Embed Size (px)
Citation preview

workimages in hematology
Bone marrow infiltration by plasmablastic neoplasm:plasmablastic myeloma or plasmablastic lymphoma?Entsar Eladl and Hong Chang, University of Toronto
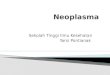
A B C
D E F
A 67-year-old HIV-negativeman presented with a history of sinuslesions and elevated serum monoclonal immunoglobulin Gkappa but no evidence of lytic bone lesions. Serum calcium,creatinine, and complete blood count were normal. Peripheralblood smear was unremarkable. A bone marrow workup showednormocellularity with trilineage hematopoiesis and partial involve-ment by an abnormal population of large cells that exhibitedamphophilic cytoplasm, oval nuclei, and variably prominentnucleoli (panel A: Wright-Giemsa stain, original magnification31000; panel B: hematoxylin and eosin stain, original mag-nification 3400). By immunohistochemistry, these abnormalcells were positive for CD138 (panel C; original magnification3200), MUM1 (panel D; original magnification 3200), CD56,C-MYCwith kappa restriction, negative for PAX5 (panel E; originalmagnification3200), CD20, CD45, CD30, CD117, cyclin D1, BCL-2, BCL-6, HHV8, and ALK1. Epstein-Barr (virus)–encoded RNAs
(EBERs) were positive by in situ hybridization (panel F; originalmagnification 3200). The proliferation index by Ki-67 immuno-staining approached 95%. C-MYC translocation was demon-strated by fluorescence in situ hybridization (FISH), but no othermyeloma-associated chromosomal abnormalities were detectedby FISH. A diagnosis of plasmablastic lymphoma (PBL) wasrendered. Similar features were seen in his sinus mass.
PBL and plasmablastic myeloma are rare yet aggressive he-matologic neoplasms, with identical morphologic features andimmunophenotypical profiles, which often cause diagnosticchallenges. The presence of EBER positivity and absence ofmyeloma abnormalities detectable by FISH as well as absence ofmyeloma-defining signs of hypercalcemia, renal failure, anemia,and bone disease (CRAB) in this patient, support the diagnosisof PBL.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updatedwith new atlasand case study images. For more information, visit http://imagebank.hematology.org.
DOI 10.1182/blood.2020009735 © 2021 by The American Society of Hematology
1268 blood® 4 MARCH 2021 | VOLUME 137, NUMBER 9
Dow
nloaded from http://ashpublications.org/blood/article-pdf/137/9/1268/1801524/bloodbld2020009735.pdf by guest on 07 M
arch 2021