Embed Size (px)
Citation preview

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Bone-Targeting Agents in Prostate Cancer Care - One Thing That Is
Underrated in Taiwan
黃昭淵醫師臺大醫院 泌尿科
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Drugs to be talked about Bisphosphonate ( 雙磷酸鹽化合物 )
◦ Alendronate (Fosamax, 福善美 )◦ Clodronate (Bonfos, 骨復舒 )◦ Pamidronte (Aredia, 雷狄亞 )◦ Zoledronate (Zometa, 卓骨祂 )
RANK-ligand Inhibitor◦ Denosumab (XGEVA, 癌骨瓦 )
Bone-seeking Radioisotopes◦ Strontium-89 & Samarium-153: β-emitting particle◦ Radium-223: α-emitting particle

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Drugs to be talked about Bisphosphonate ( 雙磷酸鹽化合物 )
◦ Alendronate (Fosamax, 福善美 )◦ Clodronate (Bonfos, 骨復舒 )◦ Pamidronte (Aredia, 雷狄亞 )◦ Zoledronate (Zometa, 卓骨祂 )
RANK-ligand Inhibitor◦ Denosumab (XGEVA, 癌骨瓦 )
Bone-seeking Radioisotopes◦ Strontium-89 & Samarium-153: β-emitting particle◦ Radium-223: α-emitting particle

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Outline
Mode of action of bone-targeting agentsEfficacy and safety of bone-targeting agents
◦ Fracture Prevention in Early-Stage Prostate Cancer◦ Delaying Bone Metastases in Prostate Cancer◦ Treatment of Bone Metastases Secondary to prostate
cancer◦ Safety profile
Reimbursement criteria for bone-targeting agentsSummary

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Outline
Mode of action of bone-targeting agentsEfficacy and safety of bone-targeting agents
◦ Fracture Prevention in Early-Stage Prostate Cancer◦ Delaying Bone Metastases in Prostate Cancer◦ Treatment of Bone Metastases Secondary to prostate
cancer◦ Safety profile
Reimbursement criteria for bone-targeting agentsSummary

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
RANK Ligand Is An Essential Mediator of Osteoclast Formation, Function and Survival
Boyle WJ, et al. Nature 2003;423:337–42; Roodman GD, N Engl J Med 2004;350:1655–64.

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
A Vicious Cycle of Bone Destruction May Develop in the Presence of Tumour Cells
PDGF, platelet-derived growth factor; TGF, transforming growth factor; IGF, insulin-like growth factor; FGF, fibroblast growth factor; TNF, tumour necrosis factor.
Boyle WJ, et al. Nature 2003;423:337–42; Roodman GD. N Engl J Med 2004;350:1655–64.
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
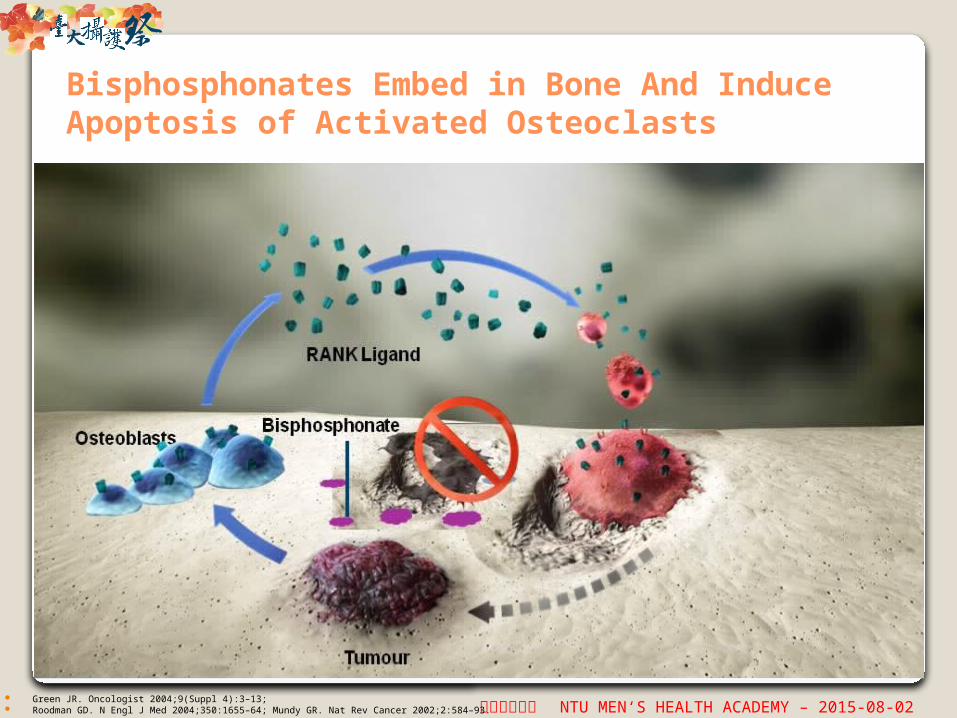
Bisphosphonates Embed in Bone And Induce Apoptosis of Activated Osteoclasts
Green JR. Oncologist 2004;9(Suppl 4):3–13; Roodman GD. N Engl J Med 2004;350:1655–64; Mundy GR. Nat Rev Cancer 2002;2:584–93.

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Denosumab Inhibits RANK Ligand to Interrupt the ‘Vicious Cycle’ of Bone Destruction
Boyle WJ, et al. Nature 2003;423:337–42; McClung MR, et al. N Engl J Med 2006;354:821–31; Mundy GR. Nat Rev Cancer 2002;2:584–93.

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Outline
Mode of action of bone-targeting agentsEfficacy and safety of bone-targeting agents
◦ Fracture Prevention in Early-Stage Prostate Cancer◦ Delaying Bone Metastases in Prostate Cancer◦ Treatment of Bone Metastases Secondary to prostate
cancer◦ Safety profile
Reimbursement criteria for bone-targeting agentsSummary

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Treatment-related fractures
Disease-related skeletal complications
Castrate-sensitive nonmetastatic
Castrate-resistant nonmetastatic
Castrate-resistant metastatic
New bone metastases
Spectrum of Bone Disease in Prostate Cancer

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
1. Kanis JA. Osteoporosis. Blackwell Healthcare Communications Ltd; 1997. 2. Eastell R, et al. J Bone Mineral Res. 2002;17(suppl 2). Abstract 1170. 3. Lee WY, et al. J Clin Endocrinol Metab. 2002;87:329-335. 4. Maillefert JF, et al. J Urol. 1999;161:1219-1222. 5. Gnant M. Breast Cancer Res Treat. 2002; 76(suppl 1):S31. Abstract 12. 6. Shapiro CL, et al. J Clin Oncol. 2001;19:3306-3311.
ADT-Associated Bone Loss
Healthy men[1]
Early menopausal women[1]
Late menopausal women[1]
AI therapy in postmenopausal women[2]
Androgen deprivation therapy [4]
AI therapy plus GnRH agonist[5]
Ovarian failure secondary to chemotherapy[6]
Bone marrow transplant[3]
0
Lumbar Spine BMD Loss at 1 Yr (%)
2 4 6 8
0.5%
1.0%
2.0%
2.6%
3.3%
4.6%
7.0%
7.7%

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
ADT and Fractures
Yrs After Diagnosis
Un
ad
juste
d F
ractu
re-F
ree S
urv
ival (%
)
2 3 4 5 6 7 8 9 1010
100
90
80
70
60
50
40
30
20
10
Over a 4-yr period 19.4% fractures on ADT 12.6% fractures not on ADT
No ADT (N = 32,931)GnRH agonist, 1- 4 doses (n = 3763)GnRH agonist, 5-8 doses (n = 2171)GnRH agonist, ≥ 9 doses (n = 5061)Orchiectomy (n = 3399)
Shahinian VB, et al. N Engl J Med. 2005;352:154-164.

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Higher Death Rate Observed at 36 Mos in Pts With Vertebral Fracture at Study Entry
Saad F, et al. ECCO/ESMO 2009. Abstract 7005.
0
1
2
3
5
7
9
All Patients Placebo
Su
bje
cts
(%
)
10
Denosumab
8
6
4
7.6%
5.1%
9.2%
4.6%
5.8% 5.6%
HR: 1.57; P = .062Adj HR*: 1.55; P = .0698
HR: 2.14; P = .0194Adj HR*: 2.13; P = .021
HR: 1.09; P = .813Adj HR*: 1.08; P = .837
Prevalent vertebral fracture
No prevalent vertebral fracture
*Adjusted for age and ADT duration
Subject incidence
Sample size
25
329
53
1035
16
174
23
504
9
155
30
531
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
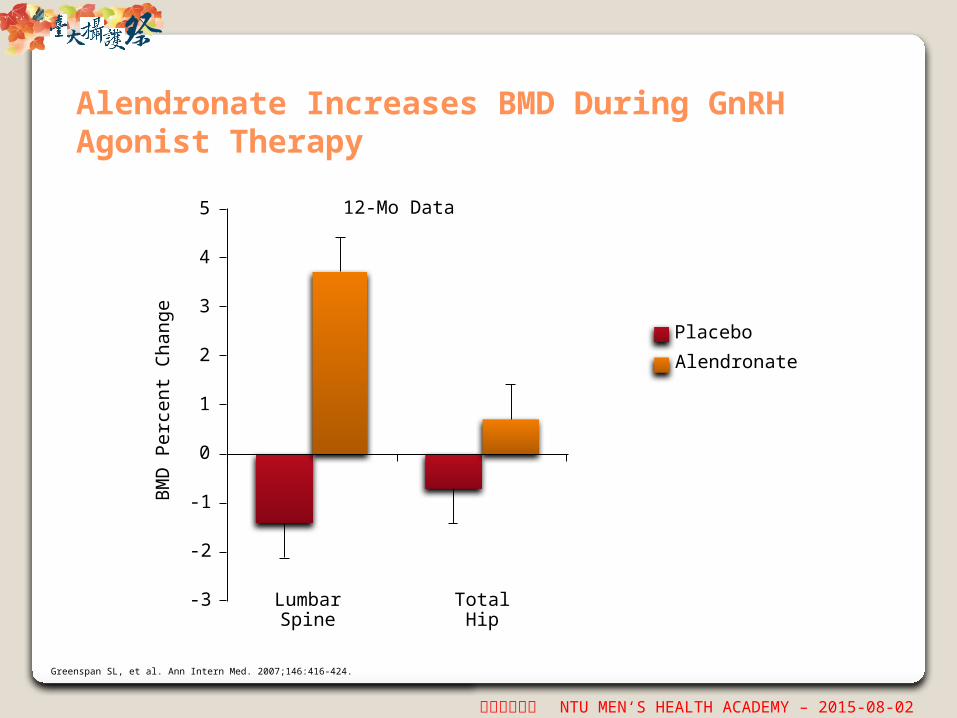
Alendronate Increases BMD During GnRH Agonist Therapy
Greenspan SL, et al. Ann Intern Med. 2007;146:416-424.
-3
-2
-1
0
1
2
3
4
5
BM
D P
erc
ent
Ch
an
ge
Alendronate
Placebo
LumbarSpine
TotalHip
12-Mo Data

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Pamidronate IV Every 3 Mos
P ≤ .005 for each comparison
Smith MR, et al. N Engl J Med. 2001;345:948-955.
-5
-4
-3
-2
-1
0
1
2
Pamidronate
No pamidronate
LumbarSpine
TotalHip
BM
D P
erc
ent
Ch
an
ge
Final 12-Mo Data

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Annual Zoledronic Acid Increases BMD During GnRH Agonist Therapy
Michaelson MD, et al. J Clin Oncol. 2007;25:1038-1042.
-6
-4
-2
0
2
4
6
P < .005 for each comparison
Zoledronic acid 4 mg/yr IV
Placebo
LumbarSpine
Final 12-Mo Data
BM
D P
erc
ent
Ch
an
ge
TotalHip

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Denosumab Increased BMD at All Skeletal Sites
10
8
6
4
2
0
-2
-4
-601 3 6 12 24 36
Mos
Cha
nge
in B
MD
F
rom
Bas
elin
e (%
)
Femoral Neck
Denosumab
Placebo
Difference at 24 mos,3.9 percentage points
10
8
6
4
2
0
-2
-4
-601 3 6 12 24 36
Mos
Cha
nge
in B
MD
F
rom
Bas
elin
e (%
)
Lumbar Spine
Denosumab
Placebo
Difference at 24 mos,6.7 percentage points
Smith MR, et al. N Engl J Med. 2009;361:745-755.
8
6
4
2
0
-2
-4
-601 3 6 12 24 36
Mos
Cha
nge
in B
MD
F
rom
Bas
elin
e (%
)Placebo
Difference at 24 mos,5.5 percentage points
Distal Third of Radius
Denosumab
10
8
6
4
2
0
-2
-4
-601 3 6 12 24 36
Mos
Cha
nge
in B
MD
F
rom
Bas
elin
e (%
)
Denosumab
Placebo
Difference at 24 mos,4.8 percentage points
Total Hip10
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
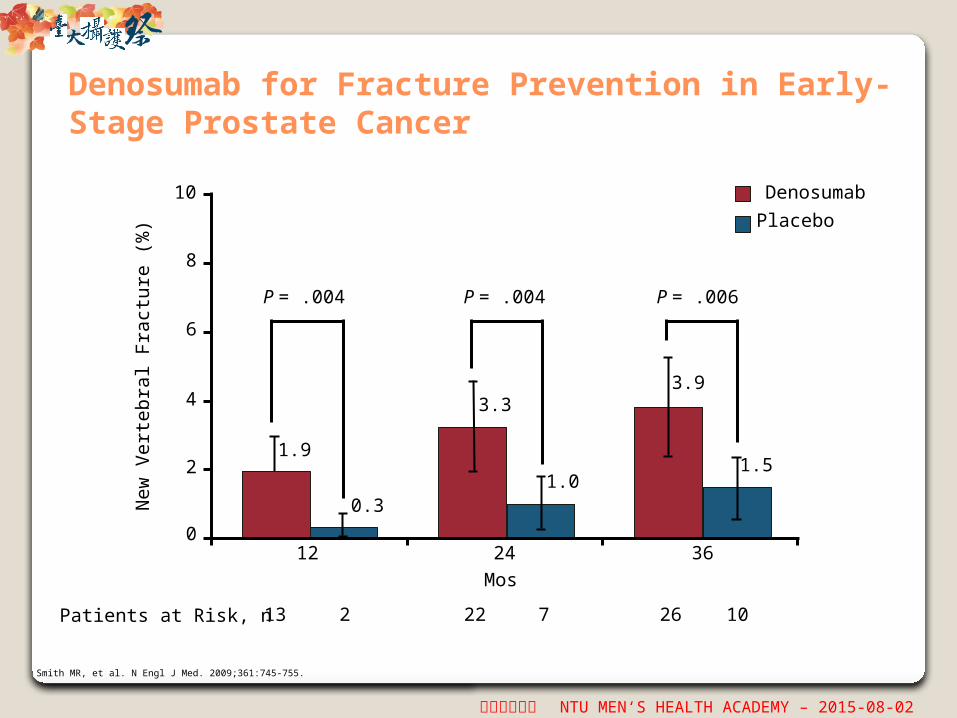
Denosumab for Fracture Prevention in Early-Stage Prostate Cancer
12Mos24 36
P = .004 P = .004 P = .006
1.9
0.3
3.3
1.0
3.9
1.5
0
2
4
6
8
10
New
Vert
eb
ral Fr
act
ure
(%
)
Placebo
Denosumab
13 2 22 7 26 10Patients at Risk, n
Smith MR, et al. N Engl J Med. 2009;361:745-755.
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Outline
Mode of action of bone-targeting agentsEfficacy and safety of bone-targeting agents
◦ Fracture Prevention in Early-Stage Prostate Cancer◦ Delaying Bone Metastases in Prostate Cancer◦ Treatment of Bone Metastases Secondary to prostate
cancer◦ Safety profile
Reimbursement criteria for bone-targeting agentsSummary

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Treatment-related fractures
Disease-related skeletal complications
Castrate-sensitive nonmetastatic
Castrate-resistant nonmetastatic
Castrate-resistant metastatic
New bone metastases
Spectrum of Bone Disease in Prostate Cancer
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Consequences of Prostate Cancer Progression on Bone Metastasis
Osteoporosis Osteopenia Worsening bone pain Spinal cord compression Bone marrow compromise Hyper/hypocalcaemia Additional therapy such as
surgery and radiation
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
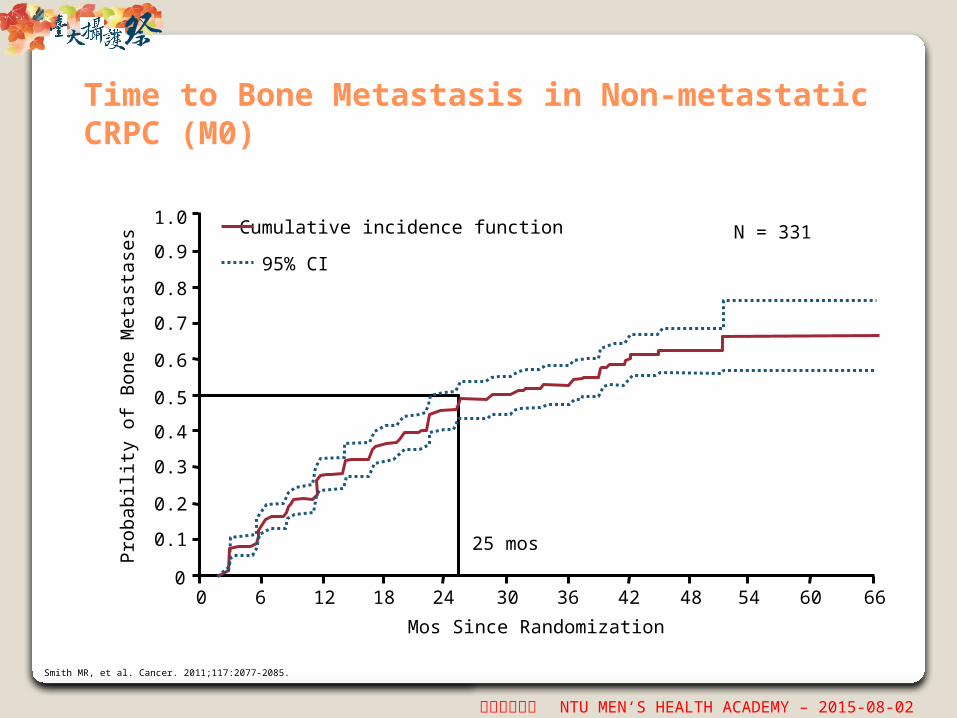
Time to Bone Metastasis in Non-metastatic CRPC (M0)
Smith MR, et al. Cancer. 2011;117:2077-2085.
25 mos
Mos Since Randomization
6 30 48 660
0.2
0.4
0.6
0.8
Pro
bab
ility
of
Bone M
eta
stase
s
0
0.1
0.3
0.5
0.7
0.9
1.0
12 18 24 36 42 6054
Cumulative incidence function
95% CI
N = 331
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
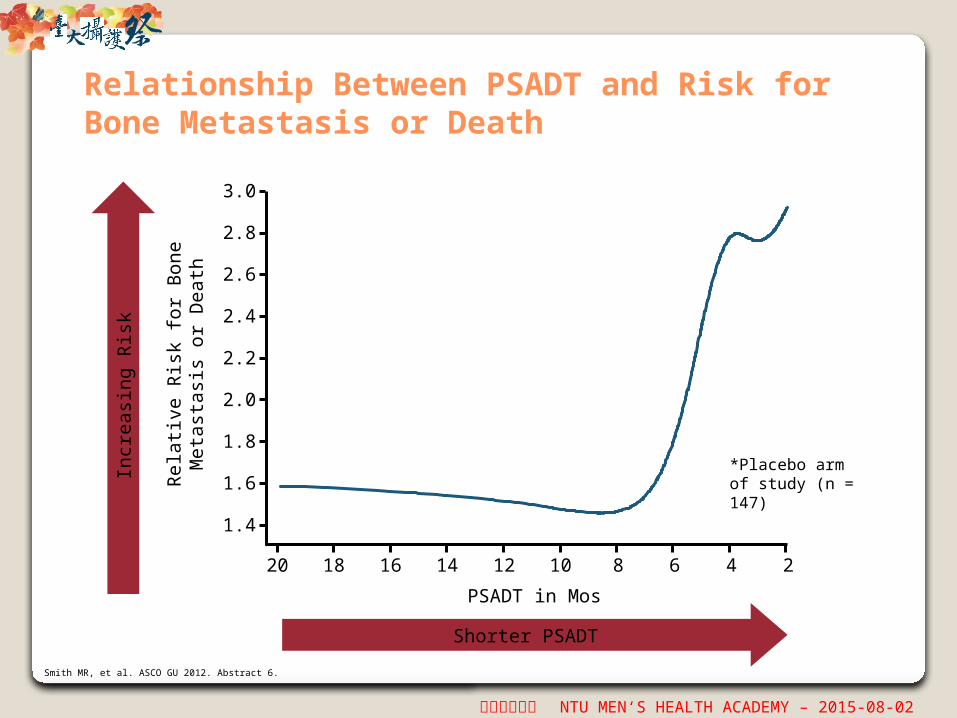
Relationship Between PSADT and Risk for Bone Metastasis or Death
Rel
ativ
e R
isk
for
Bon
eM
etas
tasi
s or
Dea
th
1.4
1.6
1.8
2.0
2.2
2.4
2.6
2.8
3.0
PSADT in Mos
20 18 16 14 12 10 8 6 4 2
Shorter PSADT
Incr
easi
ng R
isk
Smith MR, et al. ASCO GU 2012. Abstract 6.
*Placebo arm of study (n = 147)

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
PR04: Time to Symptomatic Bone Metastases or Prostate Cancer Death
Mason MD, et al. J Natl Cancer Inst. 2007;99:765-776.
60 960
20
40
60
80
0
100
12 24 36 48 8472 108
Mos From Random Assignment
Pro
port
ion F
ree o
f Sym
pto
mati
c B
on
e M
eta
stase
s and
Pro
state
Can
cer
Death
Patients at Risk, nPlacebo
Active254254
(1)(9)
248237
(8)(8)
234224
(16)(16)
204198
(11)(8)
185184
(4)(4)
174165
(9)(13)
145137
(6)(11)
118104
(4)(3)
7573
(7)(4)
3736
PlaceboClodronate
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
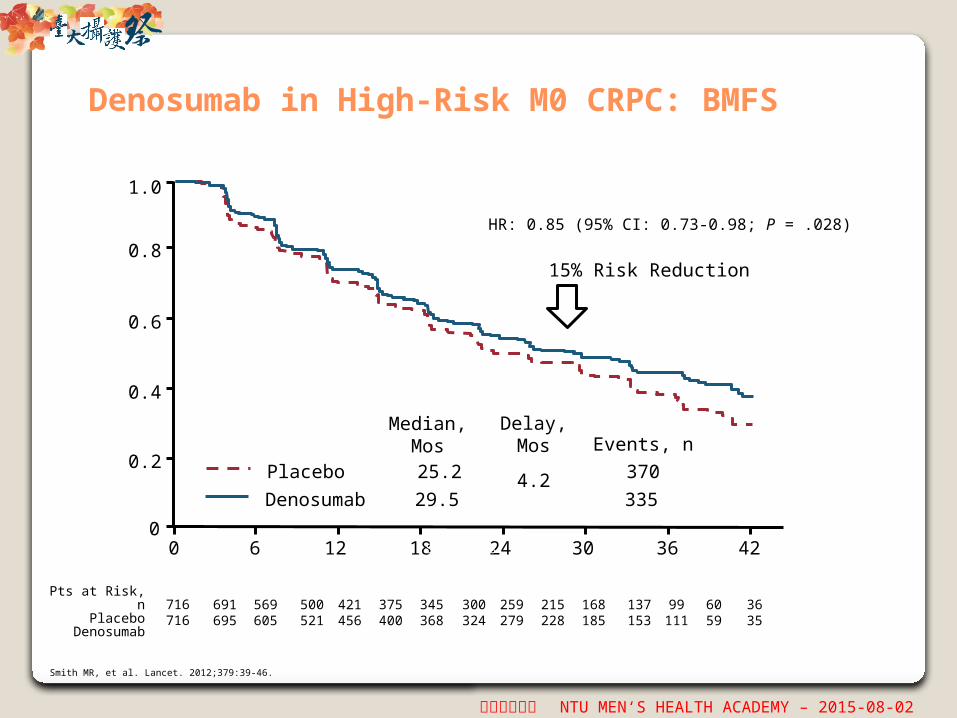
Denosumab in High-Risk M0 CRPC: BMFS
Smith MR, et al. Lancet. 2012;379:39-46.
Pts at Risk, nPlacebo
Denosumab
HR: 0.85 (95% CI: 0.73-0.98; P = .028)
15% Risk Reduction
Placebo
Denosumab
Median,Mos Events, n
25.2
29.54.2 370
335
Delay, Mos
Pro
port
ion o
f Pa
tients
W
ith
BM
FS
0
0.2
0.4
0.6
0.8
1.0
0 6 12 18 4224 30 36
716716
691695
569605
500521
421456
375400
345368
300324
259279
215228
168185
137153
99111
6059
3635
Study Mos

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Bone Metastasis–Free Survival in Patients With PSADT ≤ 6 Mos
HR: 0.77 (95% CI: 0.64-0.93; P = .006)
23% Risk reduction
Smith MR, et al. ASCO GU. 2012. Abstract 6.
Pro
port
ion o
f Pa
tients
Wit
h
Bon
e M
eta
stasi
s–Fr
ee S
urv
ival
1.0
0.6
0.8
0.4
0.2
0120 24 36
Study Mo427 323 223 176 122 78 47419 345 238 193 145 89 46
6 18 30
411406
274284
194207
148170
99109
6567
PlaceboDenosumab
MedianMos Events, n
Delay,Mos
18.725.9
7.224297
Patients at Risk, nPlaceboDenosumab

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Bone Metastasis–Free Survival in Patients With PSADT ≤ 4 Mos
HR: 0.71 (95% CI: 0.56-0.90; P = .004)
29% Risk reduction
Pro
port
ion o
f Pa
tients
Wit
h
Bon
e M
eta
stasi
s–Fr
ee S
urv
ival
1.0
0.6
0.8
0.4
0.2
0120 24 36
Study Month289 209 138 105 71 46263 217 143 117 89 56
6 18 30
279254
176176
117123
88102
5867
3538
PlaceboDenosumab
18.325.8
7.5167124
Smith MR, et al. ASCO GU. 2012. Abstract 6.
MedianMos Events, n
Delay,Mos
Patients at Risk, nPlaceboDenosumab

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Outline
Mode of action of bone-targeting agentsEfficacy and safety of bone-targeting agents
◦ Fracture Prevention in Early-Stage Prostate Cancer◦ Delaying Bone Metastases in Prostate Cancer◦ Treatment of Bone Metastases Secondary to prostate
cancer◦ Safety profile
Reimbursement criteria for bone-targeting agentsSummary

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Treatment-related fractures
Disease-related skeletal complications
Castrate-sensitive nonmetastatic
Castrate-resistant nonmetastatic
Castrate-resistant metastatic
New bone metastases
Spectrum of Bone Disease in Prostate Cancer

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Skeletal-Related Events and Clinical Consequences of Bone Metastases
Skeletal-Related Events Other Clinical Symptoms
Pathologic fractures* Spinal cord compression* Radiation therapy to bone* Surgery to bone* Hypercalcemia Change in antineoplastic
therapy
Bone pain Analgesic usage Quality-of-life deterioration Shortened survival
*Universally accepted skeletal-related events.
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
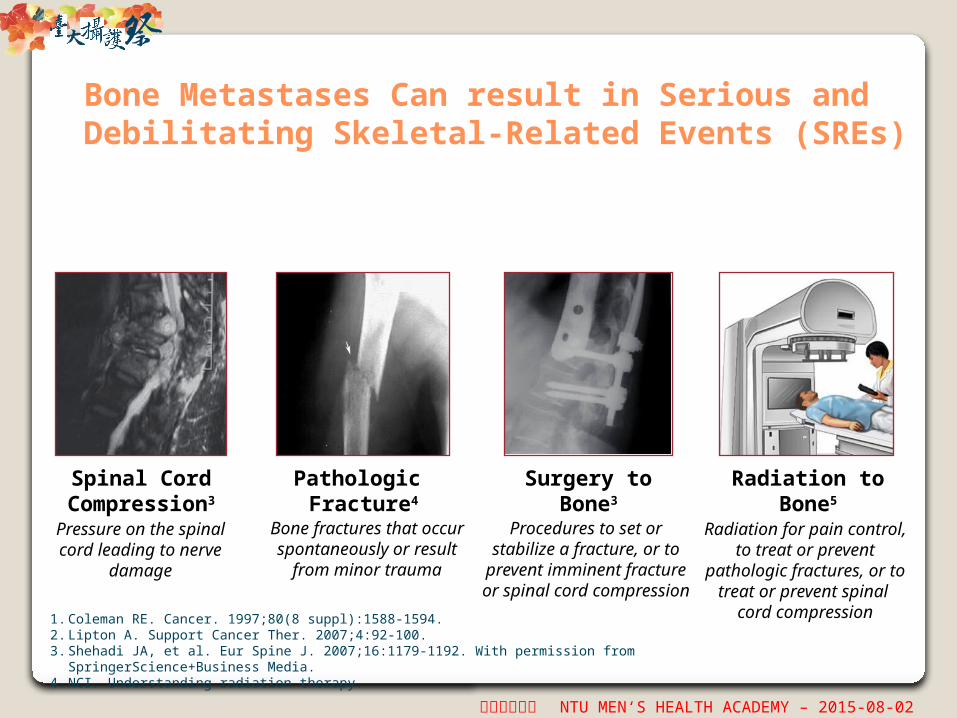
Bone Metastases Can result in Serious and Debilitating Skeletal-Related Events (SREs)
Spinal Cord Compression3
Pathologic Fracture4
Surgery to Bone3
Radiation to Bone5
Pressure on the spinal cord leading to
nerve damage
Bone fractures that occur spontaneously or result
from minor trauma
Procedures to set or stabilize a fracture, or to
prevent imminent fracture or spinal cord compression
Radiation for pain control, to treat or prevent
pathologic fractures, or to treat or prevent spinal
cord compression1. Coleman RE. Cancer. 1997;80(8 suppl):1588-1594.2. Lipton A. Support Cancer Ther. 2007;4:92-100.3. Shehadi JA, et al. Eur Spine J. 2007;16:1179-1192. With permission from SpringerScience+Business Media.4. NCI. Understanding radiation therapy.

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
PR05: Symptomatic Bone PFS
Dearnaley DP, et al. J Natl Cancer Inst. 2003;95:1300-1311.
Pro
port
ion o
f Pa
tients
Aliv
e a
nd
Wit
hout
Sym
pto
mati
c B
one
Pro
gre
ssio
n
0
0.2
0.4
0.6
0.8
0.1
0.3
0.5
0.7
0.9
1.0
0 12 48 6024 36 84
Mos From Randomization
72
Pts at Risk, n (Events)Active
Control155156
(42)(57)
11397
(36)(32)
7262
(17)(17)
5342
(8)(9)
3025
(9)(4)
811
(0)(5)
43
(0)(0)
21
ClodronateControl
Events112124
Total155156
HR: 0.79 (95% CI: 0.61-1.02;x2 = 3.39 [df = 1]; P = .066)

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Time to First SRE: Zoledronate vs Placebo
SREs: ZOL 4 mg 38%; placebo 49% (P = .028)
◦ 11% absolute risk reduction in ≥ 1 SRE
Pain/analgesia scores increased less with ZOL
No improvement in tumor progression, QoL, OS
0
20
40
60
80
100
0 120 240 360 480 600 720
Days
Median, Days
P Value
ZOL 4 mg 488.009
Placebo 321
ZOL 4 mg 214 149 97 70 47 353
Placebo 208 128 78 44 32 203
Perc
ent
Wit
hout
Event
Saad F, et al. J Natl Cancer Inst. 2002;94:1458-1468. Saad F, et al. ASCO 2003. Abstract 1523. Saad F, et al. J Natl Cancer Inst. 2004;96:879-882.

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Zoledronic Acid Studies Primary Endpoint: SRE
% W
ith
ou
t th
e E
vent
0
20
40
60
80
10
30
50
70
90
0 90 360 450180 270 540
Days After the Start of Study Drug
Patients at Risk, nZol 4 mg
Zol 8/4 mgPlacebo
214221208
163155149
113102103
926869
704643
541
000
Zol 4 mgZol 8/4 mgPlacebo
Saad F, et al. J Natl Cancer Inst. 2002;94:1458-1468.
100

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Zoledronic acid 951 733 544 407 299 207 140 93 64 47
Denosumab 950 758 582 472 361 259 168 115 70 39
Patients at Risk, n Study Mo
0
1.00
Pro
port
ion o
f Sub
ject
s W
ith
out
SR
E
0 3 6 9 12 15 18 21 24 27
0.25
0.50
0.75
KM Estimate ofMedian Mos
DenosumabZoledronic acid
20.717.1
HR: 0.82 (95% CI: 0.71-0.95;P = .0002, noninferiority;P = .008, superiority)
18%Risk
reduction
Time to First On-Study SRE: Denosumab vs Zoledronic Acid
Fizazi K, et al. Lancet. 2011;377:813-822.

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Denosumab vs ZOL in CRPC: No Effect on Overall Disease Progression and Survival
Overall Survival Time to Disease Progression
HR 1.03 (95% CI 0.91–1.17; p=0.65) HR 1.06 (95% CI 0.95–1.18; p=0.30)

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
ALSYMPCA: Overall Survival
Radium-223 541 450 330 213 120 72 30 15 3 0
Placebo 268 218 147 89 49 28 15 7 3 0
Parker C, et al. 2012 ASCO GU Cancers Symposium. Abstract 8.
OS
(%
)
Radium-223 (n = 541)Median OS: 14.0 mos
Placebo (n = 268)Median OS: 11.2 mos
HR: 0.695 (95% CI: 0.552-0.875; P = .00185)
3 6 9 12 15 18 21 24 27
MosPts at Risk, n
0
10
20
30
40
50
60
70
80
90
100
0
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Outline
Mode of action of bone-targeting agentsEfficacy and safety of bone-targeting agents
◦ Fracture Prevention in Early-Stage Prostate Cancer◦ Delaying Bone Metastases in Prostate Cancer◦ Treatment of Bone Metastases Secondary to prostate
cancer◦ Safety profile
Reimbursement criteria for bone-targeting agentsSummary

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Characteristics of Antiresorptive Agents Used for Patients with Prostate Cancer
International Journal of Endocrinology, 2015; http://dx.doi.org/10.1155/2015/838202

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Preventing and Managing Hypocalcaemia
41
1. Denosumab (XGEVA®) Summary of Product Characteristics; 2. Zoledronic acid (Zometa®) Summary of Product Characteristics;
3. Block G, et al. NFI. Orlando, USA. April 15–17 , 2010. Abstract;
4. NIH dietary supplement fact sheet: Vitamin D. Available at: http://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/ (accessed Jan 2014).
Vitamin D promotes calcium absorption in the gut and helps to maintain adequate serum calcium and phosphate concentrations4
Situation Action13
Pre-existing hypocalcaemiaCorrect before startingbone-targeted therapy
Start of bone-targeted therapyStart daily oral supplements of≥ 500 mg calcium and 400 IU vitamin D
Severe renal impairment (creatinine clearance < 30 mL/min) or dialysis
Denosumab: monitor calcium levels (recommended)Zoledronic acid: not indicated
Hypocalcaemia on therapyAdditional calcium supplementation may be necessary

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
藥物使用前的評估 是否能接受 BPs 或 Dmab 的使用 ?
沒有絕對不能接受 BPs 或 Dmab 使用的患者,只有日後產生骨壞死風險的高低。 日後產生骨壞死風險的高低決定於 –
使用前 使用前有無照會牙科進行口腔檢查,並接受口腔衛教? 使用前有無遵照牙科醫囑進行治療? 拔牙等侵入性治療,是否能在使用前至少 2-3 星期前完成?
使用期間 使用期間是否能維持良好口腔衛生?是否至少每半年牙科追蹤及洗牙?是否能發現早
期牙齒疾患,及時治療?是否活動假牙不合或配戴疼痛感時,能及時修整? 使用期間是否能避免產生拔牙、植牙、牙週病手術 ( 骨修整 ) 等侵入性手術的機會?
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
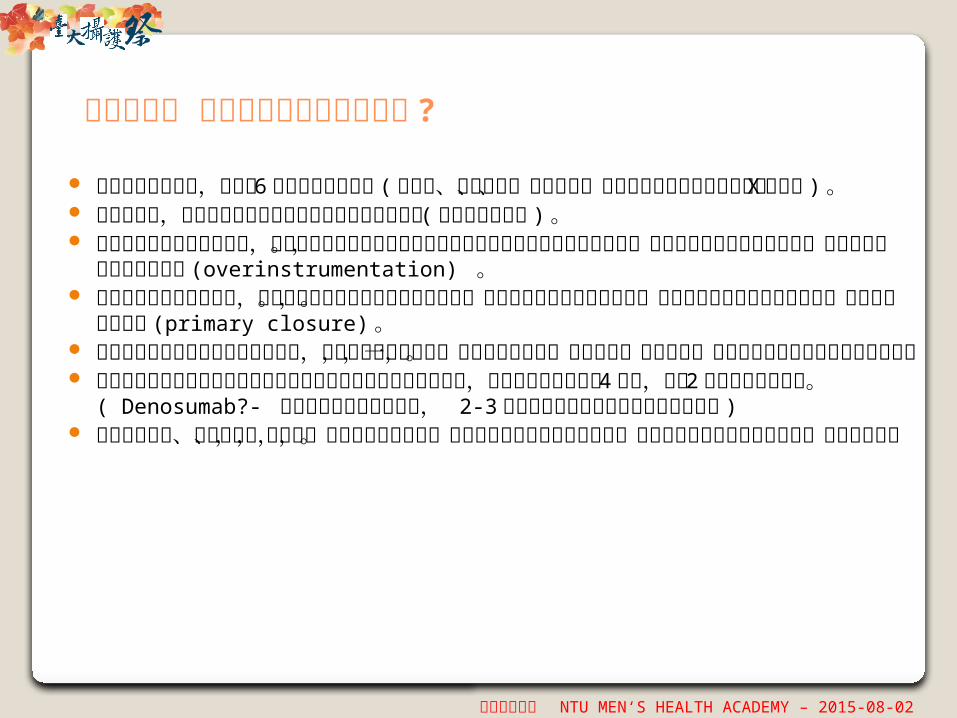
藥物使用中 如何預防顎骨壞死的產生 ?
保持良好口腔衛生,至少每 6 個月定期口腔檢查 ( 含洗牙、蛀牙填補、根管治療、修整不合活動假牙及顎骨牙齒 X 光檢查 ) 。
牙科就診時,要讓牙科醫師知道你正在使用抗骨吸收藥物 ( 頻率及使用期間 ) 。 並沒有絕對禁忌之口腔手術,但仍建議儘量避免拔牙或植牙等可能造成顎骨傷口的侵
入性治療。根管治療雖屬非侵入性治療,但需避免操作時超出根尖部(overinstrumentation) 。
若因牙科或內科急症考量,必要時拔牙或侵入性手術仍是適當的。當施行口內侵入性治療術前,先以抗生素預防及漱口水使用。傷口施行覆蓋縫合 (primary closure) 。
若有全口多處部位需進行侵入性治療,建議分次分部位進行,待傷口癒合正常,再進行另一部位治療,以避免產生多發部位顎骨壞死現象。
無證據證明停藥再施行牙科侵入性治療可減低發生顎骨壞死的風險,但對使用口服藥超過 4 年者,停藥 2 個月也許會有幫忙。 ( Denosumab?- 若要進行牙科侵入性治療, 2-3 個月的停藥有可能減少顎骨壞死發生率 )
當有牙齒鬆動、牙齦腫脹、疼痛時,儘快告知處方醫師,並至口腔顎面外科醫師處就診,以確定是否有顎骨壞死的產生,並及早治療。

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Outline
Mode of action of bone-targeting agentsEfficacy and safety of bone-targeting agents
◦Fracture Prevention in Early-Stage Prostate Cancer◦Delaying Bone Metastases in Prostate Cancer◦Treatment of Bone Metastases Secondary to
prostate cancer◦Safety profile
Reimbursement criteria for bone-targeting agentsSummary

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Bone-Targeting Agents in Taiwan
成分 適應症 健保給付規定
Clodronate• 惡性腫瘤之蝕骨性骨頭轉移• 惡性高血鈣症
• 血清鈣濃度超過 2.75 mmol/L (11.0mg
%) 或游離鈣大於 5.6 mg /dL 者• 惡性腫瘤之蝕骨性骨頭轉移之病患,在使
用嗎啡、可待因等止痛劑後仍不易控制者。• Multiple Myeloma, Breast Cancer,
Prostate Cancer併有蝕骨性骨轉移之病患
Pamidronate• 惡性腫瘤之蝕骨性骨頭轉移• 惡性高血鈣症
Zoledronic aicd
• 與標準癌症治療併用,適用於多發性骨髓瘤及固體腫瘤併有骨骼轉移之病人。用於攝護腺癌病人之骨骼轉移時,應至少接受過一種荷爾蒙治療而仍持續惡化者
• 治療惡性腫瘤之高血鈣併發症(HCM)
• 用於治療惡性腫瘤之高血鈣併發症 (HCM) ,且限用於血清鈣濃度超過 2.75
mmol/L (11.0mg/dL) 或游離鈣大於5.6 mg/dL
• Multiple Myeloma , Breast
Cancer , Prostate Cancer併有蝕骨性骨轉移之病患
Denosumab• 預防後期惡性腫瘤已擴散至骨骼
的患者發生骨骼相關事件• 乳癌、前列腺癌併有蝕骨性骨轉移之病患

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Guidelines for Management of Bone Metastases in Prostate Cancer
1. Heidenreich A, et al. EAU 2013. Available from http://www.uroweb.org/guideline (accessed Dec 2013).
2. NCCN Clinical Practice Guidelines Oncology. Prostate Cancer V4.2013. Available from www.nccn.org (accessed Nov 2013);
3. Horwich A, et al. Ann Oncol 2013;24:114162;
4. Cookson MS, et al. Castration-resistant prostate cancer: AUA guideline. J Urol 2013;190:42938.
N/A, not applicable. See guidelines for details on pre- and on-treatment monitoring/requirements.
European Associationof Urology
(2013)1
National Comprehensive Cancer Network
(2013)2
European Societyfor Medical Oncology
(2012)3
American Urological Association (2013)4
Drugs recommended
Bisphosphonates, denosumab
Denosumab,zoledronic acid
Denosumab,zoledronic acid
Denosumab, zoledronic acid
Patient population
CRPC andbone metastases
CRPC andbone metastases
CRPC and bonemetastases from CRPC at
high risk for clinically relevant SREs
Tumour burden (e.g. > 3 bone metastases, high alkaline phosphatase) and anatomic site of
bony metastases as well as previous history of
SRE can be used to judge SRE risk
CRPC andbony metastases
Optimal duration of treatment
N/A “Unclear” “Unknown” N/A

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Outline
Mode of action of bone-targeting agentsEfficacy and safety of bone-targeting agents
◦Fracture Prevention in Early-Stage Prostate Cancer◦Delaying Bone Metastases in Prostate Cancer◦Treatment of Bone Metastases Secondary to
prostate cancer◦Safety profile
Reimbursement criteria for bone-targeting agentsSummary
男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
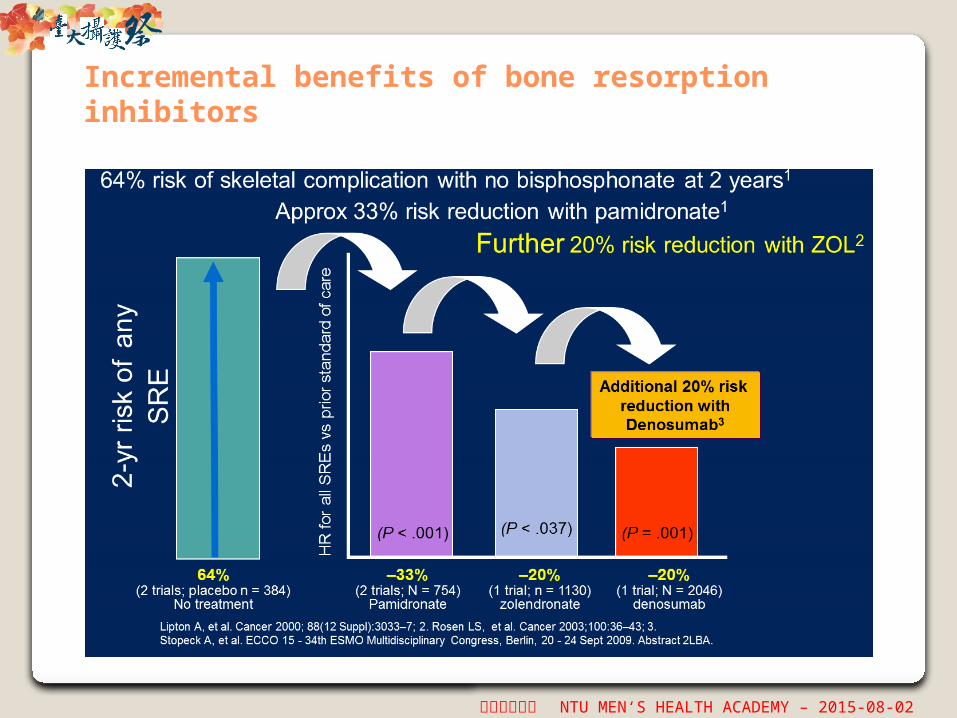
Incremental benefits of bone resorption inhibitors

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Summary of Phase III Trials Investigating the Use of Antiresorptive Drugs
International Journal of Endocrinology, 2015; http://dx.doi.org/10.1155/2015/838202

男性健康學園 NTU MEN‘S HEALTH ACADEMY – 2015-08-02
Thank you for your attention!
Discussion




![篩檢極早期失智症 AD8dharma.fgs.org.tw/shrine/fgsastw8y/01/download/AD8 I-Lan [相容模式].pdf · 篩檢極早期失智症: ad8 楊淵韓醫師 高雄醫學大學神經內科](https://img.dokumen.tips/doc/110x75/5e2457c28111f767994c2afc/coec-i-lan-cpdf-coec-ad8.jpg)
























