Embed Size (px)
DESCRIPTION
pulmo
Citation preview



BRONCHIECTASIS(brong-kee-ECK-tah-sis)
PRASENOHADI
Department of Pulmonolgy and Respiratory MedicineFaculty of Medicine, University of Indonesia

BRONKIEKTASIS = BE Proses patologi yang ditandai dengan dilatasi ireversibel dan destruksi dinding bronkus
SEJARAH
1819 René Théophile Hyacinthe Laënnec “suppurative phlegm” 1922 Jean Athanase Sicard bronkografi kontras kerusakan 1950 Lynne Reid bronkografi, patologi, prevelensi (imunisasi)
PRASS, ACEH 2005

PATOFISIOLOGIBronkiektasis (BE) penyakit bronkus dan bronkiolus infeksi dan inflamasi disertai pelepasan mediator mengakibatkan obstruksi dan kerusakan saluran napas serta infeksi berulang
PRASS, ACEH 2005
Perubahan respons selular dan mediator infiltrasi netrofil dan limfosit T peningkatan elastase dan kemoatraktan, interleukin–8, interleukin–1β, tumor necrosis factor–α (TNF–α) dan prostanoid (leukotrien B4) endotelin–1 meningkatkan CD18 dan CB11b ?desmosin dan isodesmosin urin nitrit oksida, hidrogen peroksidase, karbon monoksida

kolonisasi kumanjumlah kuman
host (pasien)respons inflamasi
gangguanbersihan bronkus
kerusakan paru
THE “VICIOUS CIRCLE” HYPOTHESIS
PRASS, ACEH 2005

TOTAL DIFFERENTIAL CELL COUNTS AND CYTOKINELEVELS IN BALF OF PATIENTS WITH BRONCHIECTASIS
AND CONTROL SUBJECTS
Am J Respir Crit Care Med 2001

Relationship betweenairway bacterial load(cfu/ml) and the % ofneutrophils andTNF–α, IL–1, IL–8concentrations inBALF
Am J Respir Crit Care Med2001

COMPARISON OF BRONCHIAL AND SYSTEMICINFLAMMATORY RESPONSE IN PATIENTS WITH
BRONCHIECTASIS
Am J Respir Crit Care Med 2001
GAMBARAN FOKAL DAN DIFUS
BE dapat dibagi menjadi 2 bentuk Proses lokal atau fokal obstruksi di lobus atau segmen Proses luas pada kedua paru dan sering berhubungan sinusitis and asthma
3 jenis sumbatan jalan napas fokal BE 1. Sumbatan benda asing (broncholith) atau tumor yang yang tumbuh lambat (biasanya jinak) 2. Sumbatan dari luar oleh pembesaran kelenjar getah bening middle lobe syndrome mikobakterium
jamur 3. Sumbatan pasca bedah
PRASS, ACEH 2005

PATOLOGI/PATOGENESISUtama dilatasi jalan napas di paru 3 bentuk dilatasi jalan napas silindrik varikosa sakular
Dilatasi bronkus Inflamasi
Kerusakan jalan napas
Gangguan mukosiliar
Gangguan bersihanJalan napas
PRASS, ACEH 2005

3 mekanisme utama terlibat pada kerusakanjaringan bronkus :
Infeksi dan inflamasi Kemoatraktan sel inflamasi (netrofil, makrofag) bahan sitotoksik kerusakan dinding bronkus / silia
Obstruksi jalan napas dan gangguan silia Gangguan silia sumbatan mukus dan infeksi
Fibrosis peribronkial Lisis jaringan elastis dinding bronkus penebalan
fibrosis
PATOLOGI/PATOGENESIS
PRASS, ACEH 2005

Normal Bronchiectasis
A Scanning ElectronMicrograph of the Surfaceof Human BronchusShowing Dense Ciliation

Outer armInner arm
Nexin link
Radial spoke
Cell membrane
Dynein arm
Absence of outer dynein arm
Normal
Bronchiectasis

CONDITIONS ASSOCIATED WITHBRONCHIECTASIS
Pasca infeksiBakteri (pseudomonas, haemophilus)Mycobacterium tuberculosisAspergillus speciesVirus (adenovirus, measles virus, influenzavirus, human immunodeficiency virus)
Kongenital (Bawaan)Primary ciliary dyskinesiaAlpha 1–antitrypsin deficiencyCystic fibrosisTracheobronchomegaly (Mounier–Kuhn syndrome)Cartilage deficiency (Williams–Campbell syndrome)Pulmonary sequestrationMarfan’s syndrome
ImunodefisiensiPrimer
HypogammaglobulinemiaSekunder
Kanker (chronic lymphatic leukemia),kemoterapi, or imunomodulator(pasca transplantasi)
Sequelae of toxic inhalation or aspirationChlorineOverdose (heroin)Foreign body
CONDITIONS ASSOCIATED WITHBRONCHIECTASIS
PRASS, ACEH 2005

CONDITIONS ASSOCIATED WITHBRONCHIECTASIS
Rematik Rheumatoid arthritisSystemic lupus erythematosusSjögren’s syndromeRelapsing polychondritis
Lain–lain Inflammatory bowel disease(chronic ulcerative colitis or Crohn’s disease)Young’s syndrome (secondary ciliary dyskinesia)Yellow nail syndrome (yellow nails and lymphedema)
PRASS, ACEH 2005

PRASS, ACEH 2005
GEJALA DAN TEMUAN KLINIK
Umumnya : batuk dan produksi sputum kronikSputum : mukoid, mukopurulen, kental, tenaciousKerusakan saluran napas akibat infeksi akut Blood–streaked atau hemoptisis Sesak napas (dyspnea) dan mengi (wheezing) : 75% pasienNyeri dada (pleuritic chest pain) : 50% pasien
Pemeriksaan fisis ditemukan suara napas tambahanbronkial (70% pasien), mengi (34%) and ronki (44%)Jari tabuh (digital clubbing) kadang–kadang (3%)
Diagnosis banding PPOK

GEJALA EKSASERBASI AKUTBRONKIEKTASIS
Perubahan produksi sputum Sesak napas (dyspnea) meningkat Batuk meningkat Demam (suhu, >38.0°C) Mengi (wheezing) meningkat Malaise, fatigue, lethargy, atau
penurunan kegiatan Faal paru menurun Radiographic changes consistent with
a new pulmonary process Perubahan suara napas
PRASS, ACEH 2005

PERBEDAAN BRONKIEKTASIS (BE) DANPENYAKIT PARU OBSTRUKTIF KRONIK (PPOK)
PRASS, ACEH 2005
VARIABEL PPOK BE
Penyebab Rokok Infeksi, genetik atau gangguan imun
Peran infeksi Sekunder Primer Organisme sputum Streptococcus H. influenzae,
pneumoniae, PseudomonasHaemophilus aeruginosa
influenzae Obstruksi jalan napas Ada Ada dan hiperesponsif Radiologi Hiperlusen, hiperinflasi, Dilatasi, penebalan,
dilatasi “mucous plugs” Sputum (stabil) Mukoid Purulen, tiga–lapis
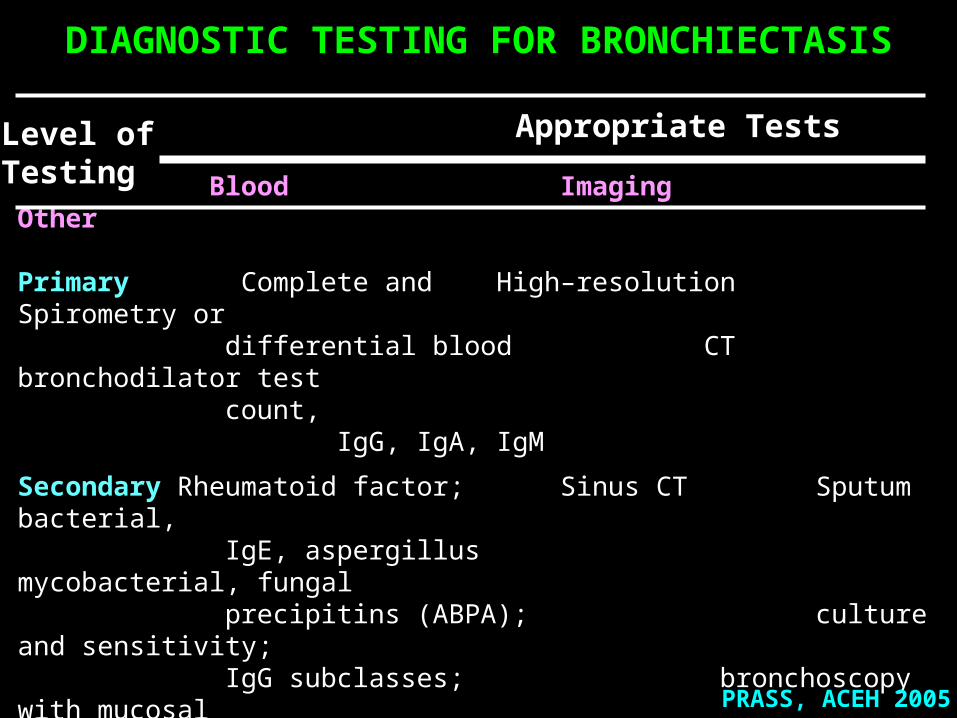
DIAGNOSTIC TESTING FOR BRONCHIECTASIS
Appropriate Tests
Blood Imaging Other
Primary Complete and High–resolution Spirometry or differential blood CT bronchodilator test count,
IgG, IgA, IgM
Secondary Rheumatoid factor; Sinus CT Sputum bacterial, IgE, aspergillus mycobacterial, fungal precipitins (ABPA); culture and sensitivity; IgG subclasses; bronchoscopy with
mucosal alpha1-antitrypsin level biopsy, cultures (for focal obstruction, infection, primary ciliary dyskinesia);
(for sweat chloride test analysis cystic fibrosis)
Level ofTesting
PRASS, ACEH 2005

Paru normal Bronkiektasis

A PA radiograph shows extensive increase in linearopacities particularly in the lower lobes suggestive of
ectatic bronchi
PRASS, ACEH 2005

Cylindrical bronchiectasis withsignet-ring appearance.Note that the luminal airwaydiameter is greater than the diameter of the adjacent vessel
Cystic and cylindricalbronchiectasis of the right lowerlobe on a posterior-anteriorchest radiograph
PRASS, ACEH 2005


PRASS, ACEH 2005
Findings:• normal upper and middle lobes• the branches to the lower lobe are slightly dilated and there is a lack of branch filling

The repeated episodes of inflammation can result in scarring,which has resulted in fibrous adhesions between the lobes.Fibrous pleural adhesions are common in persons who havehad past episodes of inflammation of the lung that involve the pleura.With extensive involvement, the pleural space may be obliterated.

PRASS, ACEH 2005

PRASS, ACEH 2005
FAAL PARU
- Penurunan rasio volume ekspirasi paksa detik 1 (VEP1) terhadap kapasiti vital paksa (KVP) - Normal atau penurunan KVP - Penurunan VEP1
Penurunan KVP hambatan aliran udara mukus, atelektasis, pneumonitis paru
Merokok memperburuk faal paru gangguan obstruksi
Hiperesponsif jalan napas 40% pasien

CLINICAL CHARACTERISTICS AND SPIROMETRICVALUES OF PATIENTS WITH BRONCHIECTASIS AND
CONTROL SUBJECTS
Am J Respir Crit Care Med 2001

Lung function, Medical Research Council (MRC),five–point flow limitation (FL), high–resolution computed
tomography (HRCT) score and maximal power output (WRmax)in bronchiectatic patients colonised (PA) and not colonised
(non-PA) with Pseudomonas aeruginosa
Eur Respir J 2003 = significant

PENATALAKSANAAN
PRASS, ACEH 2005
ANTIBIOTIKA eksaserbasi akut
Mucociliary stimulants meningkatkan bersihan
MUKOLITIK kurang efektif
STEROID eksaserbasi akut, kontrofersi
BRONKODILATOR hiperesponsif jalan napas
PEMBEDAHAN
“Airway clearance therapy” pencegahan intervensi dini

PROGNOSIS
PRASS, ACEH 2005
Keistinen et al. (National Hospital Discharge Register) di Finland mengidentifikasi 842 pasien BE usia 35 – 74 tahun antara1982 s/d 1986 dan membandingkan dengan pasien asma dan PPOK
Selama 8.0–12.9 tahun hingga akhir 1993, jumlah pasien BE yang dirawat bervariasi (range, 1 – 51; rerata, 2.2)
239 kematian pasien BE (28%), 165 kematian pasien asma (20%) dan 319 kematian pasien PPOK (38%).

PRASS, ACEH 2005
References : 1. Angrill J, Agustí C, Torres A. Bronchiectasis. Curr Opinion Infect Dis 2001; 14: 193–7. 2. Barker AF. Bronchiectasis. N Eng J Med 2002; 346: 1383–93. 3. Tsang KWT, Zheng L, Tipoe G. Cilliary assessment in bronchiectasis. Respirologi 2000; 5: 91–8. 4. Angrill J, Agustì C, De Celis R, Filella X, Raňó A, Elena M, De La Bellacasa JP, Xaubet A, Torres A. Bronchial inflammation and colonization in patients with clinically stable bronchiectasis. Am J Respir Crit Care Med 2001; 164: 1628–32. 5. Koulouris NG, Retsou S, Kosmas E, Dimakou K, Malagari K, Mantzikopoulos G, Koutsoukou A, Milic-Emili J, Jordanoglou J. Tidal expiratory flow limitation, dyspnoea and exercise capacity in patients with bilateral bronchiectasis. Eur Respir J 2003; 21: 743–8. 6. Greenstone M. Changing paradigms in the diagnosis and management of bronchiectasis. Am J Respir Med 2002; 1: 339–47. 7. Braverman JM. Airway clearance indications in bronchiectasis: An overview. Advanced Respiratory.

IDIOPATHICPULMONARY FIBROSIS
( IPF )
PRASENOHADI
Department of Pulmonolgy and Respiratory MedicineFaculty of Medicine, University of Indonesia

Terbanyak pada “idiopathic interstitial pneumonias”
Tidak respons terhadap pengobatan
= “cryptogenic fibrosing alveolitis”= “chronic fibrosing interstitial pneumonia”
Penyebab tidak diketahui
IPF termasuk dalam “idiopathic interstitial pneumonias”
IDIOPATHIC PULMONARY FIBROSIS
PRASS, ACEH 2005

Prevalensi 1.5–1.8 per 10 000 orang pertahun
Insidens 0.5 per 10 000 orang pertahun
Prevalensi laki–laki : perempuan = 1.4:1.0
Insidens rasio laki–laki : perempuan = 1.3:1.0
Usia 40–70 tahun, kebanyakan diatas 60 tahun
Survival (setelah diagnosis) 3.2–5 tahun
EPIDEMIOLOGI
PRASS, ACEH 2005

ETIOLOGICigarette smokingSeveral occupational factors (farming, hairdressing,
stonecutting, and exposure to livestock, birds,and dust from metals and vegetables)
Viral proteins and antibodies (Epstein–Barr virus,influenza A virus, hepatitis C virus,parainfluenza viruses 1 and 3, HIV-1, herpesvirus 6)
Genetic predisposition to IPF Familial IPF autosomal dominant Inherited abnormalities in surfactant proteins interleukin-1 (IL-1) receptor antagonist, polymorphism of the tumour necrosis factor–α complement receptor 1
PRASS, ACEH 2005

PATOGENESIS (1)
Initial injury recruitment of inflammatory cells release of cytokines and eventually,
increased fibroblast activity,parenchymal remodelling and fibrosis.
Alveolar epithelial cells transforming growth factor–β1 (TGF–β1) platelet-derived growth factor (PDGF) tumour necrosis factor α (TNFα) interleukin–1 (IL–1) insulin–like growth factor 1 (IGF1) basic fibroblast growth factor (bFGF)
PRASS, ACEH 2005

Release of cytokines fibroblast proliferation migration to various sites in the lung differentiation of the fibroblast phenotype
First, differentiated cell to be more resistant to apoptosis (natural cell death) repair of tissue without excessive scarring
Second, the altered cells responsiveness tofibrogenic cytokines (TGF-beta, bFGF)
PATOGENESIS (2)
PRASS, ACEH 2005

Immunological pathogenesis of IPF
Type 2 T–cell response predominates,
Increase IL–4 and IL–13
Elevated circulating autoantibodies antinuclear antibodies, anti–DNA antibodies, anti–cytokeratin 8 antibodies immune complexes
PATOGENESIS (3)
PRASS, ACEH 2005
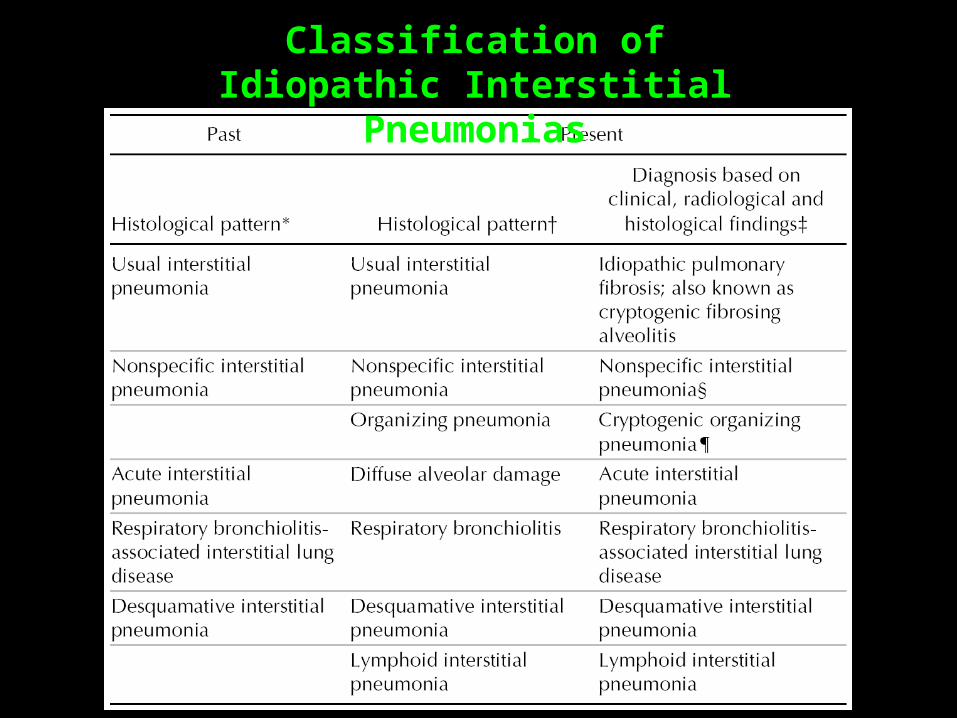
Classification ofIdiopathic Interstitial Pneumonias

GAMBARAN KLINIS Umumnya batuk dengan produksi sputum minimal
Sesak napas (dispnea) progresif dalam 3–4 bulan
Jari tabuh (clubbing finger)
Auskultasi ronki halus (tengah – akhir inspirasi)
Tekanan jantung kanan meningkat Gagal jantung kanan
Diagnostik :anamnesis, pemeriksaan fisis, radiologi,pemeriksaan faal paru, serologi, histopatologi
PRASS, ACEH 2005

• Unclear diagnosis• Age < 50 yr• Systemic complaints• Radiological features atypical of idiopathic
pulmonary fibrosis• Rapid progression of disease• Normal chest radiograph• Recurrent pneumothorax• Benefit of correct diagnosis outweighs the risk of
surgery• Detection of a fibrotic process related to an exposure
that may be important for compensation purposesfor the patient
Suggested Indications for Surgical Biopsyin Patients with Diffuse Interstitial Lung Disease
PRASS, ACEH 2005

Major criteria Exclusion of known causes of interstitial lung disease, such as drug toxicity, exposure to environmental respiratory hazards and the presence of connective tissue disease Evidence of restrictive lung disease such as reduced vital capacity, impaired gas exchange with an increased alveolar– arterial oxygen gradient, decrease in partial arterial pressure of O2 at rest or during exercise, decreased CO gas transfer High–resolution CT showing bibasilar reticulonodular opacities with minimal or no ground-glass appearance A transbronchial biopsy or bronchoalveolar lavage findings that would not support other diagnosis such as sarcoidosis, hypersensitivity pneumonitis, malignant disease, infection, cryptogenic organizing pneumonia or pulmonary alveolar proteinosis
Major and Minor Criteria for the Diagnosis of IPF in the Absence of a Surgical Lung Biopsy (1)
PRASS, ACEH 2005

Major and Minor Criteria for the Diagnosis of IPF in the Absence of a Surgical Lung Biopsy (2)
Minor criteria Age > 50 yr Insidious onset of dyspnea with no discernible cause Duration of symptoms > 3 mo Bilateral inspiratory crackles
Diagnosis requires : all 4 major criteria 3 of the 4 minor criteria
PRASS, ACEH 2005

HISTOPATOLOGI
Bagian paru yang dipisahkan lung saat otopsi pasien denganIPF menunjukkan kista sarang tawon(honeycomb cysts)

HISTOPATOLOGI
Tampak gambaran kista sarang tawon
HISTOPATOLOGI
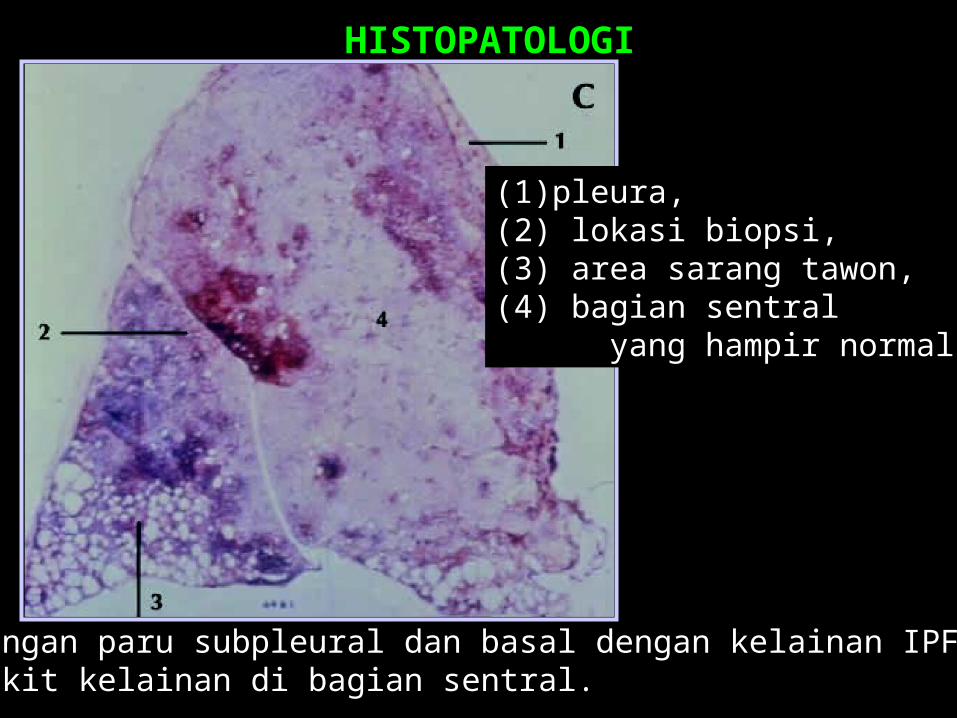
Potongan paru subpleural dan basal dengan kelainan IPF dansedikit kelainan di bagian sentral.
(1) pleura,(2) lokasi biopsi,(3) area sarang tawon,(4) bagian sentral yang hampir normal

HISTOPATOLOGI
Jaringan paru normal (N), fokus fibroblas (panah) dan
fibrosis interstisial ()

Fibrosis subpleura, kista sarang tawon, bronkiektasis (panah besar) danfibrosis paraseptal (panah kecil) dan perubahan minimal di paru tengah
Gambaran Radiologi IPF dengan high–resolution CT

Pharmacotherapy immunosuppressive agents
antifibrotic agents
Nonpharmacologic
PENATALAKSANAAN (1)
PRASS, ACEH 2005

Single/combined immunosuppressive agentCorticosteroids (standard therapy)
survival ?, side effects and complications
Prednisone (20 mg/d) Azathioprine (3 mg/kg daily, not to exceed 200 mg/d) stabilize lung function monitored for hepatotoxic effects, renal dysfunction and bone marrow suppression osteoporosis prevention with vitamin D and calcium supplementation and bisphosphonates
PENATALAKSANAAN (2)Terapi Imunosupresif
PRASS, ACEH 2005

PENATALAKSANAAN (3)Terapi Antifibrotik
Collagen synthesis (clinical trials) pirfenidone interferon gamma–1b interferon beta–1a colchicine penicillamine
SURVIVAL ?
PRASS, ACEH 2005

PRASS, ACEH 2005
Examples of anti-inflammatory and antifibrotic agents as potential therapeutic options for the treatment of IPF

PENATALAKSANAAN (4)Nonpharmacological treatment
Fitness Good nutrition Oxygen supplementation
Lung transplantation improve survival single lung transplantation reduced
the risk of death by 75% comparedwith patients with IPF on the transplantwaiting list
PRASS, ACEH 2005

IPF adalah penyakit paru interstisial progresif yang tidak diketahui sebabnya dan sulit diobati
Pengobatan yang telah ada perlu dikombinasi dengan obat baru meskipun dalam tahap uji klinik
Pasien IPF membutuhkan penanganan secara klinik spesialistik dan kemungkinan untuk dilakukan transplantasi paru
KESIMPULAN
PRASS, ACEH 2005
































