Embed Size (px)
Citation preview

Brain Death
Shawn Ng
• ANZICs Statement on death and organ donation Edition 3.2 (2013)

CICM Fellowship exam /2012With regards to the determination of brain death: 1. Apart from identifying evidence of sufficient intracranial pathology, list the preconditions that must be met prior to the determination of brain death by clinical criteria:
2. What is the recommended minimum time for observation in cases of hypoxic- ischaemic brain injury, prior to performing clinical testing of brain-stem function?
3. For each of the following brainstem reflexes, list the cranial nerves that are tested:a. Cough reflexb. Vestibulo-ocular reflexc. Pupilary light reflexd. Corneal reflexe. Gag reflex
4. List three contraindications to performing apnoea testing:
5. List the acceptable imaging techniques that may be used to demonstrate brain death as an alternative to clinical testing as recommended by the ANZICS Statement on Death and Organ Donation

Which of the following precludes certification of death by clinical brain death testing?
• A) Flexion of the right elbow on painful stimulus within the cranial nerve distribution
• B) Unilateral hemotympanum• C) No family consent• D) Isolated Brainstem infarction without
cerebral injury• E) Avulsion of one eye
Brain Death
• Brain death occurs in the setting of a severe brain injury associated with marked elevation of intracranial pressure.
• Inadequate perfusion pressure results in a cycle of cerebral ischaemia and oedema and further increases in intracranial pressure.
• When intracranial pressure reaches or exceeds systemic blood pressure, intracranial blood flow ceases and the whole brain, including the brain-stem dies.
• Determination of brain death requires that there is unresponsive coma, the absence of brain-stem reflexes and the absence of respiratory centre function.
• These findings are irreversible. • In particular, there must be definite clinical or
neuro-imaging evidence of acute brain pathology consistent with the irreversible loss of neurological function.

• Brain death cannot be determined without evidence of sufficient intracranial pathology.
• Cases in which brain-stem has been the primary site of injury and death of the brain-stem has occurred without death of the cerebral hemispheres.
• Thus brain death cannot be determined when the condition causing coma, and loss of all brain stem functions has affected only the brain stem, and there is still blood flow to the supratentorial part of the brain.
• Whole brain death is required for the legal determination of death in Australia and NZ. (cf to the UK.)
• The 3 essential findings in brain death are– Coma(unresponsiveness)– Absence of brainstem reflexes– Apnoea
Brain death determination
• Clinical testing if preconditions are met• Imaging that demonstrates the absence of
intracranial blood flow.
• There is no documented case of a person who fulfills the preconditions and criteria for brain death ever subsequently developing any return of brain function.
Determination of Brain death by clinical examination
• Preconditions– Evidence of sufficient intracranial pathology
• ALL the following preconditions must be met if brain death is to be determined by clinical examination. – cause for coma consistent with brain death– at least 4 hours of observation during which preconditions
must be met (GCS 3, pupil non-reactive, no cough, apnoea)– neuro-imaging consistent with acute brain pathology that
could cause brain death– normothermia (T>35C)
Brain death preconditions
• normotension (SBP>90 or MAP>60mmHg in an adult)• no sedation or analgesia (dependent on types of drugs used,
renal and hepatic function; use antagonists if concerned)• absence of severe electrolyte, metabolic and endocrine
disturbances (glucose, Na+, PO43-, Mg2+, renal and hepatic function)
• no paralysis (use NMJ monitor or electromyography if concerned)
• ability to assess brain stem reflexes (at least one eye and ear)• ability to perform apnoea test (doesn’t have severe hypoxic
respiratory failure or have a high cervical spine injury)

• In cases of acute hypoxic ischaemic brain injury, clinical testing for brain death be delayed for at least 24 hours subsequent to ROSC.
• Therapeutic hypothermia may modify outcome prediction after cardiac arrest.
• It is therefore recommended when induced hypothermia has been used after resuscitation from cardiorespiratory arrest that clinical testing for brain death be delayed for at least 24 hours AFTER rewarming.
• Brain death may be determined PRIOR to 24 hours by demonstration of absent cerebral blood flow.

Brain death examination

“It’s about testing connections”
• GCS 3 – no response in CN distribution (supraorbital compression) and deep nail bed pain in all four limbs
• !!Spinal reflexes may be present in patients with brain death
• Observations that are incompatible with brain death– Decerebrate/decorticate posturing– True extensor or flexor motor responses to painful stimuli– Seizures

Brain Stem Reflexes testingALL MUST BE ABSENT
• pupils fixed, no reaction to light (CN II, III) – must be > 4mm
• !! Anticholinergic drugs such as atropine can cause pupillary dilatation
• Cataract or iris surgery is not a CI for clinical testing

• no corneal reflex (CN V, VII)
• !! Touching the sclera is not sufficient

• Reflex response to pain in the trigeminal nn distribution- CN V-VII
• no oculo-vestibular reflexes (CN III, IV, VI, VIII)
• !! Ruptured eardrums does not invalidate test• # to BOS or petrous temporal bone may
obliterate the response on the side of the #• Testing for the oculocephalic reflex –
submaximal stimulus/aggravate spinal injury

• no gag (CN IX, X)

• no cough (CN X)
• !! Efferent nerves are the phrenic/innovation of the thoracic and abdominal musculature. Therefore it cannot be assessed in patients with high cervical cord injury.
• positive apnoea test (after preoxygenation, and pH 7.3, no breath taken after disconnection from ventilator with a PaCO2 > 60mmHg; or increase in PCO2 by 20 mmHg if COPD/ CO2 retainer)
Apnoea test

• independent examination by 2 suitably trained and experienced doctors
• can be sequential (don’t have to wait 2 hours between testing)
• time of death is the time of completion of the second examination
Brain Death Investigations
• the indication for cerebral perfusion imaging is when clinical brain death can not be determined (any of the preconditions can not be met)
• an investigation showing absent cerebral parenchymal blood flow is required
• Problematic in– Infants– Massive skull fractures– Craniotomy with extensive bone removal
Imaging
• 4 vessel angiogram • Tc-99 HMPAO SPECT radionuclide • CT angiography • Transcranial doppler (TCD)

Other ancillary tests
• Cerebral Perfusion Scintigraphy• XeCT• MRAngiography• MR perfusion

ANZICS recommendation
• 4 vessel angiography• Radionuclide imaging• CT A may be acceptible, although experience
in the technique is limited.
• MRI and TCD are not recommended.

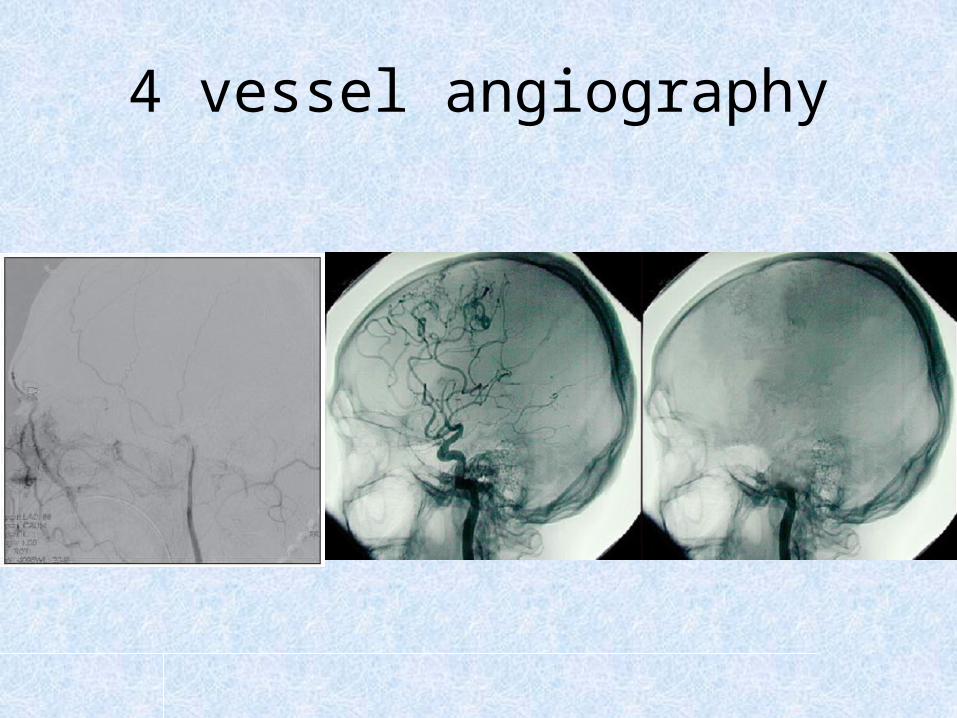
4 vessel cerebral angiography• Gold standard of confirmatory tests.• No false positives reported.• False negative examinations may occur if – No significant elevation of the ICP– Contrast is injected too vigorously into the
downstream circulation, thereby artifactually opacifying the intracranial vasculature. (?screen with TCD)

4 vessel angiography
• Advantages– Able to visualise cerebral and posterior fossa
blood flow– Gold standard
• Disadvantages– Invasive– Expensive– Exposed donor to toxic contrast material– False negatives
4 vessel angiography

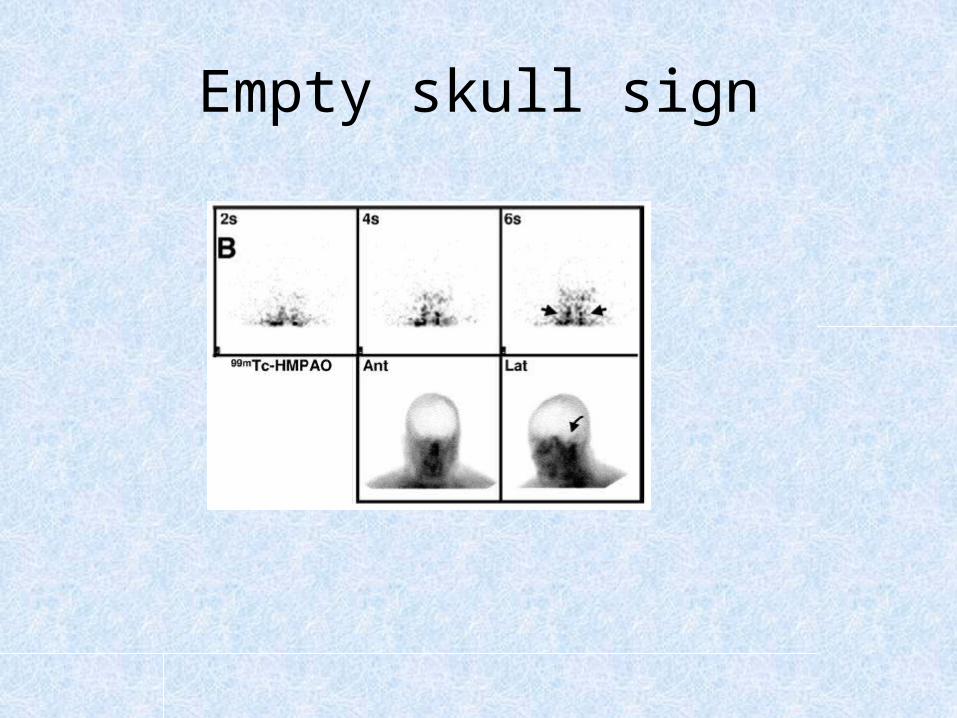
Tc-99 HMPAO SPECT radionuclide
• Absence of intracranial perfusion.• IV bolus of radioactive material Crosses BBB to
be retained in the parenchyma• There are occasional technical failures due to
inadequate bolus injection of the radiopharmaceutical.
• Single Photon Emission CT(SPECT) provides superior imaging in adults and in children Vs 2-planar imaging

• Advantages:– ?Ability to detect blood flow patients who are in a
coma due to drug intoxication.• Disadvantages:– Posterior fossa circulation not evaluated– Occasional technical failure- inadequate bolus
injection of the radiopharmaceutical.
Empty skull sign
CT angiography
• Small studies have shown absent enhancement bilaterally of peripheral intracranial arteries and central veins on CTA at 60 secs. There should be absent enhancement bilaterally on ALL these– MCA cortical branches- that is beyond the sylvian branches– P2 segment of the posterior cerebral arteries– Pericallosal arteries– Internal cerebral veins
• to perform this examination, the potential risk of contrast-mediated tissue injury is still present

CT angiography
• No large studies with matched controls• When compared to clinical testing for brain
death, the CTA test had a sensitivity of 0.85• (Cochrane systematic review -The use of
computed tomography angiography (CTA) to confirm the clinical diagnosis of brain death Taylor et al 31.3.2014
CT angiography
• Advantages– Cheap, easily accessible– Only needs IV access
• Disadvantages– Low overall sensitivity-0.85– Contrast mediated toxicity to donor organs
Transcranial Duplex US
• Classical findings in a patient who is brain dead are short systolic spikes or peaks, oscillating movement of blood within the assessed arteries, and disappearance of systolic flow on subsequent testing when previously documented as present
• TCD is not considered an accurate and reliable ancillary test in the confirmation of brain
• Advantages– Easily accessible, portable– Relatively inexpensive– No contrast agents
• Disadvantages– Lack of validation. Many false positives and
negatives– 20%- thick cranium
• Used as a screening tool

Brain Death Controversy
• Controversial• ?non acceptance of brain death as death.• The idea that irreversible loss of brain function is
a sufficient condition for the certification of death?
• Ariel Sharon? 8 years- vegetative state.– fMRI – response to stimuli from family?
• Jahi McMath?


One case study of reversible brain death.
• One case study• “reversible brain death after cardiopulmonary
arrest and induced hypothermia”• Webb Adam C. MD, Samuels, OwenB MD• Critical care Medicine June 2011 Vol 39- issue
6 pp 1538-1542• ICU of an academic tertiary care hospital

Reversible brain death?• 55 yo M• This patient had a PEA arrest from asthma with time to ROSC of 20mins. His
sats were 60% even before the arrest. • Cardiac arrest preceded by respiratory arrest.• Therapeutic hypothermia for neuroprotection. ?not indication to be cooled• After rewarming to 36’5, sluggishly reactive pupils, spontaneous myoclonic
movements, absent corneal reflexes, and intact gag and spontaneous respirations.
• Over 24 hours, remaining cranial nn function was lost. Clinical examination consistent with brain death. Apnea test and repeat clinical examination after 6 hours confirms brain death.
• Family consented for organ donation• 24 hours after brain death pronouncement, in OT, patient regained corneal
and cough reflex, and spontaneous respirations.
DBD,DNDD
• Problems with terminology. “brain death”, “cardiac death” and “circulatory death” is that they are inaccurate and potentially misleading.
• “Donation after Neurological Determination of Death” DNDD

• Failure to distinguish between patients who are “dead,” “brain-dead,” “in a chronic vegetative state,” “minimally conscious,” “comatose,” or “terminally ill but conscious” is a source of endless confusion.
1. Apart from identifying evidence of sufficient intracranial pathology, list the preconditions that must be met prior to the determination of brain death by clinical criteria.Minimum period of 4 hours in which the patient is observed to have unresponsive coma, unreactive pupils, absent cough/tracheal reflex and no spontaneous respiratory effort • Normothermia (temp >35oC) • Normotension (SBP >90 mmHg, MAP >60 mmHg in adult) • Exclusion of sedative drugs • Absence of severe electrolyte, metabolic or endocrine disturbance • Intact neuromuscular function • Ability to examine the brainstem reflexes including at least one ear and one eye • Ability to perform apnoea testing
2. What is the recommended minimum time for observation in cases of hypoxic- ischaemic brain injury, prior to performing clinical testing of brain-stem function? 24hours
Answers to CICM exam question
3. For each of the following brainstem reflexes, list the cranial nerves that are testeda. Cough reflex - cranial nerve Xb. Vestibulo-ocular reflex - cranial nerve III,IV,VI,VIIIc. Pupilary light reflex - cranial nerve II & IIId. Corneal reflex - cranial nerve V & VIIe. Gag reflex - cranial nerve IX & X(for each part of this question ALL cranial nerves are required in order to receive the 5 marks, no marks should be given for an incomplete response)
4. List three contraindications to performing apnoea testinga. Concomitant high cervical cord injury b. Severe hypoxaemiac. Haemodynamic instability
5. List the acceptable imaging techniques that may be used to demonstrate brain death as an alternative to clinical testing as recommended by the ANZICS Statement on Death and Organ Donation • Four vessel intra-arterial catheter angiography with digital
subtraction (preferred) • Radionuclide imaging with Tc-99mHMPAO and single photon
emission computerised tomography (SPECT) (preferred) • CT angiography (limited experience to date) (acceptable)