Embed Size (px)
Citation preview
Bruce Rosen Ronni Gamzu
Myers-JDC-Brookdale Institute Israel Ministry of Health
Phase 1: confusion
PRIVATE
PRIVATE
PUBLIC
DELIVERY
FINANCE
FINANCE
PUBLIC
DELIVERY
Phase 2: separation
The public-private mix in financing
The public-private mix in delivery
Key directions along which the literature in the field developed
Finer gradations on the finance side
Finer gradations on the delivery side
Identification of additional dimensions of the public-private mix
But no change with regard to the separation issue…
The public-private mix in financing
The public-private mix in delivery
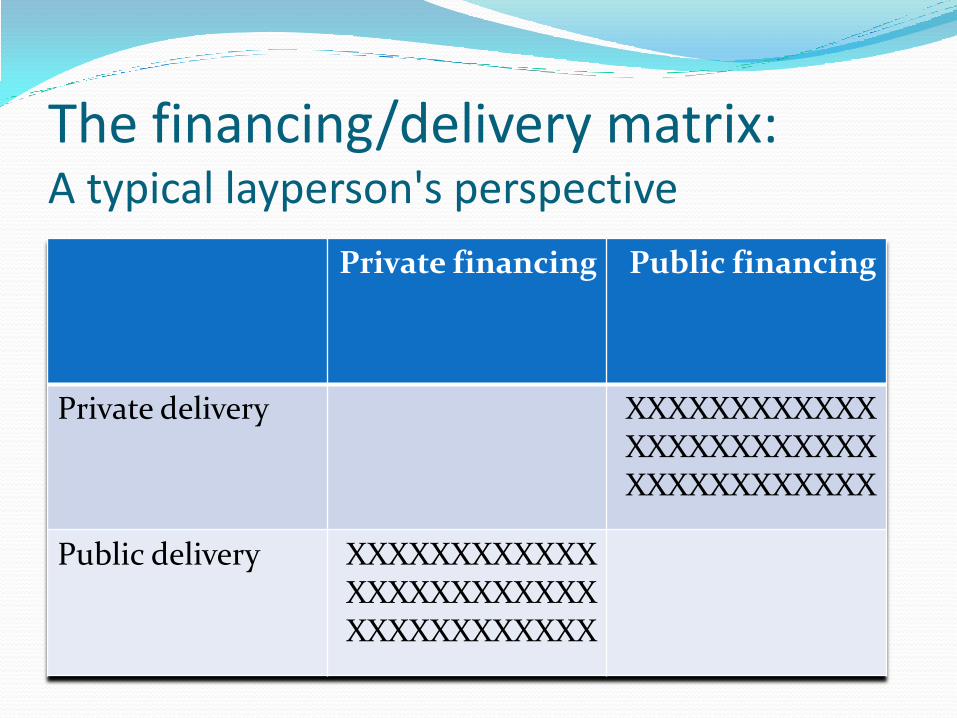
The financing/delivery matrix: A typical layperson's perspective
Private financing Public financing
Private delivery XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
Public delivery XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
The financing/delivery matrix: Scholars' point that all options are open
Private financing Public financing
Private delivery
Public delivery
The financing/delivery matrix: An historically significant policy position
Private financing Public financing
Private delivery ******
Public delivery
Has the time come for phase 3, reflecting a more sophisticated and more integrated approach?
Three reasons to develop a more integrated approach
Iterative relationship between finance and delivery
Common causes (alongside distinct causes)
Common effects (alongside distinct effects)

The Israeli case

What do we usually include in "private financing" in the Israeli context?
Supplemental insurance
Commercial insurance
Out-of-pocket payments Note: Some "private financing" goes for the types of services included in NHI, and some for other types of services
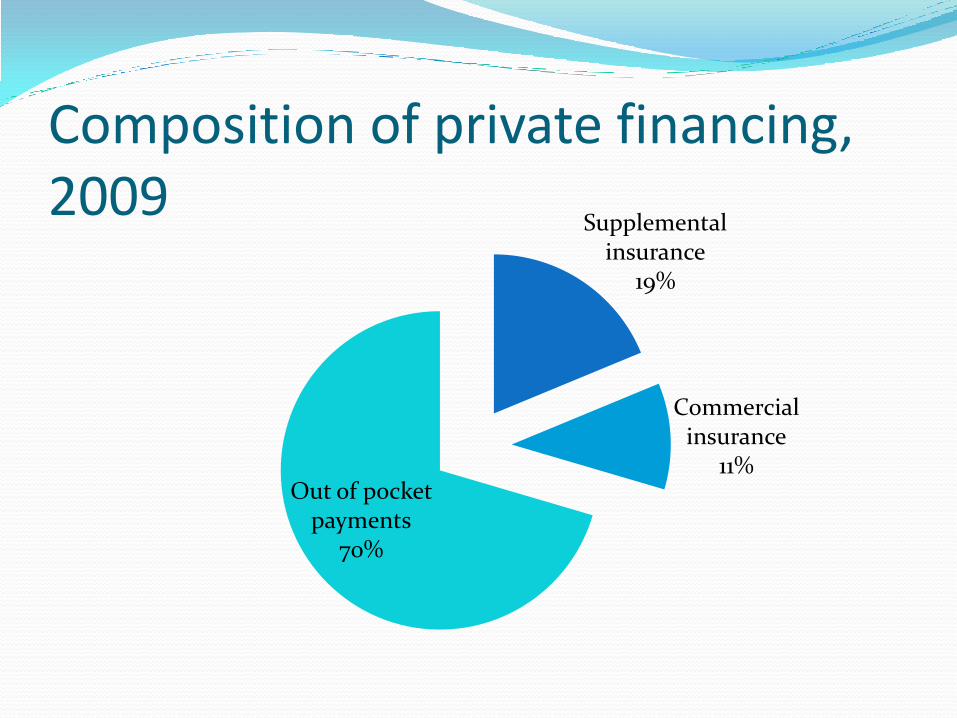
Composition of private financing, 2009
Supplemental insurance
19%
Commercial insurance
11% Out of pocket
payments 70%
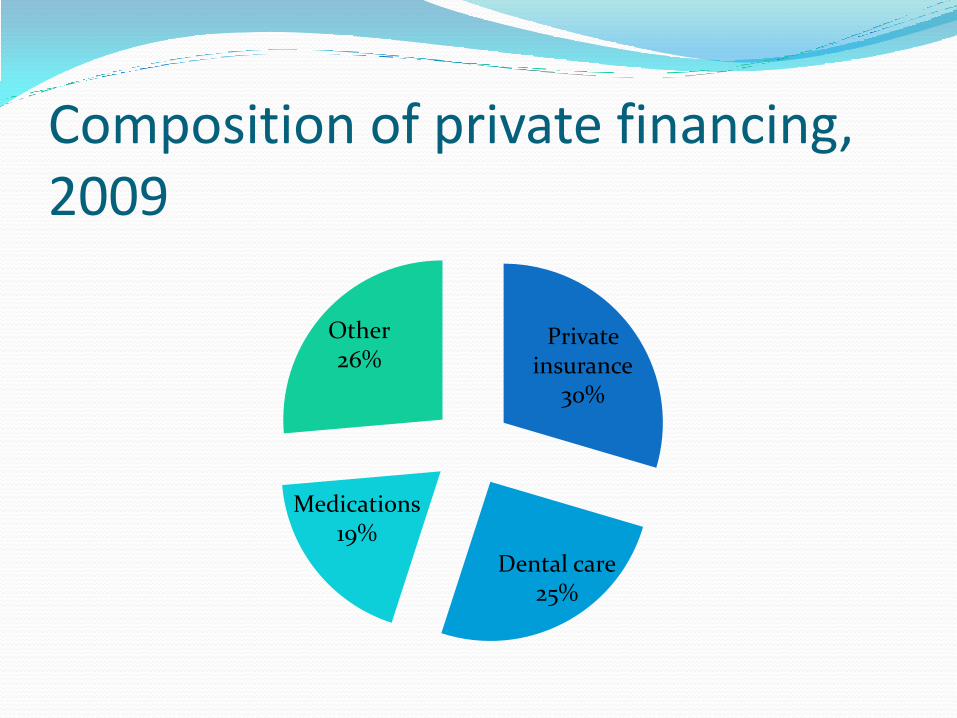
Composition of private financing, 2009
Private insurance
30%
Dental care 25%
Medications 19%
Other 26%
Key facts regarding the growth in private financing in Israel since 1995 1. Major growth in the private share of total financing
(from 30% in 1995 to 42% in 2009)
2. Private per capita spending grew rapidly while public per capita spending was relatively stable
3. Growth in share of health in household expenditures (from 3.8% in 1997 to 5.1% in 2009)
4. Major growth in per capita spending on private insurance (Increase of 280% between 1997 and 2008)
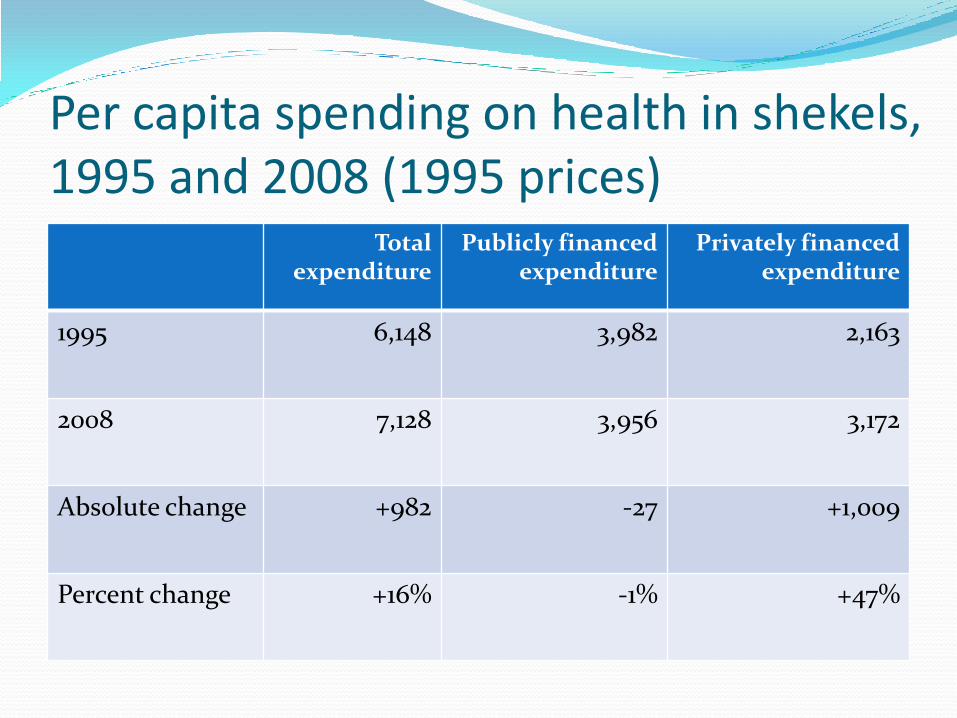
Per capita spending on health in shekels, 1995 and 2008 (1995 prices)
Total expenditure
Publicly financed expenditure
Privately financed expenditure
1995 6,148 3,982 2,163
2008 7,128 3,956 3,172
Absolute change +982 -27 +1,009
Percent change +16% -1% +47%
What do we usually include in "private delivery" in the Israeli context?
For-profit hospitals (but not voluntary hospitals) and other for-profit institutions
Services of physicians and other professionals that are provided "outside" of public frameworks
Other for-profit services and providers
Note: Some "private delivery" is for the types of services included in NHI, and some for other types of services
Key facts regarding the growth in private delivery in Israel since 1995 1. Share of for-profit producers in National Health
Expenditures up from 24% in 2004 to 28% in 2009
2. Major growth in private medical services in Jerusalem's public hospitals; categorization issue
3. Major growth in the number of operations in for-profit hospitals
4. Public hospitals and health plans increasing involved in for-profit ventures
In comparison with financing, apparently less change and harder to monitor

The financing/delivery matrix (2010; in NIS billions)
Private financing
Public financing
Total
Private delivery
?? ?? 17.1 (28%)
Public delivery
?? ?? 44.1 (72%)
Total
23.4 (38%)
37.8 (62%)
61.2 (100%)
Is there an iterative relationship?
Growth of private
financing
Growth of private delivery

How growth in private financing might contribute to growth in private delivery
Private insurers more willing than health plans to pay the high rates demanded by private providers
Private insurers might cast aspersions on the quality of public providers
Private insurance coverage of expensive privately provided services makes them more affordable to the middle class
How growth in private delivery might contribute to growth in private financing
When for-profit provision becomes more available, visible and normative, households have a greater incentive to purchase private insurance packages
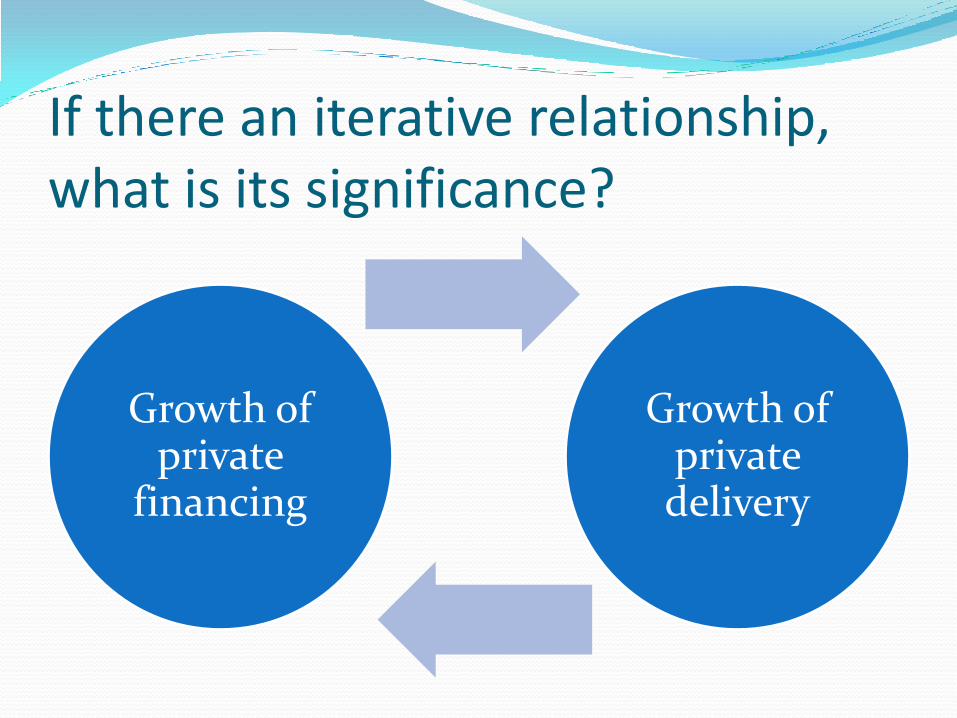
If there an iterative relationship, what is its significance?
Growth of private
financing
Growth of private delivery
Why might we care about the growth in private financing? Equity:
Unequal access to important services Possibility of reduced access to important services
Increased prices and demands for publicly financed services
Erosion of public support for public financing - Less need - Less confidence
Diversion of resources to uses that contribute relatively little to population health
Possible contributor to growth in private delivery
Why might we care about the growth in private delivery?
Drawing away scare manpower from public providers
Cream-skimming: Focusing on profitable services, regions and population groups
Erosion of confidence in public providers
Possible contributor to growth in private financing
But important not to forget:
1. Private financing and private delivery can also provide important advantages
2. The slowdown in economic growth may make privatization more attractive
3. The key question is not whether there should be private elements, but rather what should be their scope and nature
Issues for further consideration How much do private financing (PF) and private provision (PP)
influence one another and what other influences are important?
How much does PF trouble us and why? How much does PP trouble us and why? Of the two, which is the more troubling?
Empirically, what really are the impacts of PF and PP?
If we want to constrain PF, what are the best ways to do so?
If we want to constrain PP, what are the best ways to do so?

Issues for further consideration: Complementary formulation
How much do private financing (PF) and private provision (PP) influence one another and what other influences are important?
How much does PF attract us and why? How much does PP attract us and why? Of the two, which is the more attractive?
Empirically, what really are the impacts of PF and PP?
If we want to expand PF, what are the best ways to do so?
If we want to expand PP, what are the best ways to do so?
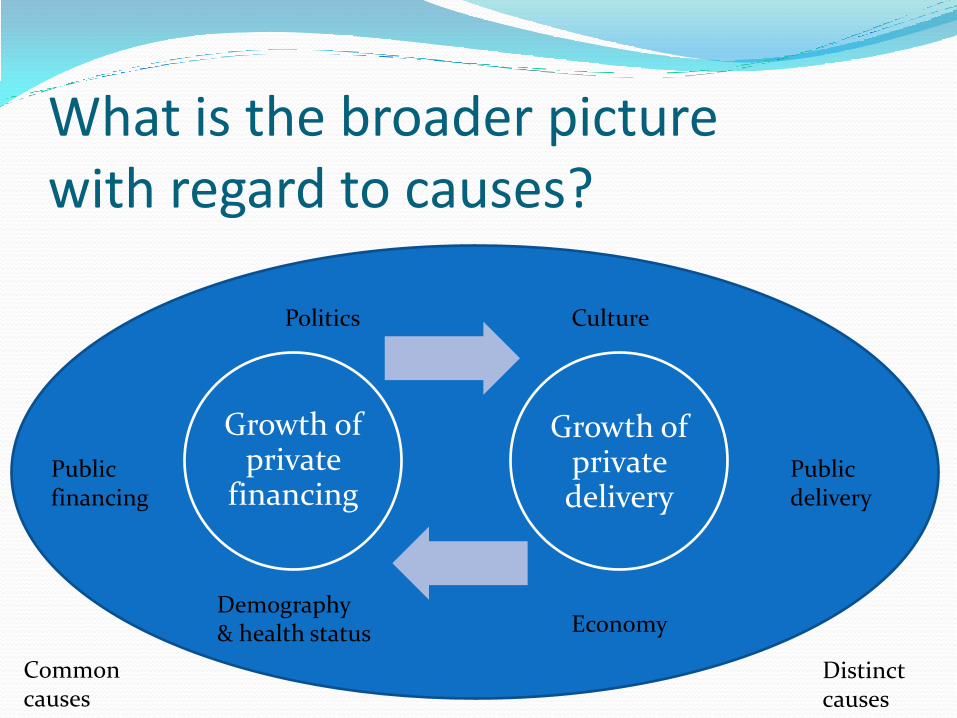
What is the broader picture with regard to causes?
Growth of private
financing
Growth of private delivery
Public delivery
Public financing
Demography & health status Economy
Culture Politics
Common causes
Distinct causes
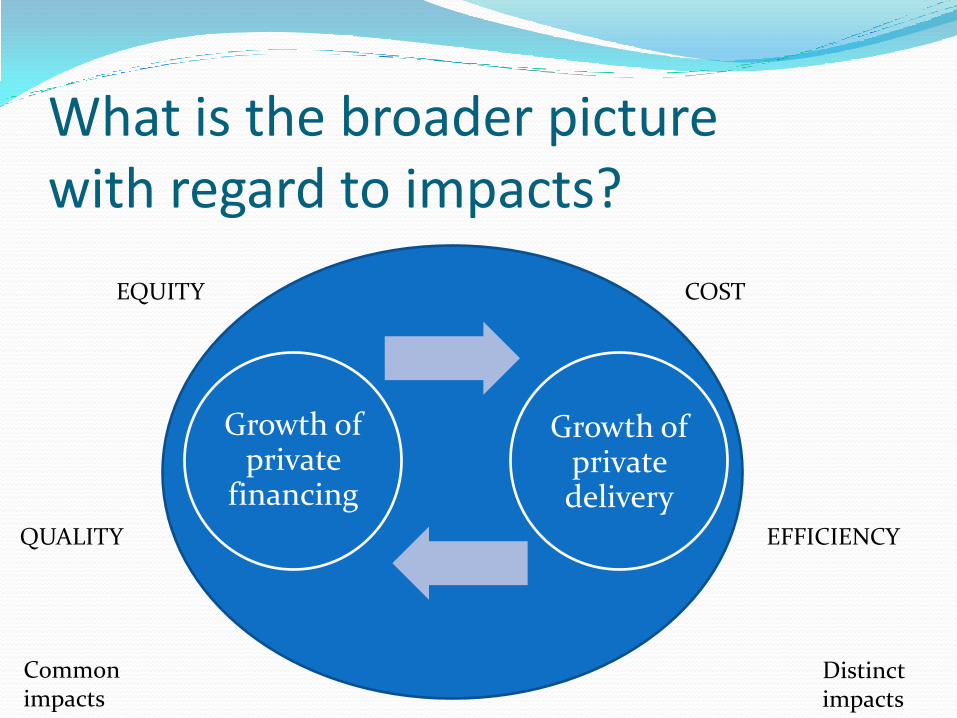
What is the broader picture with regard to impacts?
Growth of private
financing
Growth of private delivery
QUALITY EFFICIENCY
COST EQUITY
Common impacts
Distinct impacts
Summary: A more integrated, phase 3 approach is needed for at least three reasons
1. Iterative, synergistic effects
2. Common causes
3. Common effects And perhaps also common interventions….

Bruce Rosen Ronni Gamzu
Myers-JDC-Brookdale Institute Israel Ministry of Health

The Democracy Index: Five distinct, but related components
1. Electoral process and pluralism
2. Civil liberties
3. Functioning of government
4. Political participation
5. Political culture
If there an iterative relationship, what is its significance?
Growth of private
financing
Growth of private delivery





























