Embed Size (px)
Citation preview

BuildingonSuccess– MalariaControlandEliminationSwissTPHWinterSymposium2016
Definingsuccessfornextgenerationmalariavaccines
MelissaPenny,Basel8th December2016
Epidemiology and Public HealthHealth Systems Research and Dynamical Modelling

Elimination?
Bhattetal(2015)TheeffectofmalariacontrolonPlasmodiumFalciparuminAfricabetween2000and2015,Nature, 526:207
2000 2015
Vectorcontrol
2000-2015reductioninmalariaincidenceandmortality
• 2015-2030targets:90%casereduction,eliminatein35countries• Successwillnotbesimplecontinuationsofcurrenttoolsand
interventionmixes. Newtoolswillberequired• Drug andinsecticideresistance
Vectorcontrol
MalariaincidenceavertedReductioninmalariaprevalence
treatment

Frameworkfortoolsforelimination
Reducetransmission• Vectorcontrol• Prophylaxis• VaccinesClearinfections• Case-management• Diagnostics• Drugs• Campaignsandreactivecasedetection
andtreatmentPreventreintroduction• Surveillanceandresponse• Casemanagement
Availabletools(present+10years)Combinationswillberequired• Drugs
⎯ Singleencounterradicalcure⎯ Prophylaxis
• Diagnostics• Futurevaccines• Vectorcontrol
⎯ InsecticideTreatedNets⎯ IndoorResidualSpraying⎯ Larvalcontrols,sourcemanagement⎯ Novelpush-pull
• Logisticssupport• Modellingandquantitativeanalysis
Region/geographictailoredinterventionmixes– basedonepidemiologyandcapacity

Designingnewmalariavaccines
Discovery Preclinical Earlyclinical Clinical Implementation
ResearchanddiscoveryAntigendiscovery
PotencyToxicologyScheduleDeliverysystemAdjuvantMechanismofaction
RouteofimmunizationDose/intervalsTargetgroupsAdjuvantEfficacy:challengestudiesTrialDesign
PhaseII/IIIefficacyTrialdesignHealthImpactassessmentEconomics/cost-effectiveness
>10years < 10years

Designingnewmalariavaccines
Discovery Preclinical Earlyclinical Clinical Implementation
ResearchanddiscoveryAntigendiscovery
PotencyToxicologyScheduleDeliverysystemAdjuvantMechanismofaction
RouteofimmunizationDose/intervalsTargetgroupsAdjuvantEfficacy:challengestudiesTrialDesign
PhaseII/IIIefficacyTrialdesignHealthImpactassessmentEconomics/cost-effectiveness
< 10years
Modellingandsimulationtoinformdevelopment

Potentialimpact
• Guide thinkingonmalariadynamics• Exploreminimumpropertiesrequiredofnewtools(e.g.efficacy,duration)
• Testscenarios/strategies:estimateimpactofnewtoolsfordifferenttargetages,coverage,roll-out.Whatcoverageisrequiredtomeethealthgoals?
• Explorecombinationstofindmixesthatoptimise overvariouscriteria
• Effectivenessofinterventionsintherealworldandimpactbeyondtrials
• Economicanalysis
Modellingandsimulation:frameworksfordecisions
Model-basedframeworksDifferentmodeltypes• static• spatial• deterministic• stochastic• compartmental• Individual-based
models
• Naturalhistoryofmalaria
• Mechanismsofactionofnewinterventions
• Earlyestimatesofimpact/protectionandaction
• Efficacyfromlatertrials
Observable/Data /earlyknowledgeof
interventions

Simulationmodelofmalariaepidemiologyandcontrol
Uninfected Infected Infectious
Drug
Death
Sick
• Uncomplicated• Severe
Seektreatment• Treatment• Hospitalised
• Parasitedensities• Infectiousness• Numberofinfections• Immunity• Druglevel
• Healthsystem• Drugs&quality• Adherence• Compliance
• Infectiousness• Mosquitodensity• Feedingcycle• Parasitedevelopment
• Seasonality
Calibratedbyformalfittingtodatafromfieldstudies.
OpenMalaria:Individual-basedstochasticsimulatorofmalariaepidemiologyandcontrol
opensource:
https://github.com/SwissTPH/openmalaria/wiki
• Drugs• VectorControl• Vaccine• Masstreatment

Designingnewmalariavaccines
Discovery Preclinical Earlyclinical Clinical Implementation
PhaseII/IIIefficacyTrialdesignHealthImpactassessmentEconomics/cost-effectiveness
< 10years
Example:modellingtoestimateRTS,Simpact

Circumsporozoite proteinGeneticallyengineeredcentralCS-tandemrepeatfusedwithS-antigenofHBs
TheGSKmalariavaccineRTS,S/AS01
RTS,S/AS01PhaseIIIVaccineefficacy(VE)againstclinicaldisease(32monthspostdose3)
VEinchildren[95%CI]3doses
VEininfants[95%CI]3dose
VEinchildren[95%CI]4doses
VEininfants[95%CI]4doses
Clinicalmalaria 35·2%[30·5to39·5] 20·3%[13·6to26·5] 43·9%[39·7to47·8] 20·3%[13·6to26·5]
Severe malaria 4·5%[–20·6to24·5] 7·9%[–23·3to31·2] 34·9%[15·6to50·0] 11·9%[-18·3to34·5]
TheRTS,SClinicalTrialsPartnership(2015)Lancet
Infants6-12weeksofage:7100Children5-17monthsofage:890011centersin7Africancountries
Moderatelyefficaciousvaccine
• EMApositivescientificopinion• WHOrecommendation:pilotimplementationsbeforewidercountry
levelintroduction…toensurethat4dosesofmalariavaccinecanbegiven……in3-5distinctepidemiologicalsettings insub-SaharanAfrica,atsubnationallevel,coveringmoderate-to-hightransmissionsettings

RTS,S clinicaldevelopment
1984 1994 2004 2014 2024 2034
Identificationofcandidate
FirstCHMItrials
PhaseIIIResults
FirstEndemiccountrytrials
StartofPhaseII
Likelymodeofaction
Targetgroupdetermined
WHO:modelbasedpredictionsofimpactbeyondatrial
Vaccinatedandprotected
RationaleProtecttheagegroupswithhighestmalariaburdenFeasibilityindelivery:schedules• 6-12weeks• 5-17months
Rolloutof ACTandITNsGatesMalariaForum: “chartalong-termcoursetoeradicate…...”
FirstEfficacyEstimates
StartofPhaseIII
Estimatesofdurationofeffectonclinicaldisease
EMApositivescientificopinionWHOrecommendation

Age of vaccinee
Cas
es a
vert
ed b
y R
TS,S
• Noone‘perfect’model• Differencesreflectmodelingchoicesanduncertaintyincalibrationdata
• Ensembleapproachallowsexplorationofoutcomeranges
Ensembleapproachtomodelinghealthimpact
WHO requestedpredictionsfor:• Definedtargetagegrouporschedule• Realisticcoverage ofchildren• Harmonised inputsandoutputs• Expectedeffectiveness:%and numbereventsaverted• cost-effectiveness(& comparisonwithinterventions &
vaccines)• Rolein additiontohighcoverageofinsecticidetreated
netsandroutinetreatment
WHY?:• Understandimpactbeyondthetrial
(controlsettings).Trialnotpoweredtoevaluateimpactagainstseverediseaseandmortality,especiallyinlow-moderatetransmissionsettings.
Whatwasnotsimulated:• Indicateimpactoutsideoftestedage
Potentialof alternativevaccinedeliveryorintegrationintootherprograms

Dynamicalmodelingisinformedbytrialdatatoprojectfuturepublichealthimpact
• High treatmentrates• High insecticidetreated
net(ITN)use• Limitedtransmission
settings• <5year follow-up• Data:Vaccineefficacy
Clinical Trial Setting
DATA
Future Use Case
• Range oftreatmentrates• Range ofITNuse• Broadspectrumof
transmissionsettings• >5year impact• Mortalityimpact• Deliverystrategy:
Vaccinationat6-9months,27months
SIMULATIONS
Calibrated Malaria Models• Trial data• Historical
data
Assessed Vaccine
Properties
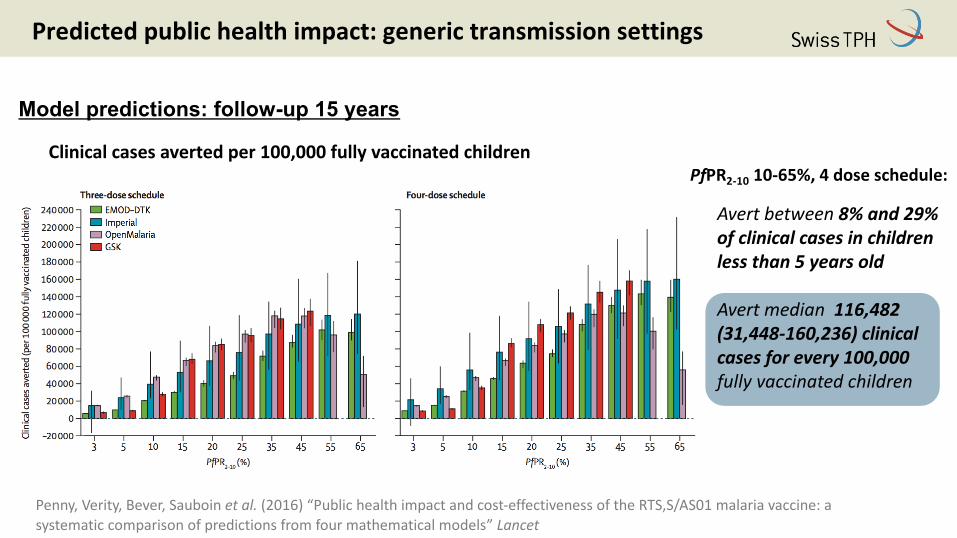
Predictedpublichealthimpact:generictransmissionsettings
Clinicalcasesavertedper100,000fullyvaccinatedchildrenPfPR2-10 10-65%,4doseschedule:
Avertbetween8%and29%ofclinicalcasesinchildrenlessthan5yearsold
Avertmedian116,482(31,448-160,236)clinicalcases forevery100,000fullyvaccinatedchildren
Model predictions: follow-up 15 years
Penny,Verity,Bever,Sauboin etal. (2016)“Publichealthimpactandcost-effectivenessoftheRTS,S/AS01malariavaccine:asystematiccomparisonofpredictionsfromfourmathematicalmodels”Lancet

Publichealthimpact– ageshiftofclinicaldisease
low endemicity
age (years)
clin
ical
cas
es a
verte
d (t
hous
ands
)
0 5 10 15
010
2030
40
(PfPR2−10=10%)
high endemicity
age (years)
clin
ical
cas
es a
verte
d (t
hous
ands
)
0 5 10 15
010
2030
40
(PfPR2−10=50%)
Clinicalcasesavertedper100,000fullyvaccinatedchildrenbyage
Vaccinatedchildrennotbecominginfected
Vaccineprotectionwornoff,leftwithlowerimmunitycomparedtonon-vaccinated
Age(years) Age(years)
Penny,Verity,Bever,Sauboin etal. (2016)“Publichealthimpactandcost-effectivenessoftheRTS,S/AS01malariavaccine:asystematiccomparisonofpredictionsfromfourmathematicalmodels”Lancet

• RTS,Sislikelytohavepositiveimpactwithpotentialforsubstantialpublichealthbenefits,butthatcarefulconsiderationofthecost-effectivenesscomparedtootherinterventionsshouldbemadeinthecontextoflocalprioritiesandhealthsystems.
Cost-effectivenessrangeandcomparisonwithothermalariapreventativeinterventions
1.Whiteetal.2011(MalariaJournal)ITN:Insecticide-Treated Nets;IRS:IndoorResidual Spraying;IPT:IntermittentPreventive Treatment
RangesshowvariationsacrosscountriesandmodelsforRTS,Sandacrossstudiesforotherinterventions
WHOandGAVIperspective:comparisontootherinterventions• Vaccinepricerangetestedfrom$2to$10
perdose• Cost-effectivenessestimatesforother
malariainterventionsfromliterature1
• Cost-effectivenessestimatesfromtheliteraturehavebeenmadeinadifferentcontextthancurrentmodelingwork
Penny,Verity,Bever,Sauboin etal. (2016)“Publichealthimpactandcost-effectivenessoftheRTS,S/AS01malariavaccine:asystematiccomparisonofpredictionsfromfourmathematicalmodels”Lancet

Country-levelorsub-nationalperspective:estimatesofRTS,Simpactandcost-effectiveness
Mixofprevalencelevels
Seasonality
Accesstocare&costofillness
DTPcoverage
country-levelestimates
Costofvaccination
Country-specificinputsDemographics
models
Cumulativenumberofclinicalcasesavertedper100,000vaccinated(atyear10followingvaccineintroduction)
Galactionova etal.(2016)“Countryspecificpredictionsofthecost-effectivenessofmalariavaccineRTS,S/AS01inendemicAfrica” Vaccine

1984 1994 2004 2014 2024 2034
Identificationofcandidate
FirstCHMItrials
PhaseIIIResults
FirstEndemiccountrytrials
StartofPhaseII
Rolloutof ACTandITNsGatesMalariaForum: “chartalong-termcoursetoeradicate…...”
Likelymodeofaction
Referenceperiodformodellingofnextgenerationmalariavaccines
FirstEfficacyEstimates
Targetgroupdetermined
Estimatesofdurationofeffectonclinicaldisease
StartofPhaseIII
Nextgenerationmalariavaccines
Target/schedules/eliminationgoals
NextgenerationmalariavaccinesCHMI/trials
WHO:modelbasedpredictionsofimpactbeyondatrial
SuccessforRTS,Sandfuturevaccines

Modellingtoguidethinkingforfuturemalariavaccines
Discovery Preclinical Earlyclinical Clinical Implementation
< 10years
Modellingandsimulationtoinformdevelopment
Vaccinesmusthaveimpactontransmission,ratherthanjustonmortalityandmorbidityreduction• Immunogenicityandimmunecorrelates(Whiteetal(2015)LancetInf.Dis.)• Prioritizationoftargetproductprofiles (combinations,doses,tradeoffbetweenefficacy,
durationofprotection,coverage)• immunizationschedulesanddeliveryroutes (andfeasibility)• targetdemographicgroups• Dosing(andfeasibility)• Settings(prevalence,seasonality,healthsystems)• TPPforMassvaccination:high-riskpopulations(pregnantwomen)• UseofControlledhumanmalariainfectionandmodelsforcandidateprioritization

Minimalandoptimalproperties,alternative deliveries
rain
Durationofprotection
rain rain
Malaria
Idealeliminationvaccine
Foreseeable:vaccinewithshorterdurationofprotectionvaccine
Booster Booster
rain
Malaria
rain
Malaria
Adapted from BMGF and PATH-MVI

Roleforelimination:exampletransmissioneffects0.
000.
020.
040.
060.
08
Low transmission Medium transmission High transmission
prop
ortio
n of
vec
tors
infe
cted
at e
ach
feed
EPI
EPI booster
EPI mass vaccination
0 5 10 15 20 0 5 10 15 20time (years)
0 5 10 15 20
Pre-erythrocytic vaccines• Observesomereductionoftransmissionwithhighinitial
efficacy(herdimmunitywhendeliveredviamassvaccination)• Interruptionoftransmissionforlowtransmissionsettings
Penny et al. (2008) Plos One
Modellingcanguide thinkingon:• Coverageofmassvaccination
toachievesuccess• Longevityofprotection
required? =minimalandTargetProductProfiles
• Determinantsofsuccess:minimumcoveragelevel?minimumnumberofrounds?
• Costsavings?

Predictionsoftransmissionblockingvaccineeffectsovertime
TransmissionblockingvaccinesPossibletoinduceherdimmunityandinterrupttransmissionwhendeliveredviamassvaccination
Massvaccination
prop
ortio
nofvectors
infected
ate
achfeed
Lowtransmission Mediantransmission
0 5 10 15 20 0 5 10 15 20
time(years)
0.00
0.02
0.04
0.06
0.08
EPIMassvaccination
time(years)
Immunizinginfants
Modellingcanguide thinkingon:• Howmanyrounds,coverageand
timingofmassvaccinationtoachievesuccess?
• Longevityofprotectionrequired?• Otherinterventioncombinationsto
accelerateinterruption oftransmission
Penny et al. (2008) Plos One

Episodes per person year
0
1
2
3
4
Years since start of intervention
-1 1 3 5 7 9 11 13 15 17 19 21
Clinical incidence envelopearm2=no int
Episodes per person year
0
1
2
3
4
Years since start of intervention
-1 1 3 5 7 9 11 13 15 17 19 21
Clinical incidence envelopearm2=IRS
Episodes per person year
0
1
2
3
4
Years since start of intervention
-1 1 3 5 7 9 11 13 15 17 19 21
Clinical incidence envelopearm2=rescue
Clin
ical
epi
sode
s pe
r per
son
per a
nnum
No intervention
IRS
IRS & SSM-TBV
Years since start of program
Combinationwithotherinterventions
No IRS or SSM-TBVIRS IRS and SSM-TBV
Exampleeffectonclinicalincidenceandprobabilitytointerrupttransmission
• Profileofnewinterventionsneededontopofexistinginterventionstoachieveelimination
• Whichsettings?
Smith et al. (2008) Trends in Parasitology

Challengesformodellingclose-to-elimination
Vivax andothermalariaspecies
Lowtransmissionandeliminationsettings• Parasitediversityandparasiterelatednessastransmissiondeclines• Incidencebyagewithchangingpopulationandindividualimmunity• Data:mostmodelsdesignedandparameterised forhyper- andmesoendemic settings
Effectsofpopulationsizeandconnectivityonthechancesofelimination• Connectionbetweenpopulations(movementsofpeople/mosquitoes)makeeliminationmoredifficult• Bothpopulationsizeandconnectivityarehardtoquantify

Fromdefiningsuccesstoachievingsuccess
Otherimportanttoolsforinnovatingnewinterventions:• Community• Ideas• Integrationofalldisciplinesinthe
developmentpathwaythroughtoimplementation
Availabletools(present+10years)Combinationswillberequired• Drugs
⎯ Singleencounterradicalcure⎯ Prophylaxis
• Diagnostics• Newvaccines• Vectorcontrol
⎯ InsecticideTreatedNets⎯ IndoorResidualSpraying⎯ Larvalcontrols,sourcemanagement⎯ Novelpush-pull
• Fieldlogisticssupport• Modellingandquantitativeanalysis

With many thanks to WHO Advisory Committeethe RTS,S Clinical Trials Partnership and Clinical trial units, and vaccinated children and their families.
Acknowledgements
ChristopheSauboinNicholasVandeVelde
RobertVerityMichaelWhiteJamieGriffinAzra Ghani
MelissaPennyKatyaGalactionovaPeterPemberton-RossNicolasMaireOlivierBrietTomSmithMarcelTannerMalariamodellingteamatSwissTPH
StefanFlascheMarkJit
CaitlinBeverEdwardWengerPhilipEckhoff
Farzana MuhibDebAtherlyCarlaBotting
FundingPATH-MalariaVaccineInitiativeBillandMelindaGatesfoundation





























