Embed Size (px)
Citation preview

Bone Metastases and Mortality: Can We Be Doing More?
Leonard G. Gomella, MD Chairman, Department of Urology President Society of Urologic Oncology Sidney Kimmel Cancer Center Thomas Jefferson University Hospital

Economic Burden of CaP to Bone

Bone Health Issues In Prostate Cancer
• Use of ADT and osteoporosis risk – Epidemiology – Preven@on strategies
• Morbidity and mortality of bone metastasis and prostate cancer – Epidemiology and physiology of bone metastasis – Basis of new bone targeted agents – Minimizing risk of bone metastasis – Prac@cal aspects of radium 223

Bone Health Issues In Prostate Cancer
• Use of ADT and osteoporosis risk – Epidemiology – Preven9on strategies
• Morbidity and mortality of bone metastasis and prostate cancer – Epidemiology and physiology of bone metastasis – Basis of new bone targeted agents – Minimizing risk of bone metastasis – Prac@cal aspects of radium 223

Propor@on of Pa@ents with Fractures 1 to 5 Years AKer CaP Diagnosis
Shahinian et al. N Engl J Med. 2005;352:154-164.
0
3
6
9
12
15
18
Any Fracture
Fracture Resulting in Hospitalization
Freq
uen
cy (
%)
+2.8%; P < 0.001
+6.8%; P < 0.001 ADT (n = 6650)
No ADT (n = 20,035)
12.6
21
5.2
19.4
2.4

Survival AKer Hip Fracture
6 Trombetti A et al. Osteoporos Int. 2002;13:731-737
Hip fractured Women
Hip fractured Men
Women
Men
Expected survival in the general population
2 4 6 8 10 0.00
0.25
0.50
0.75
1.00
Surv
ival
pro
babi
lity
Time after hip fracture (years) 0

Prevalence of Osteoporosis Increases with ADT Dura@on
Morote J, et al. Urology. 2007;69:500-504.

Diagnosing Osteoporosis
• In clinical prac@ce, Bone Mineral Density (BMD) remains the gold standard.
• BMD is one of the best determinants of bone strength
• Correlates with fracture risk
• BMD predicts fracture as reliably as blood pressure predicts stroke
US Dept of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General 2004. Marshall et al. BMJ 1996: 312: 1254-1258

WHO Criteria for Osteoporosis by DXA
9 Kanis JA et al. J Bone Miner Res. 1994;9:1137-1141
T-‐Score Normal -‐1 and above
Low bone mass -‐1 to -‐2.5
Osteoporosis < -‐2.5
Established osteoporosis < -‐2.5 and one or more fractures

WHO/FRAX® Risk Assessment
https://www.shef.ac.uk/FRAX/tool.jsp Accessed December 22, 2016.

Osteoporosis and Bone Metastasis Preven@on and Treatment
• Vitamin D supplementa9on – 20%-‐35% decrease fracture risk with >480 IU Vitamin D – Maximum bone density achieved with Vitamin D levels > 40, lowers risk of fracture
– The spine is not affected by Vitamin D – Calcium absorp@on in the gut is directly dependent of Vitamin D. If deficient, need 3000 mg Calcium to get absorbed, if sufficient (>32) only need 1000 mg calcium
• Recommend 1000 IU – 1200 IU daily – Obtain a 25(OH)D (only accurate way to evaluate) not 1,25(OH)D which is normal/elevated in Vit. D deficiency.
Bischoff-Ferrari HA et al. JAMA .2005;293:2257. Dawson-HughesB, et al. Osteoporosis Int. 2005;16:713. Heaney RP. J Am Coll Nutr. 2003;22:142-146Holick MF Mayo Clin Proc. 2006;81:353-73.

Osteoporosis and Bone Metastasis Preven@on and Treatment
Calcium Supplementa9on
• Recent data: calcium supplementa@on of >1000 mg increased risk of CVD mortality by 20% in men.
• Some now recommend: obtain most of calcium through diet, supplement if needed with calcium 600 mg daily – Not widely promoted
• My OTC Choice: Caltrate 600+D3 – (800 IU cholecalciferol)
Larson S. JAMA InterMed.2013;173(8):647-648.

Bisphosphonates • Inhibits osteoclast ac@vity, reducing bone resorp@on and turnover
• Increase BMD: spine by 5-‐8%; hip 3-‐6% aKer 3 years.
• Reduced incidence of vertebral fractures by 40-‐70% • Do not give if GFR <30 • Need dental exam before star@ng and every 6 months
Black DM, et al. J Clin Endocrinol Metab. 2000;85:4118-4124. Harris ST et al. JAMA. 1999;282:1344-52. Chesnut CH et al. J Bone Min Res. 2004;19:1241-1249. Black DM, et al. N Eng J Med. 2007;356:1809-1818.

Common Bisphosphonate Side Effects
• Dysphagia • Esophagi@s, ulcera@on • Nausea, dyspepsia • Uvei@s • Osteonecrosis jaw • Hypocalcemia • Renal impairment • Musculoskeletal pain • Class Warnings:
– Infrequent bone, joint and/or muscle pain – Osteonecrosis of the jaw – Atypical fractures of femoral shaV.
14

Denosumab • Monoclonal an@body that binds to RANK ligand to inhibit forma@on, func@on, and survival of osteoclasts therefore reducing bone resorp@on
• Increases bone density by 6.7% at the spine aKer 2 years
• Decreased incidence of vertebral fractures by 68%, hip by 40%
Cummings SR, et al. N Eng J Med. 2009;361: 751. Smith, MR et al. N Eng J Med 2009; 361:745.

Common Osteoporosis Agents in Men

Two Forms/Indica@ons for Denosumab
• Prolia®: Men on ADT or osteoporosis • 60 mg SC Q 6 mo
Denosumab
• Xgeva® : Men w/mets , not men w/ osteoporosis
• 120 mg SC Q mo Denosumab

Na@onal Osteoporosis Founda@on Fracture Preven@on Guidelines for Men
• Consider FDA-‐approved medical therapies based on the following – A vertebral or hip fracture – Femoral neck or spine T-‐score ≤ -‐2.5 – FRAX 10-‐yr probability of a hip fracture ≥ 3% or 10-‐yr probability of any major fracture ≥ 20%
National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of Osteoporosis. 2010.

Healthy Bone Program: ADT hip fracture reduced >70%
• DEXA scans for all men aged > 70 years • Men aged >50 years undergo screening if addi@onal risk factors are present, including ADT.
• DEXA repeated every 5 years. – T-‐score from -‐2.0 to -‐2.5: low bone mineral density – T-‐score of < -‐ 2.5 for a diagnosis of osteoporosis. – T-‐scores > -‐ 2.5 are advised on smoking cessa@on, regular exercise, adequate calcium intake (1200 mg/d), and adequate vitamin D intake (400-‐800 IU/d).
– T-‐scores < -‐2.5 are treated with pharmacologic interven@on;
• the first-‐line treatment is a bisphosphonate, and the pa@ent is followed up by an endocrinologist.
Zhumkhawala AA, Urology. 2013 May; 81(5):1010-‐7.

Bone Health Issues In Prostate Cancer
• Use of ADT and osteoporosis risk – Epidemiology – Preven@on strategies
• Morbidity and mortality of bone metastasis and prostate cancer – Epidemiology and physiology of bone metastasis – Basis of new bone targeted agents – Minimizing risk of bone metastasis – Prac9cal aspects of radium 223

Skeletal-‐Related Events and Clinical Consequences of Bone Metastases
Skeletal-‐Related Events • Pathologic fractures* • Spinal cord compression*
• Radia@on therapy to bone*
• Surgery to bone* • Hypercalcemia • Change in an@neoplas@c therapy
Other Clinical Symptoms • Bone pain • Analgesic usage • Quality-‐of-‐life deteriora@on
• Shortened survival
*Universally accepted skeletal-‐related events; Modified from Clinical Care Op@ons in Oncology [email protected]

Impact of PCa Bone Metastasis on Survival
Norgaard J Urol 2010; 184 (1); 162

Site of Pca Metastasis and Survival

CaP And Bone Metastasis • > 90% of pa@ents with mCRPC have bone metastases and experience skeletal-‐related events (SRE)
• SREs include spinal cord compression, pathological fracture, and need for surgery or radiotherapy
• Bone metastases are a major cause of death, disability, decreased quality of life, and increased treatment cost
• The an@-‐resorp@ve, bone-‐targeted therapies (zoledronic acid and denosumab) – do not improve survival – Do not delay metastasis – In some studies may delay or prevent SREs and others have not shown an advantage
J Clin Oncol. 2014 Apr 10;32(11):1143-‐50

CaP And Bone Metastasis
• About 50% of men with CRPC will develop metastasis within 2 years of CRPC diagnosis
• Median survival with mCRPC varies from 9 to 30 months on average
• More than 30% of men with CRPC thought to be M0 (non metasta@c) actually harbor mets and are actually M1 – Based on ENTHUSE (endothelin trial)

RADAR Study
Crawford ED Urology 2014 83(3):664

Alk Phos and PSA: Predict risk of Bone Mets

Bone an9resorp9ve therapy with MI disease

Fizazi K, et al. Lancet. 2011;337:813-822.
Phase 3 Study of Zoledronic Acid Versus Denosumab: Time to First SRE

• Common side effects that are similar between treatment groups: anemia, bone pain, nausea, decreased appe@te, cons@pa@on
• More hypocalcemia with denosumab (13% vs 6%) – Calcium and Vitamin D will decrease likelihood – No fatal episodes
• Osteonecrosis of jaw (ONJ) incidence low – 2% denosumab vs 1% zoledronic acid, P=0.09
• Acute phase reac@ons – 8% denosumab vs 18% zoledronic acid
Fizazi K, et al. Lancet. 2011;337:813-822.
Zoledronic Acid Versus Denosumab: Adverse Events

St. Galen Advanced CaP Consensus
Annals of Oncology 26: 1589–1604, 2015

St Galen Advanced CaP Consensus
Annals of Oncology 26: 1589–1604, 2015

The Curies and their Discovery of Radium
The Curies informed the l'Académie des Sciences, on December 26, 1898, that they had come upon an additional very active substance that
behaved chemically almost like pure barium. They suggested the name of radium for the new element.
1903 Mme. Curie shared the Nobel Prize with her husband
(and Henri Becquerel)


Radium Targets Osteoblastic Bone Metastases by Acting as a Calcium Mimetic
McDevitt et al. Eur J Nucl Med. 1998;25:1341-1351.
Calcium Strontium
Radium Barium

Radium Is a Bone-Seeking Calcium Mimetic That Binds to Hydroxyapatite [Ca10(PO4)6(OH)2]
Bruland et al. Clin Cancer Res. 2006;12:6250s-6257s.
Hydroxyapatite is intertwined with osteoid and cancer cells in the osteoblastic lesion
Cancer Cells
New Bone

Alpha vs Beta radioisotope therapy
1. Robinson et al Radiographics 1989 2. Serafini et al J Clin Oncol 1998 3. Parker et al New Engl J Med 2013

Critical Differences in Alpha- and Beta-Particles
α β Relative particle mass 7300 1 Initial energy (MeV) per particle 3-8 0.01-2.5 Range in tissue (µm) 40-100 50-5000 LET (KeV/µm) 60-230 0.015-0.4 DNA hits to kill cells 1-10 100-1000
LET = linear energy transfer. Henriksen et al. J Nucl Med. 2003;44:252-259.
Alpha Beta

Lethality of Alpha-Particles Is due to DNA Double-Strand Breaks
More Repairable
Bruland et al. Clin Cancer Res. 2006;12:6250s-5627s.
Single-strand breaks
Double-strand breaks
Lethal, more difficult to repair
Alpha radiation
Beta and gamma radiation

Bottom Line: Radium-223 Is Short Range But Deadly
• Highly localized cell killing with minimal damage to surrounding hematopoietic tissueα-particles cause double-strand DNA breaks in nearby tumour cells
• Limited penetration of α emitters (~ 2-10 cell diameters) results in highly localized killing of tumor cells with minimal collateral damage to normal tissue in surrounding area
2-10 cell diameter range of alpha-particle
Radium-223
Perez et al. Principles and Practice of Radiation Oncology. 5th ed. Lippincott Williams & Wilkins; 2007

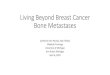
Choline PET Images Before and After Radium-223
Miyazaki et al. Nuc Med Mol Imag 49:314, 2015
Before Radium-223 After Radium-223


TREATMENT
6 injections at 4-week intervals
Radium-223 (50 kBq/kg) + Best standard of care
Placebo (saline) + Best standard of care
R A N D OM I S E D
2:1
N = 922
PATIENTS
• Confirmed symptomatic CRPC
• ≥ 2 bone metastases
• No known visceral metastases
• Post-docetaxel or unfit for docetaxel
ALSYMPCA Phase III Study Design
• Total ALP: < 220 U/L vs ≥ 220 U/L • Bisphosphonate use: Yes vs No • Prior docetaxel: Yes vs No
STRATIFICATION
Parker et al. N Engl J Med. 2013;369:213-223. 43

ALSYMPCA Overall Survival in mCRPC
Radium-223 Median OS: 14.9 months
Placebo Median OS: 11.3 months
HR = 0.70 95% CI, 0.581, 0.832 P = 0.00007
Month 0 3 6 9 12 15 18 21 24 27 30 33 36 39 Radium-223 614 578 504 369 274 178 105 60 41 18 7 1 0 0
Placebo 307 288 228 157 103 67 39 24 14 7 4 2 1 0
%
0
10
20
30
40
50
60
70
80
90
100
Parker et al. N Engl J Med. 2013;369:213-223. 44

ALSYMPCA Time to First Symptomatic Skeletal Event in mCRPC
0
10
20
30
40
50
60
70
80
90
100
Pat
ient
s w
ithou
t Ske
leta
l Eve
nt (%
)
Months since Randomization 0 3 6 9 12 15 18 21 24 27 30
Radium-223
Placebo
Radium-223 (N = 614)
Placebo (N = 307)
Hazard Ratio (95% CI)
Median time to first SRE
15.6 months
9.8 months
0.66 ( 0.52-0.83)
Parker et al. N Engl J Med. 2013;369:213-223. 45

ALSYMPCA Adverse Events of Interest
All Grades Grade 3 or 4 Patients with AEs n, (%)
Radium-223 n = 600
Placebo n = 301
Radium-223 n = 600
Placebo n = 301
Hematologic
Anemia 187 (31) 92 (31) 77 (13) 39 (13)
Neutropenia 30 (5) 3 (1) 13 (2) 2 (1)
Thrombocytopenia 69 (12) 17 (6) 38 (6) 6 (2)
Non-hematologic
Bone pain 300 (50) 187 (62) 125 (21) 77 (26)
Diarrhea 151 (25) 45 (15) 9 (2) 5 (2)
Nausea 213 (36) 104 (35) 10 (2) 5 (2)
Vomiting 111 (19) 41 (14) 10 (2) 7 (2)
Constipation 108 (18) 64 (21) 6 (1) 4 (1)
Parker et al. N Engl J Med. 2013;369:213-223. 46

ALSYMPCA Conclusions
In CRPC patients with bone metastases:
• Radium-223 significantly prolonged Overall Survival by 3.6 mo – P value = 0.00185; HR = 0.695; 95% CI, 0.552-0.875
• Radium-223 significantly prolonged time to first SRE by 5.8 mo – P value = 0.00046; HR = 0.610; 95% CI, 0.461-0.807
• Radium-223 was very well tolerated

Radium-223: Survival after 1-4 injections versus 5-6 injections in
Early Access Program
Sartor et al. ASCO 2015, #5063

Radium-223 and Bisphosphonates: No combined effect on survival in ALSYMPCA
but positive effect on Symptomatic SRE’s
Sartor et al. Lancet Oncology 15:738, 2014

ALP and PSA as Ra-‐223 Markers
• PSA not reliable; may only slow increase • ALP (alkaline phosphatase) shows u@lity • Phase 3b study 696 men (ESMO 2016)
– 298 men 43% no decline – 398 men 57% ALP decline
• 70% decreased death • 53% decreased SRE
Annals of Oncology (2016) 27 (6): 243-‐265. 10.1093/annonc/mdw372

Ra-‐223 for M1 DISEASE

Radium-‐223 Label INDICATIONS AND USAGE
• Xofigo is an alpha par@cle-‐emiwng radioac@ve therapeu@c agent indicated for the treatment of pa@ents with castra@on-‐resistant prostate cancer, symptoma@c bone metastases and no known visceral metasta@c disease.
DOSAGE AND ADMINISTRATION • The dose regimen of Xofigo is 55 kBq (1.49 microcurie)/kg BW,
given at 4 week intervals for 6 injec@ons. DOSAGE FORMS AND STRENGTHS
• Single-‐use vial at a concentra@on of 1,100 kBq/mL (30 microcurie/mL) at the reference date with a total radioac@vity of 6,600 kBq/vial (178 microcurie/vial) at the reference date
CONTRAINDICATIONS • Pregnancy

2016 Dosing Change
• The Na@onal Ins@tute of Standards and Technology (NIST) revised the standards for radium-‐223 in 2015
• The numerical value of the radioac@vity (in Bq/mL) contained in vials of radium Ra 223 and hence the pa@ent dose in Bq/kg body weight increase by ~10%:
• Result: increase of the radioac@vity from 1000 kBq/mL to 1100 kBq/mL at the reference date.
• Increase in pa9ent dose, from 50 kBq/kg body weight to 55 kBq/kg body weight (increase from 1.35 uCi (microcurie)/kg BW to 1.49 uCi /kg body weight)
hyps://hcp.xofigo-‐us.com/downloads/PP-‐600-‐US-‐2066_Xofigo_NIST_Update_Dear_HCP_Leyer.pdf

Can J Urol. 2016 Jun;23(3):8301-‐5

Ra-‐223 Protocol (cont.)
Can J Urol. 2016 Jun;23(3):8301-‐5

Ra-‐223 Lab parameters
Can J Urol. 2016 Jun;23(3):8301-‐5

Conclusions • In pa@ents on ADT consider monitoring DEXA; start with basic management strategies before Rx
• Strongly consider an@resorp@ve therapy with M1 – Many consider it standard with mCRPC
• Radium 223 useful in mCRPC with symptoms and significant bone mets – Sequencing of mCRPC agents under study – Combina@ons w/other mCRPC agents appears safe
• Ins@tu@onal programma@c support to u@lize Radium-‐223 in the clinic