Embed Size (px)
Citation preview

Bristol Genetics Laboratory 2010
Congenital Central Hypoventilation Syndrome;
a polyalanine repeat disorder- the UK cohort
Sarah Burton-JonesBristol Genetics Laboratory

Bristol Genetics Laboratory 2010
Congenital Central Hypoventilation Syndrome(Formerly called ‘Ondine’s Curse’)
• Autonomic nervous system disorder • Incidence ? 1 in 20000-50000 live births• Diagnosis in infancy / early childhood (NB. can be later onset)
• Characteristic respiratory phenotype
Failure of autonomic control of ventilation
- Same respiratory rate awake and asleep hypoventilation- No automatic response to hypoxia/hypercarbia- ‘Asphyxia’ when awake, without exertion

Congenital Central Hypoventilation Syndrome
More severe phenotype:
• Hirschprung’s Disease - colon aganglionosis
• Neural crest tumours- e.g. neuroblastoma, ganglioneuroma
• Can also present with: cardiac irregularities, dysphagia, eye abnormalities, temperature regulation problems, altered perception of anxiety and pain, and other symptoms
PHOX2B now known as ‘the disease-defining gene for CCHS’
Bristol Genetics Laboratory 2010

Bristol Genetics Laboratory 2010
• Paired-Like Homeobox• 4p12, 3 exons, 314 amino acids• Highly conserved homeodomain transcription factor• 2 polyalanine repeat tracts (9 and 20 Ala)
– Imperfect repeats; can expand by unequal allelic recombination
The PHOX2B Gene
5’ 3’1 2 3
NH2 COOH
PHOX2B structure
PHOX2B transcript
Adapted : Amiel et al. (2003) Nature Genetics 33(4), 459-461
Ala repeats

Bristol Genetics Laboratory 2010
Distribution of PHOX2B Mutations
Figure from Weese-Mayer DE et al (2009) Pediatric Pulmonology 44:521-535
A de novo interstitial 4p12 deletion encompassing the PHOX2B gene has also been reported Benailly HK et al Clin Genet 2003; 64: 204-209.

Pathogenic PHOX2B Variants
FeaturePolyalanine expansion
(+4 to +13 Ala)Frameshift / missense
mutation (NPARM)
Location in PHOX2B 20 alanine tract in exon 3Exon 3 or
end of exon 2 (most)
Proportion of all pathogenic variants
~90% ~10%
Present with Hirschprung’s Disease
<20% >87%
Develop neural crest tumour
~1% (all ≥+11 Ala) ~50% over 1 year old
Parent carries mutation Up to 14% Almost all de novo
Predicted effect on proteinMisfolding, cytoplasmic
aggregate formation, nuclear exclusion
Nuclear sequestration
Bristol Genetics Laboratory 2010
Figures from published data
Bristol Genetics Laboratory 2010
Bristol PHOX2B Service
● Developed as a trainee project at Bristol ● Gene dossier submitted to the UKGTN Steering Group● Approved as a NHS diagnostic service test Feb 2005
Benefits of molecular genetic analysis:– Fast confirmation of diagnosis, aids clinical decision making– Parents can be tested for carrier status– Prenatal diagnosis offered
Diagnostic referrals from:Neonatology, Respiratory Medicine, General Paediatrics,
Neurology, Clinical Genetics.

PHOX2B Testing Strategy; BGL
• All diagnostic requests
• Familial expansion testing
• Exclusion testing
• Strong clinical suspicion of CCHS or LO-CHS
Polyalanine expansion analysis (GC rich PCR)
PHOX2B sequence analysis
At request of referring clinician
Report, request parental samples
Report
+ve -ve
Bristol Genetics Laboratory 2010

Bristol Genetics Laboratory 2010
Polyalanine Expansion Analysis
• All expansions are confirmed by sequencing of PHOX2B exon 3 (fragment B)
Normal control +6 Ala expansion Parent mosaic for +6 Ala

Bristol Genetics Laboratory 2010
CCHS UK Diagnostic Results
PolyAla and sequence analysis, no mutation detected
PolyAla analysis only, no mutation detected
Polyalanine expansion mutation detected
Non-expansion mutation (NPARM) detected
46 (20%)
5 (2%)
159 (69%)
20 (9%)
Bristol Genetics Laboratory 2010
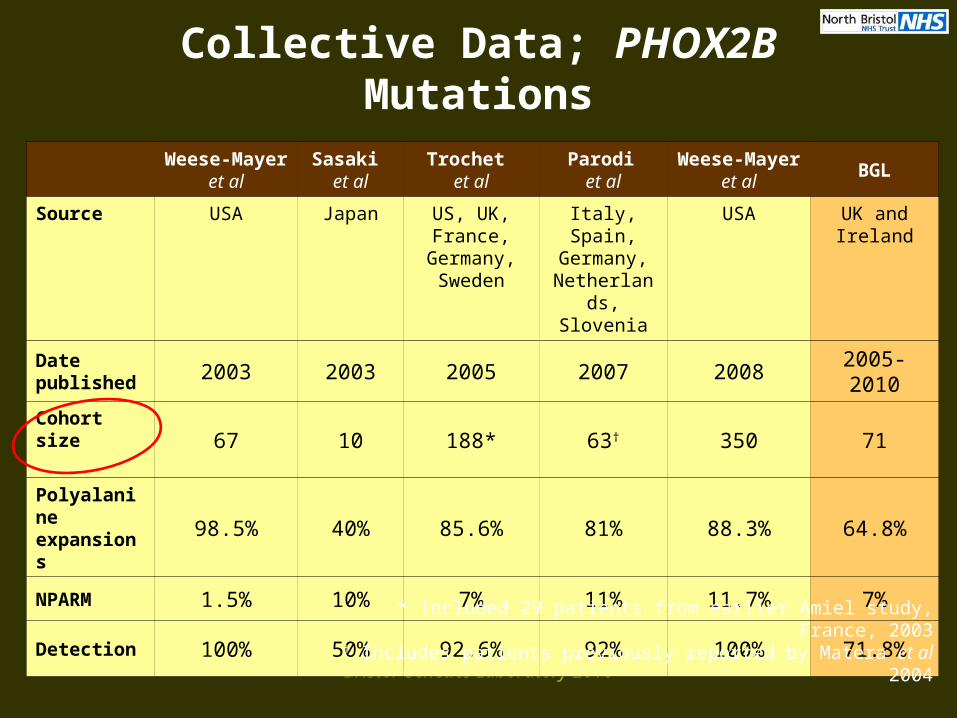
Collective Data; PHOX2B Mutations
Weese-Mayer et al
Sasaki et al
Trochet et al
Parodi et al
Weese-Mayer et al
BGL
Source USA Japan US, UK, France,
Germany, Sweden
Italy, Spain, Germany,
Netherlands, Slovenia
USA UK and Ireland
Date published 2003 2003 2005 2007 2008 2005-2010
Cohort size67 10 188* 63† 350 71
Polyalanine expansions 98.5% 40% 85.6% 81% 88.3% 64.8%
NPARM 1.5% 10% 7% 11% 11.7% 7%
Detection 100% 50% 92.6% 92% 100% 71.8%
* Included 29 patients from earlier Amiel study, France, 2003† Includes patients previously reported by Matera et al 2004

Bristol Genetics Laboratory 2010
BGL CCHS Data in Context
Comparison of PHOX2B global data with UK and Ireland data (BGL)
0%
5%
10%
15%
20%
25%
30%
35%
Cont -
7/-7 +4
+4/+
4 +5 +6 +7 +8 +9 +10
+11
+12
+13
NPARM
PHOX2B mutant allele
% all mutations detected
Weese-Mayerreview2009(n=640)
UK &Ireland(n=51)

Bristol Genetics Laboratory 2010
Parental Studies; Expansion Mutations
• Autosomal dominant, incomplete penetrance– However, majority de novo occurrence
• Possible paternal origin bias Arai et al J Hum Genet (2007) 52:921-925 and (2010) 55:4-7
• Studies indicate 7-14% cases are inherited:
• Carriers who report no symptoms may show respiratory anomalies in sleep studies Parodi et al (2010) Clin Genet (epub ahead of print)
• Somatic mosaicism common• No reports of germinal mosaicism in the literature to date
Publication Parental carrier rate
Weese-Mayer et al (2003) Am J Med Genet 123A:267-268 7.4% (4/54)
Parodi et al (2008) Hum Mutat 29:206 13.9% (6/43)
Trochet et al (2008) Am J Respir Crit Care Med 177:906-911 8.1% (10/124)

Bristol Genetics Laboratory 2010
Polyalanine Expansion Cases; BGL
Expansion size
Number of probands
Neither parent tested or
one tested and normal
Both parents tested or
one tested and positive
Parents positive for expansion
+5 10 6 4 1 Father carrier, affected
+6 15 4 11 2 Fathers mosaic, unaffected
+7 17 5 12
1 Father mosaic, unaffected1 Mother mosaic, unaffected1 Mother carrier, unaffected
(non-penetrant)
+10 1 0 1 -
+11 1 0 1 -
+12 1 0 1 -
+13 1 1 0 -
Total 46 16 30 6 (13% of 46, 20% of 30)

Bristol Genetics Laboratory 2010
Parents of Expansion Cases; BGL
• In 13% all probands, or 20% where we have complete data, the expansion was also detected in a parent.
(Published figures up to 14% with complete data)
• No somatic mosaicism seen in +5 Ala expansion cases, consistent with published data*
• Expansions of ≥ 6 alanines postulated to be fully penetrant*, but note unaffected +7 carrier mother
• New evidence for germinal mosaicism from a UK case...
* Parodi S et al (2008) Hum Mut 29(1) 206

Bristol Genetics Laboratory 2010
UK Germinal Mosaic Case?
• Urgent referral aged 9 days, ventilator dependent• 5-alanine PHOX2B expansion in proband and twin brother• Dizygous twins; fraternity and paternity confirmed by QF-
PCR zygosity analysis (AWMGLS Cardiff)
• Both parents N/N using DNA from peripheral blood• Saliva samples requested• Expansion test sensitivity determined to be 2%
N/N N/N
CCHS,N/+5 Ala
CCHS, N/+5 Ala

Bristol Genetics Laboratory 2010
PHOX2B Mutations (NPARM); BGL
* from Weese-Mayer DE et al (2009) Pediatric Pulmonology 44:521-535
Mutation type
BGL examples
Phenotype Published data*
Frameshift
c.722_759delc.722_759delc.721_739del
c.861dupTc.866dupG
Died 27 days. Ventilated from birth, Hirschprung’s. (OX)
Died 4 weeks. Colon aganglionosis. (NOTTS)
Apnoea. Colon aganglionosis. Treatment withdrawn. (OX)
Died 40 days. Ventilated from birth. Aganglionosis. (BRIS)
Hypotonia, apnoea, Hirschprung’s. Died (cardiac). (BRIS)
78%
Missensep.Ala140Glu
(NB. Non-UK)
Variable; late onset in father, congenital with Hirschprung’s in son (LEIDEN)
19%
Nonsense None to date - 3%

Bristol Genetics Laboratory 2010
Parental Studies; NPARMs
• Rarely reported• Variable penetrance• Single base deletions in exon 3 upstream of poly Ala tract
– c.618delC Matera et al (2004) J Med Genet 41:373-380
– c.577delG Berry-Kravis et al (2006) Am J Respir Crit Care Med 174:1139-1144
• Exon 2 missense substitution– c.422G>A (p.Arg141Gln), 2 families Berry-Kravis et al (2006) as above
• Recent Bristol case referred from Netherlands:– Father presented with late-onset Central Hypoventilation Syndrome
– Newborn son affected from birth, also has Hirschprung’s
– Exon 2 missense mutation p.Ala140Glu detected in both
– Previously reported only in isolated LO-CHS cases
Bristol Genetics Laboratory 2010
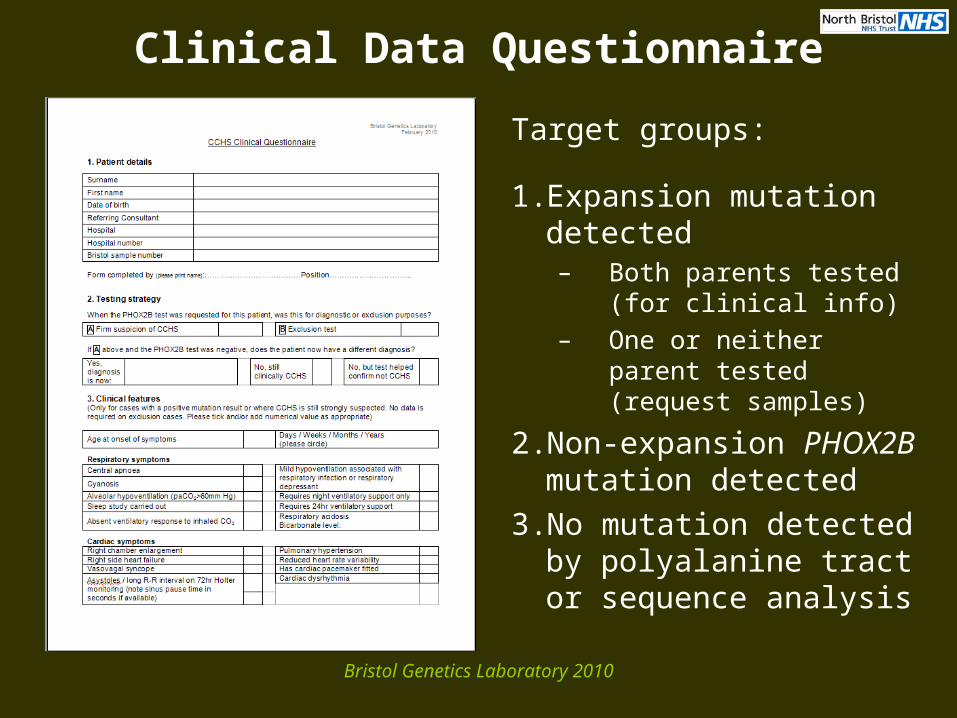
Clinical Data Questionnaire
Target groups:
1. Expansion mutation detected– Both parents tested (for
clinical info)– One or neither parent
tested (request samples)
2. Non-expansion PHOX2B mutation detected
3. No mutation detected by polyalanine tract or sequence analysis

Bristol Genetics Laboratory 2010
Conclusions
• UK PHOX2B mutation data closely matches distribution reported elsewhere
• Sequencing of PHOX2B relevant even if late onset CHS• Majority of PHOX2B referrals (up to 69%) now seemingly
for exclusion of CCHS• Clinical detail often lacking; questionnaire to refine
genotype-phenotype data• Higher than expected parental carrier rate (20% vs 7-14%)• Carrier parents may be unaware of symptoms• Evidence for germinal mosaicism in a UK family• Prenatal diagnosis available

Bristol Genetics Laboratory 2010
Acknowledgements
Bristol Genetics Laboratory
Maggie Williams
Claire Faulkner
Thais Simmonds
Teresa Lamb (Patrick)
Julie Evans
Bristol Clinical Team
Peter Fleming
Peter Lunt
All Wales Genetics Service
Rachel Butler
Julian Sampson
Rhianedd Ellwood-Thompson
Leiden
Dietje Fransen van de Putte





























