Embed Size (px)
Citation preview

Review
Breast Reconstruction with a Tissue Engineering and Regenerative
Medicine Approach (Systematic Review)
E. DONNELY ,1 M. GRIFFIN,1,2 and P. E. BUTLER1,2
1Division of Surgery and Interventional Science, University College London,Royal Free Hospital Campus, London, UK; and 2Department of Plastic Surgery, Royal Free Hospital, London, UK
(Received 1 August 2019; accepted 21 September 2019; published online 1 October 2019)
Associate Editor Eric M. Darling oversaw the review of this article.
Abstract—Current techniques for breast reconstructioninclude an autologous-tissue flap or an implant-based pro-cedure, although both can impose further morbidity. Thissystematic review aims to explore the existing literature onbreast reconstruction using a tissue engineering approach;conducted with the databases Medline and Embase. A totalof 28 articles were included, mainly comprising of level-5evidence with in vitro and animal studies focusing on utilizingscaffolds to support the migration and growth of new tissue;scaffolds can be either biological or synthetic. Biologicalscaffolds were composed of collagen or a decellularized tissuematrix scaffold. Synthetic scaffolds were primarily composedof polymers with customisable designs, adjusting the internalmorphology and pore size. Implanting cells, includingadipose-derived stem cells, with combined use of basicfibroblast growth factor has been studied in an attempt toenhance tissue regeneration. Lately, a level-4 evidence humancase series was reported; successfully regenerating 210 mL oftissue using an arterio-venous pedicled fat flap within a tissueengineering chamber implanted on the chest wall. Furtherresearch is required to evaluate whether the use of cells andother growth factors could adjust the composition ofregenerated tissue and improve vascularity; the latter a majorlimiting factor for creating larger volumes of tissue.
Keywords—Breast reconstruction, Tissue engineering, Re-
generative medicine, Scaffold, Cellular therapy, Stem cells,
Adipose-derived stem cells.
INTRODUCTION
Breast cancer poses a significant problem, being themost common cancer in the UK female population. In2015 alone there were 54,800 new cases diagnosed,with incidence rates projected to increase 2% by theyear 2035.4 Despite this increase, better screening andtreatment options are leading to an improvement insurvival rates, meaning almost eight out of 10 womensurvive greater than 10 years after diagnosis.4 By theend of 2010, there was just under half a million womenin the UK living with a diagnosis of breast cancer. Andits not just affecting the UK, with an estimated twomillion new cases diagnosed worldwide in 2018.2
Following a diagnosis of breast cancer, 81% ofpatients undergo surgery to remove the primary tumor.4
This can be accompanied by neoadjuvant or adjuvantchemotherapy and radiotherapy, tailored according tothe individual case. Surgery, whether lumpectomy ormastectomy, has long been associated with a significantburden of disease; the disfiguring surgical procedureleading to psychological distress, loss of femininity,sexual dysfunction and even suicidal ideation.23,28
Breast reconstruction can be offered immediately atthe time of initial surgery in the case of neoadjuvanttherapy, or as a delayed procedure following anyrequired adjuvant therapy and necessary planning. Thetiming of reconstruction is highly dependant on suchtherapy, with a delayed autologous tissue flap moreindicative if postmastectomy radiation is required dueto an increased risk of capsular contracture or flapfailure if performed as an immediate procedure priorto radiation.26 Patients undergoing a mastectomy plusbreast reconstruction have a significantly decreasedincidence of anxiety and depressionwhen compared with
Address correspondence to E. Donnely, Division of Surgery and
Interventional Science, University College London, Royal Free
HospitalCampus,London,UK.Electronicmail: Edward.donnely10@
alumni.imperial.ac.uk
Annals of Biomedical Engineering, Vol. 48, No. 1, January 2020 (� 2019) pp. 9–25
https://doi.org/10.1007/s10439-019-02373-3
BIOMEDICALENGINEERING SOCIETY
0090-6964/20/0100-0009/0 � 2019 The Author(s)
9

mastectomy alone.6 Breast reconstruction provides anaesthetic benefit and the current standard of practice iseither an autologous tissue flap or implant based (siliconor saline) procedure. However both can impose furthermorbidity that should not be unheeded and require an in-depth discussion between clinician and patient evaluatingthe risks and benefits of each. The sequalae of an autol-ogous tissue flap includes the short-term complication offlap failure and long-term complications of fat necrosisand donor site morbidity17 while the silicone/saline im-plant based procedure incurs short-term risk of infectionand long-term risks of capsular contracture and implantrupture.15 Textured implants are at present under reviewdue to a possible association with anaplastic large celllymphoma.3 These risks emphasise the need for a newtechnique of breast reconstruction.
Since stem cells were first identified, scientists andhealth professionals alike have been working towardrepairing and replacing human tissue damaged sec-ondary to disease and trauma using tissue engineeringand regenerative medicine. Their aim of using autolo-gous cells to proliferate and replenish the desired tissuecould eliminate the long-term complications associatedwith either technique, such as capsular contracture orthe need to harvest an autologous flap and hence do-nor site morbidity.
The breast is composed of glandular and adiposetissue, the latter forming majority of the volume.Autologous fat grafting has been used to fill soft tissuedefects within the body, including the breast, althoughthe limitation of resorption and unable to maintainvolume for significant periods of time still persists.13
Cell-assisted lipotransfer involves the enrichment ofthe fat graft with adipose-derived stem cells, hypothe-sizing the ability to withstand longer periods ofhypoxia. Although one study still reported loss of 47%of the initial post-operative volume following breastaugmentation.24,34 To address this issue, the idea ofdesigning a support structure capable of providingstructural integrity to the developing tissue has beenhypothesized and is leading the way to a tissue engi-neered breast.
This article aims to explore and perform a system-atic review of the current literature on breast recon-struction using a tissue engineering and regenerativemedicine approach.
METHODS
A systematic review was conducted with the litera-ture databases Medline (OvidSP; 1946 to 6/12/2018)and Embase (Ovid; 1974 to 12/12/2018), adhering tothe PRISMA guidelines.
The search criteria was formulated to identify arti-cles on ‘breast reconstruction’ AND ‘tissue engineer-ing’. The base search filters for ‘breast reconstruction’included {MAMMAPLASTY/OR MASTECTOMY/(MeSH terms)} OR {‘‘breast reconstruct*’’ ORmamm?plasty OR mastectomy OR (breast ANDlumpectomy) (keywords)}. The base search filters for‘tissue engineering’ included {TISSUE ENGINEER-ING/OR BIOMEDICAL ENGINEERING/OR RE-GENERATIVE MEDICINE/(MeSH terms)} OR{(‘‘tissue engineer*’’ OR ‘‘biomedical engineer*’’ OR‘‘regenerative medicine’’ OR biomaterial* OR ‘‘addi-tive manufactur*’’ OR ‘‘3D print*’’ OR scaffold)(keywords)} OR {(TISSUE SCAFFOLDS/(MeSHterm) OR (‘‘tissue scaffold*’’ OR scaffold*) (key-words)) AND (lipofill* OR lipotransfer* OR ‘‘fatgraft*’’ OR ‘‘adipo* stem cell*’’ OR ‘‘adipo* derivedstem cell*’’ OR ADSC) (keywords)}.
The search was restricted to the English language.Letters and review articles were excluded. The inclu-sion criteria incorporated the use of animplantable scaffold ± cellular therapy to engineertissue for the purpose of breast reconstruction. Articlesregarding the use of commercially available breastimplants were excluded, as the aim of the review was tohighlight methods that reconstruct the breast withautologous tissue only and avoid the implantation andhence complications of permanent foreign devices.
RESULTS
The systematic review identified 28 articles com-prising mainly of level five evidence in vitro and animalstudies, and two level four evidence human case series(Fig. 1). Current techniques have focussed on twodifferent biological scaffolds (eight articles; Table 1)and 13 synthetic scaffolds (fifteen articles; Table 2) tomimic the shape and support of native breast tissue.One article the scaffold material was not stated. A
Medline (Ovid)154 ar�cles
Embase (Ovid)289 ar�cles
319 ar�cles
124 duplicate ar�cles removed
28 ar�cles included in the systema�c
review
289 ar�cles excluded
FIGURE 1. A flow chart illustrating the database search andexclusion criteria to identify the articles included.
BIOMEDICALENGINEERING SOCIETY
DONNELY et al.10

TA
BL
E1.
Bio
log
ical
scaff
old
s:
syste
mati
cre
vie
wd
ata
extr
acti
on
.
Auth
ors
Title
Year
Journ
al
Stu
dy
aim
Stu
dy
model
Scaff
old
Scaff
old
—bio
logic
al/
synth
etic,
bio
/non-
bio
degra
dable
Volu
me/s
ize
of
scaff
old
Cell
thera
py
Cell
nic
he±
gro
wth
facto
r
Huss
and
Kra
t-z
Mam
mary
epithelia
lcell
and
adip
ocyte
co-c
ul-
ture
ina
3-D
matr
ix:
the
firs
tste
pto
ward
stissue-e
ngin
eere
dhum
an
bre
ast
tissue
2001
Cells
Tissues
Organs
To
culture
hum
an
mam
mary
epithelia
lcells
with
adip
ocyte
son
a3-D
bio
-lo
gic
alm
atr
ix
Invitro
model.
Colla
gen
gel
Bio
logic
al
Bio
degra
dable
Unknow
n—
gel
Hum
an
mam
-m
ary
epithe-
lialcells
with
adip
ose
tis-
sue
Dulb
ecco’s
modifi
ed
Eagle
sm
ediu
m(D
ME
M)
with
10%
feta
lcalf
seru
m(F
CS
)and
antibio
tics
DM
EM
/Ham
sF
12
with
in-
sulin
,tr
ansfe
rrin
,tr
i-io
doth
yro
nin
e,
hydro
cort
i-sone,
chole
rato
xin
,epithelia
lgro
wth
facto
r,7%
FC
S,
1.5
%adenin
eand
antibio
tics.
Tada
and
Fuji-
sato
Adip
ose
tissue
engin
eer-
ing
for
abre
ast
recon-
str
uction
(Confe
rence
abstr
act)
2012
Journalof
Tissue
Engineer-
ingand
Regenera-
tiveMedi-
cine
To
engin
eer
adi-
pose
tissue
usin
gdecellu
-la
rized
matr
ixobta
ined
from
rat
lungs
Invivo
anim
al
model
Ath
ym
icm
ice
Decellu
larized
rat
lungs.
Bio
logic
al
Bio
degra
dable
Unknow
nA
dip
ose
cell
line
3T
3-L
1A
circula
tory
culture
syste
m
Tsuji etal.
Sim
ple
and
longsta
ndin
gadip
ose
tissue
engi-
neering
inra
bbits
2012
Journalof
Artificial
Organs
To
engin
eer
long-
sta
ndin
gadi-
pose
tissue
without
FG
F2
Invivo
anim
al
model
New
Yeala
nd
white
rabbits
Poly
pro
pyle
ne
colu
mn
cage
with
pore
siz
e200um
Suspended
type
1col-
lagen
sponge
Synth
etic
and
Bio
-lo
gic
al
Bio
degra
dable
20
mm
dia
me-
ter
10
mm
thic
k-
ness
3.1
4m
Lcolla
-gen
sus-
pensio
n.
––
Debels
etal.
Susta
inable
fat
gra
ftin
g.
Optim
izin
gfa
tgra
ftin
gin
anin
vivo
tissue
engin
eering
cham
ber
model(C
onfe
rence
Abstr
act)
2013
Woundrepair
andregen-
eration
To
impro
ve
long
term
outc
om
eoffa
tgra
ftin
gby
addin
ga
novel
adip
ose
derived
matr
ix
Invivo
anim
al
model
Rat
model.
Adip
ose
derived
acellu
lar
matr
ic(A
DM
)
Bio
logic
al
Bio
degra
dable
2m
LM
inced
auto
lo-
gous
fat
Adip
ose
derv
ied
acellu
lar
matr
ix
Wang
etal.
Com
bin
ing
decellu
larized
hum
an
adip
ose
tissue
extr
acellu
lar
matr
ixand
adip
ose-d
erived
ste
mcells
for
adip
ose
tissue
engin
eering
2013
Acta
Bioma-
terialia
To
com
bin
ehD
AM
and
AD
SC
sfo
radip
ose
tissue
engin
eering
for
soft
tissue
de-
fect
repair
Invivo
anim
al
model
Nude
rat
mod-
el.
Decellu
larized
hum
an
adi-
pose
tissue
EC
M(h
DA
M)
Bio
logic
al
Bio
degra
dable
0.5
cm
91
cm
Hum
an
adi-
pose-d
erived
ste
mcells
hD
AM
Om
idi
etal.
Chara
cte
rization
and
assessm
ent
of
hyper-
ela
stic
and
ela
stic
pro
pert
ies
of
decellu
-la
rized
hum
an
adip
ose
tissues
2014
Journalof
Biome-
chanics
To
bio
mechani-
cally
chara
c-
terise
DA
Tscaff
old
sderived
from
various
adip
ose
depots
inth
ebody
Invitro
model.
Decellu
larized
adip
ose
tis-
sue
(DA
T)
Bio
logic
al
Bio
degra
dable
Unknow
n–
–
BIOMEDICALENGINEERING SOCIETY
Breast Reconstruction with a Tissue Engineering and Regenerative Medicine Approach 11

further four articles were identified that describe thereconstruction of the nipple areolar complex (Table 3).
DISCUSSION
Scaffolds
Since the idea of a tissue engineered breast was firstproposed, researchers have been analysing materialssuitable to use as an implantable scaffold that wouldsupport growth and allow regeneration of host tissue.An ideal scaffold would combine the key principles ofbiodegradability, low immunogenicity, porous archi-tecture and structural integrity. The scaffold compos-ites can broadly be categorized into biological scaffoldsand synthetic scaffolds.
Biological Scaffolds
Eight articles were identified that utilized a biolog-ical scaffold. All were biodegradable and could be sub-divided into two techniques; either a collagen basedscaffold as a gel or sponge, or a decellularized tissuebased scaffold created from adipose tissue, rat lungs orporcine mammary glands.
Collagen-Based
Huss and Kratz published the first step towardregenerating human autologous breast tissue on a 3-Dbiological matrix.22 Human mammary epithelial cellswith adipose tissue were cultured in vitro on collagengel. The typical growth pattern comprised largeepithelial patches of fibroblast-like shaped cells withpreadipocytes in between acquiring a round shape andaccumulating lipids with time. Cells require adhesivematerials in order to survive and type I collagen isknown to have an excellent porous structure; a suit-able scaffold for cell migration and proliferation.20
Utilizing a polypropylene cage implanted into thebilateral fat pads of rabbits and injecting a 3.14 mLsuspension of minced type I collagen sponge and sal-ine, a study reported significant adipogenesis filling92.8 ± 6.6% of the cage volume after 12 months.42
Significant volumes of adipose tissue had been gener-ated from surrounding tissue, along with the endoge-nous production of growth factors essential foradipogenesis and angiogenesis. These included fibrob-last growth factor-2 (FGF2), vascular endothelialgrowth factor (VEGF), platelet-derived growth factor(PDGF), epidermal growth factor (EGF) and insulin-like growth factor-1 (IGF-1), that were all detectable inthe wound drainage fluid. Although the polypropylenecage used was non-absorbable and too hard for breast
TA
BL
E1.
co
nti
nu
ed
Auth
ors
Title
Year
Journ
al
Stu
dy
aim
Stu
dy
model
Scaff
old
Scaff
old
—bio
logic
al/
synth
etic,
bio
/non-
bio
degra
dable
Volu
me/s
ize
of
scaff
old
Cell
thera
py
Cell
nic
he±
gro
wth
facto
r
Debels
etal.
Advances
inT
issue
Engi-
neering;
aN
ovel
Technol-
ogy
Makin
gU
se
of
an
invivo
Vascula
rized
Cham
ber
2015
Acta Chirur-
gicaBel-
gica
To
engin
eer
tissue
usin
gA
dip
ogel
and
an
art
eri-
ovenous
loop
within
aT
EC
Invivo
anim
al
model
Rat
model.
Adip
ose
derived
acellu
lar
matr
ix(A
DM
)(A
dip
ogel)
within
apoly
carb
onate
perf
ora
ted
hem
ispheric
cham
ber.
Bio
logic
al
Bio
degra
dable
2m
L–
Adip
ose
derv
ied
acellu
lar
matr
ix
Gia
tsid
isB
reast
tissue
engin
eering:
Decellu
larized
scaff
old
sderived
from
porc
ine
mam
mary
gla
nds
(Confe
r-ence
abstr
act)
2015
Journalof
the
Ameri-
canCol-
legeof
Sur-
geons
To
investigate
the
eff
ectiveness
of
decellu
larizin
gporc
ine
mam
-m
ary
gla
nds
Invitro
model.
Decellu
larized
porc
ine
mam
mary
gla
nds
Bio
logic
al
Bio
degra
dable
20
cm
940
cm
93
cm
––
BIOMEDICALENGINEERING SOCIETY
DONNELY et al.12

TA
BL
E2.
Syn
theti
cscaff
old
s:
syste
mati
cre
vie
wd
ata
extr
acti
on
.
Auth
ors
Title
Year
Journ
al
Stu
dy
aim
Stu
dy
model
Scaff
old
Scaff
old
—bio
logic
al/
synth
etic,
bio
/non-
bio
degra
dable
Volu
me/s
ize
of
scaff
old
Cell
thera
py
Cell
nic
he±
gro
wth
facto
r
Choetal.
Engin
eering
of
volu
me-
sta
ble
adip
ose
tissues
2004
Biomaterials
To
engin
eer
adi-
pose
tissue
usin
gm
echani-
calsupport
str
uctu
res
Invivo
ani-
mal
mod-
el
Ath
ym
icm
ice.
Dom
eshaped
sup-
port
str
uctu
refo
rmed
of
Poly
(gly
colic
acid
)(P
GA
)and
Poly
(L-lactic
acid
)(P
LLA
).
Synth
etic
Bio
degra
dable
0.1
2cm
3H
um
an
Pre
-adip
ocyte
sT
hro
mbin
—fibrinogen
solu
tion
with
hep-
arin
(form
ing
afib-
rin
gel)
Basic
fibro
bla
st
gro
wth
facto
r(b
FG
F).
Choetal.
Engin
eere
dadip
ose
tis-
sue
form
ation
en-
hanced
by
basic
fibro
bla
st
gro
wth
fac-
tor
and
am
echanic
ally
sta
ble
environm
ent
2007
CellTransplan-
tation
To
enhance
adi-
pose
tissue
regenera
tion
by
com
bin
ing
am
echanic
al
support
with
bF
GF
Invivo
ani-
mal
mod-
el
Ath
ym
icm
ice.
Dom
eshaped
sup-
port
str
uctu
refo
rmed
of
Poly
(gly
colic
acid
)(P
GA
)and
Poly
(L-lactic
acid
)(P
LLA
).
Synth
etic
Bio
degra
dable
0.1
2cm
3H
um
an
Pre
-adip
ocyte
sT
hro
mbin
—fibrinogen
solu
tion
with
hep-
arin
(form
ing
afib-
rin
gel)
Basic
fibro
bla
st
gro
wth
facto
r(b
FG
F).
Fin
dla
yetal.
Tis
sue-e
ngin
eere
dbre
ast
reconstr
uction:
bridgin
gth
egap
to-
ward
larg
e-v
olu
me
tis-
sue
engin
eering
inhum
ans
2011
Plasticand
Reconstruc-
tiveSurgery
To
engin
eer
tis-
sue
togeth
er
with
asupport
-iv
evascula
ture
ina
larg
eani-
malm
odel
Invivo
ani-
mal
mod-
el
Porc
ine.
Perf
ora
ted
poly
car-
bonate
cham
ber
with
apoly
(L-
lactide-c
o-g
ly-
colid
e)
sponge
inhalf
the
cham
bers
.
Synth
etic
Bio
degra
dable
78.5
mL
5m
Ladip
ose
tissue
flap
–
Hett
iara
chic
hi
etal.
The
eff
ects
ofbio
physic
al
and
bio
chem
ical
envi-
ronm
ent
on
pre
-adip
ocyte
diffe
rentia-
tion
(Confe
rence
abstr
act)
2012
JournalofTis-
sueEngi-
neeringand
Regenera-
tiveMedi-
cine
To
investigate
the
eff
ect
of
scaf-
fold
stiff
ness
on
adip
ocyte
dif-
fere
ntiation
Invitro
mod-
el.
Poly
acry
lam
ide
gel
Synth
etic
Bio
degra
dable
Unknow
n3T
3-L
1cells
Norm
alor
adip
ogenic
media
Shpais
man
etal.
One-s
tep
synth
esis
of
bio
degra
dable
cur-
cum
in-d
erived
hydro
-gels
as
pote
ntialsoft
tissue
fille
rsaft
er
bre
ast
cancer
surg
ery
2012
BioMacro-
molecules
To
develo
pa
cur-
cum
in-d
erived
hydro
gelfo
ruse
as
asoft
tissue
fille
rand
dru
gdeliv
ery
syste
m
Invitro
mod-
el.
Curc
um
in-d
erived
hydro
gel.
(Non-
toxic
Poly
(-eth
yle
ne
gly
col)
and
desam
ino-
tyro
syl-ty
rosin
eeth
yleste
r)
Synth
etic
Bio
degra
dable
Unknow
n-
Hydro
gel
––
Chhayaetal.
Susta
ined
regenera
tion
of
hig
h-v
olu
me
adi-
pose
tissue
for
bre
ast
reconstr
uction
usin
gcom
pute
raid
ed
de-
sig
nand
bio
manufa
c-
turing
2015
Biomaterials
To
investigate
PD
LLA
scaf-
fold
sfo
rpote
n-
tialto
engin
eer
hig
hvolu
me
adip
ose
tissue
Invivo
ani-
mal
mod-
el
Ath
ym
icnude
rats
.
Poly
(D,L
)-Lactide
poly
mer
(PD
LLA
).
Synth
etic
Bio
degra
dable
3cm
3H
um
an
um
bili
cal
cord
perivascula
rcells
for
6w
eeks.
Then
hum
an
um
bili
calvein
endoth
elia
lcells
(HU
VE
Cs).
Thro
mbin
—fibrinogen
solu
tion.
BIOMEDICALENGINEERING SOCIETY
Breast Reconstruction with a Tissue Engineering and Regenerative Medicine Approach 13

TA
BL
E2.
co
nti
nu
ed
Auth
ors
Title
Year
Journ
al
Stu
dy
aim
Stu
dy
model
Scaff
old
Scaff
old
—bio
logic
al/
synth
etic,
bio
/non-
bio
degra
dable
Volu
me/s
ize
of
scaff
old
Cell
thera
py
Cell
nic
he±
gro
wth
facto
r
Chhaya
etal.
Tra
nsfo
rmation
of
Bre
ast
Reconstr
uctionvia
Additiv
eB
iom
anufa
c-
turing
2016
ScientificRe-
ports(N
a-
ture)
To
assess
pre
-vascula
riza-
tion
and
adi-
pose
tissue
gro
wth
with
aP
CL
scaf-
fold
Invivo
anim
al
model
Imm
unocom
pete
nt
min
ipig
s.
Medic
algra
de
poly
capro
lac-
tone
(mP
CL).
Synth
etic
Bio
degra
dable
75
cm
3A
uto
logous
lipoaspirate
–
Morr
ison
etal.
Cre
ation
of
aLarg
eA
di-
pose
Tis
sue
Constr
uct
inH
um
ans
Usin
ga
Tis
sue-e
ngin
eering
Cham
ber:
AS
tep
For-
ward
inth
eC
linic
al
Applic
ation
of
Soft
Tis
sue
Engin
eering
2016
EBioMedicine
To
engin
eer
larg
eclin
i-cally
rele
-vant
vol-
um
es
of
adip
ose
tis-
sue
infe
-m
ale
patients
with
aT
EC
and
fat
flap
Invivo
hum
an
case
series
Wom
en
with
pre
vi-
ous
masec-
tom
ies.
Dom
eshaped,
hollo
w,
3m
mth
ick
perf
ora
ted
acry
liccham
-bers
.
Synth
etic
Non-b
iodegra
dable
140-3
60
mL
(custo
mm
ade)
Thora
codors
al
art
ery
perf
o-
rato
r(T
AP
)fa
tflap.
–
Wuetal.
Self-A
ssem
blin
gR
AD
A16-I
Peptide
Hydro
gelS
caff
old
Loaded
with
Tam
ox-
ifen
for
Bre
ast
Recon-
str
uction
2017
BioMedRe-
search
International
To
com
bin
eta
moxifen
and
apep-
tide
scaff
old
for
use
as
asoft
tissue
fille
rand
dru
gdeliv
ery
syste
m
Invivo
anim
al
model
Ath
ym
icm
ice.
Tam
oxifen
loade-
d—
RA
DA
16-I
peptide
hydro
-gel
Synth
etic
Bio
degra
dable
Un- know
n—
H-
ydro
gel
Hum
an
adi-
pose-d
erived
ste
mcells
(hA
DS
Cs)
Hig
h-g
lucose
DM
EM
supple
mente
dw
ith
10%
FB
S,
dexam
-eth
asone,
isobuty
l-m
eth
ylx
anth
ine,
in-
sulin
,in
dom
eth
acin
.
Xuetal.
Self-a
ssem
blin
gR
AD
A16-I
peptide
hy-
dro
gels
caff
old
loaded
with
tam
oxifen
for
bre
ast
reconstr
uction
follo
win
glu
mpecto
my
(Confe
rence
abstr
act)
2017
ClinicalThera-
peutics
To
com
bin
eta
moxifen
and
apep-
tide
scaff
old
for
use
as
asoft
tissue
fille
rand
dru
gdeliv
ery
syste
m
Invivo
anim
al
model
Ath
ym
icm
ice.
Tam
oxifen
loade-
d—
RA
DA
16-I
peptide
hydro
-gel
Synth
etic
Bio
degra
dable
Un- know
n—
H-
ydro
gel
Hum
an
adi-
pose-d
erived
ste
mcells
(hA
DS
Cs)
–
Xia
o etal.
Pre
-shaped
larg
e-v
olu
me
engin
eere
dvascula
r-iz
ed
pedic
led
adip
ose
flaps
ina
rabbit
model:
Atw
osta
ge
tissue
engin
eering
cham
ber-
based
pro
cedure
(Full
Text
not
availa
ble
)
2017
JournalofBio-
materials
andTissue
Engineering
To
engin
eer
adip
ose
tis-
sue
usin
ga
TE
Cand
adip
ose
flaps
Invivo
anim
al
model
Rabbits.
Tis
sue
Engin
eer-
ing
Cham
ber
(TE
C);
un-
know
nm
ate
rial
Synth
etic
Non-b
iodegra
dable
Unknow
nA
dip
ose
flaps
(0.8
mL)
with
vesselpedi-
cle
–
BIOMEDICALENGINEERING SOCIETY
DONNELY et al.14

TA
BL
E2.
co
nti
nu
ed
Auth
ors
Title
Year
Journ
al
Stu
dy
aim
Stu
dy
model
Scaff
old
Scaff
old
—bio
logic
al/
synth
etic,
bio
/non-
bio
degra
dable
Volu
me/s
ize
of
scaff
old
Cell
thera
py
Cell
nic
he±
gro
wth
facto
r
Rossietal.
Decora
tion
of
RG
D-m
imetic
poro
us
scaff
old
sw
ith
engin
eere
dand
devital-
ized
extr
acellu
lar
matr
ixfo
radip
ose
tissue
regen-
era
tion
2018
Acta
Biomate-
rialia
To
cre
ate
ahybrid
scaff
old
form
ed
of
asynth
etic
poly
mer
and
decellu
lar-
ized
tissue
Invivo
anim
al
model
Ath
ym
icm
ice.
Hybrid
EC
M-O
PA
AF
scaff
old
EC
Mfr
om
decellu
lar-
ized
hA
SC
sO
PA
AF
—R
GD
-mim
etic
poly
(am
idoam
ine)
olig
om
er
macro
p-
oro
us
foam
.
Synth
etic
and
bio
-lo
gic
al
Bio
degra
dable
8m
mdia
me-
ter
3m
mth
ick-
ness.
–In
itia
llyF
GF
-2,
in-
sulin
,dexam
-eth
asone,
in-
dom
eth
acin
,IB
MX
prior
todecellu
lariza-
tion
O’H
allo
ran
etal.
Evalu
ating
anoveladip
ose
tissue
engin
eering
str
at-
egy
for
bre
ast
recon-
str
uction
post-
maste
cto
my.
(Confe
r-ence
Abstr
act)
2018
IrishJournalof
MedicalSci-
ence
To
assess
the
oncolo
gic
al
safe
tyof
AD
SC
shar-
veste
dfr
om
patients
fol-
low
ing
chem
oth
era
py
Invitro
model
Hydro
gels
of
2%
w/v
hyalu
ronic
acid
(29
cro
sslin
kin
gdensity
loaded
with
adip
o-
cyte
sat
6.7
%to
tal
gelvolu
me)
Synth
etic
Bio
degra
dable
Un- know
n—
H-
ydro
gel
Adip
ose
De-
rived
Ste
mC
ells
(AD
S-
Cs)
–
Gerg
es
etal.
Explo
ring
the
pote
ntialof
poly
ure
thane-b
ased
soft
foam
as
cell-
free
scaff
old
for
soft
tissue
regenera
-tion
2018
Acta
Biomate-
rialia
To
assess
the
bio
mechani-
caland
physio
chem
ical
pro
pert
ies
of
apoly
-ure
thane-b
ased
scaff
old
and
adip
ose
tissue
gen-
era
tion
Invivo
anim
al
model
CD
1fe
-m
ale
mic
e
Poly
(ure
thane)-
based
scaff
old
sS
ynth
etic
Bio
degra
dable
8m
mdia
me-
ter
4m
mth
ick-
ness.
––
Leong
etal.
ReF
ilx-s
ynth
etic
bio
degra
d-
able
soft
tissue
fille
rsfo
rbre
ast
conserv
ing
sur-
gery
inbre
ast
cancer
(Confe
rence
abstr
act)
2018
CancerRe-
search
To
evalu
ate
ReF
ilxas
asoft
tissue
fille
rfo
rbre
ast
conserv
ing
surg
ery
de-
fects
Invivo
anim
al
model
Yucata
nm
inip
-ig
s.
Poly
ure
thanes
(am
ino-
acid
based)
Synth
etic
Bio
degra
dable
Un- know
n—
h-
ydro
gel
––
Kaufm
an
etal.
Inte
rim
report
of
aclin
ical
regis
try:
669
patients
im-
pla
nte
dw
ith
a3-d
bio
ab-
sorb
able
mark
er
(Confe
rence
abstr
act)
2018
Annals
ofSur-
gicalOncol-
ogy
Inte
rim
report
tosum
marize
data
colle
cte
din
an
IRB
-appro
ved
Regis
try
Invivo
hum
an
case
series.
3-D
bio
absorb
able
impla
nt
(unknow
nm
ate
rial)
Unknow
nB
iodegra
dable
Unknow
n–
–
BIOMEDICALENGINEERING SOCIETY
Breast Reconstruction with a Tissue Engineering and Regenerative Medicine Approach 15

TA
BL
E3.
Nip
ple
are
ola
rco
mp
lex
scaff
old
s:
syste
mati
cre
vie
wd
ata
extr
acti
on
.
Auth
ors
Title
Year
Journ
al
Stu
dy
aim
Stu
dy
model
Scaff
old
Scaff
old
—bio
logic
al/
synth
etic,
bio
/non-
bio
degra
dable
Cell
thera
py
Cell
nic
he±
gro
wth
facto
r
Cao etal.
Tis
sue-e
ngin
eere
dnip
ple
reconstr
uction
1998
Plasticand
Reconstruc-
tiveSurgery
To
tissue
engin
eer
auto
lo-
gous
cart
ilage
inth
eshape
of
ahum
an
nip
ple
Invivo
anim
al
model
Porc
ine.
Plu
ronic
F-1
27
hydro
gel(p
oly
-eth
yle
ne
oxid
eand
poly
pro
py-
lene
oxid
ecopoly
mer)
.
Synth
etic
Non-b
iodegra
dable
(Scaff
old
dis
-solv
es
over
tim
e).
Auto
logous
chro
n-
dro
cyte
s.
–
Tie
rney
etal.
Bio
logic
colla
gen
cylin
der
with
skate
flap
techniq
ue
for
nip
-ple
reconstr
uction
2014
PlasticSurgery
International
To
reconstr
uct
the
nip
ple
usin
ga
bio
logic
colla
gen
cylin
der
with
skate
flap
Invivo
hum
an
case
series.
Rolle
dcylin
der
of
EC
Mcolla
gen
derived
from
por-
cin
esm
all
inte
sti-
nalsubm
ucosa
Bio
logic
al
Bio
degra
dable
––
Pashos
etal.
Atissue
engin
eere
dnip
ple
and
are
ola
com
ple
x(C
onfe
rence
abstr
act)
2015
Molecular
Therapy
To
desig
na
scaff
old
form
ed
of
adecellu
larized
whole
NA
Cfo
rtissue
engin
eer-
ing
Invivo
anim
al
model
Rhesus
Maca-
que
Non-
hum
an
pri-
mate
s.
Decellu
larized
NA
CB
iolo
gic
al
Bio
degra
dable
Rhesus
bone
mar-
row
-derived
ste
mcells
–
Pashos
etal.
Chara
cte
rization
of
an
acellu
lar
scaff
old
for
atissue
engi-
neering
appro
ach
toth
enip
ple
–are
ola
rcom
ple
xre
constr
uction
2017
Cells
Tissues
Organs
To
cre
ate
anonim
munogenic
scaff
old
from
adecellu
lar-
ized
NA
Cfo
ruse
as
an
onla
ygra
ftth
at
ispatient
specifi
c
Invivo
anim
al
model
Rhesus
Maca-
que
Non-
hum
an
pri-
mate
s.
Decellu
larized
NA
CB
iolo
gic
al
Bio
degra
dable
Bone
mar-
row
-derived
mes-
enchym
alste
mcells
(BM
SC
s)
from
rhesus
ma-
caques
a-m
odifi
ed
Eagle
sm
ed-
ium
(feta
lbovin
eser-
um
,L-g
luta
min
e,
penic
illin
,str
epto
-m
ycin
,am
phote
ricin
BIOMEDICALENGINEERING SOCIETY
DONNELY et al.16

reconstruction, continuing the search for the appro-priate scaffold.
Decellularized Tissue
The search began to look at the concept of decel-lularizing tissue; using a solution to completely removethe cellular component leaving only the extracellularmatrix (ECM) to form a scaffold. Tada and Fujisato40
showed that rat lungs could be decellularized, injectedwith adipocytes and implanted into nude mice. Severalresearchers developed protocols for decellularizingadipose tissue11,32,40,43; decellularized adipose tissue(DAT), decellularized human adipose tissue ECM(hDAM) or adipose derived acellular matrix (ADM).To aid adipocyte infiltration and proliferation into thescaffold, and overall structure of the reconstructedbreast, it is crucial that the scaffold have similarbiomechanical properties and deformability to that ofnative breast tissue. Omidi et al.32 showed that DATscaffolds sourced from different areas of femalepatients (breast, subcutaneous abdominal region,omentum, pericardial depot or thymic remnant) all
exhibited linear elastic and hyperelastic propertiesalike, and were consistent with the previously reportedYoung’s modulus of adipose breast tissue36; an averagevalue of 3250 ± 910 Pa. Advantageously this wouldmean the DAT scaffolds could be sourced from any ofthe areas for commercial use and would demonstratesimilar stiffness and deformability as a natural breastunder gravity loading from prone to supine bodypositions.
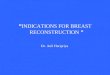
Subcutaneously implanting the hDAM scaffolds(0.5 cm 9 1 cm) in a nude rat model exhibited aminimal inflammatory response after 30 days withoutobvious rejection, with initially well vascularizedgrafts.43 However from week 2 to 8, there was a sig-nificant decrease in graft vascularization; this wasthought due to a gap still present between the scaffoldand native adipose tissue. To improve graft vascular-ization, a femoral arteriovenous loop was trialled in-side a perforated tissue engineering chamber (TEC;formed of polycarbonate) containing 2 mL of ADMtermed ‘‘Adipogel’’ using a rat animal model.11 Atboth 6 and 12 weeks post implantation, the chambers
FIGURE 2. H&E stained cross sections demonstrating tissue scaffold. (a, b) At 6 weeks. avl = arteriovenous loop. The arrowsdemonstrate areas of tissue growth within the nubbins of the TEC and the diamond areas of un-remodeled Adipogel. (b) the brownstaining demonstrating viable fat cells. (c, d) exhibit scaffold at 12 weeks with substantially more viable adipose tissue. SourceDebels11
BIOMEDICALENGINEERING SOCIETY
Breast Reconstruction with a Tissue Engineering and Regenerative Medicine Approach 17

were half filled with well vascularized connective tissue(0.946 mL ± 0.161), but only containing 135 lL ± 76adipocytes along with some myocytes. The adiposetissue appeared to be away from the arteriovenousloop at the outer margin of the TEC, while muscle cellgrowth was at the arteriovenous loop origin near theinguinal-abdominal muscle intersection (Fig. 2). De-bels hypothesized this is either due to migrating stemcells or cell-to-cell signaling pathways from local nativetissue. Meanwhile all chambers demonstrated animmunological reaction and were encased by anexternal fibrotic capsule. Giatsidis19 took the decellu-larization concept further, applying the technique toporcine mammary glands. The resultant scaffold pre-served original morphology with histological analysisresembling native architecture of ECM and vascu-lar/ductal networks. This study also demonstrated thebenefit of harvesting adjacent glands together andmolding the scaffold to the required shape.
The major limitations of biological scaffolds includerapid enzymatic and hydrolytic degradation, alongwith a strong immunogenic response in vivo. Tech-niques have been developed to decrease the rate ofdegradation, such as enzymatic pre-treatment or cross-linking using various agents, which improve robustnessand maintain integrity; however the effectiveness canvary.30 A key requirement of the scaffold is to providemechanical support during regeneration until the tissueis mature enough to support itself, which unfortunatelybiological materials have been unable to guarantee.Hence current research is now focussing on utilizingsynthetic polymers.
Synthetic Scaffolds
Fifteen articles were identified that utilized syntheticscaffolds, with 13 different techniques. These com-prised of eleven biodegradable scaffolds and two non-biodegradable tissue engineering chambers (TEC) thatare to be removed once the tissue has generated.
The majority of these scaffolds are synthesized fromthermoplastic polymers and can be further sub-divideddepending on their structure; either a hydrogel filler ora solid structural support.
Hydrogel Structure
As with biological scaffolds, the biomechanical andbiochemical environment of synthetic scaffolds influ-ences adipocyte migration and proliferation. Het-tiarachichi et al.21 were investigating the stiffness of apolyacrylamide gel and effect on adipocyte differenti-ation in vitro. The most favourable matrices were thosethat had a similar stiffness to endogenous adipose tis-sue; Young’s moduli above 4.1 kPa elicited maximal
spreading of adipose cells, while moduli below 4.1 kPaa more spherical phenotype.
Along with providing a soft tissue support to re-place breast tissue, the idea that hydrogels could beused as drug delivery systems was hypothesized. Cur-cumin-derived hydrogels were synthesized frompoly(ethylene glycol) (PEG) and desaminotyrosyl-ty-rosine ethyl ester (DTE), that upon hydrogel degra-dation led to local release of active curcumin (CUR).37
Through a condensation polymerization protocol,different compositions of hydrogel could be synthe-sized that altered its overall properties, including cur-cumin concentration and swelling ability;CUR50PEG50 exhibited the most favourable withstable curcumin release and compression moduluscomparable with native breast tissue. In vitro analysisdemonstrated selective cytotoxicity against breastcancer cells, but no cytotoxicity to noncancerous pri-mary human dermal fibroblasts, further suggestingpromising use as a bioactive void filler for excisedcancerous tissue.
Additional attempts to engineer artificial therapeu-tic breast tissue led to the efficacious incorporation oftamoxifen into a self-assembled injectable polypeptide,RADA16-I.44 The hydrogel scaffold provided supportfor cell attachment and proliferation, with resultssuggesting the 3D environment enhanced toxicity oftamoxifen on breast cancer cells, while reducing theeffect on human adipose derived stem cells (hADSCs).After subcutaneous implantation into nude mouseanimal models, the scaffold formed a round mass withregular shape and clear edge, retaining its shape uponcompression. Although the scaffold was completelydegraded and absorbed within 7 days in vivo, high-lighting long-term persistence as the major challenge.For the time being, therapeutic benefits of bioactiveimplants in human based studies are limited inoncoplastic surgery, only providing tissue support anda tumor bed target for radiation therapy.25
Poly(urethane)-based scaffolds have shown promisefor use as hydrogel fillers to restore breast volume.18,27
A polyurethane-based soft foam (PUF) demonstratedfatigue resistance and tuneable mechanical propertiesby adjusting the ratio of poly(ethylene glycol) (PEG) topolyester (PE) segments. The optimum balance shownto be PUF 3/10 (PEG/PE) enhanced the hydrophiliccharacter of the scaffold, favouring efficacious diffu-sion of body fluids. Although degradation kineticsshowed after 6 months loss of more than 50% originalweight. In vivo the undifferentiated mesenchymal cellsattached themselves to the periphery of the scaffold,gradually infiltrating toward the centre. By day 91,initial loose fibromyxoid tissue had been partially re-placed by mature adipose tissue. Expectedly the scaf-
BIOMEDICALENGINEERING SOCIETY
DONNELY et al.18

fold elicited a foreign body reaction, although only apartial fibrous capsule was noted up to 3 months.
Solid Structure
Several solid dome shaped support structures syn-thesized from polymers have been analysed. Choet al.9,10 indicated that a mechanically stable environ-ment is crucial to maintain engineered tissue volume,creating a poly(glycolic acid) matrix (PGA) coated inpoly(L-lactic acid) (PLLA). The structure was formedby molding strips of PGA mesh and then immersing inPLLA, and was able to withstand compressive forces,maintaining stable in vivo volume (0.12 cm3) at6 weeks. Although the domed structure was hollow,minimizing surface area for cell attachment whichwould make engineering large volumes of tissue diffi-cult.
A 3D printer has been utilized to design and create apoly(D,L)-lactide polymer (PDLLA) scaffold,8 allowingthe ability to customise size and shape of the engi-neered breast. Internal morphology of the scaffold,including porosity and pore size, can be tailored toindividual patients. The PDLLA scaffold (volume3 cm3) withstood contraction forces for at least6 months in vivo (nude rat model) and did not exhib-ited any mass loss. Pore sizes of 1.5 mm allowed fortissue and vascular ingrowth, with 81% of the overalltissue at 24 weeks composed of adipose tissue; themajority being host-derived adipocytes. Scaffolds wereassociated with minimal inflammatory reaction, inte-grating into the host body and surrounded by a fibroticcapsule that decreased as the scaffold degraded.
Chhaya et al.7 went on to develop another custom-made scaffold (volume 75 cm3), using medical-gradepolycaprolactone (mPCL) through additive biomanu-facturing. On the contrary to previous designs, theslowly degrading mPCL scaffold had a stiffness valuethree orders of magnitude higher than that of native
breast tissue, hypothesizing that newly regeneratedadipose tissue needed protection from compressive andshear forces until it had matured. Scaffolds were im-planted into immunocompetent minipigs and alloweda period of prevascularization before cellular addition(Fig. 3). Prevascularization allowed a platelet-richfibrin blood clot to form inside the large pore network,stimulating angiogenesis and the production of a wellvascularized connective tissue. It was hypothesizedthat altering the initial scaffold treatment protocol(empty scaffold vs. prevascularization plus cellularaddition) could modify the composition of connectivetissue to adipose tissue, tailoring the procedure foraesthetic augmentation or breast reconstruction. Uponexplantation there were no major signs of inflamma-tion within the tissue section or scaffolds, howeverthere were low-grade granulomatous reactionslocalized around the scaffold. The role of macrophagesis not fully understood, however Chhaya et al. stipu-late it could contribute to angiogenesis, with priorresearch potentially linking the two via the secretion ofvascular endothelial growth factor (VEGF) and pla-telet derived growth factor (PDGF).39
The major disadvantage of synthetic scaffoldscompared to biological scaffolds when seeding with celland tissue components is the lower cellular affinity tothe synthetic material. To improve this, Rossi et al.35
has attempted to combine the functionalities of asynthetic polymer with a biological matrix to engineera hybrid scaffold; although this would increase the costand complexity of the biomaterial. A RGD-mimeticpoly(amidoamine) oligomer microporous foam(OPAAF) was created by free radical polymerization.The hydrophilic 3D interconnected porous networkwas decorated and then decellularized to generate ahybrid adipose ECM-OPAAF construct (Fig. 4a). Thestudy describes an effective decellularization protocolthat maintains ECM architecture. While the original
FIGURE 3. ‘‘Overall concept of the prevascularization and delayed fat injection concept.’’ An empty scaffold is implanted onto thechest wall, and after a period of prevascularization, lipoaspirate is injected into the construct. Source: Chhaya et al.7
BIOMEDICALENGINEERING SOCIETY
Breast Reconstruction with a Tissue Engineering and Regenerative Medicine Approach 19

OPAAF scaffold had similar mechanical properties tothat of native adipose tissue, the hybrid ECM-OPAAFconstruct had a Young’s modulus of more than dou-ble; 10.5 ± 3.4 kPa. In vitro and in vivo analysisdemonstrated a strongly enhanced adipoinductivecapacity as a result of ECM decoration, with an in-crease of infiltrating native adipocytes (Figs. 4g and4p). The interfacial biocompatibility between host andscaffold was difficult to evaluate in the immunocom-petent mouse model, with a strong immune responseagainst the human ECM. Although in vitro co-culturewith human peripheral blood exhibited a more pro-regenerative macrophage response.
As with biological scaffolds, vascularization of alarge volume of regenerated tissue in synthetic scaf-folds has been one of the main limiting variables.Utilizing previous knowledge, a small experimental piganimal study focussed on the co-development of adi-pose tissue alongside a supportive vasculature.14
Pedicled fat flaps based on superficial circumflex iliacvessels were inserted into tissue engineering chambers(TEC; perforated polycarbonate) together with apoly(L-lactide-co-glycolide) (PLGA) sponge (volume78.5 mL). At 22 weeks (12 weeks after chamber re-moval) the initial 5 mL adipose tissue flaps had ex-
panded into a larger core of 56.5 mL adipose tissuesurrounded by a fibrous capsular rim, with growthassociated with adipocyte hyperplasia. One constructwas even transferred and survived on its pedicle in anadjacent submammary pocket. Even though the studyhas a small sample and no control group to comparethe PLGA sponge, it provides proof of principle thetechnique can be used on a larger scale.
The concept was further demonstrated in a rabbitanimal model.45 An 8 mL volume TEC was implantedsubcutaneously with a vessel pedicled 0.8 mL adiposeflap inserted. The flaps expanded containingadipose tissue within and after TEC removal at8 weeks, growth continued until stabilization at weeks12–24.
The proof of concept led to the creation of a largevolume of adipose tissue construct in humans.29 Astudy of five women who had had previous mastec-tomies incorporated a thoracodorsal artery perforator(TAP) fat flap within a TEC (perforated acrylic) (vol-ume 140–360 mL) under a submuscular plane (Fig. 5).At 6 months follow-up the TECs were removed. Whileonly successful in one patient, 210 mL of newly formedtissue with ‘‘macroscopic appearance and palpabletexture very similar to native adipose tissue’’ (Fig. 6)
FIGURE 4. (a) The decellularization protocol. (b–e) The scanning electron microscope (SEM) analysis of the constructs (scalebars: 100 lm for (b and c) 10 lm for (d and e)). (f) Successful decellularization with a reduction in DNA content. (g, p) The adipocyteinfiltration at 2 weeks and 4 weeks post implantation respectively. The hybrid ECM-OPAAF construct shows superioradipoinductive capacity. Source Rossi et al.35
BIOMEDICALENGINEERING SOCIETY
DONNELY et al.20

provides evidence of the feasibility of a tissue engi-neering approach in humans.
Nipple–Areolar Complex
Even though the focus of this systematic review ison reconstructing the breast, the literature search re-turned four articles investigating the nipple-areolarcomplex (NAC) and it was deemed imperative to
mention. Thankfully nipple-sparing mastectomy isbecoming increasingly more common however noveltissue engineering reconstructive techniques must becompatible with both nipple-sparing and non-nipple-sparing techniques. The scaffold composites includedone collagen based, two decellularized tissue based andone thermoplastic polymer based.
Previously breast reconstruction had been aimed atimproving cosmesis and symmetry of female form withclothes on. Eventually more attention was attributedto the NAC to improve naked female form and skinflaps were constructed that could also be tattooed forpigmentation.38
As with the breast, a tissue engineering approachhas been proposed. Cao et al.5 described a simpletechnique by injecting a pluronic F-127 hydrogel see-ded with autologous chondrocytes into a swine animalmodel. Surrounded by a purse string suture led to thegeneration of stable cartilage tissue that at 10 weeksclosely resembled a NAC.
Additional attempts now include a rolled cylinder ofcollagen derived from the submucosa of porcine smallintestine being used in conjunction with a skate flap ina human based study.41 The outcome at the time ofsurgery ranged from 6 to 7 mm nipple projection, witha 30–50% loss at 6 months.
FIGURE 5. (a) demonstrates the 210 cm3 TEC. (b–d) The TAP fat flap design, the surgical procedure and the final result prior toclosing. Source Morrison et al.29
FIGURE 6. At 12 months, the tissue generated exhibitsadipose tissue covered by a fibrous capsule. SourceMorrison et al.29
BIOMEDICALENGINEERING SOCIETY
Breast Reconstruction with a Tissue Engineering and Regenerative Medicine Approach 21

Alternatively a decellularized NAC seeded withautologous cells to be used as an onlay graft is in initialstages of testing.33 The in vitro report demonstratespreservation of the NAC primary structures on amicroscopic scale with an effective decellularizationprotocol. Reseeding of the scaffolds with bone mar-row-derived mesenchymal stem cells exhibited initialattachment to the periphery, with cells migrating dee-per into the scaffold by day 7; 91% cell viability at 48 hand 67% undergoing proliferation by day 7.
Cellular Therapy and Growth Factors
The idea is to regenerate host tissue to replace ex-cised breast tissue and provide soft tissue support. Sofar different materials and properties of scaffolds havebeen characterized. The scaffold needs to providestructural integrity until regenerated tissue has ma-tured to support itself, upon which the scaffold de-grades (or is removed) leaving only host tissue. Thereare two main hypothesises to regenerate tissue withinscaffolds. Either scaffolds provide the space and envi-ronment for surrounding native cells to migrate intothe scaffold and proliferate or cells, ideally autologousto prevent immunogenicity, are implanted into scaf-folds and proliferate.
Fifteen of the aforementioned articles investigatedincorporation of cellular therapy to improve adipoge-nesis, including bone marrow derived stem cells, adi-pose derived stem cells (ADSCs), preadipocytes andlipoaspirate. Along with this, eight included use ofculture medium containing growth factors and pro-teins. While only one article evaluated the effect of aspecific growth factor and compared this with a con-trol group.
Chhaya et al.7 hypothesized that initial scaffoldtreatment strategy could be tailored according to theindication for the surgical procedure. An empty scaf-fold for post-mastectomy breast reconstruction wouldallow native cells to migrate in and generate organizedconnective tissue, avoiding risk of breast cancerrecurrence from using adipose progenitor cells. Whileimplanting autologous lipoaspirate into scaffolds foraesthetic breast augmentation would allow generationof higher composition of adipose tissue to connectivetissue, 47.32% ± 4.12, maintaining natural tactilesensation and mimicking morphology of the breast.
Others have likewise discovered that implantingautologous lipoaspirate into the scaffold resulted in thesignificant increase of viable adipose tissue12; althoughthe majority of originally inserted adipocytes had died,indicating neoadipogenesis. This can occur due to thepresence of adipose derived stem cells (ADSCs) withinlipoaspirate, being first isolated and reported by Zuket al.46 ADSCs are multipotent with potential to dif-
ferentiate into adipose tissue, osteocytes, chondrocytesor myocytes when cultured in the presence of specificdifferentiation factors. To direct ADSCs toward theadipose lineage in vitro, they can be cultured in high-glucose Dulbecco’s modified Eagle’s medium(DMEM) supplemented with 10% fetal bovine serum,dexamethasone, isobutylmethylxanthine, insulin andindomethacin.44 Though there is potential risk of im-planted ADSCs stimulating breast cancer recurrence,ADSCs have been isolated from breast tissue and ab-domen of patients treated with neoadjuvantchemotherapy and demonstrated better adipogenicpotential and improved oncological safety withdecreased expression of cancer driver genes.31
Once implanted, a trial studied the effect of a fibringel containing basic fibroblast growth factor (bFGF),concluding there was a significant increase in pre-adipocyte cell survival, neovascularization and volumeof generated adipose tissue when compared to a con-trol group.9 Cho et al. hypotheses two mechanisms forenhanced adipogenesis. Firstly that neovascularizationin fibrin gel may be enhanced by bFGF, leading tofactors secreted from vasculature endothelial cells thatare known to promote adipocyte precursors to migrateand proliferate.1,16 Secondly that bFGF may directlystimulate implanted preadipocytes to differentiate intoadipocytes.
Other factors effecting cell migration and prolifer-ation include the environment surrounding the cells,termed the cell niche. The hybrid ECM-OPAAFscaffold characterized previously35 demonstratedsuperior adipoinductive capacity and it was hypothe-sized this maybe due to the presence of adipokinesembedded within the ECM that were deposited byADSCs prior to decellularization. Cell signaling,whether in the form of cytokines, adhesion moleculesor cell-to-cell contact, is thought to be imperative intissue engineering. Immunohistochemical (IHC) anal-ysis of the hDAM scaffold developed by Wang et al.43
reported a well maintained composition of collagen,glycosaminoglycan and VEGF; the latter stimulatingangiogenesis and neovascularization. Although thescaffold lacked laminin, important in cell attachmentand adhesion. Implanting ADSCs into the scaffoldin vivo, the density of donor cells was preserved up toweek 4, but then decreased significantly to week 8. Onthe contrary, the density of host native cells signifi-cantly increased from week 4 to 8, indicating hosttissue integration and adipose tissue regeneration.What caused the initial survival and then loss ofADSCs? What caused the subsequent migration ofhost cells after 4 weeks of implantation? There re-mains a substantial unknown knowledge relating tothe interaction between scaffold, cellular addition andgrowth factors.
BIOMEDICALENGINEERING SOCIETY
DONNELY et al.22

Lastly, to improve vascularization a study trialledinserting human umbilical cord perivascular cells(HUCPVCs) within fibrin gels containing heparin intoPDLLA scaffolds for 6 weeks in vitro and then uponimplantation into rat animal models, human umbilicalvein endothelial cells (HUVECs) were injected.8 Mi-croCT angiography reported a high degree of vascu-larization equally distributed throughout scaffolds, andHUVECs survived the 6 month implantation process,but self-assembled functional capillary networks wereonly observed around the periphery of the scaffolds.
Vascularization of Engineered Tissue
The optimal vascularization of the newly regener-ated tissue has proved a major challenge and althoughalready discussed in part previously, its importanceshould be highlighted further. Scaffolds may showadequate properties with in vitro and small animalmodels, although upon upscaling to larger animals oreven the female patient, issues can arise with insuffi-cient vascularization of central zones leading to tissuenecrosis. The most notable techniques identified in thisreview were the pre-vascularization concept and theinclusion of an arterio-venous loop.
Chhaya et al.7 hypothesized a novel pre-vasculariza-tion concept whereby a scaffold is implanted andallowed a period of 14 days prior to delayed fat injec-tion. This period allowed the formation of a blood clotwithin the scaffold’s interconnected porous network,consisting of platelets embedded within cross-linkedfibrin fibres and the endogenous production of growthfactors including fibronectin, vitronectin and throm-bospondin. The authors correlate this process to previ-ous literature, indicating the stimulation of a strongangiogenic response and the formation of highly orga-nized connective tissue. Following the 14 day period,delayed fat injection provided an adipogenic stimulusthat lead to the engineering of tissue filling the entire75 cm3 scaffold, with the composition of 47.32% adi-pose tissue. The initial connective tissue had beenmodified to contain highly vascular areas of fat tissueandno evidence of tissue necrosis over the 24-week studyperiod. To further the concept, it will need to be studiedutilizing a larger scaffold to assess the feasibility ofengineering clinically relevant volumes of adipose tissue.
Several articles evaluated the use of an arterio-ve-nous loop and the most successful to date has beenreported in a human case series. Morrison et al.29 im-planted a custom-made TEC in a submuscular pocketon the chest wall of female patients with prior mas-tectomy. A thoracodorsal artery perforator fat flapwas transposed into the TECs and upon TEC removal12 months later, 210 mL of tissue with macroscopic
appearance of fat had been engineered that bled whenpunctured, indicating good vascularization. Themechanism is not fully understood, but hypothesizedto be hypertrophy and hyperplasia, expanding theexisting tissue of the transposed fat flap. By stretchingof the overlying tissue and creating a non-collapsiblespace with the TEC, ischemia is likely to occur andtherefore enhance angiogenesis and the sprouting ofblood vessels from the vascular pedicle.
Study Limitations
The systematic review had several limitations. Asthe concept of a tissue engineered breast is still in itsinfancy, the authors’ protocols and techniques werediverse with no standardization. Along with relativelysmall sample sizes and low study powers, made anyform of comparison challenging. Lastly, 10 of thearticles were conference abstracts with limited infor-mation and the full text of one article was unavailable.
CONCLUSION AND FUTURE WORK
To conclude, current research in tissue engineeringis demonstrating promising results for the future ofbreast reconstruction. The most popular strategy fo-cusses on regenerating breast tissue using abiodegradable synthetic scaffold to support cellmigration and proliferation.
Exploring the literature has identified keys questionsrequiring further research, which can be divided intothree areas. Firstly the scaffold itself. The internalmorphology requires optimising to aid cell migrationand improve vascularization; the latter limiting thevolume of tissue generated. Together with whatamount of time is needed for the mature regeneratedtissue to be able to support itself, at which point thescaffold should degrade. This leads onto question thelong-term safety of the scaffolds with polymer degra-dation products unknown. Secondly, the addition ofcells. Will the use of stem cells or lipoaspirate improveadipogenesis or is it safer to allow native tissue tomigrate avoiding the oncogenesis risk? And lastly,what are the effects of specific growth factors on boththe tissue generated and the development of well-or-ganized vasculature?
ACKNOWLEDGMENTS
The authors would like to thank the correspondingauthors and publishers for giving full permission to re-use the figures illustrated in this article.
BIOMEDICALENGINEERING SOCIETY
Breast Reconstruction with a Tissue Engineering and Regenerative Medicine Approach 23

FUNDING
No funding was received for this article.
CONFLICT OF INTEREST
The authors hold no conflicts of interest.
OPEN ACCESS
This article is distributed under the terms of theCreative Commons Attribution 4.0 InternationalLicense (http://creativecommons.org/licenses/by/4.0/),which permits unrestricted use, distribution, andreproduction in any medium, provided you giveappropriate credit to the original author(s) and thesource, provide a link to the Creative Commonslicense, and indicate if changes were made.
REFERENCES
1Aoki, S., S. Toda, T. Sakemi, and H. Sugihara. Cocultureof endothelial cells and mature adipocytes actively pro-motes immature preadipocyte development in vitro. CellStruct. Funct. 28:55–60, 2003.2Bray, F., J. Ferlay, I. Soerjomataram, et al. Global CancerStatistics 2018: gLOBOCAN estimates of incidence andmortality worldwide for 36 cancers in 185 countries. CACancer J. Clin. 68(6):394–424, 2018.3Brody, G. S., D. Deapen, C. R. Taylor, et al. AnaplasticLarge Cell Lymphoma Occurring in Women with BreastImplants: analysis of 173 Cases. Plast. Reconstr. Surg.135:695–705, 2015.4Cancer Research UK. Breast Cancer Statistics. Availableat: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer#heading-Five. Accessed 29 Dec 2018.5Cao, Y. L., E. Lach, T. H. Kim, et al. Tissue-engineerednipple reconstruction. Plast. Reconstr. Surg. 102:2293–2298, 1998.6Chen, W., X. Lv, X. Xu, X. Gao, and B. Wang. Meta-analysis for psychological impact of breast reconstructionin patients with breast cancer. Breast Cancer 25:464–469,2018.7Chhaya, M. P., E. R. Balmayor, D. W. Hutmacher,and J. T. Schantz. Transformation of breast reconstructionvia additive biomanufacturing. Sci. Rep. 6:28030,2016.8Chhaya, M. P., F. P. W. Melchels, B. M. Holzapfel, J. G.Baldwin, and D. W. Hutmacher. Sustained regeneration ofhigh-volume adipose tissue for breast reconstruction usingcomputer aided design and biomanufacturing. Biomaterials52:551–560, 2015.9Cho, S. W., W. S. Kang, W. R. Jong, et al. Engineeredadipose tissue formation enhanced by basic fibroblastgrowth factor and a mechanically stable environment. CellTransplant. 16:421–434, 2007.
10Cho, S. W., S. S. Kim, J. Won Rhie, et al. Engineering ofvolume-stable adipose tissues. Biomaterials 26:3577–3585,2004.
11Debels, H. Advances in tissue engineering; a novel tech-nology making use of an in vivo vascularized chamber.Acta Chir. Belg. 115:104–110, 2015.
12Debels, H., X. L. Han, J. Palmer, et al. Sustainable fatgrafting—optimizing fat grafting in an in vivo tissue engi-neering chamber model. In: Wound Repair and Regenera-tion 2013: Conference: 23rd Annual Meeting of theEuropean Tissue Repair Society. Reims France. Confer-ence Publication: (var.pagings). 21(6), p. A63.
13Elfadl, D., V. Garimella, T. K. Mahapatra, P. L. McMa-nus, and P. J. Drew. Lipomodelling of the breast: a review.Breast 19:202–209, 2010.
14Findlay, M. W., J. H. Dolderer, N. Trost, et al. Tissue-engineered breast reconstruction: bridging the gap towardlarge-volume tissue engineering in humans. Plast. Reconstr.Surg. 128:1206–1215, 2011.
15Fischer, J. P., J. A. Nelson, E. Cleveland, et al. Breastreconstruction modality outcome study: a comparison ofexpander/implants and free flaps in select patients. Plast.Reconstr. Surg. 131:928–934, 2013.
16Fukumura, D., A. Ushiyama, D. G. Duda, et al. Paracrineregulation of angiogenesis and adipocyte differentiationduring in vivo adipogenesis. Circ. Res. 93:E88–E97, 2003.
17Gart, M. S., J. T. Smetona, P. J. Hanwright, et al. Autol-ogous Options for postmastectomy breast reconstruction: acomparison of outcomes based on the American College ofSurgeons National Surgical Quality Improvement Pro-gram. J. Am. Coll. Surg. 216:229–238, 2013.
18Gerges, I., F. Martello, C. Recordati, et al. Exploring thepotential of polyurethane-based soft foam as cell-free scaffoldfor soft tissue regeneration. Acta Biomater. 73:141–153, 2018.
19Giatsidis, G. Breast tissue engineering: decellularized scaf-folds derived from porcine mammary glands. In: Journal ofthe American College of Surgeons 2015: Conference: 101stAnnual Clinical Congress of the American College ofSurgeons. Chicago, IL. Conference Publication: (var.pag-ings). 221 (4 Suppl 2), p. e117.
20Glowacki, J., and S. Mizuno. Collagen scaffolds for tissueengineering. Biopolymers 89:338–344, 2008.
21Hettiarachichi, K. D., A. J. O’Connor, S. Leo, et al. Theeffects of biophysical and biochemical environment onpreadipocyte differentiation. J. Tissue Eng. Regen. Med.6(Suppl 1):263, 2012.
22Huss, F. R. M., and G. Kratz. Mammary epithelial cell andadipocyte co-culture in a 3-D matrix: the first step towardstissue-engineered human breast tissue. Cells Tissues Organs169:361–367, 2001.
23Jamison, K. R., D. K. Wellisch, and R. O. Pasnau. Psy-chosocial aspects of mastectomy: I. The women’s perspec-tive. Am. J. Psychiatry 135:432–436, 1978.
24Jung, H. K., C. H. Kim, and S. Y. Song. Prospective 1-yearfollow-up study of breast augmentation by cell-assistedlipotransfer. Aesthet. Surg. J. 36:179–190, 2016.
25Kaufman, C., J. Barone, M. Cross, et al. Interim report of aclinical registry: 669 patients implanted with a 3-D bioab-sorbable marker. Ann. Surg. Oncol. 25(Supplement 1):S99,2018.
26Kronowitz, S. J., and G. L. Robb. Radiation therapy andbreast reconstruction: a critical review of the literature.Plast. Reconstr. Surg. 124:395–408, 2009.
27Leong, W. L., S. Sharifpoor, and K. Battiston, et al. Re-Filx-synthetic biodegradable soft tissue fillers for breastconserving surgery in breast cancer (Abstract). In: Con-ference Proceedings of the 2017 San Antonio Breast Cancer
BIOMEDICALENGINEERING SOCIETY
DONNELY et al.24

Symposium, 2017 December 5–9; San Antonio, TX.Philadelphia (PA): AACR; Cancer Res. 2018;78(4Suppl):Abstract nr P2-12-15.
28Markopoulos, C., A. K. Tsaroucha, E. Kouskos, et al. Im-pact of breast cancer surgery on the self-esteem and sexual lifeof female patients. J. Int. Med. Res. 37:182–188, 2009.
29Morrison, W. A., D. Marre, D. Grinsell, et al. Creation ofa large adipose tissue construct in humans using a tissue-engineering chamber: a step forward in the clinical appli-cation of soft tissue engineering. EBioMedicine 6:238–245,2016.
30Nair, L. S., and C. T. Laurencin. Biodegradable polymersas biomaterials. Prog. Polym. Sci. 32:762–798, 2007.
31O’Halloran, N., K. Gilligan, E. Dolan, et al. Evaluating anovel adipose tissue engineering strategy for breast recon-struction post-mastectomy. In: Irish Journal of Medical Science2018: Conference: 43rd Sir Peter Freyer Memorial Lecture andSurgical Symposium. Ireland, 187(Supplement 4), p. S59.
32Omidi, E., L. Fuetterer, S. Reza Mousavi, et al. Charac-terization and assessment of hyperelastic and elastic prop-erties of decellularized human adipose tissues. J. Biomech.47:3657–3663, 2014.
33Pashos, N. C., M. E. Scarritt, Z. R. Eagle, et al. Charac-terization of an acellular scaffold for a tissue engineeringapproach to the nipple–areolar complex reconstruction.Cells Tissues Organs 203:183–193, 2017.
34Ross, R. J., R. Shayan, K. L. Mutimer, and M. W. Ashton.Autologous fat grafting current state of the art and criticalreview. Ann. Plast. Surg. 73:352–357, 2014.
35Rossi, E., J. Guerrero, P. Aprile, et al. Decoration of RGD-mimetic porous scaffolds with engineered and devitalizedextracellular matrix for adipose tissue regeneration. ActaBiomater. 73:154–166, 2018.
36Samani, A., J. Zubovits, and D. Plewes. Elastic moduli ofnormal and pathological human breast tissues: an inver-sion-technique-based investigation of 169 samples. Phys.Med. Biol. 52:1565–1576, 2007.
37Shpaisman, N., L. Sheihet, J. Bushman, J. Winters, and J.Kohn. One-step synthesis of biodegradable cur-
cumin-derived hydrogels as potential soft tissue fillers afterbreast cancer surgery. Biomacromol 13:2279–2286, 2012.
38Sisti, A., L. Grimaldi, J. Tassinari, et al. Nipple-areolacomplex reconstruction techniques: a literature review. Ejso42:441–465, 2016.
39Spiller, K. L., R. R. Anfang, K. J. Spiller, et al. The role ofmacrophage phenotype in vascularization of tissue engi-neering scaffolds. Biomaterials 35:4477–4488, 2014.
40Tada, R., and T. Fujisato. Adipose tissue engineering for abreast reconstruction. In: Journal of Tissue Engineering andRegenerative Medicine 2012: Conference: 3rd TERMISWorld Congress 2012. Vienna Austria. Conference Publi-cation: (var.pagings), 6 (Suppl 1), p. 266.
41Tierney, B. P., J. P. Hodde, and D. I. Changkuon. Biologiccollagen cylinder with skate flap technique for nipplereconstruction. Plast. Surg. Int. 2014:194087, 2014.
42Tsuji, W., T. Inamoto, R. Ito, et al. Simple and long-standing adipose tissue engineering in rabbits. J. Artif. Org.16:110–114, 2013.
43Wang, L., J. A. Johnson, Q. Zhang, and E. K. Beahm.Combining decellularized human adipose tissue extracel-lular matrix and adipose-derived stem cells for adiposetissue engineering. Acta Biomater. 9:8921–8931, 2013.
44Wu, H., T. Zhou, L. Tian, Z. Xia, and F. Xu. Self-assem-bling RADA16-I Peptide hydrogel scaffold loaded withtamoxifen for breast reconstruction. BioMed. Res. Int.2017:3656193, 2017.
45Xiao, X., S. Zhou, J. Wan, et al. Pre-shaped large-volumeengineered vascularized pedicled adipose flaps in a rabbitmodel: a two stage tissue engineering chamber-based pro-cedure. J. Biomater. Tissue Eng. 7:261–268, 2017.
46Zuk, P. A., M. Zhu, H. Mizuno, et al. Multilineage cellsfrom human adipose tissue: implications for cell-basedtherapies. Tissue Eng. 7:211–228, 2001.
Publisher’s Note Springer Nature remains neutral with re-
gard to jurisdictional claims in published maps and institu-tional affiliations.
BIOMEDICALENGINEERING SOCIETY
Breast Reconstruction with a Tissue Engineering and Regenerative Medicine Approach 25