacology, Medical Faculty, Medical University Plovdiv;
3Department of Pharmacology and Drug Toxicology, Faculty of Pharmacy, Medical University Plovdiv, Bulgaria.
Сравняване на телесното тегло, BMI, нивата на глюкоза, кръвното налягане и пулсовата честота на различни възрастови групи пациенти включени в проекта НИРДИАБО от ПловдивГетова Д.1, Димитрова Д.1,2, Тополов М.1,3
1Лаборатория по невропсихофармакология, Високотехнологичен център за спешна медицина Пловдив;
2Катедра по фармакология и клинична фармакология, Медицински факултет, Медицински университет Пловдив;
3Катедра по фармакология и лекарствена токсикология, фармацевтичен факултет, Медицински университет - Пловдив.
РЕЗЮМЕ:
Въведение: Цел на проучването е да сесравнят различни показатели (тегло, BMI,кръвна захар, кръвно налягане и пулс) вняколко възрастови групи от Пловдив и дасе оцени възможния риск от развитие надиабет тип 2. Метод: В изследването савключени доброволци с BMI над 25, разде-лени на 5 възрастови групи: a) 20-29г; б)30-39г; в) 40-49г; г) 50-59г; д) 60-69г(n=5-9). Вземането на кръвни проби еединствената слабо болезнена процедура.Първите 2 месеца пациентите са на нискокалорична диета 1200 калории дневно.
ABSTRACT
Introduction: The aim was to comparethe different values in age groups in NIRDIA-BO project from Plovdiv region and to evalu-ate the possible risk to develop pre-diabetes.Method: The volunteers with BMI over 25were included (male and female), divided in 5age groups: a) 20-29 years; b) 30-39 years;c) 40-49 years; d) 50-59 years; e) 60-69years (n=5-9). The only mild harmful proce-dure on the patients was taking blood sam-ples. First 2 months the patients had lowcaloric diet 1200 per day. The diet includedlow fat, moderate protein and low carbohy-

24 Bulgarian medicine vol. 7 № 1/2017
Диетата включва ниско съдържание намазнини и на въглехидрати, умерено набелтъци, както и прием на пробиотик.Резултати: Най-високо телесно тегло серегистрира в групата 40-49г. В същатагрупа са и най-високите нива на глюкоза вкръвта сутрин на гладно. След натоварва-не с глюкоза същата група показа най-високи стойности над тези на гладно. Неустановихме големи промени в систолнотои диастолно кръвно налягане или в пулсо-вата честота при всички групи пациенти.Заключение: Настоящето изследване емалък принос към поддържането на подхо-дящ стил на живот при хора с наднорменотегло и риск от развитие на пред-диабет идиабет тип 2 за българската популация,поради използването на ниско калоричнадиета, съчетана с прием на пробиотик иумерена физическа активност.
Ключови думи: ниско калоричнадиета, пробиотик, предпазване от разви-тие на диабет тип 2.
drate food and probiotics. Results: The bodyweight of the patients showed the highervalue had the group 40-49 years. The highermean values of blood glucose early morningare seen in a group of 40-49 years. After load-ing with glucose only the same group showedhigher level. We do not register very bigchanges in systolic and diastolic blood pres-sures as well as in heart rate, in all groups ofpatients. Conclusion: The present study hadimportant impact in management of pre-dia-betic people and prevention from developingdiabetes type 2 in Bulgarian population due tothe usage of probiotics with appropriate lowcaloric diet and increasing the everyday phys-ical activity.
Key words: low caloric diet, probiotic, pre-vention of type 2 diabetes.
INTRoDuCTIoN
Diabetes mellitus type 2, also known asnon-insulin dependent diabetes, is among themost rapidly spread diseases in the world.This tendency is mainly due to rise of overwe-ight and obesity in population. Usually peopleat first develop the so-called pre-diabetes,which can be prevented [6].
There are several risk factors that predis-pose the development pre-diabetes. They areconsidered the same risk factors as the factorsrelated to diabetes type 2.
Weight is one of them and it is measuredmainly by body mass index (BMI). When BMIis higher than 25, the patients are at high riskfor developing pre-diabetes. Especially if thepatient carry a lot of extra weight in his/herabdomen, he/she may develop pre-diabetes.The excess of fat cells can cause the body tobecome more insulin resistant [1].
The next risk factor is the lack of physicalactivity. This often goes hand-by-hand withbeing overweight. If a person isn’t physicallyactive, he/she is more likely to develop pre-diabetes. The family history should be taken inmind, because there are also some hereditaryfactors. If a patient’s close family member has
(or had) it, he/she is more likely to developthe disease [7].
Age is also an important risk factor, becau-se old-aged people are at high risk to developpre-diabetes. It was found, that at the age of45 this risk starts rising, and after the age of65, the same risk increases exponentially [5].
Other issues like high blood pressure(hypertension) and high cholesterol level,(especially the so called “bad” LDL choleste-rol) could increase very easily the risk ofacquiring diabetes type 2 [4].
The aim of our study was to compare somevalues examined in different age groups ofvolunteers that took part in the project “NIR-DIABO”. We have evaluated the possible riskfor each group to develop pre-diabetes. Thevolunteers were from the Plovdiv region andthey participated in the first year of the pro-ject.
METhoDS
The project aimed to examine the quality oflife and the effects of some non-pharmacolo-gical interventions on volunteers with obesityand high BMI. Both male and female volunte-ers with BMI over 25 were included in this

Bulgarian medicine vol. 7 № 1/2017 25
study, and were divided in the following gro-ups: a) 20-29 years of age; b) 30-39 years ofage; c) 40-49 years of age; d) 50-59 years ofage; e) 60-69 years of age. The number ofpatients in each age group was relativelysmall (n=5-9).
All volunteers have signed a form of con-sent that they took part in the study. TheEthical Committee of Medical Universityapproved the study. The written consent inclu-des an information who of the included pati-ents have a risk of developing pre-diabetes ordiabetes type 2. If a patient followed correctlyall the written instructions and kept the neces-sary diet he/she would have low chance todevelop diabetes type 2. The results wouldhelp the patient to prevent the developmentof some cardio-vascular diseases. Thereweren’t any harmful procedures on the pati-ents excluding the weak discomfort whenblood samples were taken. It was possible fora patient to become hungry, or to suffer froma weak headache, or to feel cold, but suchreactions usually are weak and diminish easilyin the first weeks.
We have formed the following includingfactors and criteria: 1. A written and signed consent for taking part
in the study;2. BMI over 25.3. To perform a 2 hours of glucose-loading
test for study glucose tolerance.4. Motivation to take part in the study and fol-
lowing the necessary protocol for it.Excluding factors and criteria:
1. Patients with diabetes type 2 diagnose.2. Chronic diseases requiring medications that
could influence the levels of blood glucose.3. Taking part in active sport and games.4. Specific food regimen – as vegans, etc.5. Psychiatric diseases like anorexia or drug
dependence.6. Regular intake of alcohol over 21 Units for
men and 15 Units for women per week.The non-pharmacological interventions of
the study are the following:1. Two stages of diet performing;2. Moderate physical activity;3. Psychological influence.The first 2 months of the study all the pati-
ents had to run a low caloric diet of 1200 kcalper day. This diet included 5 times of food
intake during the day, but one of the nourish-ments had to be replaced with a product con-taining probiotics. The other nourishmentshad low fat, low carbohydrate, moderate pro-tein containing food. The objective was for 2months the patients to lose up to 5 % ofweight compared to the basal one.
We used „TANITA C 300 BC-420 MA bodycomposition analyzer” apparatus (USA) tomake the following measurements: age, sex,body weight, BMI. The blood pressure andpulse frequency were measured on patients’forearms by Tensoval apparatus (Hartmann,Germany). To measure waist, hips, tights, weused a simple soft tailor ruler.
Statistics: all observed values were calcula-ted and the mean for each group was estima-ted. Because of the small number of patientsin each age group the statistical significancewas not determined.
RESuLTS
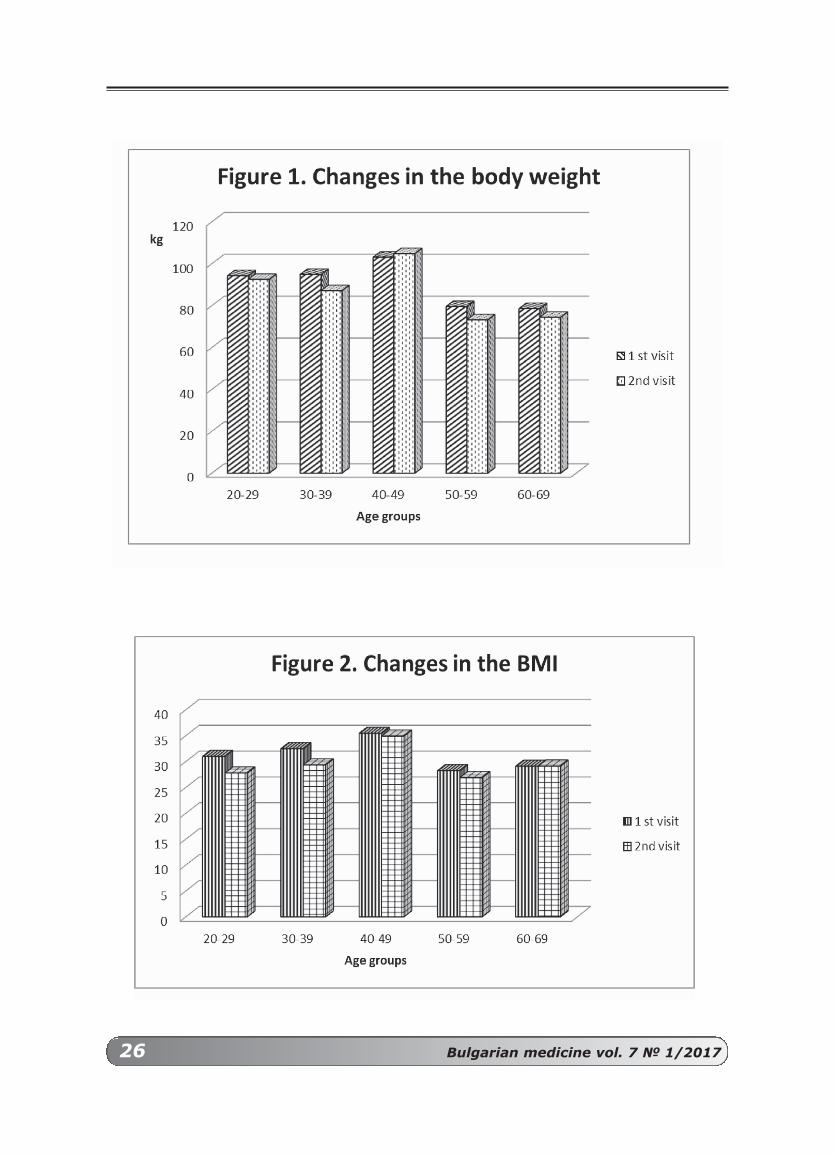
The results included in this study showedthat the age group 40-49 years had a highervalue of body weight. This group is very resis-tant to reduce body weight, despite the pre-sence of the diet. Even the fact that patientshad been following the instructions of thestudy and maintaining the new low-caloricdiet, they did not decrease weight. There isnot enough data to make a complete compa-rison of the values for statistically significantdifferences, but the tendency is quite clear(Fig. 1.).
The same tendency, we could see in theFig. 2 which illustrates the differences in BMIfor all groups of patients. Again, the middle-aged group (40-49 years old patients) did notdecrease BMI.
Patients from different age groups showeddifferent mean values of blood glucose early inthe morning on empty stomach (Fig. 3). Thehighest values are observed in the 40-49years old patients group. After loading withglucose only the above mentioned group sho-wed higher levels of blood glucose comparedto the levels before loading.
We did not register big changes in systolicand diastolic blood pressures in all groups ofpatients (Tabl. 1). Only for the systolic pre-ssure we found a slight tendency to decrease
26 Bulgarian medicine vol. 7 № 1/2017

Bulgarian medicine vol. 7 № 1/2017 27
during the second visit, probably due to theslight increase in the every day physical acti-vity, which was reported by the patients andthe low caloric diet, especially in the age group40-49 years. The heart rate was also not sig-nificantly changed in all groups.
DISCuSSIoN
Our results permit the suggestion that themain risk group is the group of 40-49 years ofage. They showed higher body weight, BMIand level of blood glucose before and after theglucose loading test. The other groups sho-wed weak decrease in their body weight andBMI after 2 months of low caloric diet, havingin mind, that patients from these groups werekeeping a moderate physical activity. This is inaccordance with some clinical studies showingthat lifestyle modification and low caloric dietare among the favorable factors contributingto the successful life without complications ofdiabetes type 2 for overweight people [1]. Thedecreased weight was not so high, but for along term period if the patients maintain thisweight or even decrease it, that would be a
big success of the NIRDIABO study. Lifestyle modifications, including both heal-
thy eating choices and increased physical acti-vity, are essential for weight management anddiabetes prevention [2, 8]. Garber [2] found,that the designed his Program for diabetesprevention and the modulation of some para-meters individually for each patient haveshown repeated success and long-term main-tenance. He made the conclusion that obesityis rather a metabolic disorder than a personalweakness. It may work with patients to add-ress this condition and improve long-termhealth outcomes. In our study during pati-ent’s visits we talk with them on this matter.
There is strong, consistent evidence thatthe relationship between blood glucose levelsand cardiovascular risk extends the diabeticrange and obesity [7]. The same authorsassumed that obesity and diabetes alsoincrease the risk of heart failure, independentof coronary heart disease and hypertensionand may cause cardiomyopathy (a frequent)and often fatal complications. In our studyonly middle age group (40-49 years of age)showed the tendency for none tolerance to

28 Bulgarian medicine vol. 7 № 1/2017
glucose loading. This group on our opinion isat higher risk for developing pre-diabetes andlater on diabetes type 2, if the patients do notchange their life style and do not keep the lowcaloric diet and more daily physical activity.
Some authors [9] found, that the obesepeople presented higher blood pressure andheart rate values at rest, compared to the eut-rophic ones. They assume that probably suchresults may be explained by a reduction inparasympathetic activity and relative pred-ominance of sympathetic activity. Wang et al.,[10] suggest that annual blood pressure mea-surements are associated with increased sur-vival and the strategy is to improve measure-ment frequency in obese patients which sho-
uld be implemented. Our results support suchview. We do not found very bug changes whenwe compare the blood pressure and heart rateduring first and second visit, but even slightdecrease in systolic values are important.
CoNCLuSIoN
The present study has important impact inmanagement of pre-diabetic people and pre-vention from developing diabetes type 2 inBulgarian population. The use of probioticswith appropriate low caloric diet and increa-sing the everyday physical activity are themilestone key for prophylaxis of diabetes type2 in our country.
Table 1. The values of systolic and diastolic blood pressure as well as heart rate,measured during the first and the second visits. Mean values for each group.

Bulgarian medicine vol. 7 № 1/2017 29
REFERENCES:
1. Dileepan K, Feldt MM. Type 2 diabetes mellitusin children and adolescents. Pediatr. Rev., 2013,34(12): 541-8.
2. Garber AJ. Obesity and type 2 diabetes: whichpatients are at risk? Diabetes, Obes, Metab.,2012, 14(5): 399-408.
3. Kim OY, Lee JH, Sweeney G. Metabolomic pro-filing as a useful tool for diagnosis and treat-ment of chronic diseases: focus on obesity, dia-betes and cardiovascular diseases. Expert. Rev.Cardiovasc. Ther., 2013, 11(1): 61-8. Doi:10.1586/erc.12.121.
4. Leblanc ME, Cloutier L, Poirier P. Sensitivity,specificity and predictive values of a forearmblood pressure measurement method in severeobesity. Blood Press. Monit., 2015, 20(2): 79-82. Doi:10.1097/MBP.00000000000000000097.
5. Marcovecchio ML, Chiarelli F. The effects of acuteand chronic stress on diabetes control. Sci.Signal, 2012, 5(247): pt.10. doi:10.1126/scisignal.2003508
6. Nicolls SJ, Brown A. Targeting obesity, diabetesand the metabolic syndrome: are we trying toclose the barn door after the horse bolted?Exprt. Rev. Cardiovasc. Ther., 2014, 12(3):279-90. Doi: 10.1586/1479072.2014.894362.
7. Picard F, dos Sants P, Catargi B. Diabetes, obe-sity and heart complications. Rev. Prat., 2013,63(6): 759-64.
8. Rajalakshmi R, Nataraj SM, Vageesh V, Dhar M.Blood pressure responses to steady treadmillexercise in overweight and obese young adults.Indian J. Physiol. Pharmacol, 2011, 55(4): 309-14.
9. Rossi RC, Vanderlei LC, Goncalves AC, VandeleiFM, Bernardo AF, Yamada KM, da Silva NT, deAbreu LC. Impact of obesity on autonomicmodulation, heart rate and blood pressure inobese young people. Auton. Neurosci., 2015,193: 138-41. Doi:10.1016/j.autneu.2015.07.424.
10. Wang S, Majumdar SR, Padwal R. BMI, annualblood pressure measurements and mortality inpatients with obesity and hypertension. BloodPress. Monit., 2015, 20(2): 32-8. Doi:10.1097/MBP000000000000000087.
Адрес за кореспонденция:
Проф. д-р ДАМЯНКА ГЕТОВА
Лаборатория по невропсихофармакология,Високотехнологичен център
за спешна медицина, Пловдив.E-mail: [email protected]
Corresponding author:
Prof. Dr. DAMIANKA GEToVA
Laboratory ofNeuropsychopharmacology,
High Technological Center forEmergency Medicine, Plovdiv.
E-mail: [email protected]

30 Bulgarian medicine vol. 7 № 1/2017
Персонализирана радиационнаонкология - концепция,реални клинични възможности В. Попов1, И. Михайлова1,2, Ж. Грудева-Попова1
1Катедра по клинична онкология - Медицински университет, Пловдив1Университетска болница „Св. Георги" - Пловдив2Радиотерапия, Специализирана болница за Активно Лечение в Онкология - София
Personalized radiation oncology -concepts, real clinical possibilities
V. Popov1, I. Mihaylova1,2, Zh. Grudeva-Popova1
1Department of Clinical Oncology - Medical University, Plovdiv1University Hospital „Sv. Georgi” - Plovdiv
2Department of Radiotherapy, Specialized Hospital for Active Treatment in Oncology - Sofia
РЕЗЮМЕ:
Целта на съвременната противораковатерапия е да се приложи генетичнаинформация за тумора, която да ръково-ди решенията за персонализирано лече-ние. Този подход се отнася до комплекс-но лечение на рак, но в момента най-голямата и най-реалистична употреба е вхимиотерапията, особено целенасоченатерапия. Интег рирането на биологичнатаинформация за подобряване на радиаци-онната стратегия и съответно на терапев-тичния отговор може да се определи катоперсонализирана лъчева терапия. Затази цел са необходими надеждни про-гнозни биологични маркери, за да сехарактеризира индивидуалната ефектив-на радиационна реакция и възможносттаза радиална токсичност. Задачата е труд-на и създава много въпроси, свързани сизбора на типа радиотерапия, фракцио-ниращи схеми, комбинирани модалностии др. Потенциалните маркери за пред-
ABSTRACT
The goal of modern anticancer thera-py is to apply genetic information abouta tumor to guide decisions on personali-zed therapy. This approach concernscomplex cancer treatment, but currentlythe largest and most realistic use is inchemotherapy, especially targeted the-rapy. Integrating biological informationto improve the radiation strategy andthe therapeutic response, respectively,can be defined as personalized radiationtherapy. For this purpose reliable predic-tive biological markers are required tocharacterize the individual effectiveradiation response and the possibility ofradial toxicity. The task is difficult andcreates many issues related to the choi-ce of type of radiotherapy, fractionationschemes, combined modalities, etc.Potential predictive markers should bediscussed as a hypoxia markers, mar-kers of DNA repair, markers of different

Bulgarian medicine vol. 7 № 1/2017 31
INTRoDuCTIoN
The goal of modern anticancer therapy is toapply genetic information about a tumor toguide decisions on therapy. This personalizedtherapy approach is a considerable deviationfrom traditional combined-modality therapy,where surgery, chemotherapy, and radiationtherapy (RT) are integrated in regimens tailo-red to the site of origin and stage of thetumor [1].
Clonal evolution and the „survival of thenastiest” remain the chief obstacles to curingcancer. But what if we could find a way to usethe principles of evolution to beat evolvingcancers cells at their own game? Is it possibleto use Darwin;s notebook to outsmart resis-tance and cancer survival? May be – targetingthe evolutionary trunk… truncal tumor neoan-tigens could allow scientists to target anddestroy tumors without harming healthy tis-sues. The heterogeneity will nearly lead to thefailure of therapies that target specific types ofcell.
RADIoThERAPy (RT)
Approximately 60% of all patients withcancer perceive RT at some point during theirtreatment course. The interaction of radiationand chemotherapy was prominently describedin the 1970s by George Steed, who postulatedfour mechanisms by which combined modalitytreatment could improve clinical outcomes[2]. Patients show an individual response tothe standard RT (fraction of 2 Gy daily for 6-7weeks). The main guidelines for optimizingthe therapeutic efficacy of radiation therapyare aimed at improving the physical and tech-nical parameters - dose and optimization ofthe treatment plan.
Chemoradiation is the standart therapyfor the majority of inoperable, locally advan-ced cancers. While there is a need to improvechemoradiation efficacy, normal tissue toxicitylimits our ability to give additional chemothe-rapy or higher doses RT. Thus, there is excite-ment about the addition of molecularly targe-ted agents, which tend to be less toxic thanchemotherapy, to chemoradiotion regimens.Unfortunately, initial empiric attempts havenot been successful. We focus on the evidencethat supports rational combinations of targe-ted agents with chemoradiation, with anemphasis on agents that target the DNAdamage response and radiation-inducedmembrane signaling.l Sensiting to chemoradiation by directly tar-
geting the DNA damage response – PI3K /AKT, MEK, TGF-beta
l Sensiting to chemoradiation by alternativestrategies
l Sensiting to chemoradiation by targetingradiation-induced membrane signaling –EGFR, VEGFREliminating chemotherapy by a dual-targe-
ted approach with radiation [3]. Studies of stereotactic ablative body RT, in
particular, suggest improved clinical outcomecompared with those previously seen withcombination of conventional radiation andchemotherapy. Although ablative treatmentsmay continue to gain traction in early-stageand oligometastatic disease, in which targetsare generally smaller and often better defined,it is unlikely that further advances in physicaltargeting and fractionation alone will result inmarked improvements in survival among pati-ents with locally advanced disease [4].
Relatively fewer efforts of researchers arefocused on including individual patients`s
сказване трябва да бъдат обсъденикато маркери на хипоксия, маркери запоправка на ДНК, маркери на различниотделения на туморна микросреда,маркери за ангиогенеза и противора-ков имунитет.
Ключови думи: лъчева терапия,персонализирана лъчетерапия, пред-сказващи маркери
compartments of the tumor microenvi-ronment, angiogenesis markers and anti-cancer immunity.
Key words: radiation therapy, perso-nalized radiotherapy, predictive markers
32 Bulgarian medicine vol. 7 № 1/2017
characteristics in determining the treatmentstrategy. There are various radiobiological fac-tors that contribute alone or in combinationfor the tumor response to radiotherapy. Theseinclude a number of stem cells and their irra-diation, repopulating capacity and reoxygena-tion in the course of radiation therapy, recove-ry of radiation tissue damage and tumorhypoxia. These indicators were researched inexperimental and clinical studies as individualirradiation factors [5].
PERSoNALIZED RADIoThERAPy
Integrating biological information to impro-ve the radiotherapy strategy and therapeuticresponse can be defined as a personalized RT.To do this, reliable predictive biological mar-kers are needed which can be used to deter-mine optimal dose, choice of fractionationschemes, or combined modalities. Biomarkerscan also be classified according to modality ofassessment , and this has implication for howparticular biomarker might be developed. Themost common types of biomarkers accordingto this classification are [6]:1. Genetic (gene mutation, gene copy num-
ber, translocations) – EGFR, HER2, BCR-abl2. Genomic ( gene expression profiles) –
Mamma Print3. Protein (serum protein assays)4. Proteomic (analysis of serum or tumor)5. Pathological (immunohistochemistry, histo-
patology)6. Imaging (PET, Blood Oxygen Level Depend
- fMRI)7. Other (Circulating Tumor Cells)
The recent progress in this area focusing onthe key stages in the biomarker developmentprocess: discovery, validation, qualificationand implementation [6]. Validation of biomar-ker involves a systematic evatuation to assurethat the technique used to assay the biomar-ker is reliable to perform its task. The processis guided by the established principles of bio-analytical method validation [7].
The currently used pretreatment parame-ters for evaluating and selecting the appropri-ate treatment plan currently include: histolo-gicy, stage of differentiation, performance sta-
tus and stage, but tumor associated biologicalparameters are not discussed. Typically,tumors are characterized by heterogeneity,which may become more pronounced duringthe course of complex treatment. The availa-bility of reliable predictive early response the-rapies would improve and individualize RT ofthe patient. Typically, tumors are characteri-zed by heterogeneity, which may becomemore pronounced during the course of com-plex treatment. The availability of reliablepredictive early response therapies wouldimprove and individualize the patient's RT. Thepossibilities of individualizing RT schemes sho-uld be based not only on morphological crite-ria but also on biological information related tothe tumor. Important indicators at baselineand during radiation therapy may be hypoxicstatus, angiogenesis, metabolic and prolifera-tive activity, activity of DNA repair systems inthe course of applied radiotherapy. In contrastto the relatively wide use of a personalizedtherapeutic approach in medical oncology, RTstatus is more conservative.
1. Individualization of Radiotherapybased on hypoxia markers
Experimental and clinical data demonstratethe role of tumor hypoxia for malignant pro-gression and RT resistance [5,8]. The mecha-nisms that can explain this association are lis-ted above: l Oxygen effect – three times higher radiation
resistance of cells in conditions of hypoxiadue to cells with normal oxygenize.
l Selection of resistant clones during carcino-genesis through hypoxic-induced acute andchronic changes in gene expression.Identifying hypoxic tumors allows the deve-
lopment of strategies to potentially overcomethe hypoxic condition [5]. For example: increa-sed oxygen import before / during irradiation,use of oxygen carriers as radiosensitizers,direct cytotoxicity by using reductant compo-unds. Results from clinical trials have shownthat some of these strategies have the poten-tial to improve the therapeutic response.However, while the prognostic value of thevarious hypoxicity markers is confirmed by anumber of experimental and clinical trials, their

Bulgarian medicine vol. 7 № 1/2017 33
feasibility as predictive markers for the indivi-dualization of therapy in hypoxic tumors hasbeen studied in a small number of studies
Serum protein оsteopontin is associatedwith tumor hypoxia with potential mechanismof negative correlation wich von Hippel-Lindau(VHL) gene expression [5,8]. VHL regulatesoxygen-dependent uptake and proteolysis ofthe hypoxia-inducible transcription factor(HIF-1a). It activated transcription of genes,responsible for the adaptive response to hypo-xia. Hypoxia-induced osteopontin secretion invitro and osteopontin plasma levels correlatewith oxygen partial pressure in the tumor inpatients with leukemia and neck cancer. Highlevels of osteopontin as a marker for hypoxiaare associated with therapeutic failure afterradiotherapy.
2. Individualization of Radiotherapybased on markers of DNA repair
RT induces a series of DNA damage moreof which can be recovered from the affectedcell, but the unresolved damage causes celldeath and mutations. Proteins involved in therepair of DNA damage are considered as apotential biomarkers for therapeutic responseat RT [8]. One of the most studied markers isthe histone protein gH2AX, which accumulatesin the focus of double-stranded DNA damageand may affect other DNA proteins [9]. Inpatients with hypoxic tumors, a lower residualgH2AX expression was observed [9,10]. Theuse of DNA repair markers is useful in identi-fying potentially resistant tumors with effecti-ve DNA repair mechanisms. In these cases,combining radiation with an inhibitor of DNArepair mechanisms is an attractive approachto overcoming radiation resistance. As a sui-table biomarker, the poly (ADP-ribose)-poly-merase-1 (PARP) enzyme that protects thecell from apoptosis is considered. PARP inhibi-tors block DNA repair and select the tumorresponse to radiation in a number of pre-exis-ting in vivo tumor models. PARP inhibition hasbeen found to result in increased accumulati-on of gH2AX focuses in lung tumors. Thesedata justify accepting that PARP may serve asa biomarker candidate for the selection ofpatients eligible for combined radiation / tar-get therapy [8,9].
3. Individualization of Radiotherapybased on markers of different compar-tments of the Tumor MicroEnvironment(TME)
Tumor MicroEnvironment (TME) emergedas one of the key factors in therapy resistan-ce. Tumor stroma - a complexity dictated bythe hypoxic TME. RT as known to influenceand modify diverse components of the TME[11]. The impact of low and high single dose,as well as fractionated RT on host cells (endot-helial cells, fibroblasts, immune and inflam-matory cells) and the extracellular matrix.Optimizing the schedule of RT (i.e. dose perfraction) and other treatment modalities is acurrent challenge. RT has a nonspecific effect,triggering both tumor and host cells.
The effect on endothelial cells depends onthe dose per fraction. At a clinical single doseof 2 Gy, endothelial cell survival as favoredthrough miRHA upregulation. Low doses RT(<1 GY) can be used as a anti-inflammatorytreatment. High dose (above 10 Gy) are morelikely to induce endothelial cell apoptosis andtumor vessel collapse [12]. This could explainthe clinical efficacy of stereotactic body radia-tion therapy and stereotactic radiation surge-ry. With intermediate doses (5-10Gy) tumorvessel normalization and dilatation are obser-ved and associated with reduced vascular lea-kage and increased tumor oxygenation[13,14].
RT can initiate inflammatory cascades bytwo main pathway: the nuclear and cytoplas-mic pathway. NK cell mobilization followingneoadjuvant RT appears crucial. Normal fib-roblasts are well known to resist to high radia-tion dose (up to 50 Gy). Cancer-associatedfibroblasts actively contribute to cancer agg-ressiveness by modulating different processes– angiogenesis, inflammation and extracellu-lar matrix remodeling [11,14].
4. Radiotherapy and Cancer Immuno -genic Effects
The balance between proimmunogenic andimmunosuppressive effects of radiotherapyand tumor rejection is very difficult [15]..Radiation promotes the priming and effectorphases of the antitumor immune response.Key molecular signals that promote priming ofantitumor T cells by dendritic cells loaded with

34 Bulgarian medicine vol. 7 № 1/2017
tumor antigens include exposure ofCalReTiculin (CRT) and High-Mobility GroupProtein B1 (HMGB1). These signals are relea-sed by the tumor cells undergoing a radiation-induced immunogenic cell death and, togetherwith InterLeukin 1b (IL-1b) lead to activationof tumor-specific T cells. Key molecular signalsthat promote the effector phase include theupregulation of chemokines CXCL9, 10, and16, which attract activated T- cells to thetumor. Tumor infiltration by T cells produceInterFeroN y (IFN-y) and Tumor NecrosisFactor-alfa (TNF-a). The process is facilitatedby upregulation of Vascular Cellular AdhesionMolecule 1 (VCAM-1) on tumor endothelium[16]. Radiation-induced upregulation of MajorHistocompatibility Complex Class 1 (MHC-1)and InterCellular Adhesion Molecule-1 (ICAM-1) on surviving tumor cells improves theirrecognition and killing by T cells. On the otherhand, radiation activates immunosuppressiveTransforming Growth Factor-beta (TGF-b) andpromotes accumulation of regulatory T-cellsand protumorogenic M2 macrophages. Datasuggest that positive effects of radiation otherpredominate over negative ones but are insuf-ficient to shift the balance of the immunosup-pressive tumor microenvironment to achievetumor rejection in the absence of targetedimmunotherapy [15,17].
5. Individualization of Radiothe rapybased on Angiogenesis markers
Tumor blood vessels are recognized asmajor actors in tumor development at leastthrough an active and passive exchange ofnutrients, waste and gaz [13,16]. The effectsof ionizing radiations on angiogenesis aremore complex than might be expected. Thereare now at least three distinct ways in whichradiation can affect vessel growth:l The protons of electromagnetic radiations
stimulate vessel growth at least in part, bycausing the increased expression of angio-genesis factors.
l Low Linear Energy Transfer (LET) chargedparticles like protons inhibit angiogenesisby an unknown mechanism although dec-reased expression of angiogenesis factorsand reduced motile tip activity is implica-ted.
l High LET heavy ions like Fe ions also inhibitangiogenesis by an unknown mechanismthat affects the later stages of tubuloge-nesis. This complexity of response opens up pos-
sibilities of greater control over angiogenesisand the resulting pathologies during coinci-dent exposure or therapy. For exposure inspace, knowledge of these mechanisms willenable more precise risk assessment and liti-gation strategies. For radiotherapy, treatmentcould be manipulated to utilize the radiationeffectively. In addition, effectiveness can beincreased further when used in the right com-bination of anti-angiogenesis drugs. Furtherresearch in this field should contribute to agreat improvement in these strategies.
CoNCLuSIoN
The hypoxia markers, markers of DNArepair, the different compartments of TME andthe angiogenesis markers are closely relatedand contribute not only to tumor progression,but also to its treatment response. RT deliveryto the primary tumor, ionizing radiation alsotarget non tumor cells the influence tumorgrowth and metastatic dissemination. TheTME-mediated and the other models of radio-resistance is now the object of researchers[14,16]. However the impact of PERSONALI-ZED RT is often neglected. Here we pointedout the impact of this element of multimodaloncology treatment.
DISCLoSuRE
The authors have declared no conflicts ofinterest.

Bulgarian medicine vol. 7 № 1/2017 35
REFERENCES:
1. Giaccia A. Modern Radiobilogy: the State of theArt. J Clin Oncol 2014; 32(26):2871-2878.
2. Morris Z, Harari P. Interaction of radiationTherapy With Molecular Targeted Agents. J ClinOncol 2014; 32 (26):2886-2893.
3. Mogan M, Parsels L, Maybaum J, et al.Improving the efficacy of chemotherapy withtargeted agents. Cancer Discov 2014;4(3):280-291.
4. Iyengar P, Timmerman R. Stereotactic ablativebody radiotherapy for NSCLC: racionale andoutcomes. J Natl Compr Canc Netw 2012;10:1514-1520.
5. Yaromina A, Krause M, Baumann M.Individualization of cancer treatment fromradiotherapy perspective. Molecular Oncology2012; 6:211-21.
6. Alymani N, Smith M, Williams D, Petty R.Predictive biomarkers for personalized anti-can-cer drug use: Discovery to clinical implementa-tion. Euro J Cancer 2010; 46:869-879.
7. Sawyers C. The cancer biomarker problem.Nature 2008; 452(7187):548-552
8. Ree A, Redalen K. Personalized radiotherapy:concepts, biomarkers and trial design. Br JRadiol 2015; 88 (1051):20150009.
9. Ree A, Redalen K. Personalized radiotherapy:concepts, biomarkers and trial design. Br JRadiol 2015; 88 (1051):20150009.
10. Coleman C, Lawrence T, Kirsch D. Enhancingthe Efficacy of Radiation Therapy: premises,
Promises, and Practicality, J Clin Oncol 2014;32(26)2832-2835.
11. Leroi N, Lallemand F, Coucke Ph, et al. Impactsof Ionizing Radiation on the DifferentCompartments of the TumorMicroenvironment.Frontiers in Pharmacology2016; 7(78): 1-9.
12. Song C, Lee Y, Griffin R, et al. Indirect tumorcell death after high-dose hypo-fractionatedIrradiation: implications for stereotactic bodyradiation therapy and stereotactic radiation sur-gery. Int J Radiat Oncol Biol Phys 2015;93:166-172.
13. Sonveaux P, Brouet A, Havaux X, et al.Irradiation-indiced angiogenesis through theUp-regulation of the nitric oxide pathway.Cancer res 2003; 63:1012-1019.
14. Pitt J, Marabelle A, Eggermont A et al.Targeting the tumor microenvironment: remov-ing obstruction to anticancer immune respons-es and immunotherapy. Annals of Oncology2016; 27(8): 1482-1492.
15. Formenti S, Demaria S. CombiningRadiotherapy and Cancer Immunotherapy: AParadigm Shift. J Natl Cancer Inst 2013;105:256-265
16. Grabham P, Sharma P. The effects of radiationon angiogenesis. Vascular Cell 2013; 5:19-26.
17. Barker H, Paget JT, Khan A, Harrington K. Thetumor microenvironment after RT: mechanismsof resistance and recurrence. Nat Rev Cancer2015; 15:409-425.
Адрес за кореспонденция:
Д-Р ВЕСЕЛИН ПОПОВ
Медицински университет - Катедра по клинична онкология
Бул. В. Априлов 15А4002 Пловдив
E-mail: [email protected] Tel / Fax: +359 32 602 880
Corresponding author:
VESELIN PoPoV, MD
Medical University - Department ofClinical Oncology
15A V. Aprilov blvd4002 Plovdiv
E-mail: [email protected] Tel / Fax: +359 32 602 880

36 Bulgarian medicine vol. 7 № 1/2017
Вътреставни апликации с тромбоцит богата плазма за лечение на колянна остеоартрозаЖелязкова М., Тодоров П., Попова В., Каралилова Р., Баталов А.
Медицински Университет – Пловдив, Медицински Факултет, Катедра „Пропедевтика на Вътрешните болести”, УМБАЛ „Каспела”, Клиника по Ревматология.
Intra-articular platelet rich plasma injections
for Knee osteoarthritisZhelyazkova M., Todorov P., Popova V., Karalilova R., Batalov A.
Medical University of Plovdiv, Faculty of Medicine, Propedevtics of Internal Diseases,
UMHAT „Kaspela”, Department of Rheumatology
РЕЗЮМЕ:
Въведение: Представя се метод залечение на колянна остеоартроза с прила-гане на тромбоцит богата плазма вътрес-тавно. Съдържанието на голям брой рас-тежни фактори обуславя нейната ефектив-ност. Цел: Да се определни ефективност-та и безопасността от чиста ТромбоцитБогата Плазма (ТБП) при лечение заколянна остеоартроза (ОА), сравнена сдруги методи на терапия- хиалуроновакиселина (ХК) и кортикостероиди (КС).Mатериали и методи: Не-рандомизира-но, единично-заслепено проучване, коетовключва 96 пациента. Случайно разпред-лени в три групи, пациентите са получилитромбоцит богата плазма, хиалуроновакиселина или кортикостероидни аплика-ции в три поредни седмици. За оценка наефективността от терапията преди лече-нието, на 1-ви, 6-ти и 12-ти месец е изпол-зван Western Ontario and McMasterUniversities Osteoarthritis Index (WOMAC).Отбелязани са настъпилите нежеланиреакции. Резултати: Изходните характе-ристики на групите са съпоставими. На
ABSTRACT
Introduction: Treatment method for kneeosteoarthritis is applications of plateler richplasma. It consists of huge number of grow-ing factors, which determine its efficacy. Aim:To determine the safеty and efficacy of purePlatelet Rich Plasma (PRP) for kneeosteoarthritis (OA) treatment, compared withother treatment methods-hyaluronica acid(HA) and corticosteroids (CS). Material andMethods: A non- randomized, single-blindedcontrol study of 96 patients. The patientswere randomly selected in three groups andreceived either platelet rich plasma, hyaluron-ic acid, or corticosteroid for a series of 3 week-ly injections. Western Ontario and McMasterUniversities Osteoarthritis Index (WOMAC)was used for evaluation of the patients beforeinjections and at 1, 6 and 12 months after thefirst application. Adverse events were alsorecorded. Results: The baseline characteris-tics of the groups are similar. At first month alltreatment methods provide efficacy with nodifference between groups but statisticallysignificant difference compared with baseline.There is a clear difference in efficacy at month

Bulgarian medicine vol. 7 № 1/2017 37
INTRoDuCTIoN
Osteoarthritis is the fourth leading cause ofinvalidation worldwide, and WHO 2012 classi-fied it inside a group of 25 diseases leading tolife in disability. Osteoarthritis is common wor-ldwide with small geographic differences. Ofa great interest are knee and hip osteoarthritisbecause of the size and money needed to betreat. The age standardized prevalence ofradiographic knee OA in adults age ≥ 45 was19.2% among the participants in theFramingham Study and 27.8% in theJohnston County Osteoarthritis Project (10).In the third National Health and NutritionExamination Survey (NHANES III), approxi-mately 37% of participants age >60 years orolder had radiographic knee OA (10). Recentstudy using cadaver-derived skeletons amongindividuals describes osteoarthritis of theknee as a ‘mismatch disease’ and explainapproximate doubling of knee OA prevalencethat has occurred in the United States sincethe mid-20th century (17). The disease is nolonger attributed to aging and obesity. Allels ofthe genes, such as GDF 5, have been shown
to influence knee OA susceptibility. Also therole of environmental factors have been risen.
Gonarthrosis is a condition that affects thearticular cartilage, synovial membrane andsubchondral bone. All of these structures areresponsible for biochemicle and biomechanicalbalance of the joint (14). OA is a pathologyaccompanied by an increased presence ofinflammatory cytokines and proteolytic mole-cules in the tissue, which in turn lead to ext-racellular matrix degeneration and functionalimpairment. Chondrocytes and synovial cellschange their quiescent phenotype in responseto an abnormal microenvironment from trau-ma-induced inflammation (6) The main proin-flammatory cytokines involved in the pathop-hysiology of OA are interleukin (IL)-1b, tumornecrosis factor, and IL-6. These cytokines con-tribute to OA pathogenesis through severalmechanisms contributing to the phenotypeshift of chondrocytes, through which activatedcells increase the expression of catabolic andproinflammatory genes. In addition, thesecytokines intensify and maintain OA diseaseby inducing the production of other proinflam-
първи месец всички терапевтични групиосигуряват ефективност без разликапомежду им, но със статистически значимаразлика спрямо базовото ниво. Изразеноразличие в терапевтичната ефективностима на 6-ти месец, където ПРП и ХК показ-ват по –добри резултати спрямо кортикос-тероидите. Липсва разлика между ПРП иХК в този период. На 12 месец и дветегрупи все още показват сигнификантно по-добри резултати, сравнени с КС, но по-лоши спрямо тези отчетени на 6 месец.Наблюдаваните странични реакции саболка, подуване, контрактура.Заключение: ТБП осигурява добро пов-лияване на болката, намаляване на скова-ността и подобряване на функцията в еже-дневието. Представлява по-добър терапев-тичен избор при колянна остеоартрозаспрямо кортикостероиди като има съпоста-вим ефект с хиалуроновата киселина отче-тено на 6 и 12 месец от терапията.
Kлючови думи: тромбоцит богатаплазма (ТБП), колянна остеоартроза, интраартикуларно
6 where PRP and HA groups illustrate betterresults compared with CS. There is no differ-ence between PRP and HA at that point. Atmonth 12 both groups still show significantresults compared with CS, but worse thanmonth 6. Adverse events are swelling, pain,temporary loss of function. Conclusion: PRPprovide good relieve of pain, reduce stiffnessand alleviate function. It is a better therapeu-tic choice for knee osteoarthritis. Still betterone from intra-articular corticosteroids andprovide similar effect as hyaluronic acid bestseen at 6 and 12 month after treatment.
Key words: platelet rich plazma (PRP),knee osteoarthritis, intra-articular

38 Bulgarian medicine vol. 7 № 1/2017
matory cytokines, such as IL-8, IL-15, IL-17,IL-8, IL-21, and leukemia inhibitory factor(8,11).
The aim of treatment is reducing pain, stiff-ness and improve function (1). There are non-pharmacological, pharmacological and surgi-cal methods. Approved intra-articular treat-ment methods are Corticosteroids (12), hya-luronic acid (3). However, ACR 2012 do notstate HA’s benefit (7). On the other hand,Hondroitin sulphate and Glucosamine sulpha-te have shown controversial results in rando-mized control trails (16), so they are notrecommended by ACR. There are not knownany disease modifying drugs for treatment ofosteoarthritis.
The purpose of the study is to establish the
efficacy and safety of intra-articular applicati-ons of platelet rich plasma for knee OA, com-pared with other methods- intra-articular hya-luronic acid and corticosteoids.
MATERIAL AND METhoDS
This was designed as s prospective, single-center, non-randomized, single-blind, 3-armgroup study. The study had a permission fromthe Ethical Comission at Medical UniversityPlovdiv. Patient selection was based on strictinclusion/exclusion criteria (Table 1) All pati-ents had a screening visit (visit 1), three tre-atment visits (visit 2, 3, 4, recpectively) andfollow up visits at 1 month (visit 5), 6 month(visit 6) and end of study visit at 12 month
Table 1. Subject eligibility criteria

Bulgarian medicine vol. 7 № 1/2017 39
(visit 7). At visit 1, 5, 6 and 7 patients wereevaluated by Western Ontario and McMasterUniversities Osteoarthritis Index (WOMAC). Atall visits patient were asked and examined forany adverse events.
The study included a total of 96 patients.Baseline characteristics of the patients shownon Table 2.
The study group consists of 37 patients. Toprepare the PRP, at each visit 2, 3 and 4 res-pectively, 20 cc of peripheral blood was ext-racted from each patient by venepuncture intoextraction tube containing 3 ml Sodium Citratas anticoagulant. The extraction tube wasconnected to SW-PRP kit, SAEWON, Korea.The PRP kit was centrifuged at 3850 RPM for7 minutes at room temperature in SW-400machine, Korea. It was followed by secondcentrifugation but for 8 minutes. Once the kitwas centrifuged, we proceeded to physicallyseparate the plasma fractions and receiveapproximally 2-3 cc of poor leucocyte, pureplatelet rich plasma ready for aplication.
The first control group consists of 27 pati-ents. They receive 3 IA injections of Sodiumhyaluronate, 20 mg/2 ml. The second controlgroup consists of 32 patients. They receive 1IA injection of Diprophos 7 mg/1 ml. A visit 3,and 4 they receive IA injection of saline-place-bo.
All intra-articular injections were applied inlateral suprapatellar recessus followed by 15minutes rest.
outcome measuresThe primary efficacy outcome was the
change in pain, joint stiffness, and physicalfunction measured using WOMAC at baseline,1 month, 6 month and 12 month. TheWOMAC consist of 24 total items devidedamong 3 subscales: pain ( 0-20), stiffness ( 0-8) and fisical function (0-68). Higher scores
are representative of greater pain and stiffnesas well as worsened physical capability.Patients answer the questions before any pro-cedure and are not allowed to review the pre-vious answers. The second outcome is safetyof the treatment method.
Statistical analysis was performed by theuse of SPSS v17.0. Nonparametric tests of U-Mann– Whitney and Kruskal–Wallis (for conti-nuous variables) were used.
RESuLTS
1. EfficacyNo difference in baseline WOMAC parame-
tes existed between the three groups, p > .05(WOMAC pain, p = .532; WOMAC stiffness, p= .250; WOMAC function, p = .628; WOMACtotal, p = .626).
At month 1, there are no difference betwe-en the three treatment groups according topain, stiffness, function, and total score(WOMAC pain, p = .679; WOMAC stiffness, p= .523; WOMAC function, p = .261; WOMACtotal, p = .396). At the end of the first monththere is continuating similarity in results bet-
Table 2. Demographics and groups of treatment
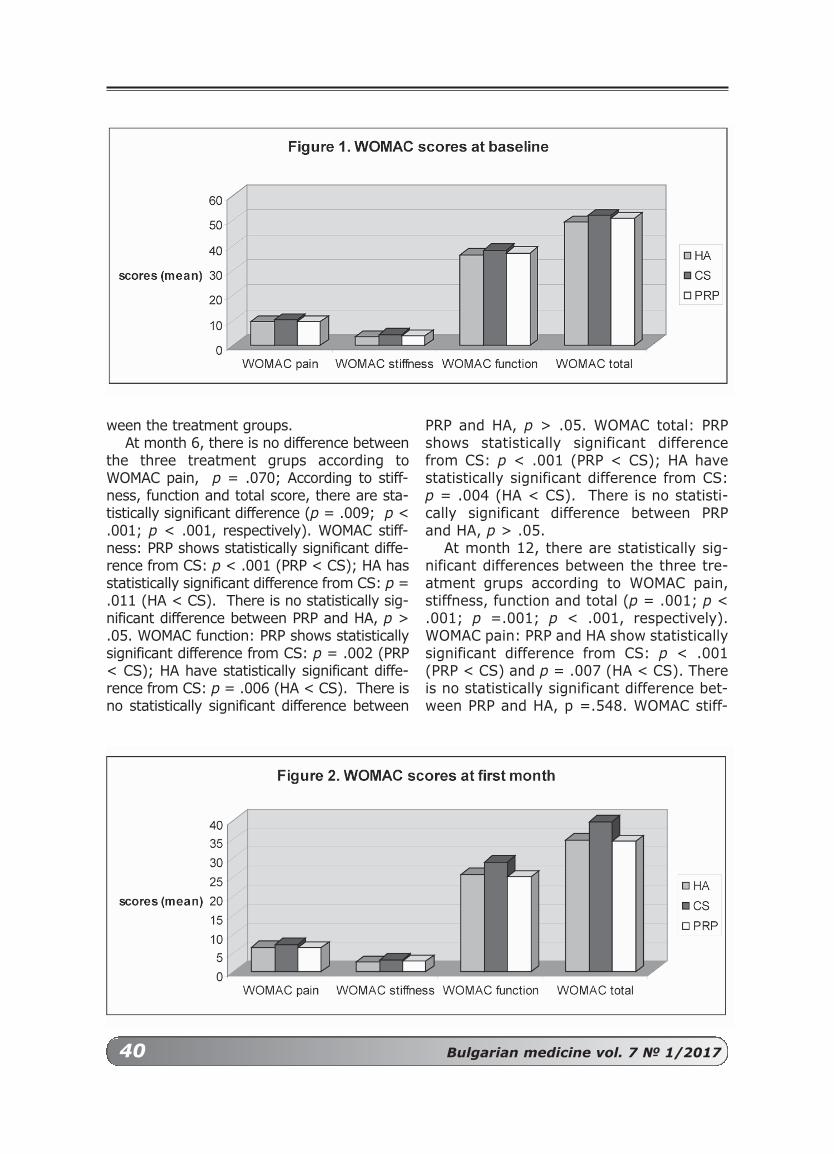
40 Bulgarian medicine vol. 7 № 1/2017
ween the treatment groups. At month 6, there is no difference between
the three treatment grups according toWOMAC pain, p = .070; According to stiff-ness, function and total score, there are sta-tistically significant difference (p = .009; p <.001; p < .001, respectively). WOMAC stiff-ness: PRP shows statistically significant diffe-rence from CS: p < .001 (PRP < CS); HA hasstatistically significant difference from CS: p =.011 (HA < CS). There is no statistically sig-nificant difference between PRP and HA, p >.05. WOMAC function: PRP shows statisticallysignificant difference from CS: p = .002 (PRP< CS); HA have statistically significant diffe-rence from CS: p = .006 (HA < CS). There isno statistically significant difference between
PRP and HA, p > .05. WOMAC total: PRPshows statistically significant differencefrom CS: p < .001 (PRP < CS); HA havestatistically significant difference from CS:p = .004 (HA < CS). There is no statisti-cally significant difference between PRPand HA, p > .05.
At month 12, there are statistically sig-nificant differences between the three tre-atment grups according to WOMAC pain,stiffness, function and total (p = .001; p <.001; p =.001; p < .001, respectively).WOMAC pain: PRP and HA show statisticallysignificant difference from CS: p < .001(PRP < CS) and p = .007 (HA < CS). Thereis no statistically significant difference bet-ween PRP and HA, p =.548. WOMAC stiff-
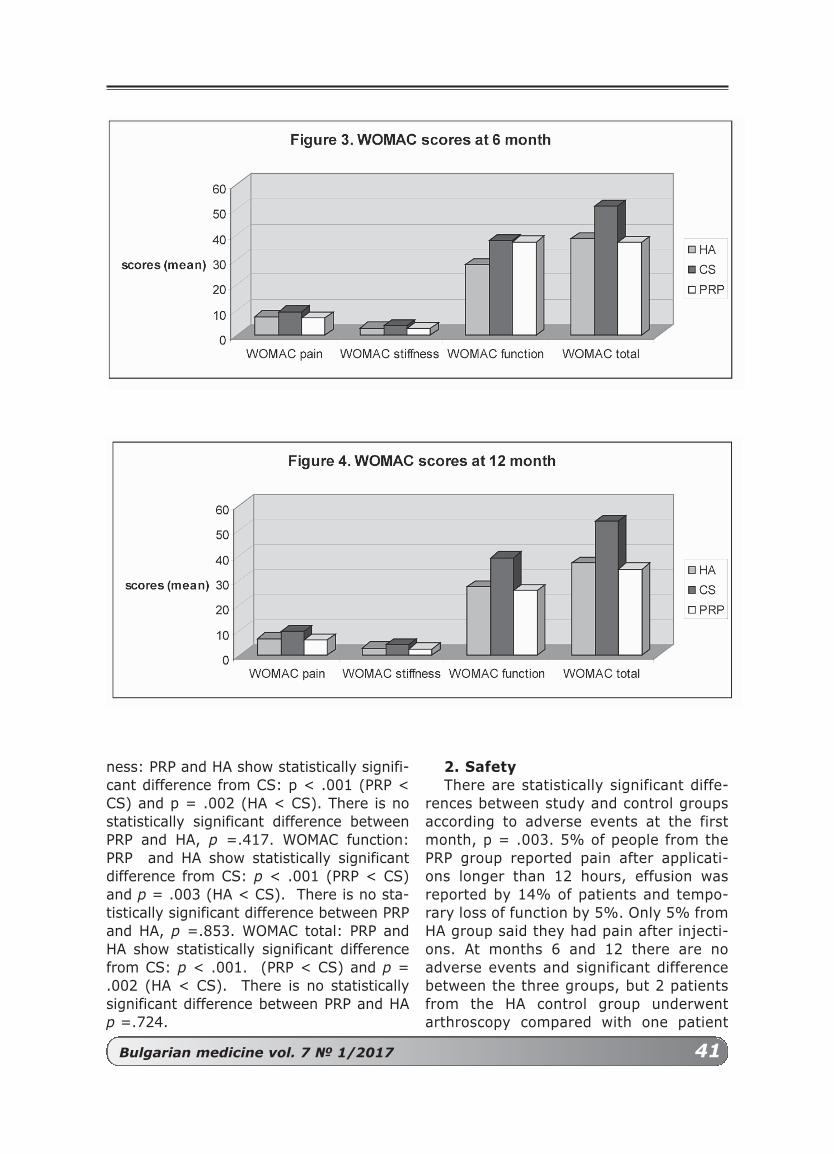
ness: PRP and HA show statistically signifi-cant difference from CS: p < .001 (PRP <CS) and p = .002 (HA < CS). There is nostatistically significant difference betweenPRP and HA, p =.417. WOMAC function:PRP and HA show statistically significantdifference from CS: p < .001 (PRP < CS)and p = .003 (HA < CS). There is no sta-tistically significant difference between PRPand HA, p =.853. WOMAC total: PRP andHA show statistically significant differencefrom CS: p < .001. (PRP < CS) and p =.002 (HA < CS). There is no statisticallysignificant difference between PRP and HAp =.724.
2. SafetyThere are statistically significant diffe-
rences between study and control groupsaccording to adverse events at the firstmonth, p = .003. 5% of people from thePRP group reported pain after applicati-ons longer than 12 hours, effusion wasreported by 14% of patients and tempo-rary loss of function by 5%. Only 5% fromHA group said they had pain after injecti-ons. At months 6 and 12 there are noadverse events and significant differencebetween the three groups, but 2 patientsfrom the HA control group underwentarthroscopy compared with one patient
Bulgarian medicine vol. 7 № 1/2017 41

42 Bulgarian medicine vol. 7 № 1/2017
from PRP group. One patient had totalknee replacement surgery from HA con-trol group. All these people were excludedfrom the statistical analysis.
DISCuSSIoN
The primary porpous of the study is toevaluate the efficacy of treatment withPRP compared to other treathment met-hods, and the second aim was evaluatingthe safty. The study confirmed the hypot-hesis that PRP is better treatment thanCS and have similar results compared toHA. This effect is seen at month 6 especi-ally for stiffness and function, but at 12month of the follow-up there are statisti-cally significant differences at all parts ofWOMAC (pain, stiffess and function).
The study shows similar results withprior studies comparing PRP with HA orPRP with CS.
Data from Duymus et al 2017 (5)shows similarities with our study. Theyperform randomized control trial with atotal of 102 patients, which were treatedwith either PRP 2 intra-articular injecti-ons, HA single-dose of intra-articualrinjection, or ozone x four times. At theend of the first month after injections,significant improvements were seen in allgroups. The result was similar with ouroutcome.
At 6 month, while the clinical efficaciesof PRP and HA were similar and continu-ed, the clinical effect of ozone had disap-peared (p < 0.001). Our results showedsimilar changes according to WOMACcompartments in PRP and HA group.
At the end of 12 month, PRP was deter-mined to be both statistically and clinical-ly superior to HA (p < 0.001) suggestedthe study team. Our study shows no sig-nificant differences between PRP an HA atmonth 12 of the follow-up period, butbetter significant results compared tobaseline. Similar results illustrated Lanaet al 2016 (9). They evaluated PRP treat-ment compared to HA or a combination ofPRP and HA. They performed a randomi-zed control trial with 105 patient, 36 trea-ted with PRP three intra-articular injecti-
ons, 36 with HA also three intra-articularinjections. The rest of the patients weretreated with a combination. The resultsshowed greater improvement in WOMACfunction at 12 month (p=0.008) whencompared to HA group. Data fromBottegoni et al 2016 (2), observed 60patents treated with PRP three intra-arti-cular injections or CS single applicationshowed worsening of the results at 6month.
Similar results at 6 month are seen indoble randomized clinical trial ofMontañez-Heredia et al 2016 (13) compa-ring 27 patients treated with PRP and 26treated with sodium hyaluronate.
Cole et al 2015 (4) performed double-blinde, randomise clinical trail with a totalot 99 patients treated with PRP or HAthree times during weekle interval. Theydiscovered no statistically significant dif-ference between the two groups at month12 according to WOMAC score.
A meta- analysis was performed byRiboh et al 2016 (15) including 6 rando-mised controlled trials (evidence level 1)and 3 prospective comparative studies(evidence level 2) with a total of 1055patients. Injection of leucocyte pour PRP(LP-PRP) resulted in significantly betterWOMAC score than hyaluronic acid (meandifference, -21.14;95% Cl, -39.63 to -2.65) or placebo (mean difference, -17.84; 95% Cl, -34.95 to -0.73) No suchdifference was observed with leucocyterich PRP (mean difference, -14.28; 95%Cl, -44.80 ti -16.25). The SUCRA analysisshowed that LP-PRP was the highest ran-ked treatment for measure of clinical effi-cacy (WOMAC)
PRP injections resulted in a higher inci-dence of adverse reactionsnthan hyaluro-nic acid (odds ratio, 5.63; 95% CI, 1.38-22.90), but there was no difference bet-ween LR-PRP and LP-PRP (odds ratio,0.78; 95% CI, 0.05-11.93). These reacti-ons were nearly always local swelling andpain, with a single study reporting medi-cal side effects including syncope, dizzi-ness, headache, gastritis, and tachycardia(17/1055 total patients). The final analy-

Bulgarian medicine vol. 7 № 1/2017 43
REFERENCES:
1. Bert JM, Bert TM. Nonoperative treatment ofunicompartmental arthritis. From
bracing to injection. Clin Sports Med. 2014;33(1):1–10.
2. Bottegoni C, Dei Giudici L, Salvemini S et al.Homologous platelet-rich plasma for
the treatment of knee osteoarthritis in selectedelderly patients: an open-label, uncontrolled,pilot study Ther Adv Musculoskel Dis 2016, Vol.8(2) 35–41
3. Bruyère O, Cooper C, Pelletier JP et al. A con-sensus statementon the European
Society for Clinicaland Economic Aspects ofOsteoporosis and Osteoarthritis (ESCEO) algo-rithm for the management of knee osteoarthri-tis—From evidence-based medicine to the real-life setting SeminarsinArthritisandRheumatism45(2016)S3–S11
4. Cole BJ et al. Hyaluronic Acid Versus Platelet-Rich Plasma: A Prospective, Double-
Blind Randomized Controlled Trial ComparingClinical Outcomes and Effects on Intra-ArticularBiology for the Treatment of KneeOsteoarthritis. Am J Sports Med 2016, 45 (2),339-346.
5. Duymus TM, Mutlu S, Dernek B, et al. Choice ofintra-articular injection in treatment
of knee osteoarthritis: platelet-rich plasma,hyaluronic acid or ozone options. Knee SurgSports Traumatol Arthrosc. 2017Feb;25(2):485-492
6. Goldring MB, Otero M. Inflammation inosteoarthritis. Curr Opin Rheumatol.2011;23:471–8. doi:10.1097/BOR.0b013e328349c2b1
7. Hochberg M, Altman R, April K, Benkhalti M etal. Recommendations for the Use of
Nonpharmacologic and Pharmacologic Therapiesin Osteoarthritis of the Hand, Hip, and Knee.Arthritis Care & Research Vol. 64, No. 4, April2012, pp 465– 474 DOI 10.1002/acr.21596 ©2012, American College of Rheumatology
8. Kapoor M, Martel-Pelletier J, Lajeunesse D,Pelletier JP, Fahmi H. Role of
proinflammatory cytokines in the pathophysiologyof osteoarthritis. Nat Rev Rheumatol.2011;7:33–42. doi:10.1038/nrrheum.2010.196
9. Lana JF, Weglein A, Sampson SE et al.Randomized controlled trial comparinghyaluronic acid, plateletrich plasma and thecombination of both in the treatment of mildand moderate osteoarthritis of the knee. J StemCells Regen Med 2016;12:69-78.
10. Lawrence RC, Felson DT, Helmick CG, et al.Estimates of the prevalence of arthritis andother rheumatic conditions in the United States.Part II. Arthritis Rheum 2008;58(1):26–35.
11. Maldonado M, Nam J. The role of changes inextracellular matrix of cartilage in the presenceof inflammation on the pathology ofosteoarthritis. Biomed Res Int.2013;2013:284873. doi:10.1155/2013/284873
12. McAlindon T, Bannuru R, Sullivan M , Arden Net al. OARSI guidelines for the non-surgicalmanagement of knee osteoarthritisOsteoarthritis and Cartilage 22 (2014) 363-388
13. Montañez-Heredia E , Irízar S , Huertas P etal. Intra-Articular Injections of Platelet-RichPlasma versus Hyaluronic Acid in the Treatmentof Osteoarthritic Knee Pain: A RandomizedClinical Trial in the Context of the SpanishNational Health Care System Int. J. Mol. Sci.2016, 17, 1064
14. Punzi L, Oliviero F, Plebani M. New biochemicalinsight into the pathogenesis of osteoarthritisand the role of laboratory investigation assess-ment. Crit Rev Clin Lab Sci. 2005;42(4):279-309
15. Riboh J, Bryan M. Saltzman, Adam B. Yanke,Lisa Fortier and Brian J. Cole Effect of LeukocyteConcentration on the Efficacy of Platelet-RichPlasma in the Treatment of Knee OsteoarthritisAm J Sports Med 2016 44: 792
16. Towheed TE, Maxwell L, Anastassiades TP,
sis said that PRP results in improved fun-ctional outcome scores compared withhyaluronic acid and placebo when usedfor treatment of knee osteoarthritis.
CoNCLuSIoN
Treatment woth PRP showed a signifi-cantly better results compared to corti-costeroids and versy similar results com-pared to hyaluronic acid. In addition, thedata illustrate significant better resultsfor PRP till 12 month of treatment withgood safety profile.

44 Bulgarian medicine vol. 7 № 1/2017
Адрес за кореспонденция:
МАРИАНА ЖЕЛЯЗКОВА
Meдицински Университет - Пловдив,Медицински Факултет,
Катедра „Пропедевтика наВътрешните болести”,
Клиника по РевматологияE-mail:
Corresponding author:
MARIANA ZhELyAZKoVA
Medical University, Plovdiv,Faculty of Medicine, Propedevtics
of Internal Diseases, Dept. of Rheumatology
E-mail: mariana_zhelyazkova
@yahoo.com
Shea B, Houpt J, Robinson V, et al. Glucosaminetherapy for treating osteoarthritis. CochraneDatabase Syst Rev 2009;2:CD002946.
17. Wallace IJ, Worthington S, Felson DT, et al.
Knee osteoarthritis has doubled in prevalencesince the mid-20th century. Proc Natl Acad SciU S A. Published online before print on August14, 2017. doi: 10.1073/pnas.1703856114

Bulgarian medicine vol. 7 № 1/2017 45
Изисквания към авторите
Списание Българска медицина е изданиена Българската академия на науките иизкуствата (БАНИ), Отделение наука,Научен център по медицина и здравеопаз-ване. Излиза 4 книжки годишно.Списанието е достъпно електронно насайта на БАНИ, раздел издания.
В списание „Българска медицина” сеотпечатват оригинални статии, казуистичнисъобщения, обзори рецензии и съобще-ния за проведени или предстоящи научнифоруми – симпозиуми, конгреси, или другив областта на клиничната и фундаменталнамедицина. Списанието излиза на английскиезик с подробни резюмета на английски ибългарски език. Изключения се правят заобзорни статии по особено значими теми.Заглавието, авторските колективи и надпи-сите и означенията на илюстрациите сеотпечатват и на двата езика.
Материалите трябва да се представят вдва еднакви екземпляра, на шрифт TimesNew Roman, размер 12, разстояние междуредовете 1.5 линии. Обемът на всяка статияе до 10 страници, 12 страници за обзорнитестатии и 3-4 страници за казуистичнитесъобщения. Библиографията и илюстра-циите са включени в този обем. За инфор-мация за научни прояви обемът е до 4 стра-ници, за рецензии на книги – до 2 страни-ци. В този обем не се включват резюметатана английски и български език, чийто обемтрябва да бъде до 200 думи с 3-5 ключовидуми. Резюметата трябва да отразяват кон-кретната работна хипотеза, използванитеметоди, получените резултати и заключе-ние.
Структурата на статиите трябва даотговаря на следните изисквания: загла-вие, имената на авторите (собствено име ифамилия), название на научната организа-ция или лечебното заведение, в коетоработят Оригиналните статии трябва даимат следната структура: въведение, мето-ди, резултати, обсъждане и заключениеили изводи. Методиките трябва да бъдатподробно описани, както и статистическиметоди, използвани в изследването. В теста
се приемат само официално приетите сък-ращения, останалите трябва да бъдат обяс-нени.За мерните единици се използва сис-темата SI. Илюстрациите се представяткато отделни файлове и се посочва мястотоим текста за улеснение при предпечатнатаподготовка.
Тези изисквания не важат за другитенаучни публикации (обзори, казуистикаили съобщения и рецензии).
Книгописът се представя на отделнастраница подреден по азбучен ред първона английски език, после източниците набългарски език. Броят на цитиранитеизточници не трябва да надвишава 20 заоригиналните статии, до 40 за обзорнитестатии и до 10 ца казуистичните случаи.Подреждането на библиографията става последния начин:
За списание: автори, заглавие на статия-та, списание, година, том, страници от..до.
За книга: автори, заглавие на главата, В:заглавие на книгата, в скоби редактори,издателство, година, страници от…до.
Адрес за кореспонденция се дава вкрая на всяка статия и съдържа данните накореспондиращия автор, включителноадреса на електронната му поща. Всичкиръкописи се изпращат с придружителнописмо подписано от авторите, в което сеотбелязва, че тя не е била предлагана надруго списание и не е отпечатвана у насили в чужбина. Ръкописите не се връщат.
Процедура по рецензиране: С огледспазване на международните стандарти,редакционната колегия е приела процеду-ра по „двойно сляпо“ рецензиране от неза-висими референти. На авторите се предос-тавя възможността да предложат на внима-нието на редакционния екип три имена наспециалисти в тяхната област като потен-циални рецензенти.
ПУБЛИКАЦИОННА ЕТИКА:
Задължения на редактора: редакто-рът носи отговорност за вземане на реше-нието коя от изпратените статии да бъдепубликувана. Редакторът се съобразява със

46 Bulgarian medicine vol. 7 № 1/2017
законовите ограничения, свързани с въз-държане от дискредитиране, нарушаванена авторски права или плагиатство.Редакторът оценява интелектуалната стой-ност на един труд без оглед на възраст,пол, расова принадлежност, сексуална ори-ентация, религиозни убеждения и др.форми на дискриминация. Редакторът неразкрива информация то отношение наръкописа на други лица освен рецензенти-те, авторите за кореспонденция, издателя идругите членове на редакционната коле-гия.
Задължения на авторите: Авторитеследва да предложат оригинални произве-дения, в които не са използвани трудове иизрази на други автори, без да бъдат цити-рани. По принцип авторите не следва дапубликуват многократно материал, койтоповтаря по същество дадено изследване вдруги списания или първични публикации.Не се приема представянето на един и същръкопис в повече от едно списание едно-временно. Трудовете и приносът на другиавтори, относими към предмета на ръкопи-са, трябва да бъдат отразени под форматана цитирания. Всички лица, които са далисвоя принос за концепцията, литературнияанализ, дизайна, изпълнението или интер-претацията на данните, следва да бъдатпосочени като съавтори. Авторът за корес-понденция носи отговорност за това всичкисъавтори да бъдат запознати и да са израз-или своето одобрение за съдържанието напредлагания за публикуване материал.
Задължения на рецензентите:Рецензентите подпомагат редактора привземане на решение, като те могат да под-помогнат автора за повишаване качествотона статията. Всички ръкописи, получени зарецензиране следва да се считат за повери-телен материал и тяхното съдържание неследва да се разкрива пред никого, освен сразрешението на редактора. Рецензентитеследва да се придържат към обективнитестандарти за оценка. Лични нападки срещу
авторите са неприемливи. Критичнитезабележки следва да бъдат подкрепени саргументи.
Конфликт на интереси:Непубликувани материали не могат дабъдат използвани в собствени изследванияна редактора без изричното писмено съгла-сие на авторите. Авторите следва да обяватвсички финансови или други съществениконфликти на интереси, които могат даокажат влияние върху интерпретацията натехните резултати. Всички източници нафинансиране на проведените проучванияследва да бъдат обявени.
Етически съображения по отношениена самите изследвания: всички трудове,които отразяват клинични проучванияследва да имат подписано информираносъгласие от пациентите и получено разре-шение за изследването от съответнатаЕтична комисия в съответствие сДекларацията от Хелзинския комитет.Експерименталните проучвания следва даимат също разрешение от съответнатаЕтична комисия и от Българската Агенцияпо безопасност на храните и лекарствата.
След положителна рецензия и одобре-ние на редколегията, авторите на статиятадължат заплащане в размер 10 лв на стра-ница на статията си, с оглед покриване наразноските по английската езикова редак-ция на текста и коректури.
Всички материали за списанието се изпращат на посочения адрес
на редакцията:Проф. д-р Дроздстой Стоянов, дм
(главен редактор):[email protected]
Проф. д-р Дамянка Гетова, дмн (изпълнителен редактор):
[email protected] Д-р Иван Киндеков, дм
(научен секретар):[email protected]

Bulgarian medicine vol. 7 № 1/2017 47
The Bulgarian Medicine journal is the offici-al edition of the Bulgarian Academy of Scienceand Arts (BASA), Science division, ResearchCenter for medicine and health care. It is pub-lished in 4 issues per year.
Bulgarian medicine is available online onthe website of the BASA, publication section.
Bulgarian Medicine journal accepts for pub-lication reviews, original research articles andcase reports (short communications), opinionon new medical books, letters to the editorand announcements for scientific events (con-gresses, symposia, workshops, etc.) in allfields of fundamental and clinical medicine.
The journal is published in English withabstracts in English and in Bulgarian. Theabstracts, its titles, the names of the authorsand their institutions should be respectively inEnglish and in Bulgarian.
The manuscript should be submitted in twoprinted copies, on standard A4 sheets, usefont Times New Roman, size 12, line spacing1.5 lines. The size of each paper should notexceed 10 pages for ariginal articles, 12 pagesfor reviews and 3-4 pages for case reports, upto 4 pages on scientific events or chronicles.The references and illustrations are included.
The abstracts are not included in the sizeof the paper. They should be submitted onseparate page with 3 to 5 key words. Theyshould reflect the most essential topics of thearticle, including objective, method, resultsand conclusion. The abstract should not exce-ed 200 words.
The basic structure of the manuscriptshould meet the following requirements:
Title page: The title of the article, forena-me, middle initials and family name of eachauthor, institutional affiliation (department,faculty and university), address and e-mail ofthe corresponding author.
Text of the article: The original researcharticle should have the following structure:Introduction (states the aim and summarizethe rational for study); Material and Methods:subjects, methods, procedures, statistics;Results: the obtained results from the studywith illustrations – tables, figures, pictures,
etc.; Discussion: should be linked with the aimof the study and appropriate conclusion.These requirements are not valid for the othertype of manuscripts. Only officially recognizedabbreviations should be used, all others sho-uld be explained in the text. Units should beused according to the International System ofUnits (S.I. units). Numbers to bibliographicalreferences should ne used according to theirenumeration in the reference list.
Illustrations: The figures, diagrams,schemes or tables should be submitted in aseparate file with consecutive numbers, title ofthe article and the name of the first author.The explanatory text accompanying the figu-res should be presented along with the res-pective number of the figure in the main textbody with the space left for insersion of thefigure.
References: The references should bepresented on a separate page at the end ofthe manuscript. It is recommended that thenumber of references should not exceed 20titles of the original articles, 40 for reviews(70% should from the last 5 years. The refe-rences should be listed in alphabetical order,English first, followed by Bulgarian ones. Thenumber of reference should be followed by thefamily name of the first author and thenhis/hers initials, name of the second author,etc. The full name of the cited article should bewritten, followed by the name of the journal,year, volume and pages. Chapter of the booksshould be cited in the same way, the authors,the full name of the chapter first, followed by“In:”, full name of the book, Editors, publis-hers, town, year, first and final page of thechapter.
ExAMPLES:
Reference to a journal article:McLachan S, MF Prunel, B. Rappoport. Cell
mediated humoral immunity. J. Clin.Endorcinol, Metab., 2011, 78(4): 1071-82.
References to a book chapter: Delange F, Endematic Cretenism. In: The
thyroid (Eds. L. Braveman and R. Utiger).Lippincot Co, Philadelhia, 2001, 942-955.
Author’s guidelines

48 Bulgarian medicine vol. 7 № 1/2017
Manuscript submission: The original andone copy of the complete manuscript are sub-mitted together with a cover letter grantingthe consent of all authors for the publication ofthe article as well as a statement that it hasnot been published previously elsewhere andsigned by the first author. The procedure sho-uld be complemented via electronic submissi-on. Manuscript accepted for publication willnot be returned to the authors.
Peer-review process: following the inter-national standards in the field, the Editorialboard has adopted double-blind peer-reviewpolicy assigned to independent referees. Theauthors are encouraged to submit the namesof three potential; referees for editorial consi-deration.
PuBLICATIoN EThICS:
Editor’s obligations: the editor is respon-sible for deciding which of articles submittedto the journal should be published. The editormay be guided by the policies of the journal’seditorial board and constrained by such legalrequirements as shall then be in force regar-ding libel, copyright infringement and plagia-rism. The editor may confer with other editorsor reviewers in making this decision. An editorat any time evaluate manuscript for their con-tent without regards of race, gender, sexualorientation, religious belief, ethic origin, citi-zenship, or political philosophy of the authors.The editor and any editorial staff must notdisclose any information about submittedmanuscript to anyone other than the corres-ponding author, reviewers, potential revie-wers, other editorial advisers and the publis-her, as appropriate.
Author’s obligations: the authors shouldensure that they have written entirely originalworks, and if the authors have used the workor words of others than this has been appro-priately cited or quoted. An author should notin general publish manuscript describingessentially the same research in more thanone journal or primary publication. Submittingthe same manuscript to more than one jour-nal concurrently constitutes unethical publis-hing behavior and is unacceptable. Properacknowledgement of the work of others mustalways be given. Authors should cite publica-tions that have been influential in determining
the nature of reported work. Authorship sho-uld be limited to those who made a significantcontribution to the conception, design, execu-tion, or interpretation of the reported study.All those who have made significant contribu-tions should be listed as co-authors. Wherethey are others who have participated in cer-tain substantive aspects of the research pro-jects, they should be acknowledged or listedas contributors.
Obligations of the reviewers: Peer revi-ew assists the editor in making editorial deci-sion and through the editorial communicationswith the author may also assist the author inimproving the paper. Any manuscript receivedfor review must be treated as confidentialdocuments. They must not be shown to ordiscussed with others except as authorized bythe editor. Reviews should ne conductedobjectively. Personal criticism of the author isunappropriate. Referees should express theirviews clearly with supporting arguments.
Disclosure and conflict of interest:Unpublished material disclosed in a submittedmanuscript must not be used in an editor’sown research without express written consentof the author. All authors should disclose intheir manuscript any financial or other subs-tantive conflict of interest mat might be con-strued to influence the results or interpretati-on of their manuscript. All sources of financialsupport for the project should be disclosed.
Ethical regulations: reports on humansubjects should have written consent signedby the patients and approved by National orRegional Ethic Committee. For studies on ani-mals the necessary permission by NationalAgency for food and drug administration orRegional Committee should be cited.
Processing charges: Following acceptan-ce for publication the authors are charged 5euroes per page for language editing and cor-rections.
Addresses for sending of manuscriptsand other editorial correspodance:
Prof. Drozdstoy Stoyanov: [email protected]
Prof. Damianka Getova-Spassova: [email protected]
Dr Ivan Kindekov: [email protected]

![[Type text] · медицинска психология, Медицински университет „Проф. д-р Параскев Стоянов“, Варна Резюме:](https://img.dokumen.tips/doc/110x75/5e60f8fc7c5b8d74eb18acbc/type-text-oe-f.jpg)



























