Embed Size (px)
Citation preview

7/30/2019 Building pyramids on Planet Zog
http://slidepdf.com/reader/full/building-pyramids-on-planet-zog 1/4
SERVICE REDESIGN
SPEECH & LANGUAGE THERAPY IN PRACTICE Autumn 20078
We are great believers in spotting any po-
tential challenges on the horizon and
proactively seeking means and methods
o addressing them beore they come
ully to ruition, or beore someone else comes along
and decides on our agenda. When we set out to discuss
the government’s recent papers and the challenges that
Children’s Centres would bring to our paediatric service,
we never suspected that a wholesale reorganisation
would emerge – or indeed that the enthusiasm and mo-
tivation rom each and every member o the team would
mean that our initial thoughts o a three to fve year plan
would turn into an almost overnight revolution…
A. THE SERVICEMiddlesbrough Primary Care Trust provides speech and
language therapy services or children in the Middles-brough and Redcar Cleveland areas in the North East o
England. (The speech and language therapy service or
adult neurological / acquired disorders is provided by
South Tees Acute Trust.) The population is in the region o
300,000 and there are 4,000 new births each year. The lo-
cality has nine Sure Start projects that are developing into
ourteen Children’s Centres, and our wards all into the
‘top ten’ most deprived in the UK (www.statistics.gov.uk).
Much o the population resides in urban areas, but there is
a proportion o rural and arming communities.
The service had a paediatric department (catering
or mainstream clinical work as well as language units
/ resource bases and assessment classes / support bases
in mainstream schools), a Sure Start department cover-
ing all nine projects, and a special needs department
(including children with learning disability, physical
disability, hearing impairment and autistic spectrum
disorders). There are 22.4 whole-time equivalent (wte)
speech and language therapists and 12.5 wte speech
and language therapy assistants supported by 4.2 wte
administrative sta.
Children aged 0 to 4 years living within Sure Start ar-
eas received therapy in homes, Sure Start Centres and
local nurseries. All other mainstream children received
therapy at one o three community clinics sited across
the patch; so children rom around 100 schools in an
area spanning 50 by 10 miles were travelling or any-
thing up to an hour each way to attend therapy. Need-
less to say, non-attendance was an issue. Children with
special needs attend specialist pre-school and educa-
tional provision, where therapy is provided.
A number o actors led us to consider a ull restruc-
turing o the service, including:
The National Service Framework or children, young
people and maternity services (DH, 2004) and Every
Child Matters (www.everychildmatters.gov.uk)
The Primary Care Trust move to locality working or
Public Health teams
Evidence rom the KITE randomised controlled trial
(Broomfeld, 2005)
Concern about ongoing non-attendance at commu-
nity clinic appointments
Concern about time lost rom schooling when chil-
dren did attend
Feedback rom parents indicating they wished to
have more accessible servicesFeedback rom education proessionals having ex-
perienced better joint working and improved liaison
rom Sure Start speech and language therapy teams
Transition rom Sure Start to Children’s Centres
Feedback rom our own sta about the benefts o
working within Sure Start teams and within localities.
B. THE PROCESSA planning week was set aside in October 2004, where
all senior speech and language therapy sta met to
conduct a SWOT (Strengths, Weaknesses, Opportunities,
Threats) analysis on current provision, determine what
our ideal service provision would be, and identiy an im-
plementation plan. All sta in the service were involvedon the frst day, identiying their wishes and concerns as
well as ideas and expectations, to inorm the process. We
1.
2.
3.
4.
5.
6.
7.
8.
9.
READ THIS IF YOUR
SERVICE
HAS PROBLEMS
WITH NON-
ATTENDANCE
LACKS EQUITY
NEEDS A CHANGE
•
•
•
Building pyramidson Planet Zog
Photos show zone teams
as they head of on a
team-building treasure
hunt.
Below let to right:
East zone, Central zone,
South zone, East
Cleveland zone, North zone, Eston zone,Redcar
zone.
A paediatric speech and language therapy service based in local communities andoering equitable provision appropriate to clinical need may sound like the stu o science fction but, as our superheroes Nikki Joyce and Jan Broomfeld relate, withcareul planning it is well within our orbit.

7/30/2019 Building pyramids on Planet Zog
http://slidepdf.com/reader/full/building-pyramids-on-planet-zog 2/4
SERVICE REDESIGN
SPEECH & LANGUAGE THERAPY IN PRACTICE Autumn 2007 9
had no external acilitator, identiying that two key mem-
bers o the management team were better placed to take
on this role. A crucial element was that each day ended
with the setting o the agenda or the ollowing day. The
timetable or the week was:
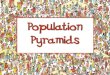
C. THE MODELThere were our major elements o the new service deliv-
ery model (fgure 1):
the caseload, including the Health Promotion aspect
o Sure Start – ‘Children’
the sta ng – ‘Service’
what we were going to do – ‘Delivery’,
where we were going to do it – ‘Location’.
Each element, based on the ‘triangle o need’, ormed a side
o a our-sided pyramid, and each element had three tiers.
1.
2.
3.
4.
1. Children (gure 2)
The base level addressed all children – regardless o any
communication need, the middle level addressed all
children with communication delay, and the top level
addressed all communication disordered children.
2. Service (gure 3)The base level addressed the nature o the locality teams,
the middle level addressed management o children with
communication delay, and the top level addressed spe-
cialist speech and language therapists within the service.
3. Delivery (gure 4)
The base level addressed health promotion and pre-
vention work, the middle level addressed assessment,
training and consultation, and the top level addressed
specifc speech and language therapy intervention.
4. Location (gure 5)
The base level incorporated working within the child’s
locality, the middle level incorporated structured set-
tings accessed by the child, and the top level addressedspecifc speech and language therapy locations.
D. IMPLEMENTATIONBetween October 2004 and September 2005, we inte-
grated our Sure Start and mainstream paediatric speech
and language therapy sta and reorganised into seven
locality teams which matched the developing Public
Health teams and the Local Authority Education clusters.
Each ‘Core Speech and Language Therapy Team’ consists
o a team lead (a senior / specialist therapist), together
with generalist speech and language therapists, speech
and language therapy assistants and administration and
clerical sessions. In addition, each specialist therapist is at-
tached to a core team, and each team has allocated timeand support rom a designated member o the speech
and language therapy management team. Each team has
been relocated to a base within their locality and has re-
sponsibility or the whole child population therein.
Each core team is responsible or
a. Caseload management – assessment and intervention
in homes, nurseries and schools within their locality
b. Training and liaison with education colleagues
c. Screening, including conducting Sure Start Language
Measures
d. Health promotion activities, linked with health visitors
and Children’s Centres
e. Gathering eedback and evaluating their practice
. Onward reerral and identifcation o children
requiring specialist input
g. Implementing care plans according to departmental
care pathways
Monday am All staf involved:Presentation by representativesrom the two Local Authoritieson Children’s CentresPresentation rom speech andlanguage therapy managementteam about aims and objectivesor the week Brainstorming session or all staf to identiy their wishes andconcerns, ideas and expectations
Monday pm Senior staf:Current acts and gures aboutthe population and caseloadsCollation o evidence and policiesDecision to move to locality
working
Tuesday Blue sky thinking – what wouldthe service look like i we werestarting rom scratch without anyresource or policy restrictions
Wednesday Determining the key elements o the service delivery model
Thursday Adding detail to the model – whowould do what to whom
Friday Identiying the action planTimescale or implementationPlan or consultation with keystakeholders – Primary Care Trust,Local Authorities includingEducation, parents, Sure StartmanagersPreparation o a presentation orall staf
Tuesday Full staf meeting to reveal theproposed model
•
•
•
•
•
•
•
•
•
Figure 3 Service
Specialistteam
Input rom core team,MDT and parents
OthersResponsibility with SLTA,
nursery, schoolInput rom SLT, specialist team as required
Core TeamInput rom specialist team, MDT, parents as required
Figure 1 The our elements
Children Service Delivery Location
Figure 2 Children
Disordered
Delayed / diferent
All children aged 0 - 16
Figure 4 Delivery
SpecicInput specifc
to disorderFrom specialist team
Assessments, training,diagnostic therapy
Support oered to core team
FocusedInput ocused on communicationInput and monitoring by others
SLTA doing specialist interventionTraining by SLT service
Assessment by core team SLTCore team SLT involved with “at risk” amilies
Holistic2 Year screening by core team SLT
Health promotion • Prevention • Training • Environmental enrichment
Figure 5 Location
SLTspecic
locationsUsed or low incidencedisorders and located
according to prevalence
Community o child’s residenceHealth settings, schools, nurseries, homes
EverywhereAll locations that the child and amily may access

7/30/2019 Building pyramids on Planet Zog
http://slidepdf.com/reader/full/building-pyramids-on-planet-zog 3/4SPEECH & LANGUAGE THERAPY IN PRACTICE Autumn 200710
SERVICE REDESIGN
tegic direction o the service. It comprises fve Clinical
Co-ordinators, a Consultant speech and language thera-
pist and a Proessional Lead. Each person has a clinical
specialism and acts in a specialist capacity. In addition,
the Clinical Co-ordinators have specifc management
responsibilities representing the whole service, such
as child protection, clinical supervision and audit. TheConsultant has responsibility or research and develop-
ment and acilitating evidence based practice. The Pro-
essional Lead has responsibility or sta and fnancial
management.
The two case examples in fgure 6 show how the mod-
el is working in practice.
E. OUTCOMESWe have recently consulted a range o parents to obtain
eedback about our reconfgured service. All responses
were extremely positive; in particular, they liked
Children being seen in schools and nurseries, as they
know the setting and they don’t need to travel
Less time being lost rom the curriculumThe same small team stays involved throughout
The service is exible to meet the needs o amilies and
children
They see speech and language therapists and teach-
ing sta talking to each other
They still have the opportunity to attend their child’s
appointments
They get termly (at least) updates by phone or post
about their child’s progress; they also still get ‘home-
work’ packs to practise
They like seeing speech and language therapists at Chil-
dren’s Centre activities, so they can chat inormally about
concerns without having to have been properly reerred.
We are in the process o conducting a ormal evaluation
with our education and health colleagues. However, com-
ments about the ollowing issues have been made inor-
mally to us rom both inside and outside the service:
Better access to speech and language therapists by
teaching sta - and o teachers by speech and lan-
guage therapy sta - to get advice, ask questions, and
discuss kids we’re worried about
Fewer inappropriate reerrals
Better attendance at appointments, so therapy is more
eective
The service is ar more exible and responsive to client
and school need
Children hardly miss any class time now
Cycle o discharge and re-reerral has all but ceased
– children are maintained on the active caseloadthroughout their pre-school years (at least)
Reerrals now made o harder to reach amilies who
wouldn’t have attended central clinic but do (usually
attend school
Increased contact with health visitors, maternity sta
and Children’s Centre teams has increased reerrals o
very young children, oten with complex needs. This
has led to earlier access to the child development cen-
tre, earlier multidisciplinary team assessment, earlier
diagnosis and appropriate support in place when the
child starts school.
Sure Start health promotion activities are being rolled
out across the patch
Multidisciplinary / multi-agency working is becominga reality.
In terms o acts and fgures, reerrals have doubled
in the space o a year rom 289 in Jan-June 2005 to 540
in Jan-June 2006, with ewer inappropriate reerrals be-
ing received. The total active caseload is 2843. The active
caseload in each zone is between 226 and 312, and the
active caseload managed by specialists is between 25
and 169. Non-attendance has dropped rom 780 in the
year 02-03 to 360 in 05-06.
Feedback rom reerrers is that they are now more aware
o who we are, where we are and what we do and thereore
they are more likely to reer. They are also more confdent
that the child will access the service as we are based in
schools and the community. The implications o this or the
service are that some o the preventative Sure Start activi-
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Figure 6 In practice
Connor was seen at home by a speech andlanguage therapy assistant or a Sure StartLanguage Measure at 2 years old. At thattime he had an expressive vocabulary o 30single words and the assistant encouragedhis mum to attend the Sure Start Parentand Toddler Group. The assistant visits thegroup each month. When on the next visitmum expressed concerns about Connor’seeding, the assistant supported mum inmaking a ormal reerral to the speechand language therapy service. Connor wasassessed at 30 months by the core teamspeech and language therapist who eltthat he would beneft rom assessment bythe dysphagia specialist.The dysphagia specialist therapist oereda joint assessment appointment with thecore team therapist at the Parent and Tod-dler Group. Guidance or management o the di culty was given to both mum andthe core team.During the next three months, the core
team therapist became increasingly con-cerned about Connor’s developmentalmilestones and reerred him to the spe-cialist pre-school assessment provision.Multidisciplinary assessment identifedmoderate global delay with specifc com-munication di culties. He was given aplace in the local Children’s Centre nurserywhere his di culties could be addressed.The core team will continue to support thenursery and mum to maximise his commu-nication potential.
h. Ensuring equity o speech and language therapy provision
across the whole patch, whilst meeting local need.
We have a number o specialist therapists, covering
specifc language impairment, specifc speech disorder,
dysuency, ENT and clet lip and palate, autism spec-
trum disorder, learning disability, physical disability and
AAC, hearing impairment and dysphagia. Each specialistis responsible or:
i. Specialist diagnostic assessment and intervention
ii. Providing advice and support to all core teams
iii. Operating ‘surgery’ time or core teams, including
conducting visits and directing therapy
iv. Reviewing and developing specifc care pathways
v. Providing training to colleagues both within and
outwith the service
vi. Conducting evaluation and appraisal o best current
evidence base
vii. Working together with the management team to
continuously evaluate and develop the service.
The speech and language therapy management team
is responsible or the operational management and stra-
Sarah was reerred or speech and lan-guage therapy assessment by her nurs-ery teacher. She was assessed at 3 years 9
months in nursery by the core team thera-pist who identifed signifcant speech di-fculties. Sarah was then placed in an earlyspeech skills group with her peers, run bythe speech and language therapy assistantin her nursery. Ater hal a term, at 4 years,Sarah was still very di cult to understandand all involved were expressing concern.The specialist therapist was consulted andit was agreed that Sarah should receive aperiod o diagnostic assessment. She wasgrouped with three similar children romthe locality and the intervention was de-livered in a local Children’s Centre locationby the specialist therapist supported bya speech and language therapy assistantrom the zone.Sarah was identifed as presenting with in-consistent deviant phonological disorder.A period o intervention ollowing the CoreVocabulary approach (Dodd et al ., 2006)then occurred; this was run weekly in nurs-ery by the specialist therapist, with both thezone therapist (or the purposes o training)and a zone assistant present. The zone as-
sistant then conducted a second weeklypractice session at home in order to keepmum involved. Ater a term o input, Sarahhad made good progress and was recently jointly re-assessed by the zone and specialisttherapists. Her next period o interventionocusing on specifc sound targets has beenplanned jointly and is being implementedby the speech and language therapy assist-ant; weekly support is available rom thezone therapist and monthly update discus-sions with the specialist are planned.

7/30/2019 Building pyramids on Planet Zog
http://slidepdf.com/reader/full/building-pyramids-on-planet-zog 4/4
SERVICE REDESIGN / RECOMMENDED READING
SPEECH & LANGUAGE THERAPY IN PRACTICE Autumn 2007 11
ties have reduced to increase time or direct intervention.
We have also become smarter about putting children
on review. Because we are more accessible and have
provided training into schools, education colleagues are
more comortable with monitoring the children and re-
reerring and we provide them with clear guidelines as
to what to look or and when to re-reer. This helps tokeep the numbers manageable.
F. NEXT STEPSThe ormal evaluation is just beginning – this will be an
ongoing process and will inuence uture modifcations
to the service. However, we have a ew outstanding mat-
ters to be addressed:
We need to consider the issue o ensuring parents are
ully engaged when children are seen in school
At present, much o the restructure has ocused on
the ‘mainstream’ element o the service, although the
special needs specialists have been involved through
surgery time and the inclusion agenda. However, a
ull review o the special needs speech and languagetherapy service is planned during 2007
The broader issue o mainstreaming the Sure Start budg-
et and securing unding or the service developments
we have identifed as a result o being more accessible is
on the agenda, but we hope that our integrated model
will have put us on a sounder ooting. Our stakeholders
have been extremely supportive o the reorganisation
to date which can only be to the good.
We are hugely grateul to the Primary Care Trust boards
and the Local Education Authority o cers or their support
and enthusiasm, and or sharing the vision with us. We are
grateul to all the parents who contributed to our thinking
through various eedback mechanisms beore, during and
ater the reorganisation. And we are indebted to every sin-
gle member o sta, whether therapist, assistant or admin-istrative o cer, or the initial drive and the ongoing com-
mitment to building pyramids on Planet Zog!
Nikki Joyce is Proessional Lead and Jan Broomfeld is Con-
sultant Speech and Language Therapist or the Children’s
Speech and Language Therapy Service o Middlesbrough
Primary Care Trust. For urther inormation please contact
them at [email protected]
ReerencesBroomfeld, J. (2005) ‘The case or ying KITEs’, Speech & Language
Therapy in Practice Winter, pp. 14-17.
Great Britain. Department o Health, Department or Education
and Skills (2004) National Service Framework or children, young
people and maternity services.London: The Stationery O ce. [On-
line at www.dh.gov.uk]Dodd, B., Holm, A., Crosbie, S. & McIntosh, B. (2006) ‘A core vocab-
ulary approach or management o inconsistent speech disorder’,
Advances in Speech-Language Pathology 8(3), pp. 220-230.
*Planet Zog is a place or situation ar removed rom what is cur-rently happening, and a general name or any sci-f planet.
1.
2.
3.
Recommended ReadingRecommended Reading Given the overwhelming amount o inormation available, we need to be selective in what we read. Even then
we fnd that papers do not always include an explicit link between the theory / experiment and its direct or
indirect implications or practice. Articles in journals have gone through a painstaking process o peer review
but it is ultimately or you, the reader, to judge whether the stated result is a) valid and b) clinically important
– in other words, why and how the article will change your practice.
In this occasional section, readers explain why they would recommend a particular article rom a peer re-
viewed journal to their colleagues. While this is a personal response that ocuses on clinical importance and
practicalities, the author may also wish to comment on actors such as study design / validity and statistics /
statistical signifcance.
Jane Armstrong says:
“This article about treatment e cacy or chronic cough was emailed to
me by my reerring ENT Consultant. In our current climate o everything
being evidence based it is nice to see an article which shouts the vir-
tues o speech and language therapy in the area o voice and cough
management. For those o us who work with voice and / or cough, this
article is a welcome sight.
There are our components to Vertigan et al.’s treatment method or
chronic cough:
1. Education
2. Strategies to reduce cough
3. Reduce laryngeal irritation / improve vocal hygiene
4. Psycho-educational counselling
The placebo group got a course on healthy liestyle education which included relaxation, stress manage-
ment, exercise and diet.
Both groups attended our intervention sessions with a qualifed speech and language therapist.
1. Education
Ideas:
No physiological beneft rom cough
Capacity or voluntary cough control
Futility o repeated coughing
Negative side eects o repeated coughing
Benefts o cough suppression
2. Cough suppression
Ideas:
Anticipate when a cough was about to occur
Pattern and degree o warning beore the cough
Implement a strategy to suppress or replace the cough
3. Vocal Hygiene
Ideas:
Reduce laryngeal irritation
Maximise hydration in order to reduce stimulation o cough receptors
Relaxed breathing exercises provided or those with inspiratory dyspnoea
4. Psycho-educational
Ideas:Address some dierences between behavioural and medical treatment
Aim to acilitate acceptance o a behavioural approach
Facilitate internalisation o control over their cough
View the cough as something individuals do in response to irritating stimuli rather than a phenomenon
outside o their control.
This approach is designed to reduce the load on the larynx by improving the e ciency o voicing and promot-
ing adequate breath support and oral resonance. Lots o home practice was encouraged.
The results show a signifcant improvement in those people who were receiving the treatment rather than the
placebo. And to quote rom the article, ‘in conclusion, clinical judgement and symptom ratings support the
hypothesis that speech pathology treatment is an eective behavioural intervention or chronic cough which
could be considered a valid alternative or individuals whose cough persists despite medical intervention.’”
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
SLTP
REFLECTIONS
DO WE THINK AHEAD SO WE CAN FORGE
OUR OWN PATH OR DO WE WAIT FOR
OTHERS TO DECIDE IT FOR US?
DO WE GIVE SERVICE REDESIGN THE
PLANNING TIME AND ATTENTION TO DETAIL
THAT IT NEEDS?
DO WE LISTEN TO WHAT CLIENTS, STAFF
AND THE WIDER TEAM SAY WORKS BEST?
•
•
•
VOICE / CHRONIC COUGH
Vertigan, A.E., Theodoros,
D.G., Gibson, P.G. & Wink-
worth, A.L. (2006) ‘E cacy
o speech pathology man-
agement or chronic cough:
a randomised placebo con-
trolled trial o treatmente cac y’,
Thorax, December 61, pp.
1065 - 1069. [Available via
www.thorax.bmj.com.]
Jane Armstrong is an independent speech and language therapist in Edinburgh.