Embed Size (px)
Citation preview

1
BRYAN PRIMARY CARE CONFERENCE 2019DAVID NEWTON, MD
GASTROENTEROLOGY SPECIALTIES/LINCOLN ENDOSCOPY CENTER
I HAVE NO RELEVANT/IRRELEVANT DISCLOSURES

2
OBJECTIVES
• Identify patients at risk for chronic hepatitis C infection
• Identify patients with chronic hepatitis C who should receive treatment
• Understand the natural history of non-alcoholic fatty liver disease
• Understand available treatment options for non-alcoholic fatty liver disease
OUTLINE
• Hepatitis C
• NASH/NAFLD
3
HEPATITIS C
Which of the following statements is TRUE regarding the epidemiology of chronic hepatitis C virus (HCV) infection?
A. The prevalence of chronic HCV has risen between 1990-2000 and 2001-2010
B. Blood transfusions before 1992 represent the most common route of transmission
C. The burden of chronic HCV is higher in North America than sub-Saharan Africa
D. The prevalence of chronic HCV is highest in U.S. adults born between 1945-1965
E. Approximately 5-10% of individuals with HIV also harbor chronic HCV infection

4
EPIDEMIOLOGY
• 37 million with current or past infection
• 21 million with chronic HCV
• Peak prevalence observed in individuals born between 1945 and 1965
• New evidence suggesting prevalence of younger individuals infected may be surpassing that of baby boomers
• Injection drug use most important risk factor
• Male gender
• Non-Hispanic African American race
• Low socioeconomic status
• High school education or less
• >10 lifetime sexual partners
RISK FACTORS
ODDS RATIO• IV Drug use 49.6
• Blood transfusion 10.9
• Sex with IV drug user 6.3
• Incarceration >3 days 2.9
• Religious scarification 2.8
• Having been struck or cut with a bloody object 2.1
• Pierced ears or body parts 2
• Immunoglobulin injection 1.6

5
CLINICAL PRESENTATION
• Patients with HCV often have high symptom burden – not often related directly to HCV, however
• Abdominal pain, itching, dark urine – only symptoms which occurred more commonly in those with HCV compared to healthy controls – small numbers
• Cognitive impairment – unclear pathophysiology
• Extrahepatic Manifestations
• Cryoglobulinemia
• Kidney disease – membranoproliferative glomerulonephritis
• AI disorders – thyroiditis, autoantibodies
• Porphyria cutanea tarda, lichen planus
• Diabetes
• Laboratory Findings
• 1/3 with normal ALT
• ¼ with ALT >2x ULN
• Alpha fetoprotein (AFP) may be elevated
NATURAL HISTORY
• Most cases of acute HCV infection asymptomatic
• Fulminant disease is rare
• Slowly progressive disease – cirrhosis generally develops over 20-30 years
• Number one cause of cirrhosis and indication for liver transplant in the US
• Once advanced fibrosis is present, cirrhosis progression 10%/year
• HCV accounts for 1/3 of all cases of HCC in the U.S. 0-3%/year
• Generally cirrhosis, but up to 10% with minimal fibrosis noted at time of resection

6
RISK FACTORS FOR PROGRESSION
• Alcohol intake >50g/day
• 34% increased rate of fibrosis progression.
• Increased risk of HCC
• Viral factors
• Multiple genotypes
• Coinfection – HBV, HIV
• Obesity, DM, insulin resistance
You are seeing a 45-year-old man for the first time for annual physical. He states that he had routine labs performed at the local health fair and was told he needed to see a doctor because of hepatitis C. He is otherwise healthy and takes no medications.
VS: unremarkable. Weight 287. AST 72 ALT 100HCV Ab +
What is the next best step in this patient’s management
A. Treat the patient with Harvoni
B. Check HCV RNA
C. Refer to hepatologist for HCV treatment
D. RUQ US
7
DIAGNOSIS AND EVALUATION
WHO TO TEST
• Elevated LFT’s
• Extrahepatic manifestations
• Cryoglobulinemia, porphyria
• Risk factors – IVDU etc.
• Born between 1945-1965
TESTING• HCV antibody
• HCV RNA – confirms diagnosis
• Initial test if patients with severe immunocompromised state (transplant patients, AIDS), HD patients, suspected acute HCV
• INR, HFP, CBC, UA, Vitamin D, HIV, HAV, HBV
• Fibrosis – US, elastography, fibrosure, biopsy
Which patient should be considered for hepatitis C treatment
A. Otherwise healthy 65 year old female infected via blood transfusion during childbirth in her 30’s
B. 55 year old man with HCV cirrhosis and hepatocellular carcinoma
C. 35 year old man with porphyria cutanea tarda
D. 60 year old man with HCV cirrhosis being considered for liver transplantation
E. 33 year old woman with alcoholic liver disease and chronic HCV infection. The patient continues to drink.
F. All of the above

8
TREATMENT
• Who to treat
• Treatment is recommended for all patients with chronic HCV infection, except those with short life-expectancy that cannot be remediated by HCV therapy, liver transplantation or another directed therapy. Patients with a short life-expectancy owing to liver disease should be managed in consultation with an expert – HCV Guidelines (4/9/19)
• SVR has been shown to result in decreased:
• Progression of fibrosis (regression!)
• Hepatic decompensation
• HCC - >70%
• Liver related mortality/transplantation –90%
TREATMENT
LIMITATIONS DIRECT-ACTING ANTIVIRAL(DAA)
• Interferon free regimens now the standard of care
• Pan-genotypic options available
• SVR rates >90% with 8-24 weeks of treatment
• Minimal side effects
9
HCV – SUMMARY
• Have a high suspicion for hepatitis C infection
• Continue to screen baby boomer population with one time HCV antibody
• Confirm positive antibody test with HCV RNA
• Treatment indicated for the majority of individuals with hepatitis C
NON-ALCOHOLIC FATTY LIVER DISEASE
10
DEFINITIONS
• Non-alcoholic fatty liver disease – steatosis with or without inflammation and fibrosis. No secondary causes of steatosis are present
• Alcohol, Meds, HCV etc.
• Non-alcoholic fatty liver – steatosis without evidence of significant inflammation
• Rarely develops into cirrhosis (~4%)
• Non-alcoholic steatohepatitis – steatosis associated with hepatic inflammation – may be indistinguishable from alcoholic steatohepatitis
• More commonly can develop into cirrhosis (~25%)
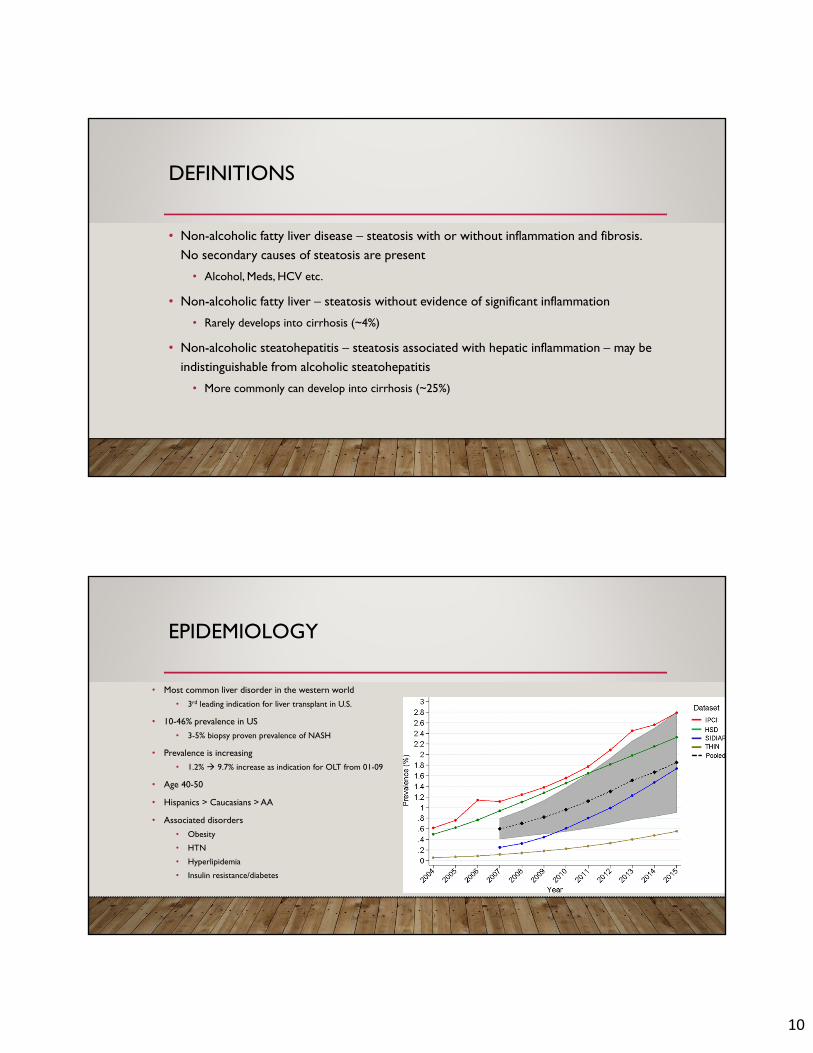
EPIDEMIOLOGY
• Most common liver disorder in the western world
• 3rd leading indication for liver transplant in U.S.
• 10-46% prevalence in US
• 3-5% biopsy proven prevalence of NASH
• Prevalence is increasing
• 1.2% 9.7% increase as indication for OLT from 01-09
• Age 40-50
• Hispanics > Caucasians > AA
• Associated disorders
• Obesity
• HTN
• Hyperlipidemia
• Insulin resistance/diabetes
11
CLINICAL MANIFESTATIONS
• Most are asymptomatic
• Fatigue, malaise, Identified by routine LFT’s, imaging tests
• RUQ pain
• PE: obesity, hepatomegaly
• Labs: mild/moderate AST/ALT elevations with ratio <1
• 2-5x ULN
• Degree of elevation does not predict degree of inflammation or fibrosis
• Normal ALT does not exclude clinically significant injury
• Increased ferritin, transferrin, ANA, ASMA
The previous patient undergoes a liver biopsy. Pathology shows Grade ¾ hepatitis and Stage III fibrosis. What is the most likely cause of death in this patient
A. Esophageal variceal hemorrhage
B. Hepatocellular carcinoma
C. Coronary artery disease
D. Hepatorenal syndrome
E. Motor vehicle accident

12
NATURAL HISTORY
• Cardiovascular disease is the most likely cause of death among patients with NAFLD
• Increased mortality in those with fibrosis almost exclusively due to CV disease
• NASH increases risk of liver-related death
• Risk factors for fibrosis• Patient related
• ETOH use
• BMI >28
• Diabetes
• Age >50
• Disease related• Inflammation on biopsy
• Ballooning degeneration plus Mallory hyaline or fibrosis on biopsy
• Elevated AST/ALT >2x ULN

13
DIAGNOSIS
• Hepatis steatosis on imaging or biopsy
• Exclusion of significant alcohol consumption
• >21/week in men and >14/week in women
• Exclusion of other causes of steatosis
• HCV, HBV, AIH, HFE, etc
• Absence of coexisting chronic liver disease
• NAFL vs. NASH
• Biopsy
• Evaluate for fibrosis
• NAFLD Fibrosis score
• Biopsy
• Transient Elastography – Fibroscan
• CT, MRI
NASH GUIDELINES
• Evaluating Incidentally Found Steatosis on Imaging
• Does the person have symptoms/signs of liver disease?
• Do they have abnormal LFTs?
• Yes - Evaluate as if they have NAFLD
• No - Assess for metabolic risk factors (e.g., obesity, glucose intolerance, dyslipidemia) and alternate causes for hepatic steatosis (EtOH, meds)
• Liver biopsy is not recommended in these patients

14
DIAGNOSIS
• Who to biopsy
• Unclear diagnosis
• Evidence of cirrhosis
• Patient request – wants to know inflammation or fibrosis present
• Patient is at increased risk of fibrosis
• Stigmata of chronic liver disease
• Splenomegaly
• Cytopenia
• Ferritin >1.5 x ULN – suggests NASH with advanced fibrosis
• Age >45 with obesity or diabetes – increased risk of fibrosis
A 34-year-old woman is recently found to have fatty liver on ultrasound. She is concerned because her father developed cirrhosis due to fatty liver disease. She has a medical history of morbid obesity, diabetes mellitus, hyperlipidemia and hypertension. She would like to know how likely she is to have extensive damage to her liver.
Which is the best predictor of the presence of fibrosis in fatty liver disease?
A. Low soluble cytokeratin 18
B. Elevated ESR
C. NASH activity score (NAS) of 3
D. AST/ALT ratio > 1
E. Spleen-liver attenuation >/= 10 Hounsfield units on CT scan

15
FIBROSIS-4 (FIB-4)
• 4 variables used to predict advanced fibrosis (F3 and above)
• <1.45 NPV of 90% for advanced fibrosis
• >3.25 97% specificity and PPV of 65%
• In initial study 70% of patients had values <1.45 or >3.25 and could have avoided liver biopsy with 86% accuracy.
VIBRATION CONTROLLED TRANSIENT ELASTOGRAPHY - FIBROSCAN
• Non-invasive measure of fibrosis and steatosis
• 87% sensitive and 91% specific in diagnosis cirrhosis
• Can be useful over time to trend steatosis

16
NASH GUIDELINES - NON-INVASIVE METHODS TO DETECT NASH
• Transient Elastography for Liver Stiffness (FibroScan)
• Measures velocity of a low-frequency shear wave going through the liver
• Stiffer the tissue, faster the shear wave
• Results are expressed in kPa (nl 5.5)
• Pros:
• Short procedure time (<5 min)
• Done at bedside
• Immediate results
• In NAFLD population, higher rate of failure and unreliable results
• Failure to obtain any measurement in 4% with unreliable results in 16%
• Worse with high BMI (>28)
• XL probe made these patients
• Failure significantly as compared to standard M probe (1.1% vs 16%; P <0.00005)
A 62 year old man with NAFLD is seeing you for evaluation. She has a PMH of diabetes mellitus (A1C 8.2), HTN, hyperlipidemia. BMI is 35 kg/m2. She was recently started in insulin therapy for her diabetes. Labs show an AST of 42 and ALT 90. CBC is normal. Liver biopsy is performed, showing grade 3 steatohepatitis and stage III/IV fibrosis.
Which of the following is the best approach to management in this patient.
A. Pioglitazone
B. Weight loss
C. Obeticholic acid
D. Vitamin E
E. Metformin
17
MANAGEMENT
• General measures
• Abstain from alcohol – some evidence to suggest that no amount of alcohol is “safe”
• Immunizations
• Modify risk factors for CV disease
• Weight loss
• >3-5% loss can lead to improvement in steatosis, normalization of LFT’s. Further weight loss recommended if this does not happen
• Bariatric surgery
BARIATRIC SURGERY
• Effective for weight loss and reducing death due to cancer and cardiovascular disease
• Safe in patients with NAFLD/NASH
• Not sufficient evidence to support bariatric surgery as a primary treatment option for NASH/NAFLD
• Patients with NASH/cryptogenic cirrhosis can be considered for bariatric surgery on case-by-case basis at an experienced bariatric center.
• Nationwide inpatient sample 1998-2007 – mortality 0.9% in compensated cirrhosis (0.3% without cirrhosis) and 16.3% in decompensated cirrhosis.
• More recent systematic review - Child’s A – 1.6% early and 2.45% late mortality associated with surgery. 0% mortality in 41 patients who underwent sleeve gastrectomy.
18
PHARMACOLOGIC THERAPY –NO FDA APPROVED TREATMENTS FOR NASH
• In general, NASH should be proven by biopsy prior to pharmacologic treatment
• Vitamin E• Biopsy-proven NASH and fibrosis stage >2
and non-diabetic – 800iu daily
• Contraindicated in males with personal or strong FH prostate CA
• Pro – decrease LFT’s, improve steatosis, inflammation (no effect on fibrosis)
• Con – increase all-cause mortality, hemorrhagic stroke, prostate CA
• 800 IU/day
• Pioglitazone• NASH and diabetes
• Considered as second line after metformin
• Weight gain, heart failure, fractures
• Liraglutide• Small study showed improvement in
inflammation and progression of fibrosis
• Clinical trials• Obeticholic acid – clinically significant
decrease in fibrosis
NAFLD SUMMARY
• NAFLD is becoming an increasingly common etiology of advanced liver disease in the US
• The #1 cause of death in patients with NAFLD is related to cardiovascular disease
• Weight loss is the #1 treatment for NAFLD
• New pharmacologic therapy is expected in the next few years.





























