Embed Size (px)
Citation preview

Research Article
Bortezomib Relieves Immune Tolerance inNasopharyngeal Carcinoma via STAT1Suppression and Indoleamine 2,3-DioxygenaseDownregulationGuan-Min Jiang1#, Hong-Sheng Wang2#, Jun Du2,Wei-Feng Ma3, Hui Wang4,Yu Qiu5, Qiu-Gui Zhang6,Wei Xu6, Hui-Fang Liu6, and Jian-Ping Liang7
Abstract
Radiotherapy is the primary treatment for nasopharyngealcarcinoma (NPC). Patients with intermediate and advanced stageNPC receiving only radiotherapy have limited survival, so newerimmunotherapeutic approaches are sought. The major impedi-ment to better clinical outcomes is tumor immune tolerance.Indoleamine 2,3-dioxygenase (IDO), an IFNg-inducible enzyme,is a major inducer of immune tolerance during tumor develop-ment; therefore, inhibition of the IDO pathway is an importantmodality for cancer treatment. We show that bortezomib, aproteasomal inhibitor, inhibited the pathways leading to STAT1and IRF-1 activation, both of which are necessary for IDO expres-sion. Bortezomib downregulated IFNg-induced IDO expressionvia inhibition of STAT1 phosphorylation and nuclear trans-location, thereby suppressing STAT1-driven IDO transcription inNPC cells. Bortezomib also promoted IkB-a phosphorylation-
ubiquitination, which released NF-kB from IkB-a. However, thereleased NF-kB could not enter the nucleus to conduct its bio-logical effects and accumulated in the cytoplasm. Negative feed-back inhibited the transcription of NF-kB, which is important foractivating IRF-1 expression. IDO expression is regulated by twoimportant transcription factor binding sites, ISREs, which bindSTAT1 and IRF-1, and GASs, which binds STAT1. Bortezomib up-regulated IRF-1 protein by inhibiting its proteasome-dependentdegradation, but it also inhibited STAT1 phosphorylation, whichdirectly inhibited the activation of GAS and indirectly inhibitedthe activation of ISRE, which needs both STAT1 and IRF-1. Thesediscoveries provide a mechanism for the antitumor action ofbortezomib and have implications for the development of clini-cal cancer immunotherapy for preventing and treating NPC.Cancer Immunol Res; 5(1); 42–51. �2016 AACR.
IntroductionNasopharyngeal carcinoma (NPC) is an Epstein–Barr virus
(EBV)-associated malignancy with high prevalence in South Chi-na and Southeast Asia (1). At present, radiotherapy is still themain treatment for this disease, but the 5- to 10-year survival rate
of patients with intermediate and advanced stages who receiveonly radiotherapy is only 40% (2). Moreover, the disease relapserate is relatively high, which is associated with poor survivalfrom recurrent or metastatic disease (3). Therefore, developmentof novel therapeutic strategies against NPC is clearly needed.
The development of therapeutic strategies that block CTLA-4 orPD-1 have had success treating a subset of melanoma patients, ashave had other immunotherapies (4, 5). Immunotherapeuticstrategies aimed at boosting antitumor immunity are also prom-ising candidates for the treatment of NPC. Many studies usingvaccines targeting EBV and other antigens have focused on revers-ing the impaired immune response to NPC tumors (6, 7). How-ever, the clinical outcomes of these immunotherapeutic strategieshave been less effective than anticipated. Immune tolerance tothese tumors is still a major impediment in cancer immunother-apy, requiring more elucidation of the immune tolerancemechanisms involved (8, 9).
Cytokine IFNg production from tumor-infiltrating lympho-cytes (TIL) in NPC patients is greater than that in healthy controls.Secretion of IFNg , a key antitumor cytokine, by activated Th1 cellsandnatural killer (NK) cells, is a trait of a successful tumor vaccine.However, IFNg has the potent ability to induce indoleamine 2,3-dioxygenase (IDO) expression in various kinds of tumors includ-ing NPC, and IDO was reported as one of the main factors thatcontribute to tumor-induced immunosuppressive mechanisms(10–13). IDO-positive cells were found scattered in the tumortissues from patients with NPC, compared with controls, with
1Department of Clinical Laboratory, Hunan Cancer Hospital and The AffiliatedCancer Hospital of Xiangya School of Medicine, Central South University,Changsha, Hunan, China. 2Department of Microbial and Biochemical Pharmacy,School of Pharmaceutical Sciences, Sun Yat-sen University, Guangzhou, Guang-dong, China. 3Department of Microbiology, School of Public Health and TropicalMedicine, Southern Medical University, Guangzhou, Guangdong, China. 4KeyLaboratory of Translational Radiation Oncology, Hunan Province, Changsha,Hunan, China. 5Department of ICU, Hunan Children's Hospital, Changsha, Hunan,China. 6Department of Clinical Laboratory, The First Affiliated Hospital ofUniversity of South China, Hengyang, Hunan, China. 7Department of ThoracicSurgery 2, Hunan Cancer Hospital and The Affiliated Cancer Hospital of XiangyaSchool of Medicine, Central South University, Changsha, Hunan, China.
#These authors contributed equally to this work.
Corresponding Authors: Guan-Min Jiang, Hunan Cancer Hospital and TheAffiliated Cancer Hospital of Xiangya School of Medicine, Central South Uni-versity, No. 283, TongzipoRoad, Changsha, Hunan410013, China. Phone: 86-731-89762682; Fax: 86-731-89762682; E-mail: [email protected]; Hong-Sheng Wang, [email protected]; and Jian-Ping Liang,[email protected]
doi: 10.1158/2326-6066.CIR-16-0102
�2016 American Association for Cancer Research.
CancerImmunologyResearch
Cancer Immunol Res; 5(1) January 201742
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102

significantly more IDO activity in the plasma of NPC patients,especially among patients with metastatic cancer (2, 14). Thesereports provide evidence that IDO is involved in tumor immuneevasion of NPC, suggesting that it could be a relevant therapeutictarget for NPC.
IDO is responsible for initiating the first, rate-limiting step intryptophan metabolism in the kynurenine (Kyn) pathway. Itcan induce immune tolerance by depleting tryptophan locallyand producing toxic tryptophan catabolites, such as kyn, whichcan induce proliferation arrest, inactivation, and apoptosis of Tlymphocytes or NK cells (15, 16). Therefore, inhibition of theIDO pathway is emerging as an important modality for cancertreatment. Currently, four IDO inhibitors are under clinicaldevelopment (17–20). In the present study, we found thatbortezomib (Velcade; formerly known as PS-341) is a peptideboronate inhibitor of the proteasome that can downregulatethe expression of IDO induced by IFNg in human NPC cells andtherefore may provide potential therapeutic strategies in tumorimmunotherapy.
Bortezomib was approved by the FDA for the treatment ofmultiple myeloma and has been evaluated for the treatmentof solid tumors (21, 22). Bortezomib combined with theHDAC inhibitor SAHA synergistically induced the killingof NPC cells. The major mechanism of cell death is reactiveoxygen species–driven caspase-dependent apoptosis. In vivo,the bortezomib/SAHA combination potently induces apopto-sis and suppresses the growth of NPC xenografts in nude mice,which provides the basis from which to progress to clinicaltesting of this drug combination regimen in patients withNPC (23). Bortezomib can pharmacologically sensitize tu-mor cells to the lytic effects of dendritic cell (DC)–activatedimmune effector cells (24). However, the mechanism remainsto be fully characterized. Here, we demonstrate that bortezo-mib downregulated the expression of the IDO induced byIFNg in NPC cells, primarily by inhibiting the JAK/STAT1signaling pathway. It throws light on the mechanism by whichimmune evasion affects the response to treatment of NPCand may have implications for the development of a clinicalimmunotherapeutic strategy for NPC.
Materials and MethodsChemicals and reagents
IFNg was purchased from Sigma-Aldrich. Bortezomib waspurchased from LC Laboratories. Vectors (pGL3-Enhancer, pRL-TK, and pNF-kB-luc) and dual-luciferase assay kit were pur-chased from Promega. Protein A/G Sepharose, the polyclonalrabbit antibody to human IDO, and mAbs to STAT1, phospho(Y701), are products of Santa Cruz Biotechnology Inc. MAbs tob-actin, NF-kB p65, IRF1, IkB-a, and p-IkB-a (ser32) areproducts of Cell Signaling Technology. SYBR Premix ExTaq IIis a product of TaKaRa BIO Inc. The secondary antibody tomouse IgG, conjugated to FITC and DAPI dye, was purchasedfrom Invitrogen.
Cell linesThe human NPC cell lines CNE2 and CNE1 were gifts from
Sun Yat-sen University (Guangzhou, China) as described pre-viously (25), received on May 2013. The CNE2 line was usedfrom January 2015 to February 2016, and the CNE1 line fromJuly to September 2016. Both cell lines were authenticated by
short tandem repeat analysis and passaged for fewer than 6months before experiments. Vials were thawed and maintainedin culture for only several weeks at a time. The CNE2 and CNE1cell lines were maintained in RPMI 1640 (Invitrogen) supple-mented with 10% heat-inactivated endotoxin-free newborn calfserum (Hyclone), streptomycin (100 mg/mL), and penicillin(100 units/mL) under a humidified 5% CO2 atmosphere at37�C in a CO2 incubator.
Cytotoxicity assayThe cytotoxicity of bortezomib toward the cultured cells was
assessed using MTT [3-(4,5-dimethylthiazol-2yl)-2,5-diphenylte-trazolium bromide] assays (Sigma Chemical Co.). CNE2 andCNE1 cells were seeded onto 96-well microplates (NunC) at adensity of 1� 104 cells per well and incubated for 24 hours. Cellswere then treated with selected concentrations of bortezomib for24 or 48 hours. Cells in culture medium alone served as theuntreated control. The MTT reagent (5 mg/mL in distilled water)was prepared immediately prior to use. After removing the incu-bation medium from the wells, cells were washed with PBS, and10 mL of MTT reagent was added. After incubation for 4 hours at37�C, MTT reagent in 100 mL of dimethylsulfoxide (DMSO) wasadded to each well. Surviving cells were then detected by mea-suring absorbance at 570nmusing aplate reader. The cell viabilitywas expressed as a percentage of the values obtained for thecontrols.
Figure 1.
Cytotoxicity of bortezomib in NPC cells. Experiments were performed by meanof an MTT enzyme assay. CNE2 and CNE1 cells were incubated in thepresence of different concentrations of bortezomib at 37�C for 12 hours (A) or24 hours (B). Each column represents the mean � SD with respect to 100%control. At least three independent assays were performed.
Bortezomib Relieves IDO-Induced Tumor Immune Tolerance
www.aacrjournals.org Cancer Immunol Res; 5(1) January 2017 43
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102

Western blot analysisCells were lysed in cell lysis buffer containing 1% NP-40, 20
mmol/L Tris-HCl (pH 7.6), 0.15 mol/L NaCl, 3 mmol/L EDTA,3 mmol/L EGTA, 1 mmol/L phenylmethylsulfonyl fluoride, 20mg/mL aprotinin, and 5 mg/mL leupeptin. Lysates were clearedby centrifugation and denatured by boiling in Laemmli buffer.
Equal amounts of protein samples were separated on 12%SDS–polyacrylamide gels and electrophoretically transferredto nitrocellulose membranes. Following blocking with 5%non-fat milk at room temperature for 2 hours, membraneswere incubated with the primary antibody at 1:1,000 dilutionovernight at 4�C and then incubated with a horseradish
Figure 2.
Bortezomib downregulated the IFNg-induced expression of IDO in a dose-dependent manner, but bortezomib did not inhibited the activity of IDO. CNE2 and CNE1cells were treated with reagents as indicated, and IDO expression was detected by Western blotting; b-actin served as the loading control. A, CNE2 and CNE1cells were treated with different concentrations of IFNg for 24 hours. B, CNE2 and CNE1 cells were treated with IFNg (100 U/mL) for the indicated times. C, CNE2and CNE1 cells were pretreated with various concentrations of bortezomib for 2 hours and then treated with IFNg (100 U/mL) for 24 hours. Similar resultswere obtained in three independent experiments. D, CNE2 cells were pretreated with or without IFNg (100 U/mL) for 12 hours, and then we changed theculture media before cells were treated with or without 2 mmol/L bortezomib for 3 hours. The Kyn contents in cell culture media were measured by HPLC. The arrowindicates the HPLC peaks of Kyn in the samples. �� , P < 0.001 and #, P > 0.05.
Jiang et al.
Cancer Immunol Res; 5(1) January 2017 Cancer Immunology Research44
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102

peroxidase–conjugated secondary antibody at 1:5,000 dilutionfor 1 hour at room temperature. Specific immune complexeswere detected using western blotting plus chemiluminescencereagent (Life Science, Inc.).
High performance liquid chromatography analysis ofkynurenine
Cells were plated into 12-well plates. When the cell densityreached 80%, cells were stimulated with or without IFNg for 12hours, thenwe changed the culturemedia before cells were treatedwith or without bortezomib for 3 hours. Cell culture media werecollected, and 1/5 volume of trichloroacetic acid was added toprecipitate the protein. The collected supernatant was then ana-lyzed by high performance liquid chromatography (HPLC;Waters 1525-2487-717). Briefly, 20mLof the samplewere injectedinto a Phenomenex Gemini C18 chromatographic column (250mm� 4.60mm, 5mm)and elutedwithKH2PO4 buffer (1mmol/LKH2PO4, pH 4.0) containing 20% methanol at a flow rate of1.0 mL/min. The Kyn content was detected using an ultravioletdetector at 360 nm for excitation and 366 nm for emission. Theretention time was previously determined with standard solutions(Sigma-Aldrich).
ImmunoprecipitationTo assess the combination of IkB-a and NF-kB, cells were
treated with or without bortezomib and IFNg for 24 hours,then washed twice with ice-cold PBS, and harvested at 4�Cin immunoprecipitation lysis buffer [50 mmol/L HEPES,pH 7.5, 150 mmol/L NaCl, 2 mmol/L EDTA, 0.5% NP-40,10% glycerol, 1 mmol/L NaF, 1 mmol/L Na3VO4, 1 mmol/Ldithiothreitol, 1 mmol/L 4-(2-aminoethyl) benzenesulfonylfluoride, leupeptin (1 mg/mL), aprotinin (1 mg/mL), andpepstatin (1 mg/mL)]. Equal amounts of protein were immu-noprecipitated using NF-kB p65 mAb, and the immune com-plexes were bound to protein A/G Sepharose. The beads werewashed with lysis buffer and subjected to Western blottingwith IkB-a mAb.
Confocal microscopy for STAT1 and NF-kBCells were grown on chamber slides. After 12 hours of culti-
vation, cells were stimulated with or without bortezomib andIFNg . Cells were fixed in 4% paraformaldehyde for 30 minutes,blocked with goat serum for 30 minutes at 37�C, and thenincubated with STAT1 and NF-kB p65 mAbs at 1:100 for 1 hourat 37�C. Slides were washed with PBS and incubated with asecondary antibody to mouse IgG, conjugated to FITC at1:1,000 for 45 minutes at 37�C. After washed by PBS, cells wereincubated with DAPI (10 mg/mL) for 10 minutes to visualize cellnuclei. Samples were examined with confocal laser scanningmicroscopy (Zeiss) to analyze nuclear translocation of STAT1and NF-kB.
Transient transfections and reporter genes assayTo examine the effect of bortezomib on STAT1-dependent
transcriptional activity, we used 7 � GAS sequence GAS7 (con-sensus TTC/ANNNG/TAA) and 4 � ISRE (IFN-stimulatedresponse elements) sequence ISRE4 (consensus AGTTTCNN-TTCNC/T; ref. 26) cloned upstream of the luciferase reporter geneof pGL3-Enhancer. The coding strand ofGAS7 plusMluI and XhoIsequences is 50-CGACGCGTTTCCAGGAATTCCAGGAATTACA-
GTAATTACAGTAATTCCAGTAATTCCTGTAATTCCTGTAACTCG-AGCGG-30, and the coding strand of ISRE4 plus MluI and XhoIsequences is 50-CGACGCGTAGTTTCGATTCGTAGTTTCGATTC-GTAGTTTCAGTTCCTAGTTTCAGTTCCTCTCGAGCGG-30. Thecoding and template strands of GAS7 and ISRE4 were synthe-sized by Shanghai Sangon Biological Engineering Technologyand Service Co., Ltd. and annealed to double strands. Thedouble strands of GAS7 and ISRE4 were digested with MluI andXhoI and inserted into pGL3-Enhancer. For measuring theactivation of GAS, ISRE, and NF-kB, cells were transfected with0.2 mg DNA/cm2 per plasmid and lipofectamine 2000 reagent(Gibco BRL) according to the manufacturer's instructions.
Figure 3.
Bortezomib inhibited STAT1 phosphorylation and nuclear translocation. A,CNE2 cells were treated with or without 2 mmol/L bortezomib for 2 hours andthen treated with IFNg (100 U/mL) for 5 or 15 minutes. The phosphorylation ofSTAT1 and total STAT1 was detected by Western blotting with a pSTAT1-Y701mAb and a STAT1 mAb, respectively; b-actin served as the loading control.Similar results were obtained in three independent experiments. Values werecompared with the control, and statistically significant values with P < 0.05 aremarked with (�). B, CNE2 cells were grown on chamber slides and werepretreatedwith or without 2mmol/L bortezomib for 2 hours, followed by treatedwith or without IFNg (100 U/mL) for 30 minutes. Immunofluorescence andconfocal microscopy were performed as described in theMaterials andMethodssection. Scale bar, 20 mm.
Bortezomib Relieves IDO-Induced Tumor Immune Tolerance
www.aacrjournals.org Cancer Immunol Res; 5(1) January 2017 45
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102

Transfection efficiency was normalized by cotransfection withpRL-TK. Transcriptional activity was determined by a lumin-ometer, using a dual-luciferase assay kit. Results are displayedas the ratio between the activity of the reporter plasmid andpRL-TK.
Quantitative real-time PCRTo achieve better quantification of NF-kB p65 mRNA expres-
sion, NF-kB p65 mRNA was measured by quantitative real-timePCR. CNE2 (2 � 105) cells were pretreated with 2 mmol/Lbortezomib for 2 hours, followed by treatment with 100 U/mLIFNg for 24 hours. Total mRNA was extracted with TRIZOLreagent. The first strand of cDNA was generated from 2 mg totalRNA using oligo-dT primer and Superscript II Reverse Transcrip-tase (GIBCO BRL). Quantitative real-time PCR was run on aniCycler (Bio-rad) using validated primers for b-actin, NF-kB p65,and SYBR Premix Ex Taq II (Takara) for detection. The cyclenumber when the fluorescence first reached a preset threshold(Ct) allowed the quantification of the specific template concen-tration. Transcripts of the housekeeping gene b-actin in the sameincubations were used for internal normalization. The primerpairs used in the subsequent quantitative real-time PCR reactionswere as follows: NF-kB p65, forward 50-CTGCAGTTTGATGAT-GAAGA-30and reverse 50-TAGGCGAGTTATAGCCTCAG-30;b-actin, forward 50-TGGCACCCAGCACAATGAA-30 and reverse50 -CTAAGTCATAGTCCGCCTAGAAGCA-30.
Statistical analysesAll values were reported as mean � SEM of three indepen-
dent experiments unless otherwise specified. Data were ana-lyzed by two-tailed unpaired Student t test between two groupsand by one-way ANOVA followed by a Bonferroni correctionfor multiple comparison involved. These analyses were per-formed using GraphPad Prism Software Version 5.0 (Graph-Pad Software Inc.). P < 0.05 was considered statisticallysignificant.
ResultsCytotoxicity of bortezomib in NPC cells
AnMTT enzyme assaywas used to determine the cytotoxicity ofbortezomib in NPC CNE2 and CNE1 cells. Bortezomib couldsuppress the proliferation of cells in a concentration-dependentmanner. At 2 mmol/L, the survival rate of cells was about 80%,whereas when cells were exposed to 4 mmol/L bortezomib, themajority of CNE2 and CNE1 cells died (Fig. 1). Therefore, insubsequent experiments, we applied bortezomib at a concentra-tion of 2 mmol/L, which did not affect the survival rate of the NPCcells significantly.
Bortezomib downregulated IFNg-induced IDO, but did notinhibit its activity
First, the effect of IFNg on IDO expression was investigated.IFNg significantly enhanced IDO expression in dose- and
Figure 4.
Bortezomibpromoted IKB-aphosphorylation and inhibited combination of IKB-awithNF-kB.A,CNE2 cellswerepretreatedwith orwithout 2mmol/L bortezomib for2 hours and then treated with or without IFNg for 24 hours. IkB-a protein in total cell lysate was detected byWestern blotting; b-actin served as the loading control.Similar results were obtained in three independent experiments. Valueswere compared with the control, and statistically significant values with P < 0.05 aremarkedwith (�). B, CNE2 cells were treated with or without 2 mmol/L bortezomib for 2 hours and then treated with IFNg (100 U/mL) for 5, 15, and 30 minutes. Thephosphorylation of IkB-a and total IkB-awas detected byWestern blottingwith p-IKB-a(ser32) and kB-amAbs, respectively; b-actin served as the loading control.Similar results were obtained in three independent experiments. C, CNE2 cells were pretreated with or without 2 mmol/L bortezomib for 2 hours and then treatedwith or without IFNg for 12 hours; total proteins in the cell lysate were subjected to immunoprecipitation with an NF-kB p65 mAb. The IkB-a combined withNF-kB p65 in immune complexwere detected byWestern blottingwith an IkB-a antibody (top). Themembranewas stripped of antibodies and immunoblottedwithan NF-kB p65 antibody (bottom).
Jiang et al.
Cancer Immunol Res; 5(1) January 2017 Cancer Immunology Research46
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102

time-dependent manners, from 4 hours at 20 U/mL through 8hours at 100 U/mL (Fig. 2A and B). We then explored theinfluence of bortezomib on IDO expression (Fig. 2C). Bortezo-mib reduced IDO induction (from 0.25 mmol/L) and almostcompletely inhibited the expression of IDO at a concentrationof 2 mmol/L. We also examined the effect of bortezomib onIDO activity (Fig. 2D) and found that while IFNg increased theconcentration of Kyn when compared with the control group,the concentration of Kyn did not change when bortezomib andIFNg were added together, suggesting that bortezomib did notinhibit the activity of IDO.
Bortezomib inhibited STAT1 phosphorylation and nucleartranslocation
IFNg induces IDO expression through the activation ofSTAT1. STAT1 phosphorylation at residue Y701 is required forits translocation to the nucleus, where it acts as an activetranscription factor (27). Therefore, we asked whether borte-zomib interfered with STAT1 Y701 phosphorylation and inhib-ited its nuclear translocation. Stimulation of cells with IFNg for5 minutes alone resulted in a rapid increase in tyrosine phos-phorylation of STAT1, and this increase was remarkably inhib-ited by bortezomib treatment (Fig. 3A). We further studiedwhether bortezomib inhibited STAT1 nuclear translocation.Results in untreated cells showed that STAT1 was localizedexclusively in the cytoplasm, and bortezomib did not alterbasal subcellular localization of STAT1. In contrast, treatmentof cells with IFNg for 30 minutes induced a significant nucleartranslocation of STAT1, but pretreatment of cells with borte-zomib for 2 hours markedly reduced IFNg-induced nucleartranslocation of STAT1 (Fig. 3B). Taken together, these resultssuggested that bortezomib blocked IFNg-induced expression ofIDO and that this block might be a result of inhibition ofphosphorylation and nuclear translocation of STAT1.
IkB-a phosphorylation and release of NF-kB by bortezomibIRF-1 is an important factor for IFNg-induced IDO expres-
sion, and the IRF-1 promoter region contains both GAS ele-ments and NF-kB binding motifs. Normally, NF-kB is com-plexed with IkB-a. When IkB-a is phosphorylated, it is degrad-ed by proteasomes, releasing the NF-kB subunit to conduct itsbiological effects (28). Stimulation of cells with bortezomibresulted in a rapid increase in phosphorylation of IkB-a(Fig. 4A). Further studies demonstrated that phosphorylatedIkB-a was partially degraded (Fig. 4B, black arrow). To deter-mine whether IkB-a released NF-kB after it degradation, NF-kBp65 was immunoprecipitated, and an IkB-a mAb was used todetect IkB-a by Western blotting. After treatment with borte-zomib, the amount of IkB-a complexed with NF-kB decreased,which revealed that bortezomib promoted the release of NF-kBfrom IkB-a (Fig. 4C).
NF-kB translocation unaffected, but IRF-1 upregulated bybortezomib
Because IFNg can induce the expression of NF-kB and promoteits nuclear translocation, we determined whether bortezomibinterfered with NF-kB nuclear translocation by confocal micros-copy with a NF-kB p65 mAb. NF-kB was localized exclusivelyin the cytoplasm of untreated cells, and bortezomib did notalter basal subcellular localization of NF-kB p65. In contrast,treatment of cells with IFNg for 30 minutes induced a significant
nuclear translocation of NF-kB p65. Pretreatment of cells withbortezomib for 2 hours did not increase IFNg-induced nucleartranslocation of NF-kB, which was unexpected, given that borte-zomib increased the amount of free NK-kB available to betranslocated (Fig. 4). Together, this suggested that the releasedNF-kB from IkB-a could not enter the nucleus to conduct itsbiological effects (Fig. 5A).
We then determined whether bortezomib affected expressionof the IRF-1 protein, because IRF-1 is important for IFNg-inducedexpression of IDO and is directly upregulated by NF-kB. Resultsshowed that IFNg significantly upregulated IRF-1 expression.However, whereas bortezomib alone could not induce the expres-sion of IRF-1, the amount of the IRF-1 protein in the group treatedwith both bortezomib and IFNg was significantly increased com-pared with the group treated with IFNg alone (Fig. 5B). This maybe the result of bortezomib inhibiting the degradation of IRF-1protein.
Figure 5.
Effect of bortezomib on NF-kB nuclear translocation and expression of IRF-1. A,CNE2 cells were grown on chamber slides and pretreated with or without 2mmol/L bortezomib for 2 hours. Cellswere then treatedwith IFNg (100U/mL) for30 minutes. Immunofluorescence and confocal microscopy were performed asdescribed in Materials and Methods. Scale bar, 20 mm. B, CNE2 cells werepretreated with or without 2 mmol/L bortezomib for 2 hours and then treatedwith or without IFNg for 8 hours. IRF-1 protein in total cell lysatewas detected byWestern blotting; b-actin served as the loading control. Similar results wereobtained in three independent experiments. Values were compared with thecontrol and statistically significant values with P < 0.05. Significant analysis ismarked with � , P < 0.05 and #, P > 0.05.
Bortezomib Relieves IDO-Induced Tumor Immune Tolerance
www.aacrjournals.org Cancer Immunol Res; 5(1) January 2017 47
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102

Bortezomib blocked IFNg-induced activation of GAS,ISRE, and NF-kB
We demonstrated that tyrosine phosphorylation of STAT1was inhibited by bortezomib. Therefore, we examined whetherthe inhibitory effect of bortezomib can block transcriptionalactivation of STAT1. The reporter gene plasmids pGL3-Enhancer-GAS7-luc, pGL3-Enhancer-ISRE4-luc, and pNF-kB-luc were trans-fected into CNE2 cells. Transfection efficiency was normalizedby cotransfection with pRL-TK. It demonstrated that dual-Glo-Luciferase analysis revealed that IFNg significantly enhanced theactivity of pGL3-Enhancer-GAS7-luc, pGL3-Enhancer-ISRE4-luc,and pNF-kB-luc, whereas bortezomibmarkedly inhibited the activ-ity of pGL3-Enhancer-GAS7-luc, pGL3-Enhancer-ISRE4-luc, andpNF-kB-luc (Fig. 6A–C). These data suggested that bortezomibdownregulated IFNg-induced expression of IDO by blockingSTAT1 phosphorylation, which drives activation of the GAS andISRE. The transcriptional activation of NF-kB may be inhibitedby the negative feedback induced by the increased NF-kB proteinsreleased from IkB-a, as shown by quantitative real-time PCR(Fig. 6D), demonstrating that bortezomib can downregulate theproduction of NF-kB mRNA significantly.
DiscussionIt was reported that the promoter of IDO gene contains a series
of putative transcription factor binding sites, including one GAS
sequence, two ISRE regions, and two AP-1 binding sites (29, 30).As an important transcriptional factor for the IFNg-inducedexpression of IDO, STAT1 is phosphorylated by JAK first, thenSTAT1 dimerizes and translocates to the nucleus, where it bindsGAS to activate IDO and IRF-1 gene expression directly. But STAT1also contributes indirectly by inducing production of IRF-1,whose promoter region contains both GAS elements and NF-kBbinding motifs, and both elements are important for IRF-1expression. The IRF-1 protein then binds to ISRE-1 and ISRE-2elements in the IDO regulatory region to activate IDO geneexpression (31, 32).
In the present study, we demonstrated that bortezomib didnot inhibit the activity of IDO in CNE2 cells, but it down-regulated the expression of IDO induced by IFNg in a dose-dependent manner. Dual-Glo-Luciferase analysis revealed thatcells treated with IFNg significantly induced transcriptionalactivity of the reporter plasmids pGL3-Enhancer-GAS7, pGL3-Enhancer-ISRE4, and pNF-kB-luc, suggesting the importance ofGAS, ISRE, and NF-kB in IFNg-induced expression of IDO.Furthermore, our results showed that bortezomib significantlyinhibited IFNg-induced transcriptional activation of the report-er plasmids pGL3-Enhancer-GAS7, pGL3-Enhancer-ISRE4, andpNF-kB-luc. This phenomenon could be explained by the factthat bortezomib inhibited STAT1 phosphorylation and nucleartranslocation, which was important and enough for STAT1binding GAS to activate IDO expression. Unlike GAS, however,
Figure 6.
Effect of bortezomib on IFNg-induced activation ofGAS, ISRE, andNF-kB. CNE2 cellswere transfectedwith pGL3-Enhancer-GAS7-luc (A), pGL3-Enhancer-ISRE4-luc(B), or pNF-kB-luc (C) reporter plasmids and treated with 2 mmol/L bortezomib for 2 hours, followed by treatment with IFNg (100 U/mL) for 24 hours.Luminescence was measured with a luminometer. pRL-TK plasmids served to correct transfection efficiency. Results are expressed as the ratio between the activityof the reporter plasmid and pRL-TK. � , P < 0.05 and �� , P < 0.001. D, CNE2 cells were pretreated with 2 mmol/L bortezomib for 2 hours, followed bytreatment with 100 U/mL IFNg for 24 hours; NF-kB p65 mRNA was detected by quantitative real-time PCR. �, P < 0.05.
Jiang et al.
Cancer Immunol Res; 5(1) January 2017 Cancer Immunology Research48
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102

activation of ISRE needed both phosphorylated STAT1 and IRF-1. Although bortezomib could upregulate the expression ofIRF-1 by inhibiting its degradation, phosphorylated STAT1 wasmore important than IRF-1. When the phosphorylation ofSTAT1 was inhibited, the ISRE was inactivated. These resultssuggested that bortezomib inhibited the IDO expression main-ly by interfering with phosphorylation and nuclear transloca-tion of STAT1 to inhibit its binding to GAS and ISRE elementsin the IDO regulatory region. Still unclear is the mechanism bywhich bortezomib inhibited IFNg-induced transcriptional acti-vation of the reporter plasmid pNF-kB-luc.
Bortezomib is the first proteasomal inhibitor to be usedtherapeutically for treating relapse cases of multiple myelomaand mantle cell lymphoma. Preclinically, it has activity in manyhematologic and solid malignancies as a single agent andenhances the activity of many chemotherapy agents in modelsof multiple myeloma, acute leukemia, and lung and pancreaticcancers (33–35). One of the major mechanisms associated withthe anticancer activity of bortezomib is through upregulation ofNOXA, which is a proapoptotic protein. NOXA may interactwith the antiapoptotic proteins of Bcl-2 subfamily Bcl-XL andBcl-2, which results in apoptotic cell death of malignant cells.Another important mechanism of bortezomib is through sup-pression of the NF-kB signaling pathway, resulting in thedownregulation of its antiapoptotic target genes (36). Theprototypical mechanism of NF-kB activation depends on thesignal-induced phosphorylation and ubiquitination of aninhibitory protein called IkB-a, which is subsequently degrad-ed by the proteasome (37).
In this article, we found that bortezomib promoted IkB-aphosphorylation, then the phosphorylated IkB-a was partiallydegraded after ubiquitination. Further immunoprecipitationdemonstrated that bortezomib promoted IkB-a phosphoryla-tion, leading to partial ubiquitination and degradation, and theamount of IkB-a complexed with NF-kB decreased. This revealedthat bortezomib enhanced the IkB-a release of NF-kB, which wasthen free to conduct its biological effects. However, imaging
results showed that the group treated with both bortezomib andIFNg did not have increased NF-kB nuclear translocation com-pared with the group treated with IFNg alone, which means thatthe NF-kB released from IkB-a could not enter the nucleus toconduct its biological effects. The accumulated NF-kB in thecytoplasm was a source of negative feedback that inhibited thetranscriptional expression of NF-kB, explaining how bortezomibinhibited IFNg-induced transcriptional activation of the reporterplasmid pNF-kB-luc.
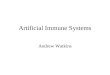
In summary, we demonstrated in NPC cells that bortezomibdownregulated IFNg-induced IDO expression by inhibitingSTAT1 phosphorylation and nuclear translocation, which sup-pressed STAT1-driven transcription of IDO. Although bortezomibcanpromote IkB-aphosphorylation-ubiquitination to release theNF-kB from IkB-a, the released NF-kB cannot enter into thenucleus to conduct its biological effects. Accumulated NF-kB inthe cytoplasmcould inducenegative feedback inhibitionofNF-kBtranscription, which then inhibited IRF-1 transcription, becauseits promoter region contains both GAS elements and NF-kBbinding motifs. However, IRF-1 is a protein degraded by theproteasome, and as a proteasome inhibitor, bortezomib caninhibit the degradation of IRF-1 and indirectly increase theamount of IRF-1 protein. Nevertheless, because phosphorylationof STAT1 is important for induction of IDO through both GASand ISRE sequences, although bortezomib can increase IRF-1protein concentrations, the inhibition of STAT1 phosphorylationby bortezomib directly inhibited the activation of GAS andindirectly inhibited the activation of ISRE, which binds bothSTAT1 and IRF-1 (Fig. 7). Although the dose of bortezomib(2 mmol/L) in this in vitro experiment is not suitable for clinicalapplication, due to toxicities such as neuropathy, structurallymodified versions that have reduced toxicity may be worthpursuing. In general, this mechanism of antitumor action ofbortezomib may have implications for the development ofclinical cancer immunotherapy, especially that which combinesbortezomib with NPC-associated tumor vaccines, as a promisingmethod for preventing and treating NPC.
Figure 7.
A proposed model to illustrate the mechanism of bortezomib downregulation of IDO. !, Direct stimulatory modification; a, direct inhibitory modification.
Bortezomib Relieves IDO-Induced Tumor Immune Tolerance
www.aacrjournals.org Cancer Immunol Res; 5(1) January 2017 49
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102

Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: G.-M. JiangDevelopment of methodology: G.-M. Jiang, J. Du, Y. Qiu, H.-S. WangAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): G.-M. Jiang, Q.-G. Zhang, W. Xu, H.-F. LiuAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): G.-M. Jiang, W.-F. Ma, H. WangWriting, review, and/or revision of the manuscript: G.-M. JiangAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): G.-M. JiangStudy supervision: G.-M. Jiang, J. Du, J.-P. Liang
Grant SupportThis work was funded by the National Natural Science Foundation of
China (Nos. 81502104 and 81472470), Hunan Natural Science Founda-tion (Nos. 2016JJ4058 and 13JJ4078), the Guangdong Natural ScienceFunds for Distinguished Young Scholar (No. 2014A030306025), and KeyLaboratory of Translational Radiation Oncology of Hunan Province(2015TP1009).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received May 10, 2016; revised October 28, 2016; accepted November 16,2016; published OnlineFirst December 6, 2016.
References1. Spano JP, Busson P, Atlan D, Bourhis J, Pignon JP, Esteban C, et al.
Nasopharyngeal carcinomas: An update. Eur J Cancer 2003;39:2121–35.
2. Liu P, Xie BL, Cai SH, He YW, Zhang G, Yi YM, et al. Expression ofindoleamine 2,3-dioxygenase in nasopharyngeal carcinoma impairs thecytolytic function of peripheral blood lymphocytes. BMC Cancer 2009;9:416.
3. Chan AT. Nasopharyngeal carcinoma. Ann Oncol 2010;21(Suppl 7):vii308–312.
4. Hodi FS,O'Day SJ,McDermott DF,Weber RW, Sosman JA,Haanen JB, et al.Improved survivalwith ipilimumab in patients withmetastaticmelanoma.N Engl J Med 2010;363:711–23.
5. Tsai KK, Zarzoso I, Daud AI. PD-1 and PD-L1 antibodies for melanoma.Hum Vaccin Immunother 2014;10:3111–6.
6. Louis CU, Straathof K, Bollard CM, Gerken C, Huls MH, Gresik MV, et al.Enhancing the in vivo expansion of adoptively transferred EBV-specificCTLwith lymphodepleting CD45 monoclonal antibodies in NPC patients.Blood 2009;113:2442–50.
7. LuoC,Wang JJ, Li YH,Hu JY, Li GC. Immunogenicity and efficacy of aDNAvaccine encoding a human anti-idiotype single chain antibody againstnasopharyngeal carcinoma. Vaccine 2010;28:2769–74.
8. Makkouk A, Weiner GJ. Cancer immunotherapy and breakingimmune tolerance: New approaches to an old challenge. Cancer Res2015;75:5–10.
9. JiangGM, XieWY,WangHS,Du J,Wu BP, XuW, et al. Curcumin combinedwith FAPalphac vaccine elicits effective antitumor response by targetingindolamine-2,3-dioxygenase and inhibiting EMT induced by TNF-alpha inmelanoma. Oncotarget 2015;6:25932–42.
10. Williams CA, Harry RA, McLeod JD. Apoptotic cells induce dendritic cell-mediated suppression via interferon-gamma-induced IDO. Immunology2008;124:89–101.
11. UyttenhoveC, Pilotte L, Theate I, Stroobant V, ColauD, Parmentier N, et al.Evidence for a tumoral immune resistance mechanism based on trypto-phan degradation by indoleamine 2,3-dioxygenase. Nat Med 2003;9:1269–74.
12. Jiang GM, He YW, Fang R, Zhang G, Zeng J, Yi YM, et al. Sodium butyratedown-regulation of indoleamine 2, 3-dioxygenase at the transcriptionaland post-transcriptional levels. Int J Biochem Cell Biol 2010;42:1840–6.
13. Munn DH, Mellor AL. Indoleamine 2,3-dioxygenase and tumor-inducedtolerance. J Clin Invest 2007;117:1147–54.
14. Ben-Haj-Ayed A,Moussa A, Ghedira R, Gabbouj S,Miled S, BouzidN, et al.Prognostic value of indoleamine 2,3-dioxygenase activity and expressionin nasopharyngeal carcinoma. Immunol Lett 2016;169:23–32.
15. Grohmann U, Fallarino F, Puccetti P. Tolerance, DCs and tryptophan:Much ado about IDO. Trends Immunol 2003;24:242–8.
16. He YW, Wang HS, Zeng J, Fang X, Chen HY, Du J, et al. Sodium butyrateinhibits interferon-gamma induced indoleamine 2,3-dioxygenaseexpression via STAT1 in nasopharyngeal carcinoma cells. Life Sci 2013;93:509–15.
17. Liu X, Shin N, Koblish HK, Yang G, Wang Q, Wang K, et al. Selectiveinhibition of IDO1 effectively regulatesmediators of antitumor immunity.Blood 2010;115:3520–30.
18. Koblish HK, Hansbury MJ, Bowman KJ, Yang G, Neilan CL,Haley PJ, et al. Hydroxyamidine inhibitors of indoleamine-2,3-dioxygenase potently suppress systemic tryptophan catabolismand the growth of IDO-expressing tumors. Mol Cancer Ther 2010;9:489–98.
19. Iversen TZ, Engell-Noerregaard L, Ellebaek E, Andersen R, Larsen SK,Bjoern J, et al. Long-lasting disease stabilization in the absence oftoxicity in metastatic lung cancer patients vaccinated with an epitopederived from indoleamine 2,3 dioxygenase. Clin Cancer Res 2014;20:221–32.
20. Vacchelli E, Aranda F, Eggermont A, Sautes-Fridman C, Tartour E, KennedyEP, et al. Trial watch: IDO inhibitors in cancer therapy. Oncoimmunology2014;3:e957994.
21. Richardson PG, Barlogie B, Berenson J, Singhal S, Jagannath S, Irwin D,et al. A phase 2 study of bortezomib in relapsed, refractory myeloma. NEngl J Med 2003;348:2609–17.
22. Cusack JC. Rationale for the treatment of solid tumorswith the proteasomeinhibitor bortezomib. Cancer Treat Rev 2003;29Suppl 1:21–31.
23. Hui KF, Lam BH, Ho DN, Tsao SW, Chiang AK. Bortezomib and SAHAsynergistically induce ROS-driven caspase-dependent apoptosis of naso-pharyngeal carcinoma and block replication of Epstein-Barr virus. MolCancer Ther 2013;12:747–58.
24. Schumacher LY, Vo DD, Garban HJ, Comin-Anduix B, Owens SK, DissetteVB, et al. Immunosensitization of tumor cells to dendritic cell-activatedimmune responses with the proteasome inhibitor bortezomib (PS-341,Velcade). J Immunol 2006;176:4757–65.
25. Yan M, Zhang Y, He B, Xiang J, Wang ZF, Zheng FM, et al. IKKalpharestoration via EZH2 suppression induces nasopharyngeal carcinomadifferentiation. Nat Commun 2014;5:3661.
26. Platanias LC. Mechanisms of type-I- and type-II-interferon-mediated sig-nalling. Nat Rev Immunol 2005;5:375–86.
27. Darnell JE Jr, Kerr IM, Stark GR. Jak-STAT pathways and transcriptionalactivation in response to IFNs and other extracellular signaling proteins.Science 1994;264:1415–21.
28. Chon SY, Hassanain HH, Gupta SL. Cooperative role of interferon regu-latory factor 1 and p91 (STAT1) response elements in interferon-gamma-inducible expression of human indoleamine 2,3-dioxygenase gene. J BiolChem 1996;271:17247–52.
29. Dai W, Gupta SL. Regulation of indoleamine 2,3-dioxygenase gene expres-sion in human fibroblasts by interferon-gamma. Upstream control regiondiscriminates between interferon-gamma and interferon-alpha. J BiolChem 1990;265:19871–7.
30. Kadoya A, Tone S, Maeda H, Minatogawa Y, Kido R. Gene structure ofhuman indoleamine 2,3-dioxygenase. Biochem Biophys Res Commun1992;189:530–6.
31. Robinson CM, Hale PT, Carlin JM. The role of IFNgamma and TNF-alpha-responsive regulatory elements in the synergistic induction of indoleaminedioxygenase. J Interferon Cytokine Res 2005;25:20–30.
32. Chon SY, Hassanain HH, Pine R, Gupta SL. Involvement of tworegulatory elements in interferon-gamma-regulated expression ofhuman indoleamine 2,3-dioxygenase gene. J Interferon Cytokine Res1995;15:517–26.
Cancer Immunol Res; 5(1) January 2017 Cancer Immunology Research50
Jiang et al.
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102

33. Boccadoro M, Morgan G, Cavenagh J. Preclinical evaluation of theproteasome inhibitor bortezomib in cancer therapy. Cancer Cell Int2005;5:18.
34. Adams J. Preclinical and clinical evaluation of proteasome inhibitor PS-341 for the treatment of cancer. Curr Opin Chem Biol 2002;6:493–500.
35. Lonial S, Anderson KC. Association of response endpoints with survivaloutcomes in multiple myeloma. Leukemia 2014;28:258–68.
36. Chen D, Frezza M, Schmitt S, Kanwar J, Dou QP. Bortezomib as the firstproteasome inhibitor anticancer drug: current status and future perspec-tives. Curr Cancer Drug Targets 2011;11:239–53.
37. Sunwoo JB, Chen Z, Dong G, Yeh N, Crowl Bancroft C, Sausville E, et al.Novel proteasome inhibitor PS-341 inhibits activation of nuclear factor-kappa B, cell survival, tumor growth, and angiogenesis in squamous cellcarcinoma. Clin Cancer Res 2001;7:1419–28.
www.aacrjournals.org Cancer Immunol Res; 5(1) January 2017 51
Bortezomib Relieves IDO-Induced Tumor Immune Tolerance
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102

2017;5:42-51. Published OnlineFirst December 6, 2016.Cancer Immunol Res Guan-Min Jiang, Hong-Sheng Wang, Jun Du, et al. 2,3-Dioxygenase DownregulationCarcinoma via STAT1 Suppression and Indoleamine Bortezomib Relieves Immune Tolerance in Nasopharyngeal
Updated version
10.1158/2326-6066.CIR-16-0102doi:
Access the most recent version of this article at:
Cited articles
http://cancerimmunolres.aacrjournals.org/content/5/1/42.full#ref-list-1
This article cites 37 articles, 11 of which you can access for free at:
Citing articles
http://cancerimmunolres.aacrjournals.org/content/5/1/42.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerimmunolres.aacrjournals.org/content/5/1/42To request permission to re-use all or part of this article, use this link
on September 27, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 6, 2016; DOI: 10.1158/2326-6066.CIR-16-0102