Embed Size (px)
DESCRIPTION
med
Citation preview

April 18, 2023 Theme III - Scientific Basis of Clinical Practice
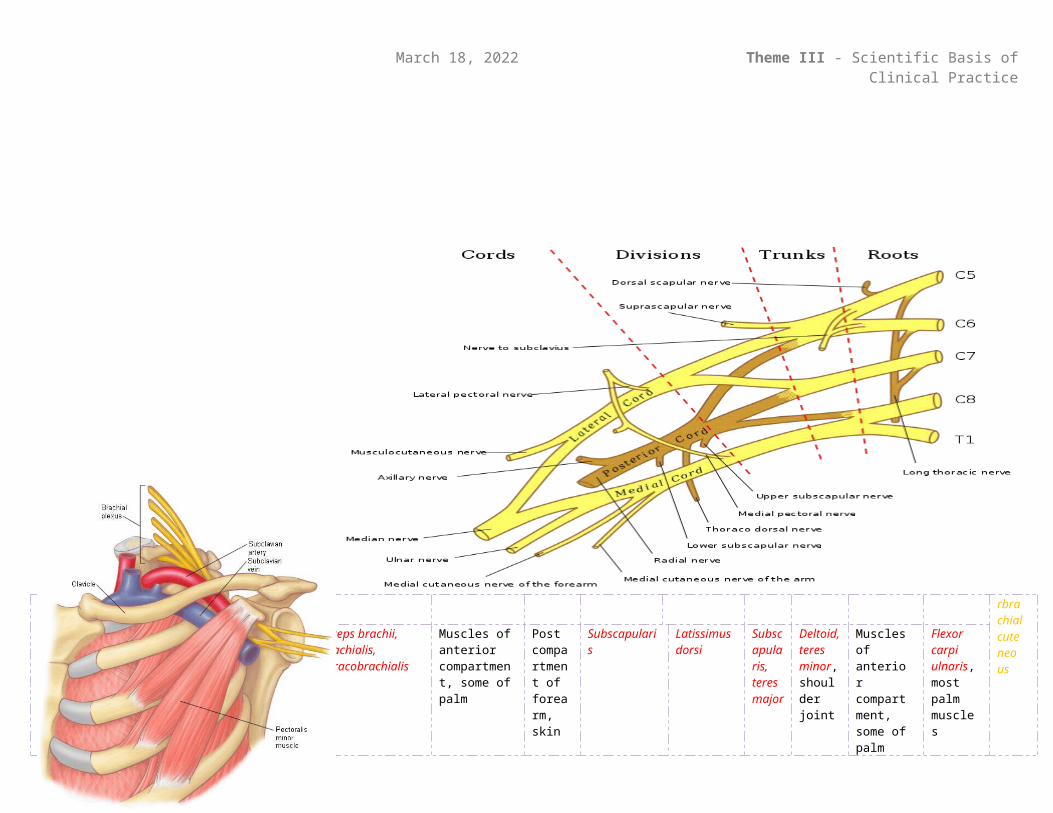
A plexus is a network of intersecting (intermingle but don’t join) nerves. Ventral rami (not T2-T12) merge with one or more adjacent anterior rami to form major somatic plexuses in which fibers intermingle and form a new set of multisegmental peripheral nerves, which contain fibers from multiple spinal nerves. Most nerves in the upper limb arise from the brachial plexus, protected proximally by the cervico-axillary canal and the axillary sheath. It is a complex network of merging and separating nerves, 5Rm3Ts6Dm3Cs3B, formed by the union of ventral rami C5-T1, which constitute the roots of the plexus. Almost all branches (terminal outgrowths) arise in the axilla, after the plexus has crossed the first rib.
ROOTS (emerge from intervertebral foramina, pass between anterior and middle scalene with subclavian artery)
C5Dorsal scapular nerve
arises superiorly - rhomboids
C6 C7 C8 T1
Long thoracic nerve leaves posteriorly – serratus anterior
TRUNKS (inferior trunk passes through subclavian artery groove posterior to scalene tubercle on first rib)
Superior trunkSubclavian nerve inferiorly - subclaviusSuprascapular nerve (runs through foramen of superior transverse scapular ligament, then along spine and winds around lateral border for i/spinatous) – supraspinatous, infraspinatous
Middle trunk Inferior trunkWith subclavian artery, traverses groove posterior to scalene tubercle of first rib
DIVISIONS (divisions pass through cervicoaxillary canal, under coracoid process, merging to cords occurs infraclavicularly). Anterior divisions supply flexor compartments, posterior divisions supply extensor compartments.
Anterior Posterior Anterior Posterior Posterior Anterior
CORDS (surround the axillary artery posteriorly, medially, and laterally)
Lateral cord - LML Posterior cord - ULTRA Medial cord - MMMMU
BRANCHES
Terminal branches are MARMU: Musculocutaneous C5-C7 Axillary C5-C6 Radial all Median all Ulnar C7-T1
Lateral pectoral nerve passes costacoracoid membrane to reach deep surface of pectoral muscles
Musculocutaneous nerve pierces coracobrachialis, descends between biceps brachii and brachialis, continues as lateral cutaneous nerve of forearm
Lateral branch of median nerve merges with medial root lateral to axillary artery, passes slightly medially in cubital fossa
Radial nerve passes posterior to humerus in radial groove,
Upper subscapular nerve passes posteriorly to enter subscapular fossa
Thoracodorsal nerve runs inferolaterally to apical part of latissimus dorsi
Lower subscapular nerve
Axillary nerve
Medial branch of the median nerve merges with lateral root
Ulnar nerve
Medial pectoral, medial brachial/anterbrachial cuteneous
Pectoralis major, pectoralis minor
Biceps brachii, brachialis, coracobrachialis
Muscles of anterior compartment, some of palm
Post compartment of forearm, skin
Subscapularis Latissimus dorsi
Subscapularis, teres major
Deltoid, teres minor, shoulder joint
Muscles of anterior compartment, some of palm
Flexor carpi ulnaris, most palm muscles
BRACHIAL PLEXUS
April 18, 2023 Theme III - Scientific Basis of Clinical Practice
Recall that injection of anaesthesia into or around the axillary sheath (proximal artery, vein, nerve) combined with an occlusive tourniquet produces upper limb nerve block, in which sensation is blocked to all deep muscles of the upper limb and the skin distal to the elbow.
Brachial plexus injuries influence movements and cutaneous sensation in the upper limb, resulting in paralysis and anaesthesia. These may be the result of

April 18, 2023 Theme III - Scientific Basis of Clinical Practice
Recall that injection of anaesthesia into or around the axillary sheath (proximal artery, vein, nerve) combined with an occlusive tourniquet produces upper limb nerve block, in which sensation is blocked to all deep muscles of the upper limb and the skin distal to the elbow.
Brachial plexus injuries influence movements and cutaneous sensation in the upper limb, resulting in paralysis and anaesthesia. These may be the result of
A, C – Excessive increase in neck/shoulder angle cause
B – Waiter’s tip position
D, E – Upper limb pulled superiorly cause
F – Claw hand