Embed Size (px)
Citation preview

23/06/2015
1
Child and adolescent Mental Health can we help?
Dr Tina Nicholson CCFPFamily Practitioner and Medical Lead, Cochrane
Clinical Lecturer Dept Family Med. U of C.Member of CanReach Faculty
Absolutely none !!
2. Suggest an approach to managing such cases in the Primary Care setting
1. Raise awareness of the current available provision for child and adolescent mental health our region
3. Introduce assessment tools applicable to primary care management
4. Brief Description of CanReach course
Total Percentage of Children in Calgary with a mental disorder over the first 18 years of life
34%
50
26
11 13
0
10
20
30
40
50
60
Family Physicianor General
Practitioner
Pediatrician Psychiatrist Other
Per
cen
tage

23/06/2015
2
21%
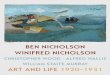
Total numbers of Children ≤ 18 years old in 2013 in Calgary ^ 300,000
Number of Children with Mental Disorders diagnosed by 81,000 Physicians in Calgary
Numbers of Children served by the entire Publically Funded Child and Adolescent Mental Health System in Calgary (present capacity)
Number of Child and Adolescent Psychiatrists in Calgary
Number of Child and Adolescent Psychiatrists in Canada
300,000
81,000
20,285
25
400
Raise our own awareness of potential psychiatric disorders in our young population
Become more familiar with interviewing and managing child and adolescent psychiatric cases
Increase levels of comfort with assessing and treating common childhood psychiatric disorders
Increase awareness and develop networks with support services in our localities
9yr old boy brought in after concerns raised by school teacher in grade 4
-Excessive fatigue- - falling asleep at desk--lack of interest in schoolwork -Unable to complete tasks--difficult to engage--high level anxiety – separation issues--never enjoys things-- no longer playing with friends-Seems very sad despite their best efforts to help him he remains closed off
- Noticed change in his behavior since parents split a year before
- Separation issues- will not travel without mum, sleeps in her bed, constantly texts or rings her whilst he is at school
- Has said he needs to be with her as if she died he would want to die too
- Initial insomnia (2am) - Disinterested and inactive - Weight gain -Always struggles with organization – worse in
last 12m
Aware that he worries a lot – wants to be with Mom all the time and constantly thinks about her when at school
Tends to like routine and does not like change Finds some things interesting but hates math Prefers to be alone and feels he is different to
his peers Has a friend with Aspergers – finds him easier
to understand as he is straightforward

23/06/2015
3
?Depression ?Separation Anxiety ?Anxiety Disorder ?Learning Disability ?ADD ?Abuse ?Bullying ASD
Additional History Developmental history - Normal School Records – Grade level, struggles in math
and with organization Past psychiatric history- none Past medical history - none Family history and social history – extensive
FH of anxiety and depression. Only child, parents separated 18m ago lives with Mom.
Do not forget physical exam - Normal
Mental Health assessment -
Chad feels sad, cannot recall the last time he felt happy or looked forward to anythingAware he is scared all the time- especially of losing his Mom – does think about her dyingDislikes school and his peersPrefers talking to adults or being alone
No thought disorder , delusions or hallucinations notedNo suicidal ideation
Lab? – none
Screening tools – Why should we use them?
–Can improve identification and assessment of mental health problems and easy to use in practice.-May increase reliability of diagnosis- Useful as a tracking tool when reviewing patient
1. C-GAS – Children's Global Assessment Scale
- A rating scale measuring psychological, social and school functioning for children aged 6-17yrs
2. SCARED- Screen for Child Anxiety Related Disorders – parent and child versions
3. Vanderbilt – ADHD diagnostic rating scale –parent and teacher versions
4. Pediatric Symptom Checklist- PSC-17Psychosocial screen designed for busy office use , takes 5mins – parent and youth versionsLooks at attention/internalizing and externalizing subscales

23/06/2015
4
C-GAS – 45 – Moderate degree of interference in functioning in most social areas or severeimpairment of functioning in one area, such as might result from, for example,suicidal preoccupations and ruminations, school refusal and other forms ofanxiety, obsessive rituals, major conversion symptoms, frequent anxiety attacks,poor to inappropriate social skills, frequent episodes of aggressive or otherantisocial behavior with some preservation of meaningful social relationships.
2. SCARED - Parental Total Score 30 ( > 25 indicates Anxiety Disorder)
Child Total Score 41
3. Vanderbilt – Parental score -Positive score for inattentive subtype ADDPositive score for Anxiety/Depression
Borderline score for ODD
4. PSCY-17 – Parent score - 18 ( >15 is positive) for internalizing i.e. anxiety/depression – but negative for ADD- Child score - 11
Separation Anxiety, panic disorder and generalized anxiety are likely to be causing moderate impairment in functioning at school, at home and when separated from MomOppositional behavior is borderline – probably as result of anxietyADD – borderline? Affected by anxiety – “chicken and egg”
-Address the most prominent impairment - ANXIETY
-Team approach:- ChildParents and carersSchool – teachers and psychologistBehavioral health nurse in clinicHealthy minds /Healthy child SWphysician
- Remember - It takes a village to raise a child

23/06/2015
5
Educate and counsel families and child about the diagnosis and possible treatments
What are they actually getting?Support only ? OR –Evidence based psychotherapy such as - CBT-Interpersonal Psychotherapy
-Anxiety Management strategies for both child and parents
Prescribe homework:-
Anxiety management techniquesBreathing and relaxationStrategies for avoiding catastrophising thoughtsDipping into the AnxietyBC.com website – both parents and child
Review progress and consider adding in medicationChad took melatonin to aid sleep prior to presentation.
For Chad the decision to add medication was made 4months after initial visit as progress had been slow and Mom was getting burnt out trying to manage his anxiety
SSRI’s –Health Canada states no indication for their use under aged 17, but there are FDA approvals for some medications and evidence based support in their use in conjunction with therapy in this age group for anxiety and depression

23/06/2015
6
FluoxetineSertralineEscitalopram
START LOW , GO SLOW, MONITOR WEEKLY
Rx given Escitalopram 5mg dailyCarefully monitored for side effects, suicidality.No effects after 2 weeks – dose increased to 7.5 mg and then 10mg – this caused disinhibition so dose reduced back to 7.5mg with good effect
Nausea and Dry MouthSomnolence or insomniaTremorEjaculatory dysfunctionDecreased libidoSerious- Serotonin Syndrome, increased Suicidality
Worsening Depression or mania
Chad continued to feel tired but showed some disinhibition as dose increased – adjusted accordingly
Despite SSRI, academic performance was not improving2months post Rx – C-GAS now 55–variable functioning in some social areasVanderbilt scoring also improved in social functioning but worse in academic functionDecision taken to treat his inattentive ADDAddition of Methylphenidate– again start low and go slowMonitor mood, weight and height , BP and pulse
Stimulants :-MethylphenidateAmphetamines
Advantages – can have immediate onset- ability to alter dose “drug holiday” - multiple options for delivery, peak
actions and duration of actions
Disadvantages – tolerance or psychological dependence- worsen tics- may suppress growth- cardiac effects?
Atomoxetine – SNRI- weight based dose- less chance of abuse potential- no apparent effect on growth or
tics
Disadvantages – delayed onset of action (1-2 weeks)
- not as effective for some- side effects – irritability and
insomnia
Also – Wellbutrin ClonidineGuanfacine
Anxiety symptoms much improved -Marked reduction in texting and phoning Mom- Coped with weekends at Dads house better- No more panic attacks--sleep improved
-ADD – meds made him feel jittery but marked difference noted by Mom and teachers in school performance-Despite this he does not like the taste or how he feels so has asked to switch to alternative - just initiated-He will remain under close observation until stable

23/06/2015
7
YES! Chad commented on laughing spontaneously at school with friends – without pretending !His anxiety is minimal nowHis attention is improvingHis Mom is very happy with his progress so far and feels much better equipped to support him.
SCARED – Parent score now 20 ( previously 30)Child Score now 5 ( previously 41)
C-GAS – 68 – generally functioning wellVanderbilt- no longer positive for inattentive ADD – both parent and teacher scorings
“A 6 month mini-fellowship in Child and Adolescent psychopharmacology”Aim : train primary care providers in effective and evidence based mental health assessment and intervention to help them transform their practices, increase productivity, and improve work satisfaction
Structure: 3 day (15 hour) course that uses a combination of intensive face-to-face teaching and hands-on practice followed by 6 months of ongoing case-based coaching using distance learning
You will never be alone in managing these cases again!!THANK YOU !