-
Musculoskeletal diseasestendon
Tomoya Sakabe, and Takao Sakai,*
Department of Biomedical Engineering, Lerner Research Institute,
Cleveland Clinic, Cleveland, OH44195, USA, and Orthopaedic and
Rheumatologic Research Center, Cleveland Clinic, Cleveland,OH
44195, USA
Introduction: Tendons establish specific connections between
muscles and the
skeleton by transferring contraction forces from skeletal muscle
to bone thereby
allowing body movement. Tendon physiology and pathology are
heavily
dependent on mechanical stimuli. Tendon injuries clinically
represent a serious
and still unresolved problem since damaged tendon tissues heal
very slowly
and no surgical treatment can restore a damaged tendon to its
normal structural
integrity and mechanical strength. Understanding how mechanical
stimuli
regulate tendon tissue homeostasis and regeneration will improve
the treatment
of adult tendon injuries that still pose a great challenge in
todays medicine.
Source of data: This review summarizes the current status of
tendon treatment
and discusses new directions from the point of view of
cell-based therapy and
regenerative medicine approach. We searched the available
literature using
PubMed for relevant original articles and reviews.
Growing points: Identification of tendon cell markers has
enabled us to study
precisely tendon healing and homeostasis. Clinically, tissue
engineering for
tendon injuries is an emerging technology comprising elements
from the fields
of cellular source, scaffold materials, growth factors/cytokines
and gene
delivering systems.
Areas timely for developing research: The clinical settings to
establish
appropriate microenvironment for injured tendons with the
combination of
these novel cellular- and molecular-based scaffolds will be
critical for the
treatment.
Keywords: tendon injury/tissue engineering/regenerative
medicine/stem cells/scleraxis/mechanical force
Accepted: May 3, 2011
British Medical Bulletin 2011; 115
DOI:10.1093/bmb/ldr025
& The Author 2011. Published by Oxford University Press.
All rights reserved. For permissions, please e-mail:
[email protected]
*Correspondence address:
Department of
Biomedical Engineering,
Lerner Research Institute,
Cleveland Clinic, ND20,
9500 Euclid Avenue,
Cleveland, OH 44195,
USA. E-mail: sakait@ccf.
org
British Medical Bulletin Advance Access published July 4, 2011
by guest on A
ugust 7, 2015http://bm
b.oxfordjournals.org/D
ownloaded from
-
Tendon physiology
Tendon, a fibrous connective tissue made of specialized
fibroblastscalled tenocytes and an abundant collagenous
extracellular matrix(ECM), is a tissue whose physiology and
pathology is heavily depen-dent on mechanical stimuli.1 Tendons
establish specific connectionsbetween muscles and the skeleton by
transferring contraction forcesfrom skeletal muscle to bone,
thereby allowing body movement.2
Tendons exhibit high mechanical strength, good flexibility and
anoptimal level of elasticity to perform their unique role. The
tensilestrength of a tendon is related to its thickness and
collagen content: forexample, a tendon with an area of 1 cm2 is
capable of bearing 5001000 kg.3 Tendons have relatively few blood
vessels and function at alow metabolic rate. Tendons receive oxygen
and nutrients from threemain sources: internally via the
myotendinous junction and osteotendi-nous junctions, and externally
through the paratenon or the synovialsheath.4
Tendon development and adult homeostasis
During embryonic development, tenocytes originate from
mesodermalcompartments, as do skeletal myoblasts, chondrocytes and
osteoblasts.5
Some of the multipotent mesenchymal progenitor cells that arise
fromthese compartments express the basic helix-loop-helix
transcriptionfactor scleraxis. However, once they are committed to
become cellsmaking up a specific tissue, only tendon progenitor
cells and tenocytesretain the ability to express scleraxis.
Therefore, scleraxis is a highlyspecific marker of tenogenic cells
and mature differentiated teno-cytes.6,7 The scleraxis gene is thus
the first master gene found to beessential for establishing the
tendon lineage during development.8
Tenomodulin is a type II transmembrane glycoprotein. Its
robustexpression is induced in mouse tendons in a late (embryonic
day [E]17.5) developmental phase and is also observed in adult
tendonsshowing that tenomodulin is a marker of mature
(differentiated) teno-cytes.9 In vitro experimental evidence shows
that the genes composedof tendon-specific ECM are tightly regulated
in tenocytes by mechan-ical forces.2 Very recently, tendon
stem/progenitor cells have been dis-covered in human and mouse
tendon, and the proteoglycans biglycanand fibromodulin have been
identified as essential elements in a micro-environment to keep
phenotypes and differentiation of stem/progenitorcells.10 However,
the roles of these stem/progenitor cells in adulttendon homeostasis
and/or wound healing remains unknown.
T. Sakabe and T. Sakai
Page 2 of 15 British Medical Bulletin 2011
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
Mechanical force and tenocytes
Since tendon tissues are constantly exposed to variable
transmittalforces from skeletal muscles, our laboratory examined
the functionallinks between mechanical forces and tenocyte
phenotypes using scler-axis as a tenocyte marker. We utilized a
transgenic mouse strain, whichexpresses the green fluorescent
protein (GFP) marker driven by thescleraxis gene in a way that GFP
is produced in a pattern that mimicsits expression in the body6
(Scleraxis-GFP transgenic mice were kindlyprovided by Dr Ronen
Schweitzer, Research Division, ShrinersHospital for Children,
Portland, OR, USA). The vast majority of teno-cytes show robust
expression of scleraxis-GFP in adult tendon tissuesunder the
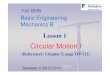
fluorescence microscope (Fig. 1a). Strikingly, the
suddeninterruption of continuous tensile loading, such as by
complete transec-tion tendon injury, leads to a decreased
expression of scleraxis andtenocyte death (Fig. 1b). Thus, these
findings indicate a critical role formechanical forces in adult
tendon homeostasis and strongly suggestnew directions for therapy
following tendon injuries.11
Tendon injury
Incidence of tendon injury
Soft-tissue injuries, including injury to tendon, ligament or
meniscus,can induce abnormal joint motions and altered loading in
the shortterm and they could contribute to degenerative joint
disease and osteo-arthritis in the long term.12. These injuries can
be acute or chronic andare caused by intrinsic or extrinsic
factors, either alone or in
Fig. 1 Tensile loading plays a crucial role in tenocytes. (a)
Achilles tendons in adultScleraxis-GFP transgenic mice. Left panel:
under fluorescence stereomicroscope; rightpanel: under microscope
with GFP/ultraviolet (UV) filters to show scleraxis-GFP (green)
andnucleus [406-diamidino-2-phenylinodole (DAPI) blue]. AT,
Achilles tendon. Bar 100 mm. (b)Analysis of cell death at 2 h after
complete transection of adult Achilles tendon inScleraxis-GFP
transgenic mice. Arrows indicate the transection edge of tendons.
Note thatthe expression of scleraxis-GFP (green) is diminished and
cells positive by terminal deoxy-nucleotidyl transferase dUTP
nick-end labeling assay (TUNEL assay: a marker for cell death,red)
are evident in the transected Achilles tendon. Bar 100 mm.
Strategies for treatment in tendon injury
British Medical Bulletin 2011 Page 3 of 15
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
combination.4 Acute tendon injury interrupts tendon continuity
withconsequent disruption of ECM architecture and dramatic loss of
trans-mittal forces from skeletal muscle.4 Tendon injuries
represent a seriousand still unresolved problem. More than 130 000
patients per yearundergo tendon-related surgery in the USA.13 The
tendons most fre-quently affected are shoulder rotator cuff (51 000
cases), Achillestendon (44 000 cases) and patellar tendon (42 000
cases).13 Injuries toAchilles tendon, patellar tendon, hand flexor
tendon and shoulderrotator cuff have clinical importance since they
can lead to loss ofmuscle function, significant disability, joint
instability and secondaryosteoarthritis, adversely affecting a
patients activities of daily livingand quality of life. The
incidence of tendon injury has increased inrecent years as the
number of aging adults continues to grow.14 Thealtered activity of
mechanical loading, and vasculature and angiogen-esis are suggested
to play a significant role in degenerative tendondiseases.15,16
Tendon healing
Tendon wound healing involves regeneration of tenocytes and
recon-struction of dense collagen fibrils, and the tendon repair
process intransected experimental animal tendons is known to
involve three over-lapping phases, as for other
organs/tissues.4,13. An initial, inflammatoryphase occurs until Day
2 after injury. It involves extensive cell death inthe injured area
and subsequent inflammatory cell infiltration. Asecond,
proliferative phase starts at Day 3. It involves cell migrationinto
the injured area, extensive proliferation and production of
collagenfibrils. A third, remodeling phase occurs from 6 weeks on.
This phasecan be divided into a consolidation stage, from 6 to 10
weeks afterinjury, and a maturation stage, after 10 weeks. It is
characterized bydecreased cellularity and collagen synthesis, and
the alignment of teno-cytes and collagen fibrils in the direction
of stress. ECM-remodelingduring tendon wound healing follows in
general the same processes asin other tissues, i.e. in an early
stage, provisional matrix formation bythe plasma proteins
fibrinogen and fibronectin, followed by replace-ment of the
provisional matrix by collagen fibrils.2,4
In the inflammatory phase, vasoactive and chemotactic factors
suchas cytokines and growth factors are released and lead to an
increasedvascular permeability, initiation of angiogenesis and
stimulation oftenocyte proliferation. In particular, various growth
factors/cytokinesplay a number of important roles, including
stimulation of tenocyteproliferation, cell migration to the wound
and synthesis of the newECM during tendon healing.17,18 In the
proliferation phase, two
T. Sakabe and T. Sakai
Page 4 of 15 British Medical Bulletin 2011
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
mechanisms, intrinsic and extrinsic mechanisms, are likely to
contrib-ute to the healing process. The intrinsic mechanism
involves the pro-liferation of tenocytes from the tendon and
epitenon. These tenocytescontribute to synthesize the new ECM,
which consists largely of col-lagens and glycosaminoglycans. Such
intrinsic healing results inimproved biomechanics and fewer
post-injury complications. In con-trast, the extrinsic mechanism
involves the migration of inflammatorycells and fibroblasts from
the overlying sheath and synovium into thewounded site.4,19 This
often causes scar tissue and results in adhesionformation, which
disrupts tendon gliding. Although tendon healingfollows the same
process as that in various connective tissues, includingskin and
muscle, tendon tissues heal more slowly than other
connectivetissues, probably because of the low metabolic rate of
tendons andtheir dense and hypocellular composition (only 5% of the
volume isoccupied by cells).4,5 Furthermore, ECM remodeling such as
increasingdiameters and cross-linking of collagen fibrils occurs
over a period ofup to 2 years following tendon injury.3 Despite
such remodeling, thebiochemical and mechanical properties of healed
tendons never matchthose of intact ones.3 The final tensile
strength in the healed tendons iseventually reduced to 30% the
strength of intact tendons.20
Therapies in tendon in injury
General concepts in therapies in tendon injury
Clinically, two main strategies for treating injured tendons are
fol-lowed:21 (i) leave them untreated to heal naturally or (ii)
performsurgery for primary repair of injured tendons using various
techniques(Table 1). These treatments are determined in general
according toclinical factors, such as age, tendon location, mode of
injury and sizeof defect. Surgical treatment of an acute Achilles
tendon rupture hasbeen considered superior to non-operative
treatment to prevent the riskof re-rupture.22,23 However,
investigators in a recent multicenter ran-domized trial
(NCT00284648 in ClinicalTrials.gov) reported thatsimilar clinical
outcomes are observed between (i) non-operativegroups with
accelerated functional rehabilitation and (ii) operativegroups.24
Thus, the treatment for acute Achilles tendon ruptureremains
inconclusive.22,24 Furthermore, for injuries to the hand
flexortendon or shoulder rotator cuff, long-term clinical outcomes
ofprimary repair remain unsatisfactory.13,25 Despite improved
surgicaltechniques and advances in postoperative therapy regimens,
these treat-ments still have potential complications such as
re-rupture of the repairsite or the formation of restrictive
adhesions.25,26 Recently, the
Strategies for treatment in tendon injury
British Medical Bulletin 2011 Page 5 of 15
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
biological grafts, such as autologous fascia, porcine small
intestinalsubmucosa or synthetic materials, have been developed and
used intendon graft procedures to fill large tissue defects (Table
2). However,no graft method exists to restore a damaged tendon to
its normal func-tion. Grafting poses several potential
complications, includingincreased inflammatory responses, antigenic
reactions, failure at thefixation sites and deficiencies in
long-term biocompatibility.25,26 Thus,current knowledge of the
biology in tendon healing has yet to lead toclinically successful
strategies for treatment.19 New treatment modal-ities are required
to promote the regeneration of tendon tissues.
Table 1 Characteristics for treatment in tendon injury.
Treatment type Indication Advantages Disadvantages
Immobilization Acute Achilles tendon
rupture
No surgical complication Failure to heal
Plaster Tendinopathy Rerupture
Brace Muscle atrophy
Tendon atrophy
Limitation of range of motion
Decreasing of tensile strength
Primary repair Most acute tendon
injury
First clinical choice Suture failure
Chronic tear of
rotator cuff
Recovery of muscle
contraction
Rerupture
Inability to achieve functional
results
Postoperative adhesion
Infection
Tendon transfer Large tendon defect Filling of tissue defect
Suture failure
Primary repair failure Recovery of muscle
contraction
Rerupture
Chronic tendon injury Inability to achieve functional
results
Postoperative adhesion
Infection
Altered biomechanics of joint
Tendon graft Large tendon defect Filling of tissue defect Suture
failure
Autograft Primary repair failure Recovery of muscle
contraction
Rerupture
Allograft Chronic tendon injury Inability to achieve
functional
results
Xenograft Destructive disease Postoperative adhesion
Synthetic
material
Congenital disorder Infection
Limited availability of
material
Altered biomechanics of joint
Deficiency of biocompatibility
Immunologic rejection
Antigenic reaction
Disease transmission
T. Sakabe and T. Sakai
Page 6 of 15 British Medical Bulletin 2011
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
New treatment strategies for tendon healing
To design efficient strategies to enhance tendon repair
following injury,it is essential that scientists and clinicians
understand the cellular andmolecular mechanisms responsible for the
development, homeostasis,regeneration and repair of tendons. To
date, however, the molecularmechanisms underlying tendon repair
remain largely unknown. Thetarget molecules for tendon repair are
based on knowledge fromgeneral wound healing, not on results
generated specifically fromanalysis of tendon healing.27
Tissue engineering is an emerging technology that offers a
novelapproach for treating tendon injuries and restoring tissue and
jointfunction.28 The most common tissue-engineering principles are
(i) theuse of healthy multipotent cells that are non-immunogenic,
easy toisolate and highly responsive to distinct environmental
cues; (ii) thedevelopment of carrier scaffolds that provide
short-term mechanicalstability of the transplant as well as a
template for spatial growth ofthe regenerating tissue; and (iii)
the delivery of growth factors thatdrive the process of cell
differentiation and maturation.25
Orthopedic tissue engineering comprises elements from the fields
ofcell biology, materials science, mechanical engineering and
surgery.12
Various types of scaffolds, such as naturally occurring ECMs as
well ascell-based strategies have been developed12,25,26,2933
(Table 2).Mesenchymal stem cells (MSCs) are becoming a subject of
increasinginterest because of their potential utility in
tissue-engineering appli-cations34,35 (Table 3). MSCs exist in
adult bone marrow and can beinduced to form different mesenchymal
tissue lineage cells such as
Table 2 Scaffold materials for tendon injury.
Biologic (naturally occurring)
Human tissue Dermis
Dura mater
Animal tissue Porcine small intestinal submucosa
Porcine dermis
Biopolymers Type I collagen
Synthetic (manufactured)
Resorbable Polyethylene
Polyglycolic acid
Polylactic acid
Poly-N-acetyl-D-glucosamine
Non-resorbable Carbon fibers
Dacronw
Nylon
Polyacrylamide
Silicone
Teflonw
Silk
Strategies for treatment in tendon injury
British Medical Bulletin 2011 Page 7 of 15
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
chondrocytes, adipocytes or osteoblasts. In fact, MSCs-based
scaffoldshave been tried in animal models of tendon wound
healing.
Cellular scaffold-based therapy
Scaffolds
The underlying concept for tissue engineering technologies has
beenchanging. Traditionally, a graft was composed of some material
(suchas nylon or silk) meant solely to fill the tissue defect.
Nowadays,implants are expected to serve as biocompatible scaffolds
(natural orsynthetic materials that can be replaced by host tissues
without undesir-able responses). These biocompatible scaffolds are
suitable as vehiclesfor implanted cells, the delivery of growth
factors, or the transfer of
Table 3 New modalities for treatment in tendon injury.
Treatment type Methods of delivery Advantages Disadvantages
Scaffolds
Biologic material Direct implantation Abundant supply (type
I
collagen)
Limited clinical
applications (autograft)
Limited recovery of
strength
Relatively low
complications (type I
collagen)
Potential complications as
in Table 1
Synthetic
material
Direct implantation Abundant supply Limited recovery of
strength
Limited regeneration
Potential complications as
in Table 1
Cell therapy
Tenocyte Direct implantation
with collagen materials
Differentiated cell Limited cellular source
Low proliferative ability
Low morbidity
Mesenchymal
stem cell
Direct implantation
with collagen materials
Excellent regenerative
capacity
Unclearness of
mechanisms in
differentiation
High proliferative ability
Low morbidity
Invasive procurement
procedure
Low yielding
Growth factors Direct administration Easy administration
Unclearness of growth
factor stability
Unclearness of effective
concentration
Gene therapy
Viral method Direct viral infection High transduction
efficiency
Inflammatory response
Transient expression Non-specific infection
Non-viral
method
Direct administration
with liposomes
Low pathogenic response Relatively low
transduction efficiency
T. Sakabe and T. Sakai
Page 8 of 15 British Medical Bulletin 2011
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
genes25,26. Both biologic and synthetic materials are used to
create scaf-folds for tendon reconstruction with a
three-dimensional biocompatibleconstruct that serves as a temporary
or permanent implant26. Asdescribed, injured tendons have very
limited spontaneous healing capa-bilities. Thus, ideal scaffold
materials need to play at least two essentialroles: to stimulate
regeneration (including proliferation and differen-tiation of
cells) at implanted sites and to establish the specific
compo-sition and structure of an ECM that can then provide an
appropriatemicroenvironment for regenerating cells. The major ECM
componentin tendons is type I collagen. The advantages of using
type I collagenfor tendon reconstruction include its strength,
capacity to resorb andability to induce the alignment of host
connective tissues.26. Scaffoldsof type I collagen cross-linked
with glutaraldehyde or carbodiimide areused in research to
regenerate tendon tissue because of the low antige-nicity and
strength.26,36 Indeed, they have improved graft strength in arabbit
Achilles tendon model.36 Synthetic non-resorbable
materials,including nylon, silk and carbon, are not biocompatible
because ofhost foreign body responses and late mechanical
failure.26 To circum-vent these problems, synthetic resorbable
materials have been devel-oped using polyglycolic acid or
polylactic acid.25 They can befabricated into three-dimensional
scaffolds of variable structure andporosity with a correspondingly
wide range of mechanical and degra-dation properties.25
Unfortunately, some synthetic resorbable scaffoldsalter the
mechanical properties of the repaired tendon, lose strengthand
integrity over time, limit tendon ingrowth, cause abrasions of
sur-rounding tissues, enhance the inflammatory response and cause
unde-sirable scar formation around the repair site.26 A study in a
goatshoulder rotator-cuff repair model indicates that the
polylactic acid-scaffold does not show significant increase in the
load-to-failurestrength, even though the polylactic acid patch is
occupied by cellularfibrous tissues.37 Therefore, despite their
potential roles in tendonreconstruction, further investigation will
be necessary to find analternative to natural materials.
Cell-based therapyCell-based therapy is also a novel technique
to improve the compo-sition, structure and biomechanical properties
of new tendon tissue:cells are initially seeded onto scaffolds, and
then they are delivered tothe injured sites as cell- and
scaffold-combined materials.26 To date,several different
combinations of cell types and biomaterial scaffoldshave been used
in experimental animal models (including MSCs-type Icollagen gel,
MSCs-knitted polylactide-co-glycolide matrix,tenocytes-non-woven
polyglycolic acid fibers), and they have thecapacity to enhance
tendon formations.3033,38 In these biomaterial
Strategies for treatment in tendon injury
British Medical Bulletin 2011 Page 9 of 15
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
scaffolds, a plenty of materials such as collagen gel or
synthetic biode-gradable polymers are commercially available. On
the other hand, cellsseeded on such a scaffold need to proliferate
rapidly in vitro to provideadequate numbers for in vivo
implantation.25 An important prerequi-site for cell-based therapy
is the successful isolation and selection ofappropriate cells.25 A
tenocyte-based method is one of the potentialcell-based therapies,
but a number of concerns still limit the practicalityof its use:
(i) a limited availability of donor sites tenocytes from
whichtenocytes may be obtained for implantation, (ii) the time
requirementsfor lengthy in vitro culture to expand the number of
cells and (iii) themorbidity of tenocytes themselves.39 To
circumvent the negativeimpact of this tenocyte-based method, MSCs
have been investigated asan alternative source for tendon
engineering. MSCs, which show anexcellent capability for
regeneration and rapid proliferation, have thepotential to
differentiate into a spectrum of specialized mesenchymaltissues,
tendon, ligament, bone, cartilage, muscle, fat and marrowstroma.25
In addition, MSCs can be relatively easily isolated from
bonemarrow, but they are also found in muscle, adipose tissue, skin
andaround blood vessels.40 The ability of MSCs for tendinogenic
differen-tiation has been documented in several studies.3133 In
fact, recruit-ment of MSCs to accelerate repair and tissue
regeneration was shownin vivo in a rabbit tendon tissue model.32
However, no significantdifferences were observed in mechanical
properties betweenMSC-transplanted and non-transplanted repaired
tissues. Moreover,28% of MSC-treated tendons developed foci of
ectopic bone, whereasno bone formed in naturally healing
contralateral controls.29,41 Thesestudies clearly indicate that the
determination of an appropriate MSCmicroenvironment for tenocyte
differentiation is a critical issue thatneeds further
investigation. We also need to take into considerationseveral more
issues relating to the clinical application of MSC-basedtherapy:
long-term safety of the patient, large-scale culture and storageof
cells, ideal scaffold materials, optimal cell seeding conditions
and analternative mode of applying MSC-material composite to the
injuredsite.4,25
Molecular-based therapy
Growth factors and cytokines
Growth factors/cytokines represent one of the largest
molecularfamilies involved in the wound healing process, and a
considerablenumber of studies have been undertaken in an effort to
elucidate theirmany functions and behaviours during healing
progression.17 Severalmolecules have been identified as key factors
during the repair processof tendons, including transforming growth
factor-b (TGF-b), insulin-like growth factor 1 (IGF-1),
platelet-derived growth factor (PDGF),
T. Sakabe and T. Sakai
Page 10 of 15 British Medical Bulletin 2011
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
vascular endothelial growth factor (VEGF), basic fibroblast
growthfactor (bFGF) and growth and differentiation factor
(GDF)-5through 7.26 Since TGF-b regulates a wide variety of
cellular processes,including the expression of scleraxis during
tendon formation inembryonic development,42 such multifunctional
aspects of TGF-b havebeen extensively studied in relation to adult
tendon injury and homeo-stasis. The expression levels of TGF-b in
adult tendons are dramaticallyupregulated in a short time after
injury, and TGF-b initiates an inflam-matory response to tissue
damage.17 In contrast, TGF-b upregulatesthe production of ECMs,
which results in excessive scar formation.Indeed, the local
administration of a neutralizing antibody of TGF-bcan diminish
excessive production of ECM and improve the postopera-tive range of
motion in a rabbit model of complete transection of thehand flexor
tendon.43 Thus, such contradictory functional aspects ofTGF-b make
it difficult to rely on TGF-b for clinical use in tendonhealing.3
IGF-1 stimulates synthesis of DNA, collagen and proteogly-cans, as
well as tenocyte proliferation and migration in vitro.44 IGF-1also
acts synergistically with PDGF to stimulate tenocyte
migration.44
A study in a rat Achilles tendon transection model indicates
that theinjection of IGF-1 at injured sites accelerates functional
recovery ofAchilles tendon.45 GDF-5, -6 and -7 (members of the
TGF-b superfam-ily that are related to bone morphogenetic proteins)
can induce neoten-don formation, as assessed by histochemical
analysis when injected atsubcutaneous sites in rats.18 Another
study shows that the injection ofGDF-5, -6 or -7 into injured
Achilles tendons in rats results in a signifi-cant dose-related
increase of mechanical properties in rat Achillestendon.46
Some success has been achieved utilizing single growth factors
astherapeutics.17 Direct injection of a growth factor at the
injured site maygive a temporary boost of a single healing signal
but has only limitedeffect on the final outcome.17 The combination
of patients own growthfactors to promote healing in injured tissues
is a potentially very fruitfularea of research.17 Platelet-rich
plasma (PRP), easily harvested fromwhole blood by a few
centrifugation steps, contains autologous growthfactors such as
PDGF, TGF-b, IGF-1 and -2 and bFGF.47 Postoperativedirect injection
of PRP significantly improves mechanical strength andstiffness in a
rat Achilles tendon repair model.48 Recently, there has
beenincreasing interest in the field of sports medicine to
facilitate healing andearlier return to activity after tendon and
ligament injury.49 Severalclinical trials investigating the
efficacy of PRP treatment have been per-formed for Achilles tendon
rupture (NCT00731068 in ClinicalTrials.gov) and rotator cuff injury
(NCT01000935; NCT01152658;NCT01170312 in ClinicalTrials.gov).
However, recent randomized
Strategies for treatment in tendon injury
British Medical Bulletin 2011 Page 11 of 15
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
clinical trials indicate that PRP treatment has no significant
effect on thehealing of tendon and ligament injuries.49,50
Gene therapy
A variety of gene transfer methods have been used both in vitro
and invivo to induce local production of growth factors such as
GDF-7 orPDGF by means of viral (e.g. adenovirus, retrovirus) or
non-viralvectors (e.g. liposomes) to accelerate the tendon repair
process.51,52
The use of a non-viral vector-mediated delivery is less
pathogenicbecause of the absence of viral proteins but is also less
efficient thanthe use of viral vectors.25 The expression of a
transgene is transient butgenerally manipulated for up to 810
weeks: this method is more ben-eficial than repeating local
injection of growth factors/cytokines.3,25 Todate, the recombinant
viral system is well suited for a study of itspotential as a
therapy of tendon injuries using experimental animalmodels. Two
main strategies for gene transfer using vectors can beenvisioned:
(i) in vivo transfer with a vector that is applied directly tothe
relevant tissue (in vivo direct gene transfer method) and (ii)
theremoval of cells from the body, transfer of the gene in vitro,
and thenreintroduction into the target site in the body (ex vivo
indirect genetransfer method).25 The in vivo direct gene transfer
method is less inva-sive and technically easier than transfer of
cells in vitro. However, thedisadvantages of in vivo transfer are
potential inflammatory responsesand non-specific infections at the
injury site. The ex vivo indirect genetransfer method can ensure
the collection of only selected/targeted cellsin vitro that express
the transgene at high concentrations to the injurysite with less
chance of contamination of viral DNA and proteins.Therefore, the ex
vivo indirect gene transfer method could be prefer-able for the
treatment of a large and degenerative tendon injury such asthat to
the rotator cuff, rather than an acute tendon injury.
Future directions for tendon injury treatment
Tendon injuries clinically represent the serious and still
unresolvedproblem of how best to restore a damaged tendon to more
nearlynormal structural integrity and mechanical strength.
Considering theunique feature of tendons with their constant and
high mechanicalloading, new treatment modalities are required to
promote the regener-ation of tendon tissues. Tissue engineering
offers many approaches fortreating tendon injuries and restoring
tissues and joint functions.Indeed, a variety of synthetic and
biologic scaffolds have been devel-oped. The combination of several
scaffolds, including syntheticmaterials, cells such as MSCs or
tendon progenitor cells and growth
T. Sakabe and T. Sakai
Page 12 of 15 British Medical Bulletin 2011
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
factors/cytokines, could be an attractive way to generate an
appropriatemicroenvironment for both transplanted and tendon cells
at the injuredsite. We also foresee many other novel cellular
sources and technol-ogies, induced pluripotent stem (iPS) cells or
tendon stem/progenitorcells and nanomedicine scaffolds. The
emerging interventions usingthose orthopaedic tissue engineering
technologies have shown a thera-peutic effect in experimental
animal models of tendon injury.However, their efficacy and safety
in humans remains to be elucidatedin the clinical setting.
Unfortunately, to date, the development of newtreatment strategies
for injured tendons has been hindered because ofour limited
understanding of basic tendon biology. Nevertheless, thetranslation
of basic research into improved therapeutic approaches isan
essential step in the management of patients with tendon
injuries,having the potential for significant benefit to public
health.
Acknowledgements
We wish to acknowledge many outstanding contributions of
investi-gators in the field whose work could not be cited because
of spaceconstraints.
Funding
This work was supported in part by National Institutes of
Health,grant no. R01 DK074538, The Cleveland Clinic and the
SumitomoFoundation, Japan (to T. Sakai).
References
1 Zhang G, Young BB, Ezura Y et al. Development of tendon
structure and function: regulationof collagen fibrillogenesis. J
Musculoskelet Neuronal Interact 2005;5:521.
2 Kjaer M. Role of extracellular matrix in adaptation of tendon
and skeletal muscle to mechan-ical loading. Physiol Rev
2004;84:64998.
3 Sharma P, Maffulli N. The future: rehabilitation, gene
therapy, optimization of healing. FootAnkle Clin 2005;10:38397.
4 Sharma P, Maffulli N. Tendon injury and tendinopathy: healing
and repair. J Bone Joint SurgAm 2005;87:187202.
5 Tozer S, Duprez D. Tendon and ligament: development, repair
and disease. Birth Defects ResC Embryo Today 2005;75:22636.
6 Pryce BA, Brent AE, Murchison ND et al. Generation of
transgenic tendon reporters,ScxGFP and ScxAP, using regulatory
elements of the scleraxis gene. Dev Dyn2007;236:167782.
7 Schweitzer R, Chyung JH, Murtaugh LC et al. Analysis of the
tendon cell fate usingScleraxis, a specific marker for tendons and
ligaments. Development 2001;128:385566.
Strategies for treatment in tendon injury
British Medical Bulletin 2011 Page 13 of 15
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
8 Schweitzer R, Zelzer E, Volk T. Connecting muscles to tendons:
tendons and musculoskeletal
development in flies and vertebrates. Development
2010;137:280717.9 Docheva D, Hunziker EB, Fassler R et al.
Tenomodulin is necessary for tenocyte proliferation
and tendon maturation. Mol Cell Biol 2005;25:699705.10 Bi Y,
Ehirchiou D, Kilts TM et al. Identification of tendon
stem/progenitor cells and the role
of the extracellular matrix in their niche. Nat Med
2007;13:121927.11 Maeda T, Sakabe T, Sunaga A et al. Conversion of
mechanical force into TGF-b-mediated bio-
chemical signals. Curr Biol 2011. [Epub ahead of print].12
Butler DL, Shearn JT, Juncosa N et al. Functional tissue
engineering parameters toward
designing repair and replacement strategies. Clin Orthop Relat
Res 2004;427S:S1909.13 Butler DL, Juncosa N, Dressler MR.
Functional efficacy of tendon repair processes. Annu
Rev Biomed Eng 2004;6:30329.14 Jozsa L, Kannus P.
Histopathological findings in spontaneous tendon ruptures. Scand J
Med
Sci Sports 1997;7:1138.15 Pufe T, Petersen WJ, Mentlein R et al.
The role of vasculature and angiogenesis for the patho-
genesis of degenerative tendons disease. Scand J Med Sci Sports
2005;15:21122.16 Boesen MI, Koenig MJ, Torp-Pedersen S et al.
Tendinopathy and Doppler activity: the vascu-
lar response of the Achilles tendon to exercise. Scand J Med Sci
Sports 2006;16:4639.17 Molloy T, Wang Y, Murrell G. The roles of
growth factors in tendon and ligament healing.
Sports Med 2003;33:38194.18 Wolfman NM, Hattersley G, Cox K et
al. Ectopic induction of tendon and ligament in rats
by growth and differentiation factors 5, 6, and 7, members of
the TGF-beta gene family. JClin Invest 1997;100:32130.
19 Hsu C, Chang J. Clinical implications of growth factors in
flexor tendon wound healing. JHand Surg Am 2004;29:55163.
20 Leadbetter WB. Cell-matrix response in tendon injury. Clin
Sports Med 1992;11:53378.21 Maffulli N, Longo UG, Denaro V. Novel
approaches for the management of tendinopathy. J
Bone Joint Surg Am 2010;92:260413.22 Bhandari M, Guyatt GH,
Siddiqui F et al. Treatment of acute Achilles tendon ruptures: a
sys-
tematic overview and metaanalysis. Clin Orthop Relat Res
2002;400:190200.23 Metz R, Verleisdonk EJ, van der Heijden GJ et
al. Acute Achilles tendon rupture: minimally
invasive surgery versus nonoperative treatment with immediate
full weightbearinga ran-domized controlled trial. Am J Sports Med
2008;36:168894.
24 Willits K, Amendola A, Bryant D et al. Operative versus
nonoperative treatment of acuteAchilles tendon ruptures: a
multicenter randomized trial using accelerated functional
rehabili-tation. J Bone Joint Surg Am 2010;92:276775.
25 Huang D, Balian G, Chhabra AB. Tendon tissue engineering and
gene transfer: the future of
surgical treatment. J Hand Surg Am 2006;31:693704.26 DeFranco
MJ, Derwin K, Iannotti JP. New therapies in tendon reconstruction.
J Am Acad
Orthop Surg 2004;12:298304.27 Hildebrand KA, Frank CB, Hart DA.
Gene intervention in ligament and tendon: current
status, challenges, future directions. Gene Ther
2004;11:36878.28 Rodeo SA, Delos D, Weber A et al. Whats new in
orthopaedic research. J Bone Joint Surg
Am 2010;92:2491501.29 Awad HA, Boivin GP, Dressler MR et al.
Repair of patellar tendon injuries using a cell-
collagen composite. J Orthop Res 2003;21:42031.30 Cao Y, Vacanti
JP, Ma X et al. Generation of neo-tendon using synthetic polymers
seeded
with tenocytes. Transplant Proc 1994;26:33902.31 Butler DL, Awad
HA. Perspectives on cell and collagen composites for tendon repair.
Clin
Orthop Relat Res 1999;367S:S32432.32 Young RG, Butler DL, Weber
W et al. Use of mesenchymal stem cells in a collagen matrix
for Achilles tendon repair. J Orthop Res 1998;16:40613.33 Awad
HA, Butler DL, Boivin GP et al. Autologous mesenchymal stem
cell-mediated repair of
tendon. Tissue Eng 1999;5:26777.34 Caplan AI. Review:
mesenchymal stem cells: cell-based reconstructive therapy in
orthopedics.
Tissue Eng 2005;11:1198211.
T. Sakabe and T. Sakai
Page 14 of 15 British Medical Bulletin 2011
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from
-
35 Shenaq DS, Rastegar F, Petkovic D et al. Mesenchymal
progenitor cells and their orthopedicapplications: forging a path
towards clinical trials. Stem Cells Int 2010;2010:519028.
36 Kato YP, Dunn MG, Zawadsky JP et al. Regeneration of Achilles
tendon with a collagentendon prosthesis. Results of a one-year
implantation study. J Bone Joint Surg Am1991;73:56174.
37 MacGillivray JD, Fealy S, Terry MA et al. Biomechanical
evaluation of a rotator cuff defectmodel augmented with a
bioresorbable scaffold in goats. J Shoulder Elbow
Surg2006;15:63944.
38 Ouyang HW, Goh JC, Thambyah A et al. Knitted
poly-lactide-co-glycolide scaffold loadedwith bone marrow stromal
cells in repair and regeneration of rabbit Achilles tendon.
TissueEng 2003;9:4319.
39 Hankemeier S, Keus M, Zeichen J et al. Modulation of
proliferation and differentiation ofhuman bone marrow stromal cells
by fibroblast growth factor 2: potential implications for
tissue engineering of tendons and ligaments. Tissue Eng
2005;11:419.40 Caplan AI, Bruder SP. Mesenchymal stem cells:
building blocks for molecular medicine in the
21st century. Trends Mol Med 2001;7:25964.41 Harris MT, Butler
DL, Boivin GP et al. Mesenchymal stem cells used for rabbit tendon
repair
can form ectopic bone and express alkaline phosphatase activity
in constructs. J Orthop Res2004;22:9981003.
42 Pryce BA, Watson SS, Murchison ND et al. Recruitment and
maintenance of tendon progeni-tors by TGFbeta signaling are
essential for tendon formation. Development2009;136:135161.
43 Chang J, Thunder R, Most D et al. Studies in flexor tendon
wound healing: neutralizing anti-body to TGF-beta1 increases
postoperative range of motion. Plast Reconstr
Surg2000;105:14855.
44 Abrahamsson SO, Lundborg G, Lohmander LS. Recombinant human
insulin-like growth
factor-I stimulates in vitro matrix synthesis and cell
proliferation in rabbit flexor tendon. JOrthop Res
1991;9:495502.
45 Kurtz CA, Loebig TG, Anderson DD et al. Insulin-like growth
factor I accelerates functionalrecovery from Achilles tendon injury
in a rat model. Am J Sports Med 1999;27:3639.
46 Forslund C, Rueger D, Aspenberg P. A comparative
dose-response study of cartilage-derived
morphogenetic protein (CDMP)-1, -2 and -3 for tendon healing in
rats. J Orthop Res2003;21:61721.
47 Foster TE, Puskas BL, Mandelbaum BR et al. Platelet-rich
plasma: from basic science to clini-cal applications. Am J Sports
Med 2009;37:225972.
48 Aspenberg P, Virchenko O. Platelet concentrate injection
improves Achilles tendon repair inrats. Acta Orthop Scand
2004;75:939.
49 Paoloni J, De Vos RJ, Hamilton B et al. Platelet-rich plasma
treatment for ligament andtendon injuries. Clin J Sport Med
2011;21:3745.
50 Schepull T, Kvist J, Norrman H et al. Autologous platelets
have no effect on the healing ofhuman achilles tendon ruptures: a
randomized single-blind study. Am J Sports Med2011;39:3847.
51 Lou J, Tu Y, Burns M et al. BMP-12 gene transfer augmentation
of lacerated tendon repair. JOrthop Res 2001;19:1199202.
52 Nakamura N, Shino K, Natsuume T et al. Early biological
effect of in vivo gene transfer ofplatelet-derived growth factor
(PDGF)-B into healing patellar ligament. Gene
Ther1998;5:116570.
Strategies for treatment in tendon injury
British Medical Bulletin 2011 Page 15 of 15
by guest on August 7, 2015
http://bmb.oxfordjournals.org/
Dow
nloaded from