Embed Size (px)
Citation preview

Building Relationships with Campus Partners: A Necessity to Providing Culturally Competent
Services
Mona Ghosheh, PhD

Objective and Outline• Discuss reasons for underutilization of traditional services
by students of color.
• Describe concept of organizational cultural competence and its significance to outreach for racial and ethnic minorities.
• Identify indicators of OCC in counseling center setting.
• Utilize methods to increasing the visibility of counseling
center OCC by developing relationships campus partners.
Problem: Underutilization • A general problem across the US
– Especially for racial and ethnic minorities
• Concerning because:– minority groups tend to experience similar community rates of
mental disorders – Utilize services at lower rates– And receive poorer quality of care
• Results in higher proportion of unmet mental health needs in minority communities
U.S. Department of Health and Human Services, 2001

Racial & Ethnic Minorities
• Race– the category to which others assign individuals on the basis of
physical characteristics and the generalizations and stereotypes made as a result (APA, 2003)
• Ethnicity– Shared practices, customs, and heritages of particular groups
(Phinney, 1996)
• + Minority – Individuals or groups other than those of the dominant
European or Caucasian-American cultural group
Racial and Ethnic Minority• Experience of minority groups (Vacc, DeVaney, & Brendal,
2003):– Experience a pattern of disadvantage or inequality – Share a sense of self-consciousness or physiological awareness
that is associated with their group membership and its status– Experience the identification with and internalization of
stereotypes
• Further differentiation (USDHHS, 2001):– Underrepresentation and underutilization experienced by these
populations across a variety of sectors such as education and employment
– Disproportion exists despite increasing population sizes

Problem: Underutilization
University campuses are not exempt from this disparity

Possible Reasons
• Help-seeking attitudes and behaviors
• Cultural mistrust– “mental health services as a microcosm of the larger White
society” (Whaley, 2001)
• Stigma – Confounded for minority groups: “double stigma” (Gray, 2005)
• Worldview– Collectivistic worldview = help seeking within family & cultural
group – Definition of problem= external vs. internal

Reason: Incongruence
• Traditional Psychotherapy – Individualism, autonomy, and individual
responsibility vs. collectivism, group harmony, and societal responsibility (Sue & Sue, 1999)
– Treatments originally developed for European Americans (Hall, 2001; Vera & Speight, 2007)
• Accessibility – “the probability of use, given the need of services”
(USDHHS, 2001)

The Disparity
Increasing enrollment rates of minority students + Underutilization + lower accessibility = culturally relevant
treatments

Recommendation: Outreach• Proactive, Preventative, and Strength/empowerment based
– Reduces stigma (directly/indirectly)
• Consistent with collectivistic worldview– Outreach tends to be group-oriented – Accessible: occurring in the context of students’ communities – Allows for the social experience necessary for this developmental age
• Reduces cultural mistrust– Outreach providers become weaved into the fabric of acceptable sources of
help– Consistent with the educational context of the university
• Flexible formats – Allow for modification based on groups’ needs & norms

Unanswered Questions
• Are UCCs providing outreach services specific to racial and ethnic minorities? If so…– How much outreach? – What types of outreach? – What specific groups are being served?
• If not, could there be factors influencing whether a UCC provides outreach services specific to the these populations?
History of UCCs and Outreach• 1940s-50s: beginning of UCCs• 1960s-70s: beginning of outreach
– Increase of student population– Greater emphasis on prevention– Transition from individual/vocational to a overall group/overall well-being
focus
• 1980s: greater enrollment of diverse students– Increased variety of presenting concerns– Budget cuts– Restricted resources– Increased use of outreach
• Today: – Great majority of UCCs are providing outreach– 92% of 302 schools surveyed provide outreach (Gallagher, 2009)

Possible Factors• Staff size
– Larger size = more outreach • (Whitely et al., 1987)• Professional staff, pre-professionals, and support staff
• Accreditation– Accreditation = more outreach
• (Whitely et al., 1987) • IACS, APA, other accreditation
• Institution size– # of enrolled students
• Student diversity

Other Factors?• The factors identified influence the availability of
outreach in general
• What about specific to racial and ethnic minorities? – Outreach services for racial and ethnic minorities classify as
“culturally adapted mental health interventions” (Griner & Smith, 2006)
– This means that they would require some cultural competency: knowledge, awareness, and skills of cultural factors (Sue, et. al., 1992).
BUT cultural competency of individual clinicians is limited

Cultural Competency

Organizational Cultural Competency
• “the capacity of an organization to support culturally appropriate responsive care” (Geron, 2002)
• Cross et al.’s (1989) model of mental health organizational cultural competency – “a set of congruent attitudes, practices, policies,
and structures that come together in a system or agency, or among professionals that enable effective interactions in cross-cultural situations”


OCC Development
• Occurring across attitudes, policies, and practices • Occurring across the practitioner, agency, and
system level (Sue, 2001).



How Do You Measure OCC?
• Greiger’s (1996) Student Affairs Multicultural Organizational Development Checklist
• Reynolds and Pope’s (2003) Template for a Multicultural Counseling Center

OCC Markers– Mission Statement
• Explicitly use the term “diversity” and/or mulitculturalism• States that these concepts are significant to all UCC funtions• How often incorporated in publications/flyers/advertisements, etc
– Staff diversity • Percentage
– Hiring and retention practices • How often? • How often are bi-mulit-lingual staff recruited?• Retention of racial and ethnic minority staff (3yrs)
– Diversity committee • Frequency of meetings?• Client population in committee?
– Translation• How often?
– Physical environment • How often?
– Cultural competency training • How often? • For whom?
Research Questions• Are UCCs providing outreach services specific to racial and ethnic
minorities? If so…– How much outreach? – What types of outreach? – What specific groups are being served?
• Is there a relationship between the availability of outreach services to racial and ethnic minorities and institutional factors?
• How about a relationship to OCC?
• If a relationship exists between OCC and outreach, does it more significantly explain the variance in outreach to minorities as compared to institutional factors?

Participants • University Counseling Centers (151/641)-26.8%
response rate– Completed by center directors– Location
• 41 different states
– Institution type• 55% private, 45 % public
– Institution size• 187-52,000; mean 10,000 (SD-11,000)
– Student diversity • Ranged from 2% to 100%
– Staff size:• Total: 1 to 73• Senior staff professionals: 1 to 39• Pre-professionals: 1 to 50• Support staff: 1 to 8
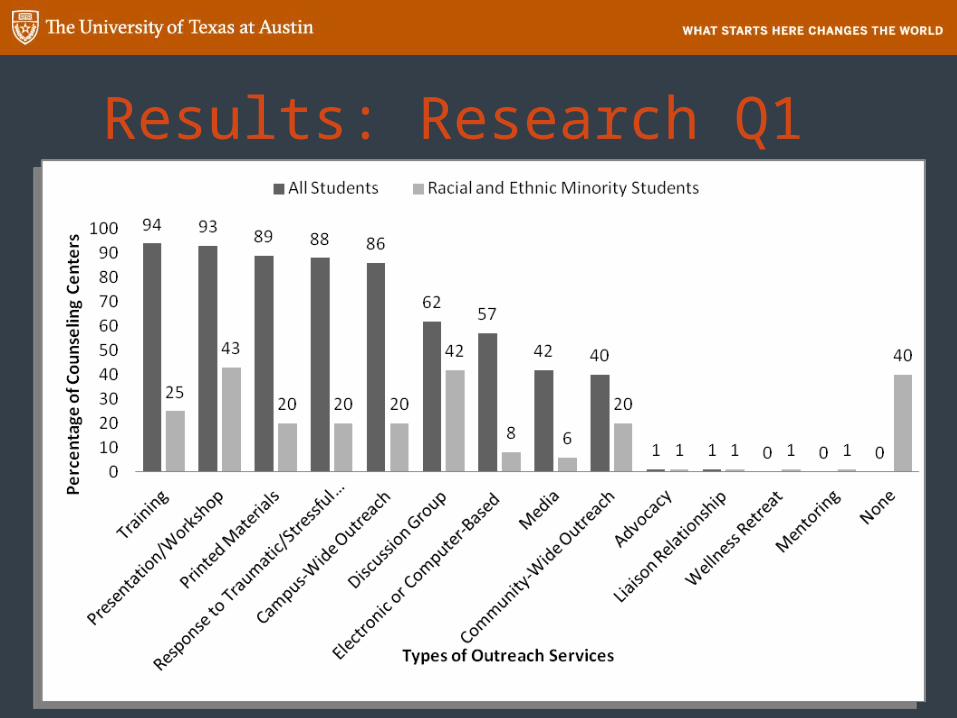
Results: Research Q1

Results: Research Q2

Results: Research Q3

Results: Research Q4 • As expected: the group of institutional variables resulted in a
significant, strong, and positive, predictive relationship of outreach availability
• (R=.651, p<.001)
• Significant Predictors:– Staff size t(141) = 2.85, p < .01 – APA and IACS accreditation t(141) = 2.15, p < .05– Other accreditation t(141) = 2.06, p < .05– Student diversity t(141) = 3.33, p < .01
• Insignificant Predictors:– Institution type– Institution size

Results: Research Q4 • OCC explained additional 6.3% of variability in the
availability of outreach services for racial and ethnic minorities (R=.697, p<.001)
• Significant Predictors:– Staff size t(141) = 2.85, p < .01 – APA and IACS accreditation t(141) = 2.15, p < .05– Other accreditation t(141) = 2.06, p < .05– Student diversity t(141) = 3.33, p < .01– CCCC measure t(141) = 4.15, p < .001

What Does this Mean?• Consistent with OCC theory and this study provides initial
support for the relationship between services to minorities and the OCC of a mental health agency.
• Institutional factors helped explain importance of :– resources – supply & demand– professional standards
• BUT an additional component is vital when servicing racial and ethnic minorities:
The multicultural competence of the organization

Implications • UCCCs not providing outreach to racial and ethnic minorities (40%).
– Self-assessment tools to improve OCC of counseling center
– The study and CCCC instrument may provide support for markers and their expression on an OCC continuum
• Diversity mission statement• Diverse staff • Hiring and retention practices• Diversity committee• Translation • Physical environment• Cultural competency training
– OCC is developmental process; so having a high availability of outreach does not eliminate the need for continuous improvement of OCC
– Approaching limited resources from the angle of OCC might help substantiate argument for need of resources

Anecdotal Experiences, Discussion, and Questions
• What about relationships with campus partners (overall community)?– How effective is OCC if the campus is not aware of or
perceiving of the UCC as a competent entity?
• How do we communicate, develop, and demonstrate cultural competency on our campuses and with campus partners? – Maybe partners need to be involved in developing services for
racial and ethnic minority students? – Maybe UCCs need to be more vocal and involved in diversity
affairs on campus? • Take a clear stance on SJ issues


• Cross, T. L., Bazron, B. J., Dennis, K. W., & Isaacs, M. R. (1989). Towards a culturally competent system of care: Volume 1. Monograph produced by the CASSP Technical Assistance Centre, Georgetown University Child Development Centre
• Gallagher, R. P. (2009). National survey of counseling center directors 2009. Washington, D.C. International Association of Counseling Services. Available at http://www.iacsinc.org/
• Gary, F. A. (2005). Stigma: Barrier to mental health care among ethnic minorities. Issues in Mental Health Nursing, 26, 979-999. • Geron, S. M. (2002). Cultural competency: How is it measured? Does it make a difference? Generations, 26, 39-45. • Griner, D., & Smith, T. B. (2006). Culturally adapted mental health intervention: A metaanalytic review. Psychotherapy: Theory, Research,
Practice, Training, 43, 531- 548. • Hall, G. C. N. (2001). Psychotherapy research with ethnic minorities: Empirical, ethical, and conceptual issues. Journal of Consulting and
Clinical Psychology, 69, 502- 510. • Hernandez, M., & Nesman, T. (2006). Conceptual model for accessibility of mental health services to culturally/linguistically diverse
populations. Presented during the grantee communities workshop entitled Operationalizing cultural competence for implementation in systems of care at the 19th Annual Research Conference: A System of Care for Children’s Mental Health: Expanding the Research Base, Tampa, Florida.
• Reynolds, A. L., & Pope, R. L. (2003). Multicultural competence in counseling centers. In D. B. Pope-Davis, R. L Toporek, & W. M. Lui (Eds.) Handbook of Multicultural Competencies in Counseling and Psychology. (pp. 365-382). Thousand Oaks, CA: Sage.
• Sue, D. W. (2001). Multidimensional facets of cultural competence. The Counseling Psychologist, 29, 790-821. • Sue, D. W., Arredondo, P., & McDavis, R. J. (1992). Multicultural counseling competencies and standards: A call to the profession.
Journal of Counseling and Development, 70, 477-486. • Sue, D. W., & Sue, D. (1999). Counseling the culturally different (3rd ed.). New York: John Wiley. • U.S. Department of Health and Human Services [USDHHS]. (2001). Mental health: Culture, race, and ethnicity: A supplement to mental
health: A report of the surgeon general. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services.
• Vacc, N. A., DeVaney, S. B., & Brendal, J. M. (2003). Counseling multicultural and diverse populations: Strategies for practitioners (4th ed.). New York: Brunner Routledge.
• Vera, E. M, Buhin, L., Montgomery, G., & Shin, R. (2005). Enhancing therapeutic interventions with people of color: Integrating outreach, advocacy, and prevention. In R. T. Carter (Ed.), Handbook of Racial-Cultural Psychology and Counseling: Training and Practice (pp. 477-491). Hoboken, N.J.: John Wiley.
• Vera, E. M., & Speight, S. L. (2007). Advocacy, outreach, and prevention: Integrating social action roles in professional training. In E. Aldarondo (Ed.), Advancing social justice through clinical practice (pp. 373-389). New York: Routledge.
• Whaley, A. L. (2001). Cultural mistrust and mental health services for African Americans: A review and meta-analysis. The Counseling Psychologist, 29, 513- 531.
• Whiteley, S. M., Mahaffey, P. J., & Geer, C. A. (1987). The campus counseling center: A profile of staffing patterns and services. Journal of College Student Personnel, 28, 71-81.