Embed Size (px)
Citation preview

BRIEF REPORT
Early Diagnosis and Treatment of Discoid LupusErythematosusSuresh Panjwani, MD, MSc, FRACGP
Discoid lupus erythematosus is a chronic dermatological disease that can lead to scarring, hair loss,and hyperpigmentation changes in skin if it is not treated early and promptly. It has a prolonged courseand can have a considerable effect on quality of life. Early recognition and treatment improves the prog-nosis. The diagnosis is usually made by clinical examination. In some cases histopathology may be re-quired to confirm the diagnosis. The histology is that of an inflammatory interface dermatosis. There isinsufficient evidence for which treatment is most effective. Because lesions are induced or exacerbatedby ultraviolet exposure, photoprotective measures are important. Potent topical steroids and antima-larials are the mainstay of treatment. Some cases of discoid lupus erythematosus can be refractory tostandard therapy; in these cases retinoids, thalidomide, and topical tacrolimus offer alternatives, as doimmunosuppressives like azathioprine, cyclosporine, mycophenolate mofetil, and methotrexate. (J AmBoard Fam Med 2009;22:206–213.)
Lupus erythematosus (LE) is thought to be anautoimmune disease among other connective tissuediseases like scleroderma, rheumatoid arthritis,polymyositis, and mixed connective tissue disease.Within the spectrum of diseases included in LE, atone end is a disease confined mainly to the skin andreferred to as discoid lupus erythematosus (DLE)and at the other end is a florid disease with systemicinvolvement of heart, lungs, brain, kidneys andother organs called systemic lupus erythematosus(SLE). In between the 2 ends of the spectrum aredisorders like subacute cutaneous lupus. Subacutecutaneous lupus erythematosus (SCLE) has arather sudden onset with annular or psoriasiformplaques erupting on the upper trunk, arms, and/ordorsa of hands, usually after exposure to sunlight.1
Although at the benign end of the spectrum, 1% to
5% of patients with discoid lupus may developSLE1 and 25% of patients with SLE may developtypical chronic discoid lesions at some time duringthe course of their illness.2
Lupus occurs in all age groups with a mean agevarying from 21 years to 50 years3 and a prevalenceof 17 to 48 in 100,000,4 with a greater prevalence inAfro-Caribbean people.5 Although LE is an auto-immune disease, it is thought to result from aninterplay of certain genetic factors, environmentalfactors like ultraviolet light, and hormonal factorswith antibodies.
The diagnosis of discoid lupus is generally madebased on clinical features. Histology may be re-quired to confirm the diagnosis; it is that of alichenoid tissue reaction with changes at thedermo-epidermal junction that include thickeningof the basement membrane (best demonstrated byperiodic acid-Schiff staining) and vacuolar degen-eration of the basal cells along with perivascularand peri-appendageal inflammatory cell infiltrationof a variable degree in the reticular dermis. Hyper-keratosis is more evident and follicular pluggingmay be seen in more mature lesions.
DLE tends to run a less severe course than SLEand has a better prognosis. It is important for fam-ily physicians to recognize DLE because it is apotentially scarring disease. Early referral and in-stitution of treatment by dermatologists increases
This article was externally peer reviewed.Submitted 13 April 2008; revised 23 June 2008; accepted 1
July 2008.From Bounces Road Surgery, Forest Primary Care Cen-
tre, London, UK.Funding: none.Prior presentation: Much of this work was presented as the
author’s MSc Thesis in Clinical Dermatology; permissionfor use granted by St. John’s Institute of Dermatology,King’s College, London.
Conflict of interest: none declared.Corresponding author: Suresh Panjwani, MD, MSc,
FRACGP, 4 Harper Close, Southgate, London N14 4ES,United Kingdom (E-mail: [email protected]).
206 JABFM March–April 2009 Vol. 22 No. 2 http://www.jabfm.org
the hope of minimizing the progression of thedisease and consequent socioeconomic impact onthe individual.
Clinical FeaturesDiscoid lupus is by far the most common manifes-tation of LE.6 It commonly presents with erythem-atous, scaly papules and plaques (Figure 1) occur-ring on sun-exposed areas, although 50% of discoidlupus lesions are found on areas of hair-bearingscalp that are presumably protected from the sun6
(Figures 2 and 3). In the localized variety of discoidlupus the lesions tend to be confined to the headand neck and in the generalized variety they occurboth above and below the neck. Patients with gen-eralized discoid have significantly greater chancesof having laboratory abnormalities and of progress-ing to systemic LE. Most people with DLE do not
have any systemic or serologic abnormality al-though antinuclear antibodies may be present.
Discoid lupus occurs at all ages and among allethnic groups; it occurs more frequently in womenthan in men, but the predilection among women isnot as marked as in systemic lupus. Discoid lupusstarts as an erythematous papule or plaque, usuallyon the head or neck, with an adherent scale. Thelesion tends to spread centrifugally and as itprogresses there is follicular plugging and pigmen-tary changes, generally hyperpigmentation at theperiphery, and hypopigmentation with atrophy,scarring, and telengiectasia at the center of thelesion (Figure 4).
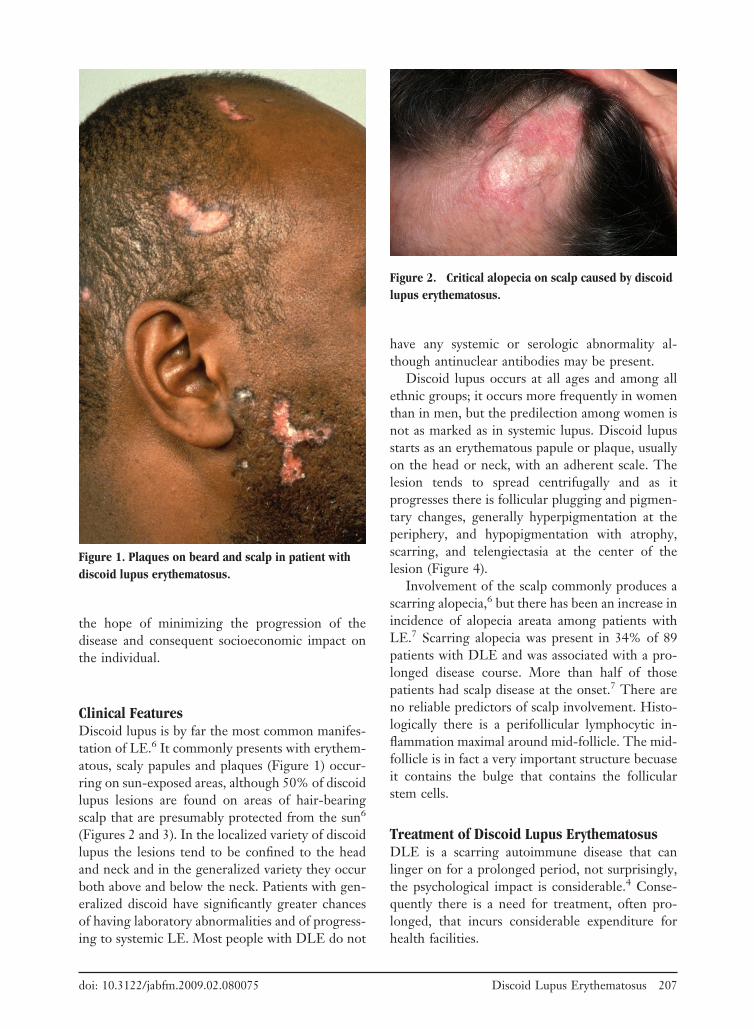
Involvement of the scalp commonly produces ascarring alopecia,6 but there has been an increase inincidence of alopecia areata among patients withLE.7 Scarring alopecia was present in 34% of 89patients with DLE and was associated with a pro-longed disease course. More than half of thosepatients had scalp disease at the onset.7 There areno reliable predictors of scalp involvement. Histo-logically there is a perifollicular lymphocytic in-flammation maximal around mid-follicle. The mid-follicle is in fact a very important structure becuaseit contains the bulge that contains the follicularstem cells.
Treatment of Discoid Lupus ErythematosusDLE is a scarring autoimmune disease that canlinger on for a prolonged period, not surprisingly,the psychological impact is considerable.4 Conse-quently there is a need for treatment, often pro-longed, that incurs considerable expenditure forhealth facilities.
Figure 1. Plaques on beard and scalp in patient withdiscoid lupus erythematosus.
Figure 2. Critical alopecia on scalp caused by discoidlupus erythematosus.
doi: 10.3122/jabfm.2009.02.080075 Discoid Lupus Erythematosus 207

Early effective treatment may lead to total clear-ing of skin lesions, but failure of treatment resultsin permanent scarring; the depressed scars, hairloss, and pigmentary changes are often extremelydisfiguring, particularly in darker-skinned people.8
According to a 2004 systematic review of treatmentof discoid lupus by Jessop et al8 only 30 trials wereidentified through a search of the Cochrane Clin-ical Trials Register (December 1999); Medline(January 1966 to December 1999); Embase (Janu-ary 1980 to January 2000); and Index Medicus(1956 to 1966).8 Only 4 of these were controlledtrials and only 2 of the latter were randomized (A,level 2). Accordingly, more evidence is needed toguide clinicians to the best treatment options forDLE, particularly for the severe type.
The treatment of DLE would in most instancesbe initiated at a dermatology department, but be-fore instituting treatment for discoid lupus patientsshould be assessed for systemic involvement. Thisshould include a full history and physical examina-tion, full blood count, erythrocyte sedimentation
rate, midstream urine, and antinuclear antibody.9 IfSLE is suspected, anti-double stranded DNA, ex-tractable nuclear antigen, C3/C4, and renal reviewshould also be included.9
General MeasuresBecause cutaneous lesions of lupus are known to beinduced or exacerbated by exposure to ultravioletlight, a logical approach in the management ofdiscoid lupus must include sun avoidance and theliberal application of sunscreens. Patients should beeducated about the use of sunscreens and protectiveclothing and behavior modification to avoid sunexposure, particularly between 10 am and 4 pm.They should also be aware of water, snow, and sandsurfaces, from which ultraviolet light may be re-flected, and where harm can occur from reflectedultraviolet light.
They should be instructed to use sunscreensdaily and apply liberally; they should reapply themif there has been prolonged sun exposure or when
Figure 3. Extensive loss of scalp hair in a patient withdiscoid lupus.
Figure 4. Close-up view of plaque in a patient withdiscoid lupus.
208 JABFM March–April 2009 Vol. 22 No. 2 http://www.jabfm.org

they are wet.10 Protection against both ultravioletA and ultraviolet B is desirable because lupus isaggravated by both.11,12 With disfigurement andalopecia, patients may benefit from advice on cam-ouflage and the wearing of a wig.
Topical CorticosteroidsTopical steroids are the mainstay of treatment ofDLE. Patients usually start with a potent topicalsteroid applied twice a day, then switch to a lower-potency steroid as soon as possible. The minimaluse of steroids reduces the recognized side effectslike atrophy, telengiaectasiae, striae, and purpura.
Intralesional SteroidsIntralesional steroids are particularly useful to treatchronic lesions, hyperkeratotic lesions, and thosethat do not respond adequately to topical steroids.Lesions at particular sites, eg, the scalp, may alsobenefit. Recognized side effects of intralesional ste-roids include cutaneous atrophy and dyspigmenta-tion, which are not significant risks in experiencedhands.13 Oral steroids may be required for thecontrol of systemic lupus but are not generallybeneficial in DLE. For patients with progressive ordisseminated disease or in those with localized dis-ease that does not respond to topical measures, theaddition of systemic agents should be considered.
AntimalarialsTreatment with antimalarial drugs constitutes first-line systemic therapy for DLE. Therapy with an-timalarials, either used singly or in combination, isusually effective.14 The 3 commonly used prepara-tions include chloroquine, hydroxychloroquin, andmepacrine. Mepacrine is not freely commerciallyavailable in the United States but is freely availablein other countries like the United Kingdom.
It is customary to start hydroxychloroquine at adose of 200 mg per day for an adult and, if there areno untoward gastrointestinal or other side effects,to increase the dose to twice a day. No more than6.5 mg/kg/day should be administered. It is impor-tant to emphasize to the patient that it may takebetween 4 to 8 weeks for any clinical improvement.In some patients who do not respond to hydroxy-chloroquine, chloroquine may be more effective.Some patients do not respond well to monotherapywith either hydroxychloroquine or chloroquine,and in such cases the addition of mepacrine may beof benefit.15
In general, hydroxychloroquine and mepacrineare safe, well-tolerated drugs and adverse effects arerelatively few, the most widely recognized beingretinal toxicity.16 Chloroquine causes macular pig-mentation that progresses to a typical bull’s eyelesion and then to widespread retinal pigment ep-ithelial atrophy resembling retinitis pigmentosa.16
This is dose related and can largely be avoided. Theside effect spectrum between chloroquine and hy-droxychloroquine is different, with ocular toxicitybeing mainly, although perhaps not exclusively,seen after chloroquine use. To prevent overdosing,doses should be calculated not on the actual weightof the patient but on ideal (lean) body weight;17 thissubstantially reduces the risk of retinal toxicity.
Other adverse effects of antimalarials includegastrointestinal symptoms, eg, nausea and vomit-ing, and cutaneous side effects including pruritus,lichenoid drug reactions, annular erythema, hyper-pigmentation, and hematological disturbances likeleukopenia and thrombocytopenia.18 Hemolysis isreported in individuals who are deficient in theenzyme glucose-6-phosphate-dehydrogenase. Hy-droxychloroquine has, on rare occasions, causedtoxic psychosis when used for the treatment ofdiscoid lupus.19 Prolonged mepacrine therapy mayproduce a yellow discoloration of the skin andurine. Hepatitis and aplastic anemia have also beenreported.
Potentially more toxic therapeutic medicationneeds to be used in the management of many casesof DLE; however, topical tacrolimus ointment hasbeen found recently to be useful in the manage-ment of DLE (see below). The different forms oftherapeutic agents used in the management of DLEare highlighted in Table 1.
Thalidomide may provide one of the most usefultherapeutic alternatives for chronic refractoryDLE, although its distribution is limited to a fewcountries because of the risk of teratogenicity andpolyneuropathy.20 However, in a retrospectivestudy of 18 patients with chronic DLE, Brocard etal21 found low-dose thalidomide treatment was ef-ficacious with good tolerance, with the most fre-quent side effect being usually mild asthenia.
Other Drugs Used for the Treatment of DLEMethotrexateIn 1995, Bottomley and Goodfield22 found thatmethotrexate may be of help to patients with DLEresistant to conventional treatment; short-term
doi: 10.3122/jabfm.2009.02.080075 Discoid Lupus Erythematosus 209

Tabl
e1.
Diff
eren
tDru
gsUs
edin
the
Trea
tmen
tofD
isco
idLu
pus
Eryt
hem
atos
us
Nam
eof
Dru
gD
ose
Adv
erse
Eff
ects
Rem
arks
Top
ical
and
intr
ales
iona
lste
roid
sSt
art
with
pote
ntto
pica
lpre
para
tion,
stre
ngth
ofin
trad
erm
altr
iam
cino
lone
3to
5m
g/m
LC
utan
eous
atro
phy,
tele
ngie
ctas
iae,
stri
ae,a
ndpu
rpur
aw
ithto
pica
lste
roid
s;at
roph
yan
ddy
spig
men
tatio
nw
ithin
tral
esio
nals
tero
ids
Side
effe
cts
from
syst
emic
abso
rptio
nin
sign
ifica
ntw
ithto
pica
lste
roid
sbu
tca
noc
cur
with
intr
ales
iona
lste
roid
sA
ntim
alar
ials
Star
tw
ith20
0m
gpe
rda
y,no
mor
eth
an6.
5m
g/kg
/day
tobe
adm
inis
tere
dG
astr
oint
estin
alup
set,
ocul
arto
xici
ty,p
ruri
tus,
drug
erup
tions
,leu
cope
nia,
thro
mbo
cyto
peni
a,ha
emol
ysis
Ocu
lar
toxi
city
mor
em
arke
dw
ithch
loro
quin
e
Top
ical
tacr
olim
us0.
1%to
pica
loin
tmen
tB
urni
ng,i
rrita
tion
ofsk
in,p
ruri
tus
Con
trai
ndic
atio
n-in
fect
ions
Tha
lidom
ide
Initi
aldo
seof
100
to20
0m
g/da
y,us
ual
mai
nten
ance
dose
of50
to10
0m
g/da
yT
erat
ogen
icity
,pol
yneu
ropa
thy,
drow
sine
ss,
naus
ea,s
kin
erup
tions
,dry
ness
ofm
outh
and
skin
,oed
ema
Pol
yneu
ropa
thy
unco
mm
onw
ithus
eof
low
dose
s
Aza
thio
prin
eU
sual
star
ting
dose
of50
to10
0m
g/da
y,us
ual
mai
nten
ance
dose
of25
to50
mg/
day
Mye
losu
ppre
ssio
n,na
usea
,inf
ectio
nspa
ncre
atiti
s,ra
rely
hepa
toto
xici
tySe
rum
thio
puri
nem
ethy
ltran
sfer
ase
shou
ldbe
mea
sure
dC
yclo
spor
inIn
itial
dose
of4
to5
mg/
kg/d
ay,w
hich
can
bere
duce
dw
ithim
prov
emen
tH
yper
tens
ion,
neph
roto
xici
ty,h
yper
lipid
emia
,hy
pom
agne
sem
ia,g
ingi
valh
yper
plas
ia,
head
ache
,tre
mor
,par
esth
esia
,hyp
ertr
icho
sis,
mal
igna
ncy
Con
trai
ndic
atio
nsin
clud
eun
cont
rolle
dhy
pert
ensi
on,u
ncon
trol
led
infe
ctio
ns,a
ndm
alig
nanc
y
Myc
ophe
nola
tem
ofet
ilU
sual
dose
of1
gtw
ice
ada
yG
astr
icup
set,
head
ache
,tre
mor
,hyp
erse
nsiti
vity
,an
emia
,leu
cope
nia
and
thro
mbo
cyto
peni
a,in
fect
ions
,neo
plas
ia
Full
bloo
dco
unts
shou
ldbe
chec
ked
regu
larl
y
Met
hotr
exat
e5
to15
mg
once
aw
eek
follo
wed
byin
itial
test
dose
of2.
5m
gG
astr
oint
estin
alup
set,
mye
losu
ppre
ssio
n,liv
erto
xici
ty,p
ulm
onar
yfib
rosi
sM
onito
rfu
llbl
ood
coun
t,liv
erfu
nctio
nte
sts,
and
rena
lfun
ctio
nA
citr
etin
0.5
to1
mg/
kg/d
ayT
erat
ogen
icity
,hyp
erlip
idem
ia,d
ryne
ssof
skin
,m
ucou
sm
embr
anes
,tas
tedi
stur
banc
es,h
air
loss
Mon
itor
full
bloo
dco
unt,
liver
func
tion
test
s,fa
stin
glip
ids
210 JABFM March–April 2009 Vol. 22 No. 2 http://www.jabfm.org

treatment is unlikely to be complicated by anysignificant side effects.22 Full blood count and liverfunction along with renal function need to bechecked before commencing treatment with meth-otrexate and regularly thereafter because it cancause myelosuppresion and hepatic and renal im-pairment.
Cyclosporin AThis is a potent immunosuppressant because of itsimmunomodulating effect on helper T-cell func-tion, inhibiting lymphocyte activation and prolifer-ation. Because DLE is an inflammatory dermatosiswith T-cell infilterate it should not be surprising ifcyclosporine is effective in the management of thecondition. In 1994 Yell and Burge23 tried cyclo-sporine in 2 patients with severe DLE and con-cluded that it was effective at a dose of 4 to 5mg/kg/day, but others have not confirmed thisfinding. Blood pressure and kidney function needto be monitored, and hypertension is a commonside effect. It can also cause gingival hyperplasiaand hirsutism. Lipid disturbances can also occurand therefore serum cholesterol and triglycerideshave to be monitored.
TacrolimusTacrolimus is a macrolide derived from the fungusStreptomyces tsukubaensis and has been used in recentyears to treat a number of inflammatory and auto-immune conditions. When used as an ointment itacts as a local immunosuppressive agent. Walker etal24 reported 2 patients with severe recalcitrantchronic discoid lupus that had not responded topotent topical steroids or antimalarials but dramat-ically responded to topical tacrolimus ointment inone case and a combination of clobetasol ointmentand tacrolimus in the other.24 Recently, Tzung etal25 conducted a randomized double-blind study inwhich 20 patients were enrolled but only 11 womenand 7 men (13 with malar rash of SLE, 4 with DLE,and 1 with SCLE) completed the study. All patientshad facial cutaneous LE and were instructed toapply 0.1% tacrolimus ointment twice daily to theaffected areas on one side of the face and 0.05%clobetasol propionate ointment on the other side;this was randomly assigned for each patient. Theseverity of lesions was assessed at each visit (weeks0–4 and posttreatment week 4) using a 7-pointrating scale. They found tacrolimus was as efficientas clobetasol in treating cutaneous LE (B, level 2).25
Mycophenolate mofetilThis is an immunosuppressive agent that has beenadded relatively recently to the other drugs in thisgroup and has been used increasingly in recentyears for the treatment of various dermatoses thatare inflammatory or autoimmune in origin. Myco-phenolate is an ester prodrug of mycophenolic acid,initially isolated from Penicillium species.26 Goyaland Nousari27 described 2 cases of refractory dis-coid lupus involving the palms and soles that re-sponded satisfactorily to mycophenolate mofetil.
AzathioprineAzathioprine, a potentially toxic drug, has beenused in refractory cases of discoid lupus, with par-ticular success among those with the involvementof the palms of the hands and the soles of the feet.28
It is a synthetic derivative of 6-mercaptopurine andis an immunosuppressive drug. There are wide dif-ferences in the activity of the enzyme thiopurinemethyltransferase in different individuals, whichcan be measured by a blood test. The chances ofmyelosuppression in a patient with very low levelsof thiopurine methyltransferase are significantlygreater than in others.
Other forms of treatment have recently beenfound to be useful in the treatment of DLE. Gul etal29 described a case of generalized DLE success-fully treated with 5% Imiquimod cream applied tolesions once a day 3 times a week. After 20 appli-cations all of the lesions regressed significantly.Usmani and Goodfield30 reported good to excel-lent responses in 12 out of 13 patients with DLEwho were treated with efalizumab, a monoclonalantibody directed against CD 11a (discoid lupus isknown to be predominantly t-cell mediated). Fi-nally, Koch et al31 suggest cryotherapy as a treat-ment option in cases of DLE lesions that are resis-tant to local or systemic recommended therapy.The standard therapies for the management of cu-taneous lupus, including sunscreens, protectiveclothing, and behavioral alteration, and topical ste-roids with or without an antimalarial agent areoften not used appropriately and can result in asituation in which the patient has a refractory dis-ease.32
ConclusionDLE is a chronic scarring and potentially disfigur-ing disease seen in all parts of the world and among
doi: 10.3122/jabfm.2009.02.080075 Discoid Lupus Erythematosus 211

all ethnic groups. It is an important cause of irre-versible hair loss and is associated with considerablemorbidity. It is extremely important for family phy-sicians to diagnose this relatively uncommon con-dition early because early effective treatment isimportant to promote the resolution of establishedlesions and to prevent scarring. There are severalforms of treatment that are effective to a lesser orgreater degree than others. There are too fewproperly conducted randomized trials to enable aninformed choice by clinicians. Clinicians at thepresent time are, therefore, likely to choose theirpreferred treatment based on their own experience.There is a need for further large randomized, con-trolled, and possibly multinational trials to be con-ducted that compare the effectiveness and safety ofone form of treatment compared with another.
References1. Fitzpatrick TB, Johnson RA, Klaus W, Suurmond
D. In colour atlas and synopsis of clinical dermatol-ogy, 4th ed. New York (NY): McGraw-Hill Com-panies; 2001:368–9.
2. Lahita RG. In systemic lupus erythematosus, 2nd ed.New York (NY): Churchill Livingstone; 1987:620.
3. Tebbe B, Orfanos CE. [Lupus erythematosus of theskin. An analysis of 97 patients.] Z Hautkr 1987;62:1563–72, 1577–8, 1583–4.
4. Tebbe B, Orfanos CE. Epidemiology and socioeco-nomic impact of skin disease in lupus erythematosus.Lupus 1997;6:96–104.
5. Hochberg MC, Boyd RE, Ahearn JM, et al. Systemiclupus erythematosus: a review of clinico-laboratoryfeatures and immunogenetic markers in 150 patientswith emphasis on demographic subsets. Medicine1985;64:285–95.
6. Hymes SR, Jordon RE. Chronic cutaneous lupuserythematosus. Med Clin N Am 1989;73:1055–71.
7. Werth VP, White WL, Sanchez MR, Franks AG.Incidence of alopecia areata in lupus erythematosus.Arch Dermatol 1992;128:368–71.
8. Jessop S, Whitelaw D, Jordaan F. Drugs for discoidlupus erythematosus. Cochrane Database Syst Rev2001;(1):CD002954.
9. Donnelly AM, Halbert AR, Rohr JB. Discoid lupuserythematosus. Australas J Dermatol 1995;36:3–10;quiz 11–2.
10. Ting WW, Sontheimer RD. Local therapy for cu-taneous and systemic lupus erythematosus: practicaland theoretical considerations. Lupus 2001;10:171–84.
11. Sanders CJ, Van Weelden H, Kazzaz GA, Sigurds-son V, Toonstra J, Bruijnzeel-Koomen CA. Photo-sensitivity in patients with lupus erythematosus: aclinical and photobiological study of 100 patients
using a prolonged phototest protocol. Br J Dermatol2003;149:131–7.
12. Lehmann P, Holzle E, Kind P, Goerz G, Plewig G.Experimental reproduction of skin lesions in lupuserythematosus by UVA and UVB radiation. J AmAcad Dermatol 1990;22:181–7.
13. Callen JP. Cutaneous lupus erythematosus: a per-sonal approach to management. Australas J Derma-tol 2006;47:13–27.
14. Callen JP. Treatment of cutaneous lesions in pa-tients with lupus erythematosus. Dermatol Clin1994;12:201–6.
15. von Schmiedeberg S, Ronnau AC, Schuppe HC,Specker C, Ruzicka T, Lehmann P. [Combination ofantimalarial drugs mepacrine and chloroquine intherapy refractory cutaneous lupus erythematosus.]Hautarzt 2000;51:82–5.
16. Cruz DD. Antimalarial therapy: a panacea for mildlupus. Lupus 2001;10:148–51.
17. Mackenzie AH. Dose refinements in the long termtherapy of rheumatoid arthritis with antimalarials.Am J Med 1983;75:40–5.
18. Lo JS, Berg RE, Tomecki K. Treatment of discoidlupus erythematosus. Int J Dermatol 1989;28:497–505.
19. Ward Q, Walter-Ryan WG, Shehi GM. Toxic psy-chosis: a complication of antimalarial therapy. J AmAcad Dermatol 1985;12:863–5.
20. Fabbri P, Cardinali C, Giomi B, Caproni M. Cuta-neous lupus erythematosus: diagnosis and manage-ment. Am J Clin Dermatol 2003;4:449–65.
21. Brocard A, Barbarot S, Milpied B, Stalder JF. Tha-lidomide in the treatment of chronic discoid lupuserythematosus. Ann Dermatol Venereol 2005;132(11 Pt 1):853–6.
22. Bottomley WW, Goodfield MJ. Methotrexate forthe treatment of discoid lupus erythematosus. Br JDermatol 1995;133:655–6.
23. Yell JA, Burge SM. Cyclosporin and discoid lupuserythematosus. Br J Dermatol 1994;131:132–48.
24. Walker SL, Kirby B, Chalmers RJ. The effect oftopical tacrolimus on severe recalcitrant chronic dis-coid lupus erythematosus. Br J Dermatol 2002;147:405–6.
25. Tzung TY, Liu YS, Chang HW. Tacrolimus vs.clobetasol propionate in the treatment of facial cu-taneous lupus erythematosus: a randomized, double-blind, bilateral comparison study. Br J Dermatol2007;156:191–2.
26. Nousari HC, Sragovich A, Kimyai-Asadi A, OrlinskyD, Anhalt GJ. Mycophenolate mofetil in autoim-mune and inflammatory skin disorders. J Am AcadDermatol 1999;40(2 Pt 1):265–7.
27. Goyal S, Nousari HC. Treatment of resistant discoidlupus erythematosus of palms and soles with myco-phenolate mofetil. J Am Acad Dermatol 2001;45:142–4.
212 JABFM March–April 2009 Vol. 22 No. 2 http://www.jabfm.org

28. Abu Shakra M, Shoenfield Y. Azathioprine therapyfor patients with systemic lupus erythematosus. Lu-pus 2001;10:152–3.
29. Gul U, Gonul M, Cakmak SK, Kilic A, Demiriz M.A case of generalized discoid lupus erythematosus:successful treatment with imiquimod cream 5%. AdvTher 2006;23:787–92
30. Usmani N, Goodfield M. Efalizumab in the treat-
ment of discoid lupus erythematosus. Arch Dermatol2007;143:873–7.
31. Koch M, Horwath-Winter J, Aberer E, SalmhoferW, Klein A. [Cryotherapy in discoid lupus erythem-atosus (DLE).] Ophthalmologe 2008;105:381–3.
32. Callen JP. Management of refractory skin disease inpatients with lupus erythematosus. Best Pract ResClin Rheumatol 2005;19:767–84.
doi: 10.3122/jabfm.2009.02.080075 Discoid Lupus Erythematosus 213





























