Embed Size (px)
Citation preview

. . . . Rural Crossroads . . . . .
Participant Satisfaction in an Adult Telehealth Education Program Using Interactive Compressed Video Delivery Methods in Rural Arkansas
Ann B. Bynum, EdD; Charles 0. Cranford, DDS, MPA; Cathy A. Irwin, PhD, RN, CS; and George S. Denny, PhD
ABSTRACT Context: Rural Americans have less access
interactive video technology. Methods: A program inistered to a convenience icipated in the program
telehealth education
D istance learning and telehealth services for consumers can bridge the knowledge disparity for rural Americans so they can have the same access to health promotion as citizens in urban areas. Arkansas
ranked 40th in terms of overall health and access to health care in the 2001 Morgan Quitno state health rankings.’ The Arkansas Delta Area Health Education Center (AHEC) reports that the rural Delta region of the state has a high school drop-out rate of 36%. Education has become one of the most widely used indicators of socioeconomic position used for mortality and health studies in both demography and epidemiology in the United States.’ Health care is a universal issue that affects all people, and relevant health information is a critical resource that enables people to make good decisions to enhance their health and well-being.
In 1995, to meet the growing need for health education in rural Arkansas, the University of Arkansas for Medical Sciences’ (UAMS) Rural Hospital Program developed a 53-site interactive compressed video network to deliver an Adult Telehealth Education Program. Affiliates with the network included hospitals, community health centers, rural health clinics, and 7 AHECs located throughout the state. Health education sessions were developed on the basis of communiv requests. The interactive sessions, originating from the UAMS main campus in Little Rock, included disease prevention and health promotion, as well as support groups for chronic disease management and parenting classes.
Central to the success of any program is the satisfaction of the end users. Socioeconomic and gm- graphic factors can potentially affect satisfaction with telehealth programs. Previous studies have not assessed the effect of these factors on satisfaction with telehealth program^.^-'^ Few studies, however, have evaluated participants’ satisfaction with telehealth education pro- grams delivered by interactive video. The compressed video technology delivers video images that have been processed to remove redundant information, thereby reducing the amount of bandwidth required to transmit them. The equipment used in this program transmits television-quality images at 30 frames per second. This study assessed satisfaction with this technology because
Earlier versions of this paper were published as abstracts in the Proceedings of the World Congress of High Tech Medicine (Hanover, Germany, October 16 to 20, 2000) and in the American Journal of Health Promotion (2000;14:332). The authors thank Marjorie A. Lacy, BA, from the Regional Programs a t the University of Arkansas for Medical Sciences, Little Rock, Ark, for her careful review and editing of the manuscript. For further informat.ilm, contact: Ann B. Bynum, EdD, director, Rural Hospital Prograr, University of Arkansas for Medical Sciences, 11 23 South University Ave, Suite 400, Slot 599A. Little Rock, AR 72204-1611; e-mail BynumCarolAQuams.edu.
The Journal of Rural Health 218 VOI. ?9, NO. 3

Rural Crossroads
it is the technology that Arkansas has chosen to use for distance education and telehealth. In addition, few studies have reported validity and reliability testing of the program satisfaction instruments utilized to evalu- ate telehealth education programs.
The purpose of this study was to assess differences in perceptions of program satisfaction among partic- ipants in the Adult Telehealth Education Program by age, gender, ethnicity, education, and community size and by program topics for the years 1996-1999. The program evaluation instrument was evaluated for internal consistency reliability and construct validity.
Methods Design and Sample. The study utilized a 1-group
post-test design with a sample of participants in the Adult Telehealth Education Program. Data were collected from January 1996 to August 1999.
Procedures. Interactive compressed video methods were used in the delivery of each of the telehealth program sessions. Topics for the programs were offered in response to specific requests by affiliates as de- termined by surveys, key informants, focus groups, and epidemiological studies. Health care professionals pre- sented topics of interest to consumers. All presenters completed a short training session on techniques for using video technology. Formats included slides, videos, demonstrations, and/or in1 eractive lectures.
delivered to distant sites around the state, including hospitals, community healtlh centers, rural health clinics, and 7 AHECs. The maximum number of sites partici- pating for 1 program was 1'2. All the programs were live and interactive, allowing the consumers at the distant sites to address questions to the presenters and interact with consumers at other sites. Programs were typically 1 hour in length, with 30 minutes each for the pre- sentation and a question-and-answer session for par- ticipants at the distant sites. Support groups were scheduled for 1.5 hours anld parenting classes for 2 hours. The UAMS Rural Hospital Program coordinator planned and scheduled the health education programs. Participants called the distant sites to enroll in the programs. All the programs were provided free of charge to participants.
Equipment for the compressed video technology included a VTEL 127 TCD Media Max video conferenc- ing system (VTEL Corporation, Austin, Tex); Polycom View Stations (Polycom, Iac, Milpitas, Calif); and ELMO- 400 Document Cameras (ELMO USA, Plainview, NY). The interactive compressed video technology was transmitted at 384 kilobits per second (Kbps) on a TI line.
Seventy-eight adult health program sessions were
After each program session, participants completed the program evaluation instrument. Site facilitators coordinated each program at the distant sites and distributed program evaluations for completion at the end of the session. The Rural Hospital Program coordinator trained site facilitators regarding proce- dures for program implementation and distribution of the program evaluation instrument. Establishing a per- manent base of community support was key to the long- term sustainability of the Telehealth Education Program. The rural hospitals, AHEC sites, local community organizations, and consumers became advocates for the delivery of programs by interactive video and assisted in program implementation.
Program Evaluation Instrument. The program evaluation instrument consisted of 7 items that evalu- ated participant satisfaction with program interest, quality, and scheduling. This instrument also included demographic information, how the participant learned of the program, comments, and requests for future topics. The response scale for this instrument consisted of a Likert-type scale ranging from strongly agree (5) to strongly disagree (1). Higher scores indicated higher program satisfaction. This instrument had not been tested previously for validity and reliability.
Statistical Procedures. Data were analyzed using the Statistical Package for Social Sciences (SPSS). Statistical procedures included the internal consistency reliability analysis, principal components factor analy- sis, 1-way analysis of variance (ANOVA), and t-test for independent samples.
Results Characteristics of the Sample. The sample for the
Adult Telehealth Program consisted of 2567 participants during 1996-1999, with a response rate of 69%. There were 2567 respondents out of 3740 total participants. The majority of the sample were women (83%), 19-64 years of age (74%), white (89%), had an educational level of a high school degree or higher (92%), and resided in small rural communities (population <15 000,73%). There were 295 (11%) respondents who were repeat program attendees, and 2272 respondents who attended 1 program session and were not repeat program attendees. Information about the program was obtained most frequently from a newsletter (20%).
Instrument Testing and Program Satisfaction for Years 1996-1999 and by Program Topics. The program evaluation instrument demonstrated adequate internal consistency reliability (Cronbachs alpha = 0.85) and construct validity. Participants in the Adult Telehealth
Bvnum, Cranford, Irwin, and c)enny 279 summer 2003

Rural Crossroads
Table 1. Mean Item Scores for Program Satisfaction: Adult Telehealth Education Program for Years 1996-1 999*
Instrument Item n Mean SD
1. I learned something from this program 2. The speaker presented the information well 3. The speaker made time for questions 4. The television equipment worked well 5. I would attend another session 6. This time of day is good for me 7. This day of the week is good for me Program satisfaction mean total score
2488 2478 2427 2477 2435 2489 2469
4.40 4.46 4.59 4.26 4.54 4.40 4.39 4.43
0 81 0.76 0.75 0.95 0.76 0.90 0.89 0.64
* Higher scores indicate higher program satisfaction (range of scores = 1 to 5)
Program had high levels of satisfaction regarding program interest and quality for years 1996-1999 (see Table 1).
The t-test for independent samples demonstrated significantly greater satisfaction with specific programs (heart disease, hormone replacement, health mainte- nance, vitamin deficiencies, diabetes, and parenting toddlers) when compared with all other programs combined (P<.OOl to P = .045). In addition, there was significantly higher satisfaction regarding the interactive video equipment for these specific programs (P< .001 to P =.035).
Program Satisfaction by Year, Gender, Age, Ethnicity, Education, and Community Size. Findings from the 1-way ANOVA indicated significantly higher satisfaction during 1998 (see Table 2). The t-test for independent samples demonstrated no significant dif- ference in program satisfaction between men and women. Results from the 1-way ANOVA with poly- nomial contrasts for linear trends indicated that adults 65 years and older had significantly higher program satisfaction. Findings from the t-test for independent samples and 1-way ANOVA indicated that black participants had significantly greater satisfaction than Asian, Hispanic, and white participants; and blacks had lower satisfaction than American Indians. Participants with a high school degree or less had significantly greater satisfaction than participants with higher edu- cational levels.
Findings from the 1-way ANOVA with polynomial contrasts for linear trends indicated that participants in small rural communities (population of 35 to 5000) had significantly higher satisfaction. Participants in those small rural communities (mean = 4.30, SD = 0.95) and in the largest urban communities (population of 75 001 to 180 000; mean = 4.33, SD = 0.75) had significantly higher
satisfaction regarding the compressed video equipment, F(1, 2537) = 5.57, P =.Om
Discussion Rural and minority populations, older adults, and
participants with lower educational levels expressed satisfaction with the Adult Telehealth Education Prw- gram delivered by interactive compressed video. Tltus finding, however, may be explained by the limited access to quality health care knowledge among these groups of program participants. The significantly higher satisfac- tion among older adults, blacks, American Indians,, and participants with a high school degree or less also might be explained by the Telehealth program methods. These methods included an emphasis on meeting participants’ learning needs for health education, the speakers’ communication with program participants, clarity od the presentation delivered by interactive compressed video, and convenient program scheduling.
tion with adult telehealth education programs. Findings from previous studies are consistent with findings from this study. Earlier studies demonstrated high levels of satisfaction among participants in telehealth education and telemedicine programs.3-6,8-10,12,13 These investiga- tions included small samples (N= 15 to 221) and did not assess significant differences in participant satisfackion by demographic variables and community size.
Limitations of the study design restrict the appli- cation of findings to other adult telehealth education programs. The 1-group post-test design also limits the ability to determine the effectiveness of methods for the Adult Telehealth Education Program. Additional limitations include the number of nonrespondents for study variables and program evaluation instrument
Few studies have evaluated participants’ satisfac-
The Journal of ~ u r a l Health 220 VOl. 19. NO. 3
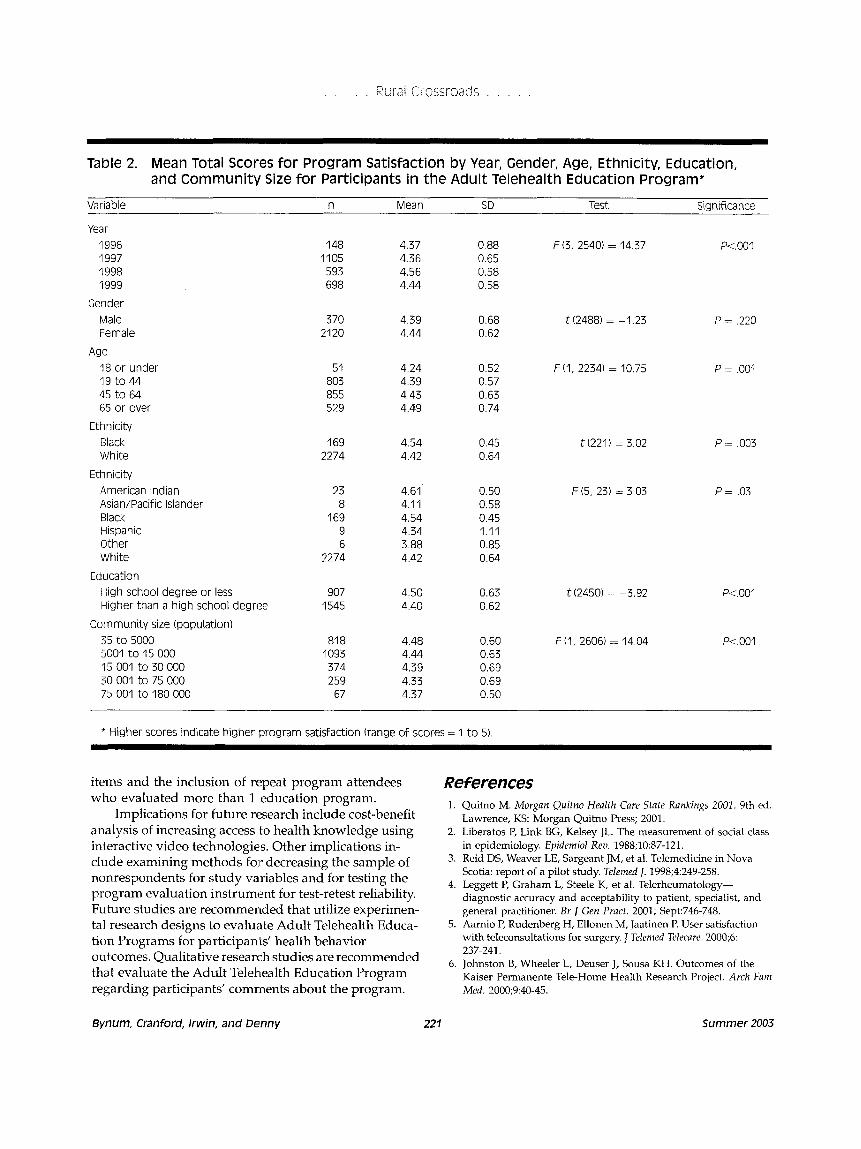
Table 2. Mean Total Scores for Program Satisfaction by Year, Gender, Age, Ethnicity, Education, and Community Size for Participants in the Adult Telehealth Education Program*
Variable n Mean SD Test Significance
Year 1996 1997 1998 1999
Gender Male Female
18 or under 19 to 44 45 to 64 65 or over
Ethnicity Black White
Ethnicity American Indian Asian/Pacific Islander Black Hispanic Other White
Age
148 4.37 0.88 F (3, 2540) = 14.37 P<.OOI 1105 4.36 0.65 593 4.56 0.58 698 4.44 0.58
370 4.39 0.68 t (2488) = -1.23 P = ,220 2120 4.44 0.62
51 4.24 0.52 F(1, 2234) = 10.75 P = ,001 803 4.39 0.57 855 4.43 0.63 529 4.49 0.74
169 2274
23 8
169 9 6
2274
4.54 4.42
4.61 4.11 4.54 4.34 3.88 4.42
0.45 t(221) = 3.02 P = ,003 0.64
0.50 F(5, 23) = 3.03 P = .03 0.58 0.45 1.11 0.85 0.64
Education High school degree or less 907 4.50 0.63 t(2450) = -3.92 Higher than a high school degree 1545 4.40 0.62
Community size (population) 35 to 5000 81 8 4.48 0.60 F(1, 2606) = 14.04 5001 to 15 000 1093 4.44 0.63 15 001 to 30 000 374 4.39 0.69 30 001 to 75 000 259 4.33 0.69 75 001 to 180 000 67 4.37 0.50
P<.OOI
P<.OOl
* Higher scores indicate higher program satisfaction (range of scores = 1 to 5)
1.
Implications for future research include-cost-benefit analysis of increasing access to health knowledge using interactive video technologies. Other implications in- clude examining methods for decreasing the sample of nonrespondents for study variables and for testing the program evaluation instrument for test-retest reliability. Future studies are recommended that utilize experimen- tal research designs to evaluate Adult Telehealth Educa- tion Programs for participants’ health behavior outcomes. Qualitative research studies are recommended that evaluate the Adult Telehlealth Education Program regarding participants’ comrnents about the program.
2.
3.
4.
5.
6.
items and the inclusion of repeat program attendees References Quitno M. Morgnn Quitno Health Care State Rankings 2001. 9th ed. who evaluated more than 1 education program. Lawrence, K S Morgan Quitno Press; 2001. Liberatos P, Link BG, Ketsey JL. The measurement of social class in epidemiology. Epidemiol Rezt 1988;10:87-121. Reid DS, Weaver LE, Sargeant JM, et al. Telemedicine in Nova Scotia: report of a pilot study. Telenzed J. 1998;4:249-258. Leggett P, Graham L, Steele K, et al. Telerheumatolom- diagnostic accuracy and acceptability to patient, specialist, and general practitioner. Br J Gen Prnct. 2001; Sept:746-748. Aarnio P, Rudenberg H, Ellonen M, Jaatinen P. User satisfaction with teleconsultations for surgery. J Telenzed Telecare. 2000;6:
Johnston B, Wheeler L, Deuser J, Sousa KH. Outcomes of the Kaiser Permanente Tele-Home Health Research Project. Arch Fam Med. 2000;9:40-45.
237-241.
Bynum, Cranford, Irwin, and Denny 221 Summer 2003
. . . . , Rural Crossroads . . . , .
:7. Aires LM, F d e y JP. Telemedicine activity at a Canadian 11. university medical school and its teaching hospitals. J Telemed Telecure. 2000;631-35.
8. Cheung ST, Davies RF, Smith K, Marsh R, Sherrard H, Wilbert JK. The Ottawa telehealth project. Telemed 1. 1998;4259-266.
9. Curran VR, Church JG. A study of rural women's satisfaction with a breast cancer self-help network. J Telemed Telecure. 1999;5: 47-54.
10. Elford R, White H, Bowering R, et al. A randomized, controlled trial of child psychiatric assessments conducted using videoconferencing. J Telemed Telecare. 2000;6:
12.
13.
73-82.
The Journal of Rural Health 222
Gelber H, Alexander M. An evaluation of an Australian videoconferencing project for child and adolescent telepsychiatry.
Mekhjian H, Turner JW, Gailiun M, McCain TA. Patient satisfaction with telemedicine in a prison environment. J Telemed Telecure. 1999;5:55-61. Valero MA, Arredondo MT, del Nogal F, Rodriguez Jh4, Fnias E. Patient satisfaction with a home televisiting service based on interactive television over a cable network. J Telemed Telecwe
Telemed Telecare. 1999;5(suppl l):S21-S23.
2000;6(~~ppl 1):S99-S101.
Vol. T9. No. 3





























