Embed Size (px)
Citation preview

Breast cancer genetics
and screening
Dr Gary Sharp
1. Which familial syndromes increase the risk of breast cancer?

BRCA 1 (BReast Cancer)

BRCA1 Facts• Role – unclear. Theories include;
• Transcription factor• Assists in cell cycle• Induce apoptosis (Bennett et al., 2000)
• Accounts for ~40% of all familial breast cancer (Beauchamp et al.,)
• ~60% life time risk of developing ovarian cancer (Bennett et al., 2000)
• Usually more aggressive and receptor negative (ER, PR and c-erbB2 negative) (Bennett et al., 2000)
• BRCA1 is associated with;

BRCA 2• 1995• Long arm of chromosome 13• Accounts for ~30% of familial
breast Ca• Associated with male breast Ca
(BRCA1 is NOT)• 6% lifetime risk of breast
cancer in men (E J Meijers-Heijboer et al)
• Role – DNA repair (Bennett et al., 2000)
• Usually hormone receptor positive
• ~30% lifelong risk of ovarian Ca (Beauchamp et al)

My apologies!
Tumourgenesis• Germline mutations inactivate a
single inherited allele of BRCA 1 in every cell and this precedes a somatic event in breast epithelial cells (a second hit) which eliminates the remaining allele and causes the cancer.
Penetrance• High penetrance = early
onset/age of cancer presentation.• BRCA penetrance rises most
sharply from 40–60 years of age.
Genetics cont...• High populations of both BRCA
1/2 genetic mutation in Ashkenazi Jews (1:100) and French Canadians• The overall lifetime risk of
breast Ca in a BRCA 1/2 carrier is 50-90%• Frequency of BRCA mutation
in gen pop is 1:1000(Beauchamp et al)
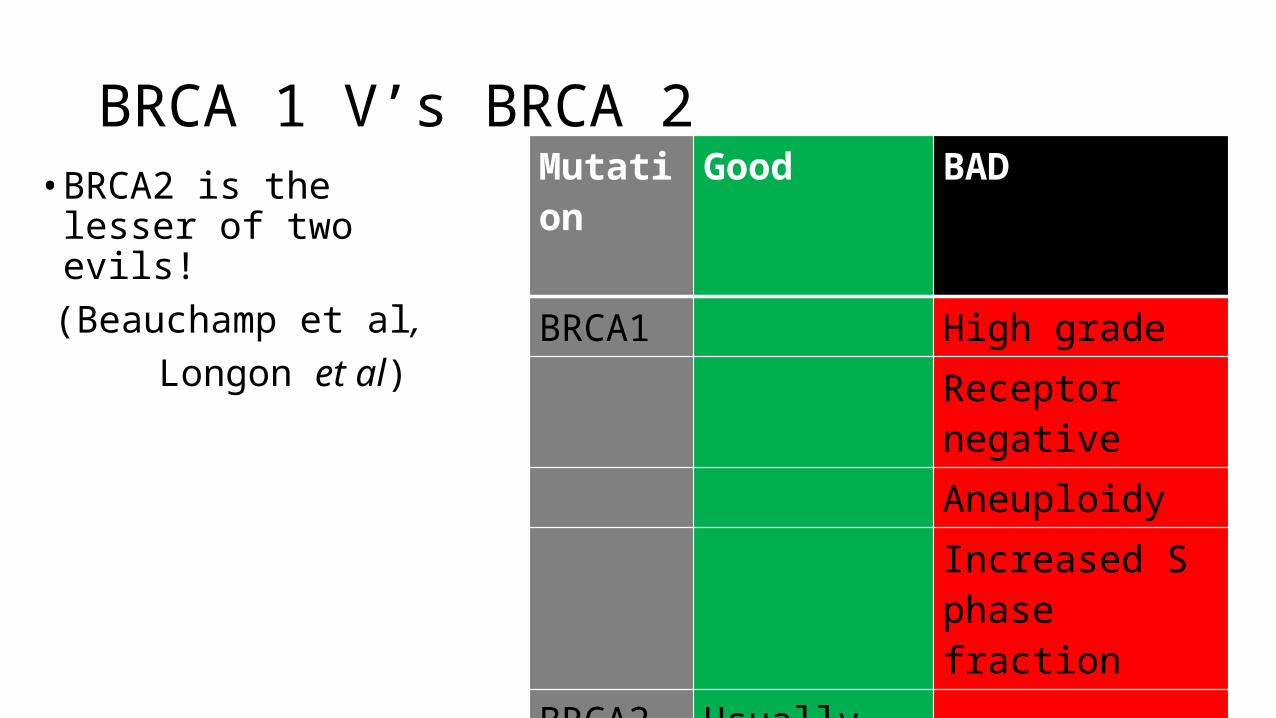
BRCA 1 V’s BRCA 2• BRCA2 is the lesser of
two evils!(Beauchamp et al,
Longon et al)
Mutation Good BAD
BRCA1 High gradeReceptor negativeAneuploidyIncreased S phase fraction
BRCA2 Usually hormone receptor positive

2. What are the recommendations for breast cancer screening?

“So far the only breast cancer screening method that has
proved to be effective is mammography screening.”
“Breast cancer survival rates vary greatly worldwide, ranging from 80% to below 40% in low-income countries.”
“…early detection remains the
cornerstone of breast cancer
control.”

BreastScreen Australia
• Established in 1991, actually started in ‘94. • 2013-14 expanded from women 50-
69 to 50-74. • Two-yearly mammograms. • 40-49 yrs and >75 eligible for free
mammograms, but have to ask.• The initial mammogram is
performed in a screening unit. • Recalled to the MDT assessment
centre if further investigation needed.

Mammography• Better for detecting malignant
lesions than diagnosing benign ones (USS better)• Breast compressed between 2
plexiglas plates• Reduces tissue thickness = less
radiation & improves image• Two views taken;– Craniocaudal–Oblique – allows more breast
tissue and axilla to be imaged

Screening high risk patients
Performance objective 1.5:Annual screening is offered only to women atsubstantially increased risk of developing breast cancer.

High risk recommendations
…individualised surveillance program be developed ... This might include regular clinical breast examination and breast imaging with mammography and/or ultrasound.
Women are at “increased risk” if;1. two or more family members, especially
if FDR – and/or if they were <50 2. carrier of a gene mutation3. previously diagnosed with breast cancer
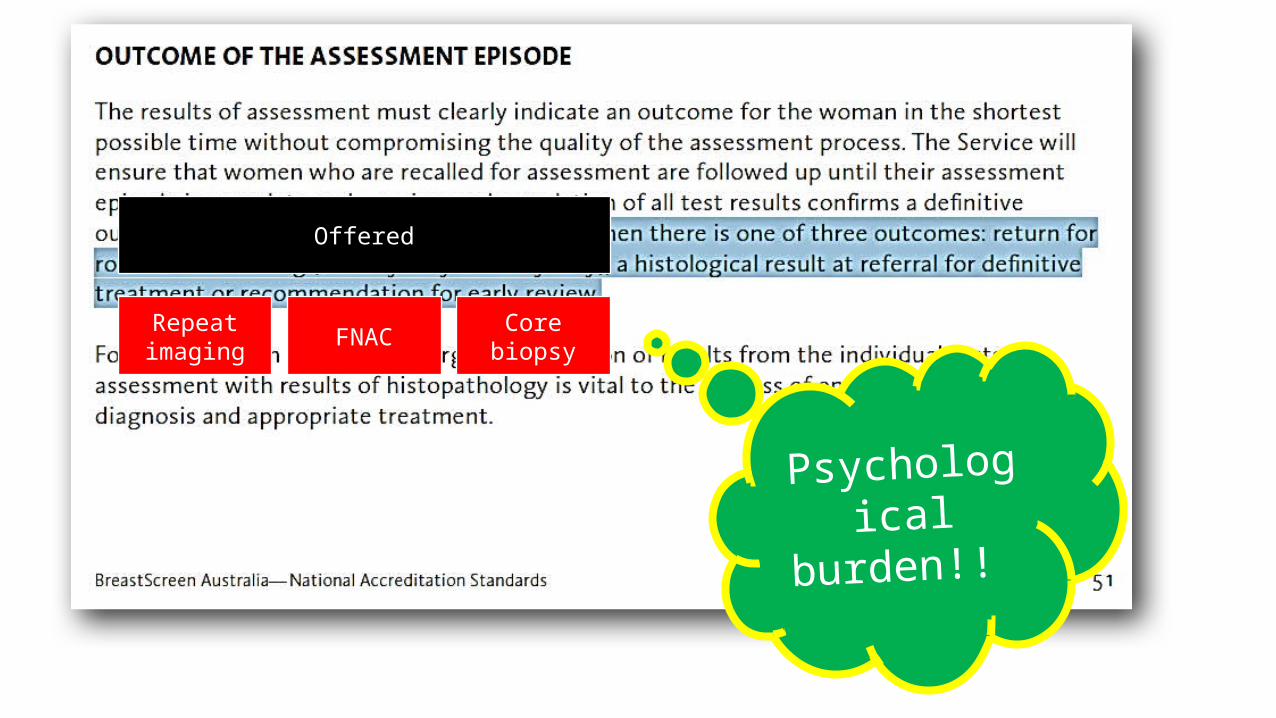
Psychological burden!!
Offered
Repeat imaging FNAC Core biopsy
Genetic testing
• Should only be performed If;• 1 FDR <40 or with bilateral disease <50 • OR• ≥2 FDR’S at any age, especially with breast and ovarian cancer in any one
individual (Bennett et al., 2000)• An exception to the above general comments are women of Ashkenazi Jewish
descent (Bennett et al., 2000)
Psychological impactHealth insurance affected
Financial ramifications

Suggested screening of BRCA +ve patients
2000

3. What is the evidence for prophylactic mastectomy?

“Currently, unaffected women with a BRCA1 or BRCA2 mutation face the choice of regular surveillance, prophylactic surgery, or chemoprevention”
53 consecutive families with a known BRCA1 orBRCA2 mutation.
Findings - 682 unaffected individuals with a 50% or 25% risk for carrying a mutation were identified and offered a DNA test.
Of the unaffected women with an identified mutation who were eligible for
prophylactic surgery, 51% (35 of 68) opted for bilateral mastectomy.
High demand BRCA1 and BRCA2 testing and of prophylactic
surgery by unaffected women with the mutation.
Young women with children especially opt for DNA testing and prophylactic mastectomy.
2000

2000
1-19% failure (breast cancer
identified)rate of prophylactic
mastectomy
Residual breast tissue and particularly ectopic breast tissue (lower chest wall, abdomen and lateral axilla)

…for prevention of a second breast cancer (contralateral as well as
ipsilateral), a bilateral mastectomy might be considered, but in
selected cases.
2005

“Prophylactic mastectomy for the prevention of breast cancer”, Cochrane Review.
•Data collection;•39 observational studies included (no RCT’s available)•n-7384 women, all underwent prophylactic mastectomy
2010

Cochrane review conclusion
•BPM was effective in reducing both the incidence of, and death from, breast cancer•Rigorous RCT needed•BPM should be considered in those with very high risk
of disease only• INSUFFICIENT EVIDENCE THAT CPM improves survival

What we MUST remember!• 16 studies investigated psychosocial issues surrounding prophylactic mastectomy• Results;
• Most reported high levels of satisfaction with the decision to have a prophylactic mastectomy
• Variable satisfaction with cosmetic outcome
• A table showing levels of “worry”;
• Adverse events (unanticipated re-operations) following prophylactic mastectomy;• 4% in those without reconstruction• 49% in those WITH reconstruction
Bilateral prophylactic mastectomy (BPM) Surveillance
Significantly reduced worry post mastectomy Greater levels of worry when compared to BPM group

Summary
1. Familial breast cancer accounts for 5-10% of all breast cancers. Germline mutation that then encounter a “second hit”.
2. Screening should be tailored to the patient and their risk coupled with their wishes.
3. No hard and fast rule regarding prophylactic mastectomy. It is associated with better outcomes in high risk patients but it is NOT a curative procedure.

References
1. Beauchamp et al., Sabiston Textbook of Surgery, 19th ed. Section 7.
2. BreastScreen Australia, National accreditation Standards, BreastScreen Australia, Quality Improvement Program.
3. E J Meijers-Heijboer, L C Verhoog, C T M Brekelmans, C Seynaeve, M M A Tilanus-Linthorst, A Wagner, L Dukel, P Devilee, A M W van den Ouweland, A N van Geel, J G M Klijn (2000). “Presymptomatic DNA testing and prophylactic surgery in families with a BRCA1 or BRCA2 mutation.” THE LANCET, Vol 355, 2015–20
4. I. C. Bennett,1 M. Gattas2 and B. T. Teh3 (2000). ”The management of familial breast cancer. REVIEW ARTICLE”. The Breast 9, 247–263
5. Longon et al., Harrisons Principles of Internal Medicine, 18th ed. Chapter 90.
6. Lostumbo et al., (2010). “Prophylactic mastectomy for the prevention of breast cancer (Review). The Cochrane Collaboration.
7. National cancer institute. Genetics of breast and ovarian cancer. http://www.cancer.gov/cancertopics/pdq/genetics/breast-and-ovarian/HealthProfessional/page1/AllPages
8. National breast Cancer centre august 2004, Early detection of breast cancer.
9. World Health Organisation, Breast cancer: prevention and control.