Embed Size (px)
Citation preview

~na~i~s associated wit
controlled loadi of bioglass-coate a~~~in~~ oxide endosteal bnplants
John R. Smith, B. Sunford, Flu.
B ioglass, a bone-bonding ceramic, apparently facilitates ankylosis at bio- material-bone interfaces, and there is much interest in its potential uses in the health sciences. Currently, little is known about the effects of force applied directly to bone without transversing the tissues that normally invest all bones. Will pressure applied directly to bone induce a cellular response? Does bioglass produce an ankylosis simulating that seen in the human dentition? On the premise that ankylosed teeth do not move under orthodontic loading, we conducted an investigation to see whether bioglass can offer a stable, biocompatible interface with bone under controlled loading.
Most biomechanical studies associated with tooth movement have been in the field of orthodontics.‘* 3o Knowledge of the bone response to compressive and tensile forces has enabled the orthodontist not only to move teeth but also to alter relationships of bones.18
Since the development of improved implant materials, their use in dentistry and medicine has increased. Many investigators have observed dental implants under occlusal loading.” I23 ” Others have placed skeletal implants in areas of stress, such as the tibia, femur, and hip joint of experimental animals.i, X3. I43 2i After animal sacrifice, tensile and torsional tests conducted on the bone-implant specimens demonstrated that the union between the bone and porous metals, porous ceramics, and bioglasses could withstand substantial force before failure. These tests provided significant information on the physi- cal characteristics of the bone-implant interface. However, the dynamic nature of the tissues under controlled unidirectional loading has received little attention in vivo.
Mechanical union has been the main method of attaching implants to bone. For example, bone grows into grooves or pores on the surface of ceramic, metallic, and polymer implants. Now it seems possible to achieve a chemical bond between the im- plant and bone by coating the implant with bioglass. Since the development of bio-
From the Department of Orthodontics, School of Dentistry, and the Regional Primate Research Center, University of Washington. This article won the 1978 Milo Hellman Research Award of the American Association of Ortho- dontists. This research was supported by United States Public Health Service Research Grants DE-02918 and DE-02931, by National Institutes of Health Grant RB-00166, and by the University of Washington Orthodontic Memorial Fund. This article is based on research submitted by the author in partial fulfillment of the requirements for the Master of Science in Dentistry degree, Department of Orthodontics, University of Washington.
0002.9416/79/120618+19$01.90/0 0 1979The C. V. Mosby Co.
Bone dynamics and bioglass-coated endostral implants 619
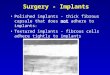
Fig. 1. Bioglass-coated aluminum oxide implant. A, Female portion of implant; B, short rod; C, post that protruded through the gingiva and accepted the gold coping.
glass, the physical and chemical properties of the bone-implant interface have been documented. 5, Iis 2g
Many bioglass compositions have been tested to determine which offers the best bonding potential to bone. One of these formulas (4535) consists of 4.5 percent Si02, 24.5 percent CaO, 24.5 percent Na,O, and 6 percent P205. Hench and Paschall” demonstrated that direct chemical bonding to bone was possible with the 45S5 formula. Stanley and associates33 found similar results, but by using bioglass with fluoride substituted for calcium they achieved ankylosis more consistently. Clark and colleague? stated that bioglass was slightly soluble in tissue fluid; when it was exposed to the acidic enzymes of wound healing, sodium ions were released from the bioglass surface. This produced a shift from an acidic to an alkaline pH. Calcium and phosphorus ions migrated toward the glass-solution interface to form an ion-rich gel. Owing to the high calcium and phosphorus concenlrations on the implant surface, osteoblasts began to differentiate from the sur- rounding tissues. Collagen fibrils and mucopolysaccharides generated by the osteoblasts were incorporated into the surface gel. Crystallization of the inorganic gel then resulted in a fusion of the bone and implant. Using tetracycline vital bone markers, mi- croradiography, and scanning electron microscopy, Hench and Paschall’j demonstrated new bone growth juxtaposed to implant surfaces. They found mature bone as early as 4 weeks and, by 12 weeks, complete laminar bone at the implant surface, producing an- kylosis,
Some authors have stated that ankylosed teeth do not respond to force loading as do normal teeth.32, 35 Mitchell and West26 orthodontically loaded suspected ankylosed teeth with bsth light and heavy forces. After 110 days of loading with forces from 6 to 12 ounces, no tooth movement was measurable. If ankylosis exists between bioglass and bone, a similar response might be seen with loading of the material in vivo.
Materials and methods
Three male rhesus monkeys (Macaca mulatta) were provided and maintained by the Regional Primate Research Center at the University of Washington in Seattle.
Smith
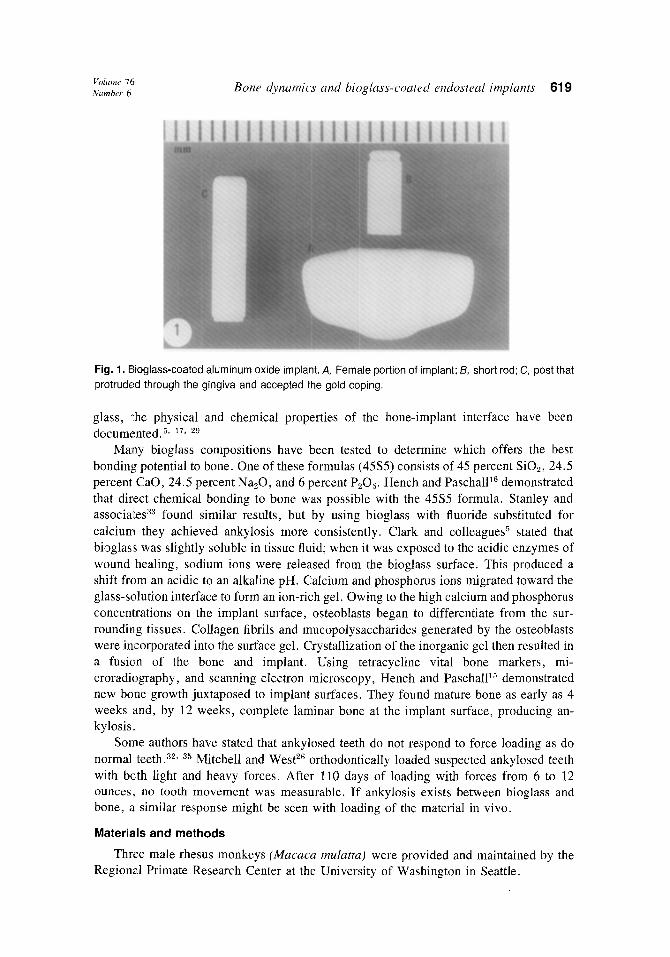
Fig. 2. Lingual arch appliance ligated into place
Monkey A (40 months old) was in the late mixed dentition with erupted first perma- nent molars and incisors. Nlonkeys B (62 months old) and C (66 months old) were in the adult dentition with third molars still unerupted. Ages of the wild-born animals were estimated according to the method described by Merrill.?-”
The animals were anesthetized with Ketamine HCl(l0 mg per kilogram) for examina- tions and with halothane for surgical procedures. They received crystalline penicillin (300,000 units) preoperatively and Bicillin (80,000 units per kilogram twice daily, every third day) postoperatively.
Greenspan and Hench”’ have established that 45S5 bioglass coated on A&O3 produces bone bonding. A similar composition was used in the present investigation. This study was begun before the findings of Stanley and his colleagues33 were published, so we did not use fluoride-substituted bioglass (45S5F).
Extraction and enucleation of all mandibular molars provided adequate recipient sites for the implants. Six weeks of healing yielded a suitable residual ridge for implantation.
The implants were designed for a two-stage surgical procedure (Fig. 1). After a full-thickness gingival flap was reflected from the extraction site, an undersized slot was cut into the residual ridge to receive the female portion of the implant. Final seating with a mallet and wood stick maximized contact between implant and bone. A short rod inserted into the female implant prevented tissue ingrowth during healing. Continuous sutures were used to establish primary closure of the surgical wound.
Nine weeks after the surgical procedure we made a small incision to remove the short rod and to cement the final post. The short implant rod on the left side in monkey B had become exposed through a small break in the gingiva after healing of the initial incision,

Volume 76 Number 6 Bone dynamics and biogluss-coated endosteal implants 621
A-SCANNING E.M. AND EDAX B-GROUND SECTION C-DECALCIFIED SECTION D-RESERVE
Fig. 3. Slabs A through D cut from block sections. Section D from monkey A subjected to SEM and EDAX analysis on the frontal plane.
so a second incision was not necessary. Durelon was used for all cementation procedures, since the polyacrylate cements offer adequate strength and no toxicity for a one-year period. 28 The animals were maintained in restraining chairs to prevent them from remov- ing or manipulating the posts. They received soft food and water ad libitum.
Tantalum implant markers placed bilaterally in the mandible allowed us to SU-
perimpose serial anteroposterior (frontal) radiographs. To minimize head-positioning error in the cephalostat, Cotton8 had implanted a cephalometric head positioneti7 in all animals 16 months earlier. During the courses of that study, however, the head positioner in monkeys B and C became mobile and could not be used for positioning in this investigation. Therefore, these two monkeys’ heads were positioned with standard ear rods and custom nasal rests made of acrylic.
Fourteen days after post cementation, cast-gold copings fabricated with buccal and lingual 0.046 inch stainless steel tubes were cemented with Durelon. The buccal tube accepted a 0.045 inch stainless steel rod, allowing measurement of angular changes of the implant with radiographic superimpositions. The lingual tube received the appliance that delivered the lingually directed continuous force. The appliance was a lingual arch made of 0.055 inch stainless steel wire. The distal ends of the wire were reduced to a diameter of 0.040 inch to facilitate insertion of the appliance into the lingual tubes on the coping. The appliance was fabricated from plaster models made from alginate impressions. Twelve weeks after insertion of the female portion of the implant, the appliance was ligated into place (Fig. 2). The constrictive force delivered to the mandibular implants was set and maintained at 425 grams by means of a coil-spring Ohaus scale.
Once a week we recorded anteroposterior (frontal) radiographs, interimplant distance and force level, and clinical estimates of inflammation and mobility. Indentations on the occlusal aspect of each coping facilitated interimplant distance measurement with a dial micrometer (Helios). Repetition of this measurement in monkey A twice at each weekly session showed the error to be 0.1 mm. The appliance remained activated while radio- graphs were made to minimize the effect of any implant mobility that might be present. Mobility was then measured with the appliance temporarily deactivated. A scale of 0

22 Smith Am. I. Urihd Drwmhrr 1979
ig. 4. Surgical exposure of the right implant in monkey 3 before insertion of post. Note reduced bone height on buccal surface of implant.
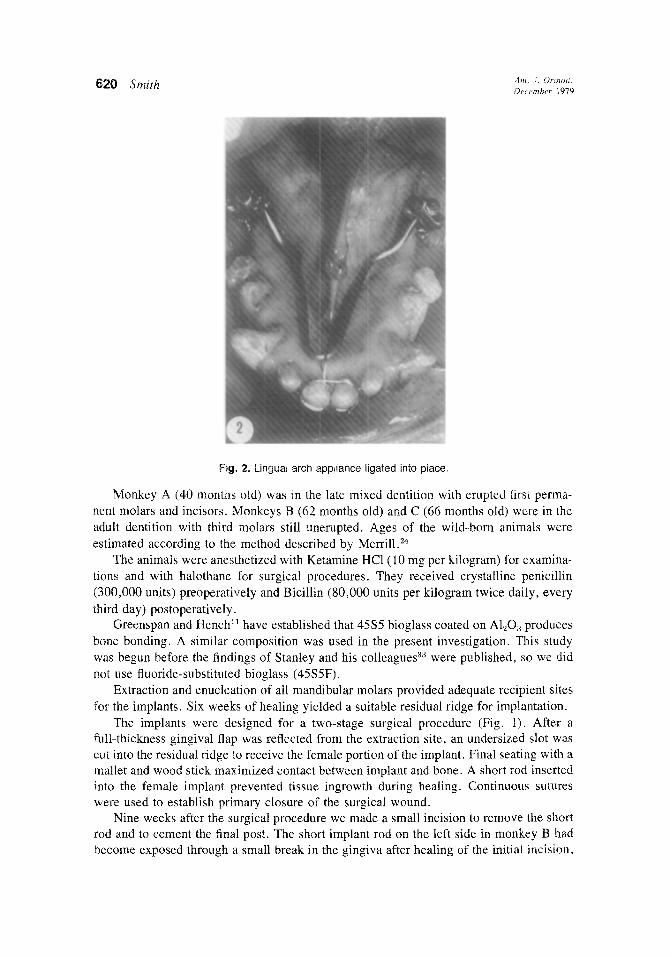
through 3 (0 = no mobility, 1 = <i mm. mobility, 2 = 1 mm. mobility, and 3 = >1 mm. mobility) quantified implant mobility. A plus (+) or minus (-) was assigned to a number to distinguish high and low variations of each range. Depending on gingival color, contour, and ease of hemorrhage, inflammation was rated as minimal, moderate, or severe. Force was measured by removing one side of the lingual arch and attaching an Ohaus scale to the free end. The 42%gram force was maintained for all animals except monkey A, which received 925 grams from the sixth week until death. Each week all teeth and implants were cleaned with a Cavitron to maintain a satisfactory level of oral hygiene and minimize plaque build-up.
Bone dynamics adjacent to the implants were documented by three oxytetracycline injections (50 mg per kilogram) administered intravenously 7 days after insertion of the female implant, on the day of force application, and on the day before sacrifice, Procion dye (H-8BS red, 100 mg per kilogram) given via the same route on the day of force application distinguished the first bone mark from the third.
After final records were obtained, the animals were killed and perfused with 10 percent formalin. Monkey A was killed at 9 weeks of loading, monkey B at 2 weeks, and monkey C at 5 weeks. Block sections containing the implants were radiographed and sectionedfrontally into four slabs, using a diamond wheel (Fig. 3). Radiographs of each
slab permitted visualization of the bone-implant interface. Slab A was divided sagittally so that the implant could be removed. The surfaces of
both implant and bone exposed by this procedure underwent scanning electron microscopy (SEM) and energy-dispersive analysis of x-rays (EDAX). Slab D from monkey A was subjected to the same analysis in the frontal plane so that the intact implant and bone junction could be visualized. Energy-dispersive analysis of x-rays consists of bombarding the specimen surface with a beam of electrons. This results in the emission of x-rays of wavelengths and intensities characteristic of the elements present. The radiation is then measured by the instrument and converted into a graphic representation of the substrate chemical composition. ” The EDAX is not sensitive to the radiation emitted by those
Volume 16 Number 6
Table I
Bone dynamics and bioglass-coated endosteal implants 623
ANIMAL A
ANIMAL B
ANIMAL C
i MOBILITY INFLAMMATION FORCE
R o-o-o-o-o-o MINIMAL
0-0-O-1’-’ (O-) 9 WEEKS) 425 g
(O+ 6 WEEKS;
L o-o-o-o-o-o MINIMAL 925 g ,“~1“~,‘-~,‘-’ (O-+ 9 WEEKS)
(6+ 9 WEEKS;
R MINIMAL+
o-o-o MODERATE
(O+ 2 WEEKS)
R a-l-l-l-l”’ MINIMAL
(O-, 5 WEEKS) 425 g
L 14’“-1”‘..1’+9-2 MINIMAL (O-+ 5 WEEKS)
(O-+ 5 WEEKS)
elements below the atomic number 9. Therefore, mineralized tissues with high calcium and phosphorus concentrations can be distinguished from connective tissue, which is mainly carbon.
Observations
Throughout the experimental period all of the animals responded well to the appliance and the restraining chair. Healing after all surgical procedures, with the exception of the left side of monkey B, was uneventful.
Visu.al assessment of the bone surrounding the implant at insertion of the post revealed that bone completely covered the implant wings in monkeys A and C. In monkey B there was considerable reduction in bone height on the buccal side of the right implant (Fig. 4). Probing of the left implant demonstrated deep pocketing on the buccal side, suggesting diminishled bone height.
Mobility and injlammation. The right implant in monkey A remained stable until the eighth week, when very slight mobility was noticed. The left implant in monkey A became slightly mobile after the sixth week of loading. The left implants in monkeys B and C were initially mobile, and the mobility progressed until both had approximately 1 mm. of movement in a buccolingual direction at the end of the loading period (Table I). The right implant in monkey B remained stable for the 2 weeks of loading before death. The right implant in monkey C was immobile initially but progressed to nearly 1 mm. of buccolingual movement.
Inflalmmation was minimal in monkeys A and C, with slight bleeding from the sulcus adjacent to the implant posts after probing (Fig. 5). Monkey B progressed rapidly to moderate inflammation bilaterally. The tissue demonstrated color changes and bled freely when probed. Gingival height had decreased significantly on the buccal aspect of the left

624 Smith
Fig. 5. The right implant in monkey C demonstrates the minimal inflammation found in the tissue around the other implants in monkeys A and C.
implant. Around every implant, a periodontal probe could be placed down the sulcus to the alveolar bone. It was doubtful that an epithelial attachment existed.
Force. The force level remained relatively stable after each week of activation. It occasionally decayed 25 to 40 grams but was easily adjusted by constriction of the anterior loop of the lingual arch.
Interimplant distance measurement. Throughout the loading period, no significant change in interimplant distance above measurement error was noted except in monkey A, which demonstrated a decrease of 0.3 mm. This decrease corresponded to the application of the 925 gram force. Since the interimplant distance remained constant after the eighth week of loading, the 0.3 mm. decrease was attributed to possible flexure of the mandible. These data are strikingly different than those reported by Cotton” (Fig. 6). In monkey A Cotton achieved 4.40 mm. of maxillary palatal expansion and a total increase of 6.90 mm. between the first permanent maxillary molars in a B-week loading period with a 1 pound force. Because of the presence of the midpalatal suture, the net tooth movement was 2.5 mm. In the present study, after the implants in monkey A had been loaded for the same amount of time and with a similar force magnitude, no movement was measurable. To further substantiate implant stability, the increase from 425 grams to 925 grams in monkey A still produced only a slight decrease in the interimplant distance. In Cotton’s study, monkey B was palatally expanded 0.72 mm. with a net first permanent molar movement of 0.49 mm. after 2 weeks of loading. Monkey C was expanded 0.88 mm. with a net first permanent molar movement of 1.14 mm. after 5 weeks of loading. No implant move- ment above measurement error was noted in this investigation for either monkey B or monkey C.
Anteroposterior Cfrontal) radiographs. Monkey A, which had the stable head posi- tioner, demonstrated a slight variation in the positions of tantalum implant markers as a result of errors in repositioning the mandible into maximum interdigitation before each radiographic exposure. Because of the very slight decrease in distance between the bio- glass implants, the superimposition error induced by tantalum implant variability in mon-

Vohmr 10 Number 6 Bone dynumics and bioglass-coated endosteal implants 625
6. ANIMALB
51
Al20rBIOGLASS IMPLANTS 4-
TANTALUM IMPLANTS ---------- 3- MAX. 1ST PERM. MOLAR . . . . . . . . . . . . . . . 2-
‘1
6. ANIMAL C
4 ] C TERMINATION OF IMPLANT LOADING ~
‘I I
2 1 ,,.... ..” ,..“.”
1; 3”’
,,,_..... ‘Y , 13 . i ,,,_, r ..,.. 3 . . . . . . . . . . .
,.: r” ..> : ” r____jl__-.i--- a---;’ 0;2.-./ ,
-I- i------ -- 1
iViEi<S' ' * ' Fig. 6. Comparison of the net change from the initial interimplant and intermolar distances, in millime- ters, for each animal in this study and in Cotton’s8 Measurements between the maxillary first perma- nent molars and small tantalum implants in the maxilla were used by Cotton to determine the degree of palatal expansion.

26 Smith
Figs. 7 and 8. Photomicroradiographs of silver-nitrate-impregnated ground sections, 250 pm thick, from the right implant in monkey A. Fig. 7 represents the lingual aspect of the implant. Note the radiolucency (F&L) between the bone (5) and implant (I). Fig. 8 represents the buccal aspect of the implant. Bone is found juxtaposed to the implant surface. (Magnification, x83.)
key A made interpretation unreliable. More variability in tantalum implant positions was found in monkeys B and C owing to ear rod positioning; thus, radiographs could not provide reliable indications of bioglass implant movements.
Microradiography. Ground sections approximately 250 km thick showed bone jux- taposed to the impiant surface at numerous areas. In other locations, a radiolucent line representing noncalcified tissue was evident (Figs. 7 and 8).
Histology. When mineralized bone is formed at the time tetracycline is injected, a bright yellow fluorescence will be observed when the undecalcified section is viewed with an ultraviolet light source. This demonstrates the bone dynamics adjacent to the implant. If remodeling changes are taking place on the pressure or tension side, distinctive patterns of fluorescent bone marks will be evident. In all samples, no marks were found adjacent to the implant.
Scanning the cortical bone and marrow spaces demonstrated that the three tetracycline marks and the procion mark were present and sufficiently brilliant to be identified. Fluorescent marks were distinct in the lingual alveolar crest above the implant, suggesting that new bone was laid down even during implant loading. The initial tetracycline label should have been present, but the drug was apparently given before mineralization had

Volume 16 Number 6 Bone dynumics and bioglass-coated endosteal implants 627
Fig. 9. Photomicrograph of the right implant in monkey A as viewed under an ultraviolet light source. No fluorescent lines are seen adjacent to the buccal (tension) surface of the implant. Marking is evident in the cortical bone. (Magnification, x 15.5.)
begun. Subsequent tetracycline marks were not evident near the implant, which implied a stable bony architecture (Fig. 9).
Fromi our knowledge of the bone dynamics adjacent to teeth under loading, we would expect bone resorption on the pressure side and apposition on the tension side. This was not the case with the bioglass-coated A&O3 implants, however. Laminar bone, verified by polarized light, was found contiguous with the bioglass surface on both the pressure and tension sides (Figs. 10 and 11). Direct contact between the bone and the implant appeared to be randomly distributed with no predilection for either side. In areas where bone was not in contact, connective tissue was present, with fiber arrangements running parallel to the implant surface. After implant removal in the laboratory, bioglass particles were still adjacent to the bone and connective tissue (Figs. 12 and 13). This combination of bone and connective tissue approximation was found around all implants except the left one in monkey B, which had total connective tissue encapsulation (Figs. 14 and 15). Osteo- blasts, osteoclasts, fibroblasts, and fat cells were found in approximately the same number

Figs. 10 and 11. Photomicrographs demonstrating the lamellar nature of the bone (LB) adjacent to the implant surface I!, on both the buccal (Fig. 11) and lingual (Fig. 10) surfaces. (Hematoxylin and eosin stain (polarized). Magnification, x87.5.)
on both sides of the implant. The majority of the inflammatory cells were concentrated around the post that exited into the oral cavity. The female portion of the implant was well tolerated by the investing tissues. Downward migration of the epithelium and inflammation stopped where the bone contacted the implant surface (Figs. 16 and 17). Occasional chronic inflammatory cells could be found below the bone-implant junction along the surface of the female portion of the implant. No resorption activity was present except on the buccal alveolar crest and occasionally the lingual alveolar crest on the outer cortical bone. This was attributed to thinning of these regions during initial female implant insertion which left a precarious ledge of bone susceptible to resorption.
Scanning electron microscopy and energy-dispersive analysis of x-ray. The intact slab D from monkey A was examined in the frontal plane with the SEM and EDAX, confirming the histologic and microradiographic interpretation of the bone-bioglass junc- tion (Fig. 18).
The implant and bony crypt exposed by the sagittal division of slab A revealed a diversity of surface characteristics when viewed with the SEM. For control data, an EDAX reading for bone, connective tissue, and bioglass was taken. Surface characteris- tics indicating bone were tested with the EDAX and compared with the controls. Tissue suggesting bone with high calcium and phosphorus levels was found on all implant surfaces except the left implant in monkey B. On the right implant of monkey A, only one

Volume 16 Number 6 Bone dynamics and bioglass-coated endosteal implants 629
Figs. 12 atnd 13. Bioglass particles (G) still attached to bone (/3) (Fig. 12) and connective tissue (CT) (Fig. 13) after implant removal. Note the presence of the squamous-like osteocytes (SO) and adipose tissue (A). (PAS-Alcian blue stain. Magnification, x255.)
slight area of bone was present. The calcified tissue deposits on the implant surfaces were randomly distributed, which substantiated the histologic findings. Bioglass, tissues of high calcium and phosphorus levels, and small amounts of aluminum were sometimes found in the bony crypt, suggesting that the bioglass was torn from the aluminum oxide substrate when the implant was separated from the bone. The SEM and EDAX verified areas where the bioglass surface was disrupted and the aluminum oxide substrate was exposed (Fig. 19).
The results of this experiment indicate that fusion between implant and bone did occur and the bond remained strong and unaffected by the prolonged period of continuous loading.
Discussion
The stability of the bioglass-coated Al,O, implant provokes an intriguing question: Why was no resorption, frontal or undermining, found in the bone on the pressure side? The typical cellular response seen with orthodontic tooth movement did not occur in this study.
The possibility that implant surface area may be the reason for the lack of normal cellular response to loading deserves scrutiny. There has been considerable debate about the optimum force level to produce the most efficient tooth movement. lg. 34 Investigators

30 Smith
Figs. 14 and 15. Comparison of the total tissue incapsulation seen with the !eft implant in monkey B (Fig. 14) versus the bony approximation seen in the right implant in monkey C (Fig. 15). (Mallory’s stain. Magnification, x 16.)
have documented the type of cellular response seen with applied light and heavy orth- odontic forces.3” 36 Regardless of the force magnitude, bone apposition and resorption were always found, on the microscopic level, associated with tooth movement. In this investigation no cellular response was evident, even after a loading period of 9 weeks. There appeared to be a deficiency in the mechanism which induced the typical tissue response. It is possible that surface area played a role in the stability of the bioglass- A1,03 implant against force. However, further studies are needed to establish how surface area influences bone dynamics and what factors initiate the complex cellular response.
The application of pressure or tension to bone does not necessarily result in resorption or apposition. Bassett3 stated that force application is not likely to act directly on the osteocytes embedded within the lacunae of the bone. Pressures seem to be transmitted throughout the compact bone along the canaliculi and lacunae. However, Bassett cautioned that hydraulic pressures, such as those described by Frost,” could be transmit- ted to the membranes of osteocytes. Curreyg stated that if localized groups of osteocytes were stimulated they may not have sufficient information to initiate the proper cellular response. Rather, a complex feedback mechanism, possibly via nerves, was necessary to integrate information on the net strain produced throughout the bone under loading. The lack of a cellular response in this study supports the concept that either osteocytes were not stimulated directly or there was insufficient stimulation to induce apposition and resorption.

Volume 76 Number 6
Bone dynamics and bioglass-coated cndostral implants 631
Figs. 16 and 17. Bone-implant union (arrow) demarcates termination of downward migration of inflam- mation, epithelium, and connective tissue on both the buccal (Fig. 16) and the lingual (Fig. 17) aspects of the implant. (Verhoeffs stain. Magnification, x40.)
All bones and roots of teeth are invested by some form of cellular connective tissue sheath. Force application to bones or teeth is necessarily mediated through this cellular envelope. With the ability to fuse an implant and apply forces directly to the bone, there is an opportunity to visualize the bone dynamics. What is seen is not resorption and apposi- tion but stability. Forces appear to be dissipated without triggering a cellular response. Therefore, the mechanism for either resorption or apposition appears to rest primarily on the ability of the investing tissue of the bones to sense changes in its environment.
Many hypotheses have evolved to explain the cell’s ability to discern changes in its local environment. Frost’O stated that apposition and resorption were a function of the mechanical stress induced in the bone during loading. When loading resulted in bone flexure, apposition was found on the concave or compressive side and resorption began on the convex or tension side. The net result was relocation of the bone with better force distribution through the bone mass. Other investigators have documented a similar cellular response with bone flexure but attribute the cellular response to bioelectric potentials which al-e generated on the bone surfaces.2. 23 Cochran and associates6 and others found that when a force was applied to the crown of a tooth the resultant tipping about the cen- ter of rotation within the root caused flexure of the alveolar bone, both lingual and buccal.3a, 3g This flexure produced an electrical potential consistent with their findings that bone apposition tended to occur at the concave surface, which was electronegative, and resorption occurred on the convex surface, which was electropositive.

Fig. 18. Scanning electron photomicrograph of bone (5) and implant (/I junction. EDAX readings verified the presence of bioglass (G), Connective tissue could not be found with the EDAX instrument between implant and bone within the brackets. (Magnification, x209.)
Theoretically, a different mechanical system is established when force is applied to the ankyiosed tooth or fused implant. Since the implant or tooth is an integral part of the bone as a result of bone fusion, the implant or tooth can no longer rotate on an axis within its own root. Rather, the center of rotation is transferred inferiorly to the bone mass. The electrical changes would probably be different. A contradiction arises concerning this hypothesis when the results of this study are reviewed. Mobility of approximately I mm. was noted in some of the implants. As mentioned earlier, this was apparently due to flexure of the bone attached to the implant surface. Why this mobility occurred and why it did not potentiate a cellular response cannot be explained by the results of this study. More experimental information on the behavior of ankylosed teeth and implant materials that fuse to bone is necessary before direct comparisons of these biologic phenomena can be made.
The bone-implant junction appeared to offer an adequate barrier to both inflammation and epithelization. The tendency for continued connective tissue “walling off” and epi- thelial surfacing was found in only one of the six implants. The favorable success rate for bone fusion without fibrous encapsulation was credited to the two-stage implant design which allowed total coverage of the implant during the first 9 weeks of healing.
The ability to produce ankylosis with a relatively strong and biocompatible material, such as bioglass-coated A&OS, offers tremendous applicability in dentistry and medicine. In orthodontics the applications could include the use of such implants for anchorage in

Volume 16 Number 6 Bone dynamics and bioglass-coated endosteal implants 633
Fig. 19. Scanning electron photomicrographs and energy-dispersive analysis of x-ray films of the lingual (N) and buccal (6) surfaces of the right implant in monkey B (x21). Areas of magnification, enclosed by the square, are represented by photographs E (x100) and F (x 190). EDAX control readings for bone (C) and bioglass (D) can be compared with those from the areas circled in E and F. These data suggest that bone was present on the lingual (compressive) surface.

34 Smith
tooth and bone movement. Such use seems very feasible when one compares the findings of Cotton8 and the results of this study.
Cotton demonstrated that a considerable degree of tooth movement occurred with paiatal expansion. Usually tooth movement during palatal expansion is an undesirable change resulting in adverse sequelae, such as poor axial inclination and inadequate func- tional relationships between the dental arches. Overexpansion is necessary because of the dental and skeletal relapse that usually follows removal of the palatal expander. Stable implants, such as those in this study, might facilitate better skeletal change, eliminating the tooth movement that causes undesirable treatment results. Methods of applying force in the presence of multiple anodontia, such as ectodermal dysplasia, may offer another potential use for biogiass implants.
Kokichz2 and others established that most of the craniofacial sutures remain patent until the later decades of life. 25 Since the suture is histologically and physiologically similar to the periodontal ligament, it should be possible to achieve bone movement with sufficient force magnitude and duration. At the present time, the teeth offer the only “handles” to which forces can be applied to bones. Their obvious limitation as anchors is their normal capacity for movement during loading and their relapse tendency afterward. Taking the concept of orthopedic movement a step further, the use of such implants may eventually enable the practitioner to influence the spatial relationships of other facial bones in severe craniofacial anomalies through extraoral force systems.
One of the major problems with orthopedic and orthognathic surgery is the mainte- nance of skeletal augmentations. For example, genial advancements by either horizontai osteotomies or biomaterials, such as silicone rubber, are often plagued by progressive resorption. Bioglass offers a stable interface between bone and implant under pressure; therefore, its use in skeletal augmentations and prostheses where functional stress is expected may prove invaluable.
The inadequacies of the conventional technique for head positioning by means of ear rods and a nasal rest were vividly demonstrated by this study. While that technique allowed precise positioning of the skull and upper face, it did not provide accurate reproducibility in positioning the mandible, and a new mode for stabilizing the mandible is therefore indicated. Future studies involving interpretation of changes within the man- dible should include a positioner placed intraosseously within the mandible. This would allow fixation directly to a static mount which would produce accurate repositioning of the mandible.
Summary and conclusions
Specially designed A&O3 implants coated with bioglass were placed bilaterally in the mandibular first molar region of three male rhesus monkeys. A lingual arch appliance fabricated to deliver a continuous lingually directed force was activated and ligated to gold copings cemented to the implant posts.
Measurements of interimplant distance established that all implants remained station- ary against a 425 gram force for periods of up to 6 weeks. The force was increased to 925 grams in one animal after the sixth week, with a resultant decrease of only 0.3 mm. at the end of the 9-week loading period. Clinical estimates of inflammation and mobility re- vealed that four of the six implants had minimal tissue changes around the implant posts, while the others had moderate changes.
Volume 16 Number 6 Bonr dqnamic,s and bioglass-coated rndosttjal implants 635
Histologic evaluation of block sections containing the implants demonstrated fusion between the bioglass and bone in five of the six implants. Further examination of the bone-implant interface by scanning electron microscopy and energy-dispersive analysis substantiated the light microscopic interpretation of bony fusion
Apparently, the union between the implant and bone was strong enough that fracture occurred in the bone rather than at the bioglass-bone interface. Bony union appeared to be random, on both the buccal and lingual surfaces of the implants. Where bone was absent, connective tissue could be found running parallel to the surface. The two-stage implant design which allowed total coverage of the implant during the first 9 weeks of healing was credited with the favorable success rate of bone fusion without fibrous encapsulation
With1 the ability to achieve fusion without intervening connective tissue between the implant and bone, the effects of force applied directly on lamellar bone were evaluated histologically. The absence of a cellular response suggested that the osteocytes were not directly stimulated or that there was insufficient stimulation to initiate apposition or resorption. Perhaps a specific threshold level of stimulation of the investing tissues of bone was necessary to induce a cellular response. An attempt to explain the absence of a cellular response on the basis of bioelectric phenomena found in bone under stress was presented.
REFERENCES 1. Armitage, J., Natiella, J., Greene, G., and Meenaghan, M.: An evaluation of early bone changes after the
insertion of metallic endosseous implants into the jaws of rhesus monkey, Oral Surg. 32: 558-568, 1971. 2. Bassett, C. A. L.: Biologic effect of piezoelectricity, Calcif. Tissue Res. 1: 252-272, 1968. 3. Bassett, C. A. L.: In Bourne, G. (editor): The Biochemistry and Physiology of Bone, ed. 2, New York,
1971, Academic Press, Inc. 4. Burstone, C. J.: The biomechanics of tooth movement. In Kraus, B. S., and Riedel, R. A. (editors): Vistas
in orthodontics, Philadelphia, 1962, Lea & Febiger. 5. Clark, A. E., Hench, L. L., and Paschall, H. A.: The influence of surface chemistry on implant interface
histology, J. Biomed. Mater. Res. Symp. 10: 161.174, 1976. 6. Cochran, G. V. B., Pawluk, R. J., and Bassett, C. A. L.: Stress generated electric potentials in the
mandible and teeth, Arch. Oral Biol. 12: 917-920, 1967. 7. Collier, J. P.. Colligan, G. A., and Brown, S. A.: Bone ingrowth into dynamically loaded porous-coated
intramedullary nails, J. Biomed. Mater. Res. Symp. 10: 485.492, 1976. 8. Cotton, L. A.: Slow maxillary expansion: Skeletal versus dental response to low magnitude force inMacacu
mulatfa, AM. J. ORTHOD. 73: l-23, 1978.
9. Currey, J. D.: The adaptation of bones to stress, J. Theoret. Biol. 20: 91.106, 1968. 10. Frost, H. M.: The laws of bone structure, Springfield, Ill., 1964, Charles C Thomas Publisher. 11. Greenspan, D. C., and Hench, L. L.: Chemical and mechanical behavior of bioglass-coated alumina, 1.
Biomed. Mater. Res. Symp. 10: 503-509, 1976. 12. Grenoble, D. E., and Kim, R. L.: Progress in the evaluation of a vitreous carbon endosteal implant, Ariz.
Dent. J. 19: 12-44, 1973. 13. Griss, P., Greenspan, D. C., Heimke, G., Krempien, B., Buchinger, R., Hench, L. L., and Jentschura, G.:
Evaluation of a bioglass-coated AlaO, total hip prosthesis in sheep, J. Biomed. Mater. Res. Symp. 10: 511-518, 1976.
14. Griss, P., Silber, R., Merkle, B., Hachner, K., Heimke, G., and Krempien, B.: Biomechanical induced tissue reactions after Al,O,-ceramic hip joint replacement: Experimental and early clinical results, J. Biomed. Mater. Res. Symp. 10: 519-528, 1976.
15. Hench, L. L., and Paschall, H. A.: Direct chemical bond of bioactive glass-ceramic materials to bone and muscle, J. Biomed. Mater. Res. Symp. 7: 25-44, 1973.
16. Hench, L. L., and Paschall, H. A.: Histochemical response at a biomaterial interface, J. Biomed. Mater. Res. Symp. 8: 49-64, 1974.

36 Smith Am. J. Orhu. Dr1 crnhrr 1979
17. Hench, L. L., Splinter, R. J., Allen, W. C., and Greenlee, T. K.: Bonding mechanisms at the interface of ceramic prosthetic materials, J. Biomed. Mater. Res. Symp. 2: 117-141, 1972.
l8. Hicks, E. P.: Slow maxillary expansion: A clinical study of the skeletal versus dental response to low magnitude force, A&l. J. ORTHOD. 73: 121.141, 1978.
19. Hixon, E. H., Aasen, T. 0.) Arango, J., Clark, R. A., Klosterman, R., Miller, S., and Odom, W. M.: On force and tooth movement, AM. J. ORTHOD. 57: 476-489, 1970.
20. Hodosh, M., Shklar, C., and Povar, M.: The totally self-supporting tooth replica polymer implant, Oral Surg. 33: 1022-1030, 1972.
21. Holt, D. B., Muir. M. D., Grant, P. R., and Boswarva, I. M.: Quantitative scanning electron microscopy, London, 1974, Academic Press.
22. Kokich, V. G.: Age changes in the human frontozygomatic suture from 20 to 95 years, AM. J. ORTHOD. 69: 41 I-430, 1976.
23. McElhaney, J. H.: The charge distribution on the human femur due to loading, J. Bone Joint Surg. 49A: 1561-1591, 1967.
24. Merrill, 0. M.: The calcification pattern of the developing permanent dentition of the Mucacu nernrstn’nu monkey as related to chronological age, M.S.D. thesis, University of Washington, 1968.
25. Miroue, M. A., and Rosenberg, L.: The human facial sutures: A morphologic and histologic study of age changes from 20 to 95 years, M.S.D. thesis, University of Washington, 1975.
26. Mitchell, D. L., and West. J. D.: Attempted orthodontic movement in the presence of suspected ankylosis, AM. J. ORTHOD. 68: 404-411, 1975.
27. Niles, J. L., and Lapitsky, M.: Biomechanical investigations of bone-porous carbon and porous metal interfaces, J. Biomed. Mater. Res. Symp. 7: 63-84, 1973.
28. Peters, W. J., Jackson. R. W., Iwano. K., and Smith, D. C.: The biological response to zinc polyacryiate cement, Clin. Orthop. 88: 228.233, 1972.
29. Piotrowski, G., Hench, L. L.. Allen, W. C.. and Miller, Cl. J.: Mechanical studies of the bone-bioglass interfacial bone, J. Biomed. Mater. Res. Symp. 9: 47-61, 1975.
30. Reitan, K.: Some factors determining the evaluation of forces in orthodontics, AM. J. ORTHOD. 43: 32-45, 1957.
31. Reitan, K.: Tissue behavior during orthodontic tooth movement; AM. J. ORTHOD. 46: 881-900. 1960. 32. Salzmann, J. A.: Principles of orthodontics, ed. 4, Philadelphia, 1966, J. B. Lippincott Company. 33. Stanley, H. R., Hench, L. L., Going, R., Bennett, C., Chellcini, S. J., King, C., Ingersole. N., Ethridge,
E., and Kreutziger, K.: The implantation of natural tooth form bioglasses in baboons, Oral Surg. 42: 339-356, 1976.
34. Storey, E., and Smith, R.: Force in orthodontics and its relation to tooth movement, Aust. J. Dent. 56: 1 l-18, 1952.
35. Strang, R. W., and Thompson, W. M.: Textbook of orthodontia, ed. 8, Philadelphia, 1958, Lea & Febiger. 36. Utley, K. R.: The activity of alveolar bone incident to orthodontic tooth movement as studied by
oxytetracycline-induced fluorescence, AM. J. ORTHOD. 54: 167-201, 1968. 37. Van Ness, A. L.: Cephalometric roentgenography for nonhuman primates utilizing a surgically implanted
head positioner, Am. J. Phys. Anthropol. 43: 141-148, 1975. 38. Zengo, A. N., Bassett, C. A. L., Pawluk, R. J., and Prountzos, G.: “In viva” bioelectric potentials in the
dentoalveolar complex, AM. J. ORTHOD. 66: 130-139, 1974. 39. Zengo, A. N., Pawluk, R. J., and Bassett, C. A. L.: Stress-induced bioelectric potentials in the dentoalveo-
IX complex, AM. J. ORTHOD. 64: 17-27, 1973.