Embed Size (px)
Citation preview
Blunt and penetrating neck injury
referenceB.J.Bailey ,et al. Head & Neck surgery
Otolaryngology.4th edition.2006 Charles W . Cummings, et al, Cummings
Otolaryngology, Head & Neck Surgery, 5th ed . 2010
D.V. Feliciano ,et al. Trauma, 6th Edition.2008
www.google.com

Zones of the Neck.Zone I: thoracic
inlet to cricoid cartilage
Zone II: cricoid cartilage to the angle of mandible
Zone III: angle of the mandible to skull base
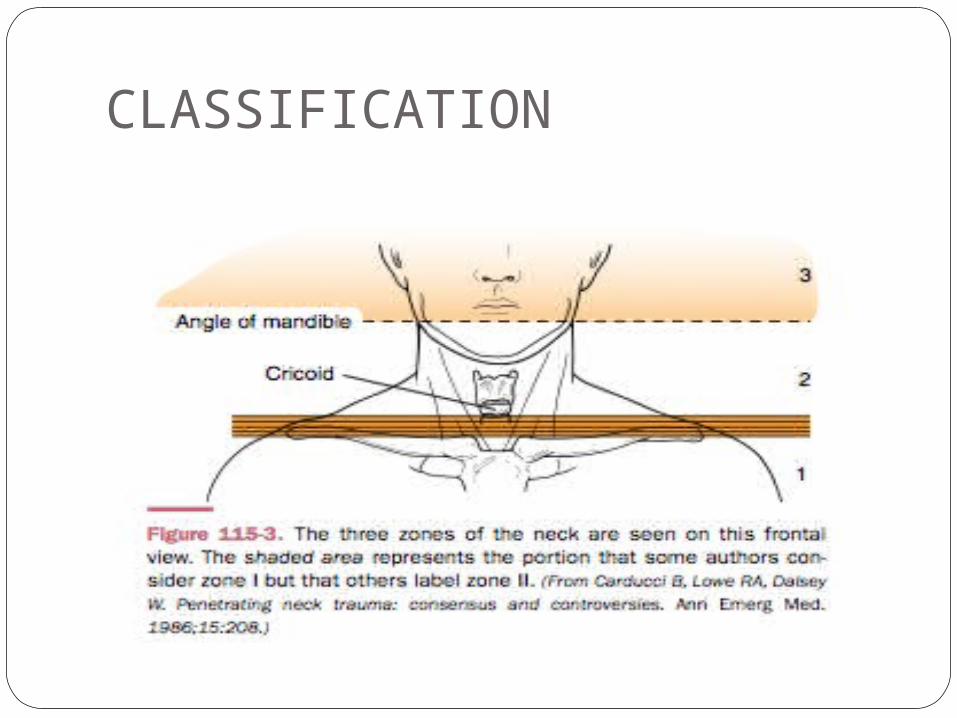
CLASSIFICATION
Zone IFrom the clavicles to the
cricoid Trachea Lungs Proximal carotid and
vertebral arteries Jugular veins Thoracic Vessels Esophagus
Superior Mediastinum Thoracic Duct Spinal Cord Brachial Plexus
Zone IIFrom cricoid to angle of mandibleTracheaLarynxCarotid and vertebral aa.Jugular VeinEsophagusSpinal Cord
Zone IIIAngle of mandible to base of skull
Distal carotid and vertebral arteriesPharynx Spinal cord
PENETRATING NECK TRAUMAPresently, penetrating neck injury
comprises 5% to 10% of all trauma cases. All penetrating neck wounds are
potentially dangerous and require emergency treatment.
Physical properties of penetrating objectshandgunRifleShotgunsKnife and stab injuries
Physical properties of penetrating objectsKinetic energy= ½ mv2
m = massV = velocity
Degree of woundFirearm
Low velocity ( < 1,000 ft/sec) handgun 300-800 ft/sec
high velocity ( > 1,000 ft/sec) shotgun 1,200 ft/sec , rifle 2,200 ft/sec
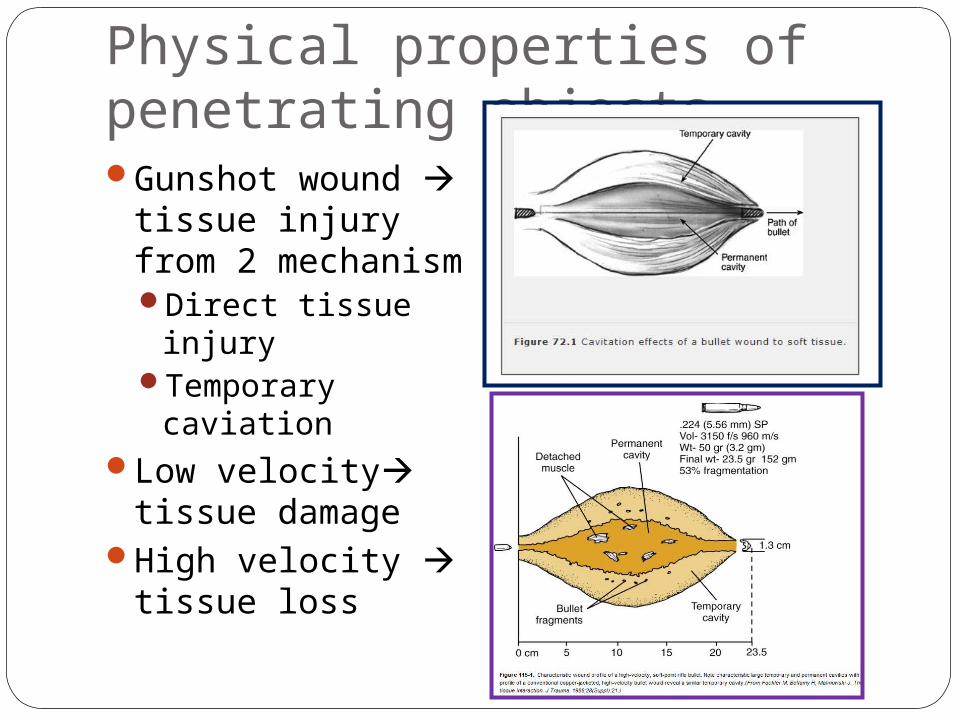
Physical properties of penetrating objectsGunshot wound
tissue injury from 2 mechanismDirect tissue injuryTemporary
caviationLow velocity
tissue damageHigh velocity
tissue loss
KNIFE and STABKnife, ice-pick, cut-glass, or razor-blade more predictable pathwayssingle-entry wound may be from multiple stab
woundscervical stab wounds have a higher incidence of
subclavian vessel laceration because stabbings to the neck often occur in a downward direction with the knife slipping over the clavicle and into the subclavian vessels.
spinal injuries, neck stab wounds have a lower incidence than cervical bullet wounds.
Genaral trauma principleA : airway with C-spine controlB : breathing and ventilationC : circulationD : disability and neurologic statusE : exposure and evaluation other injury
A : AirwayMost casecarefully
intubated transorallyIf C –spine injury is
suspected intubate with neck stabilized
Unstable airway with sig. bleed or edema in oral cavity or pharynx cricothyroidotomy or urgent tracheostomy
A : AirwayMultiple blind intubation attempts will risk
enlarging a lacerated piriform sinus wound and extending it iatrogenically into the mediastinum.
Tracheal tear may be exacerbated by extending the neck
A : AirwayObvious tracheal
injury carefully intubated through entry wound using armored/reinforced ETT
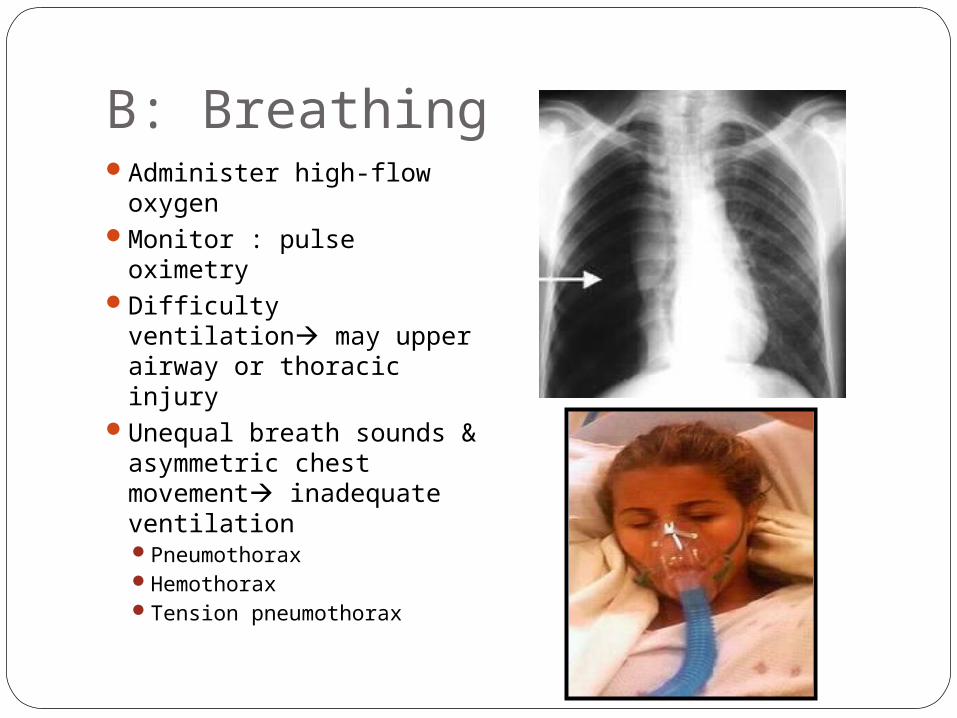
B: BreathingAdminister high-flow
oxygenMonitor : pulse oximetryDifficulty ventilation
may upper airway or thoracic injury
Unequal breath sounds & asymmetric chest movement inadequate ventilationPneumothoraxHemothoraxTension pneumothorax
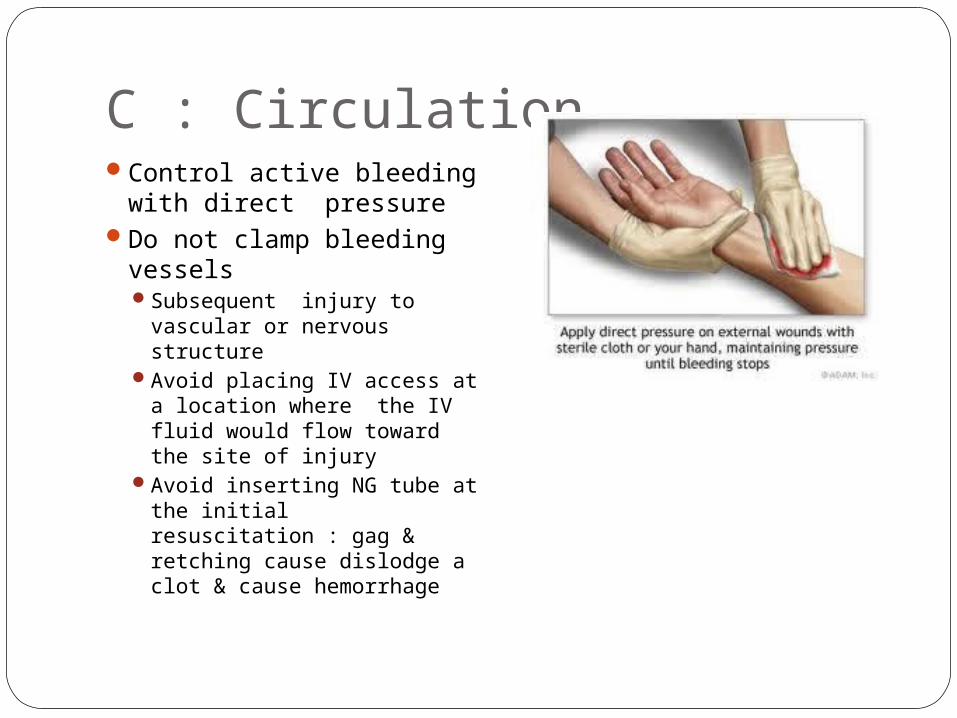
C : CirculationControl active bleeding
with direct pressureDo not clamp bleeding
vesselsSubsequent injury to
vascular or nervous structure
Avoid placing IV access at a location where the IV fluid would flow toward the site of injury
Avoid inserting NG tube at the initial resuscitation : gag & retching cause dislodge a clot & cause hemorrhage
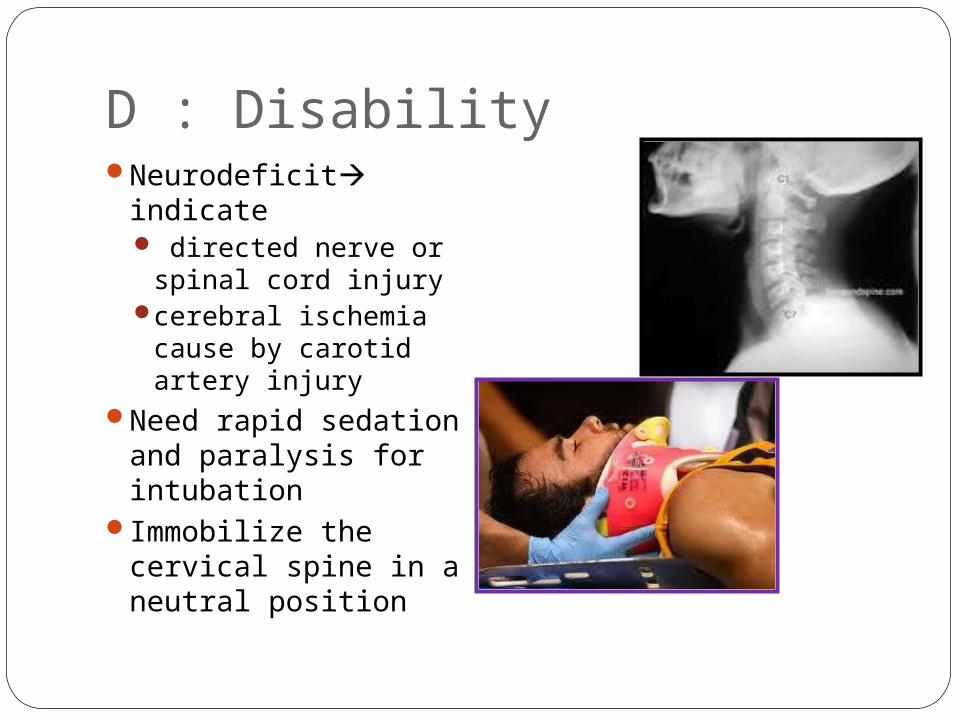
D : DisabilityNeurodeficit indicate
directed nerve or spinal cord injury
cerebral ischemia cause by carotid artery injury
Need rapid sedation and paralysis for intubation
Immobilize the cervical spine in a neutral position
Vital structures of the neck four groups: the air passages (trachea, larynx, pharynx,
lung); vascular (carotid, jugular, subclavian,
innominate, aortic arch vessels);gastrointestinal (pharynx, esophagus)neurologic (spinal cord, brachial plexus,
peripheral nerves, cranial nerves [CNs])
SYMPTOMAirway
Reparatory distress
Stridor HemoptysisHoarsenessTracheal deviationSubcutaneous
emphysemaSucking wound
Vascular System HematomaPersistent bleeding Neurologic deficitAbsent pulseHypovolemic shock BruitThrill Change of
sensorium
From Stiernberg C, Jahrsdoerfer RA, Gillenwater A, et al. Gunshot wounds to the head and neck. Arch Otolaryngol Head Neck Surg. 1992;118:592
SYMPTOMNervous System Hemiplegia
Quadriplegia Coma Cranial nerve deficit Change of sensorium Hoarseness
Esophagus/Hypopharynx
Subcutaneous emphysema Dysphagia Odynophagia Hematemesis Hemoptysis Tachycardia Fever
From Stiernberg C, Jahrsdoerfer RA, Gillenwater A, et al. Gunshot wounds to the head and neck. Arch Otolaryngol Head Neck Surg. 1992;118:592
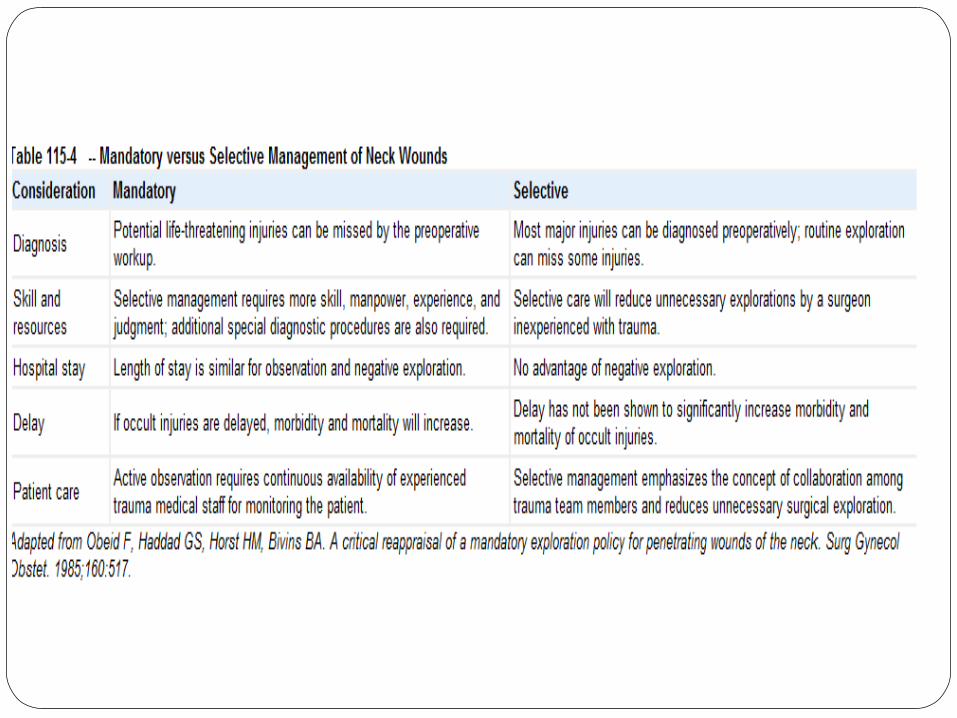
Mandatory versus Elective ExplorationImmediately life threatening: massive
bleeding, expanding hematoma, hemodynamic instability, hemomediastinum, hemothorax, and hypovolemic shock.Immediate surgical exploration
Hemodynamically stable ,non–life-threatening features can undergo thorough imaging investigations to determine the extent of injury.

Injury
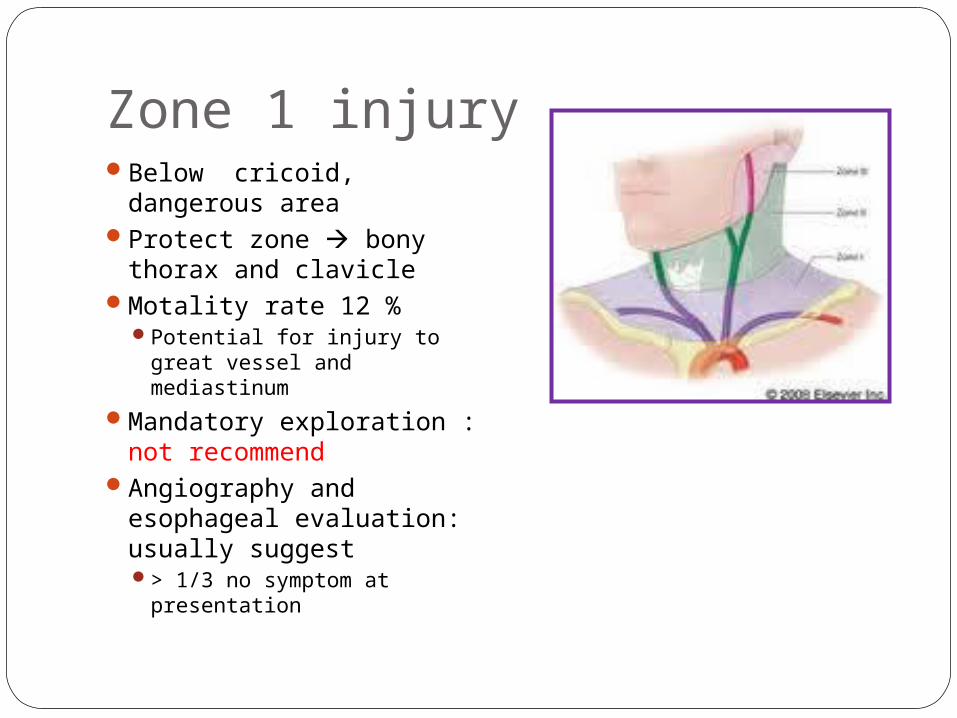
Zone 1 injuryBelow cricoid,
dangerous areaProtect zone bony
thorax and clavicleMotality rate 12 %
Potential for injury to great vessel and mediastinum
Mandatory exploration : not recommend
Angiography and esophageal evaluation: usually suggest> 1/3 no symptom at
presentation
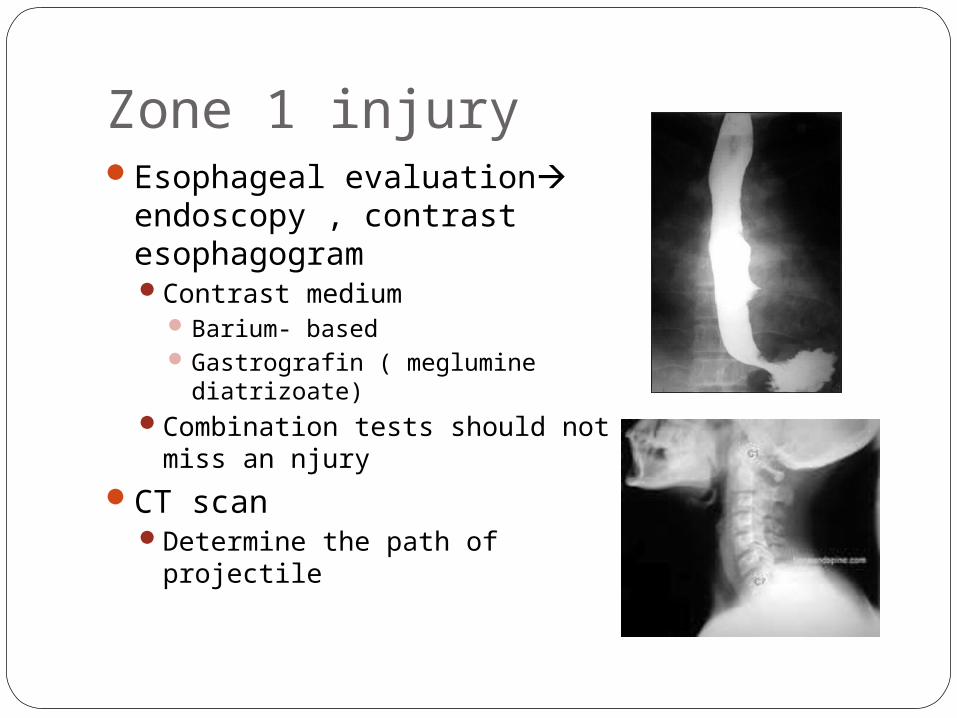
Zone 1 injuryEsophageal evaluation
endoscopy , contrast esophagogramContrast medium
Barium- basedGastrografin ( meglumine
diatrizoate)Combination tests should not
miss an njuryCT scan
Determine the path of projectile
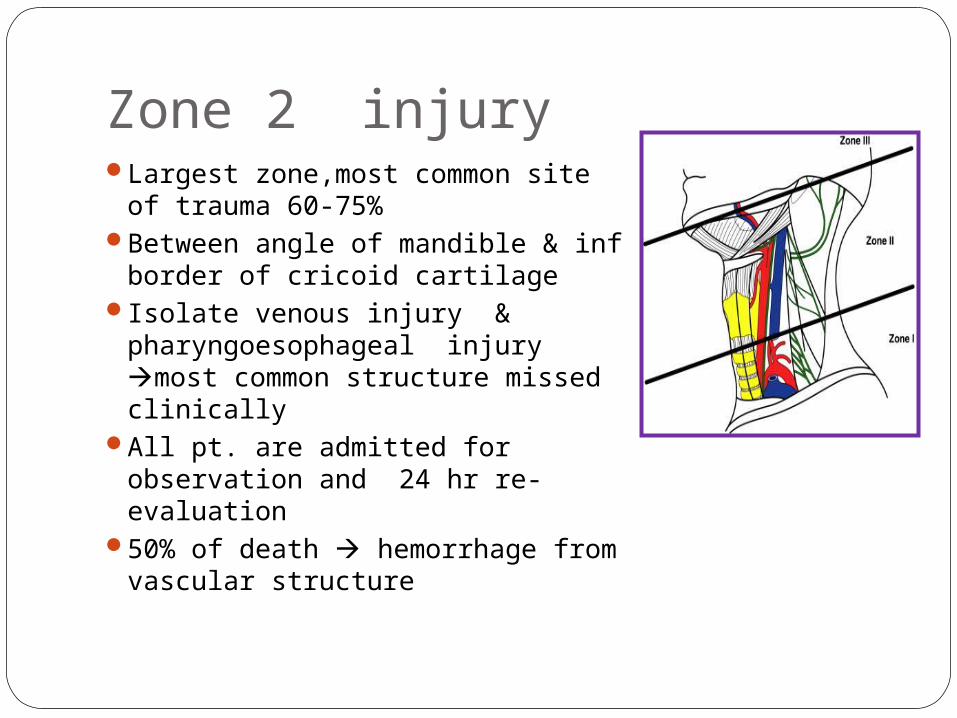
Zone 2 injuryLargest zone,most common site
of trauma 60-75%Between angle of mandible & inf
border of cricoid cartilageIsolate venous injury &
pharyngoesophageal injury most common structure missed clinically
All pt. are admitted for observation and 24 hr re-evaluation
50% of death hemorrhage from vascular structure
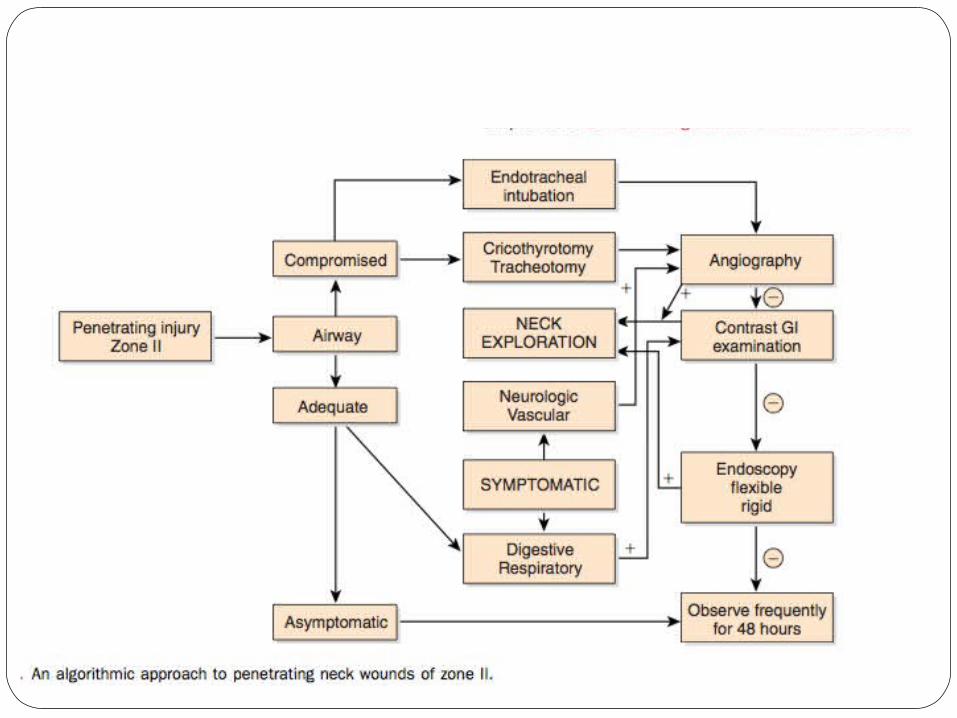
Zone 2 injurySymptomatic neck explorationAsymptomatic
Directed evaluation and serial examArteriography,Laryngotraheoscopyflexible esophagoscopybarium swallowRequires adequate physician ,24 hr facility
prepared for emergency testing and Surgery
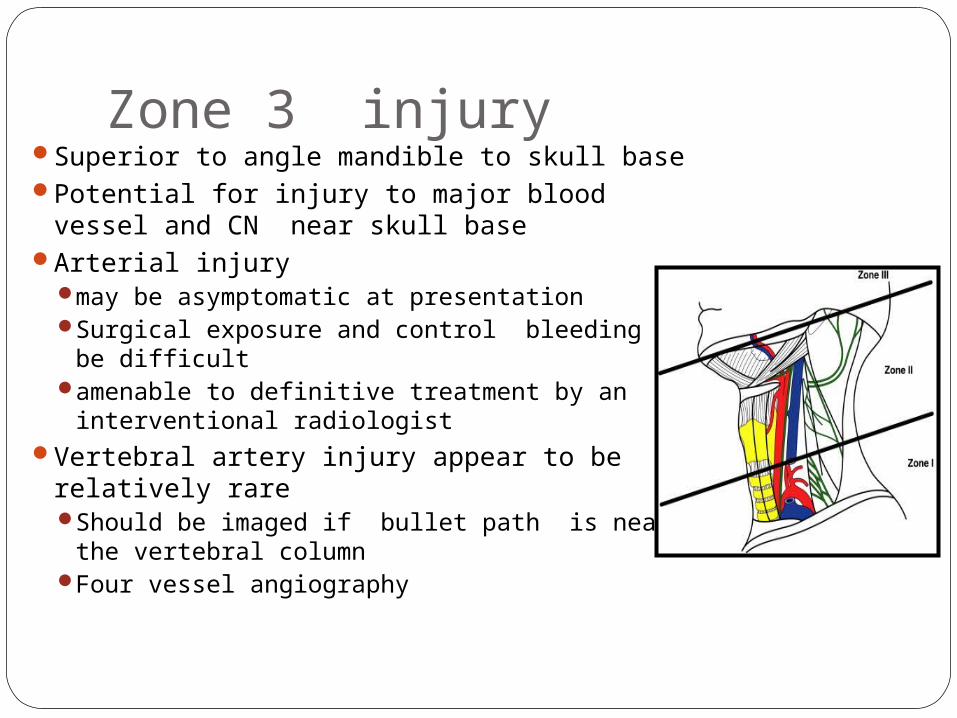
Zone 3 injurySuperior to angle mandible to skull basePotential for injury to major blood vessel and
CN near skull baseArterial injury
may be asymptomatic at presentationSurgical exposure and control bleeding may be
difficultamenable to definitive treatment by an
interventional radiologistVertebral artery injury appear to be relatively
rare Should be imaged if bullet path is near the
vertebral column Four vessel angiography


Angiography: Zone1 & 3Routine preoperative arteriography in
stable caseSurgical approach is more difficult than
zone 2If wound involve both side of neck ( stable
but symptomatic) four vessel angiography

Angiography: Zone1 & 3
Angiography: Zone2Easy accessible,low risk for explorationCertain indication for an angiogram in zone 2
Stable pt. who has persistent hemorrhageNeurodeficit compatible with adjacent vascular
structure damage eg. Horner’s syndrome , hoarseness
Need explorationPositive arteriographyNegative arteriography but positive clinical sign
Asymptomatic in zone 2 Controversy,
No sig difference btw. Clinical exam & angiographyCTA fast ,minimal invasive in hemostatic stable
Management of vascular injuryzone 1Vascular
perforation requires thoracic Sx Mediastinotomy
extension or formal lateral thoracotomy
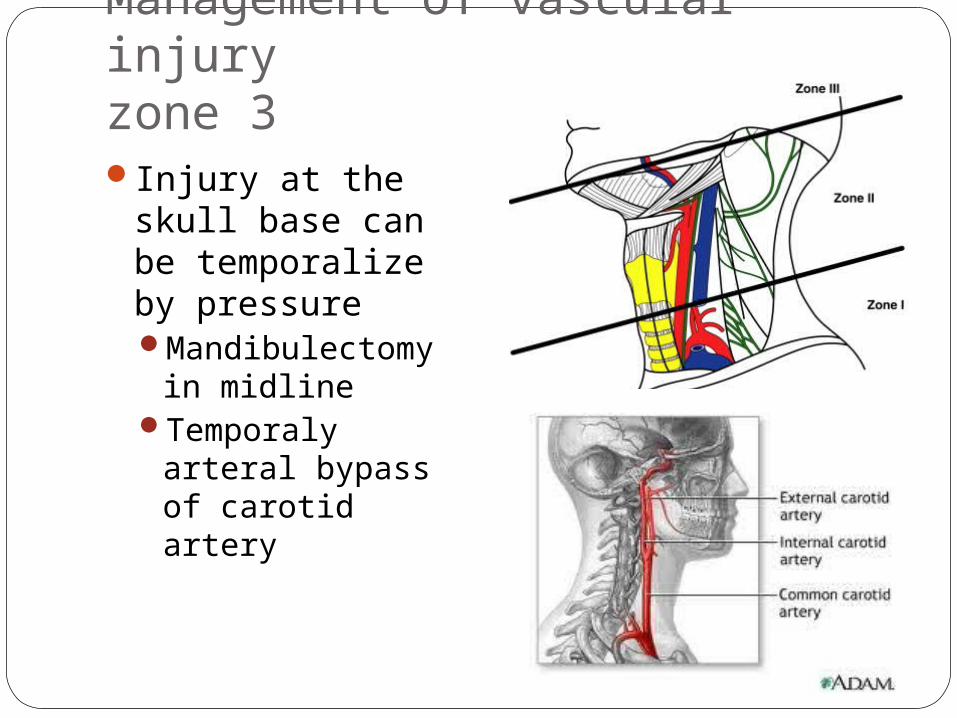
Management of vascular injuryzone 3Injury at the skull
base can be temporalize by pressureMandibulectomy in
midlineTemporaly arteral
bypass of carotid artery
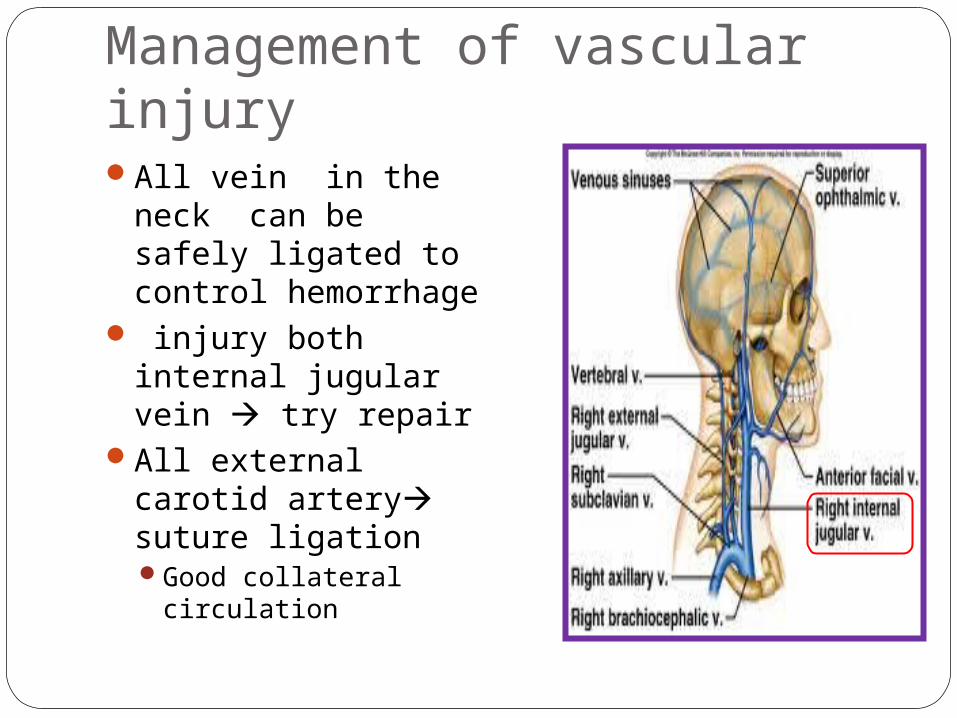
Management of vascular injuryAll vein in the neck
can be safely ligated to control hemorrhage
injury both internal jugular vein try repair
All external carotid artery suture ligationGood collateral
circulation
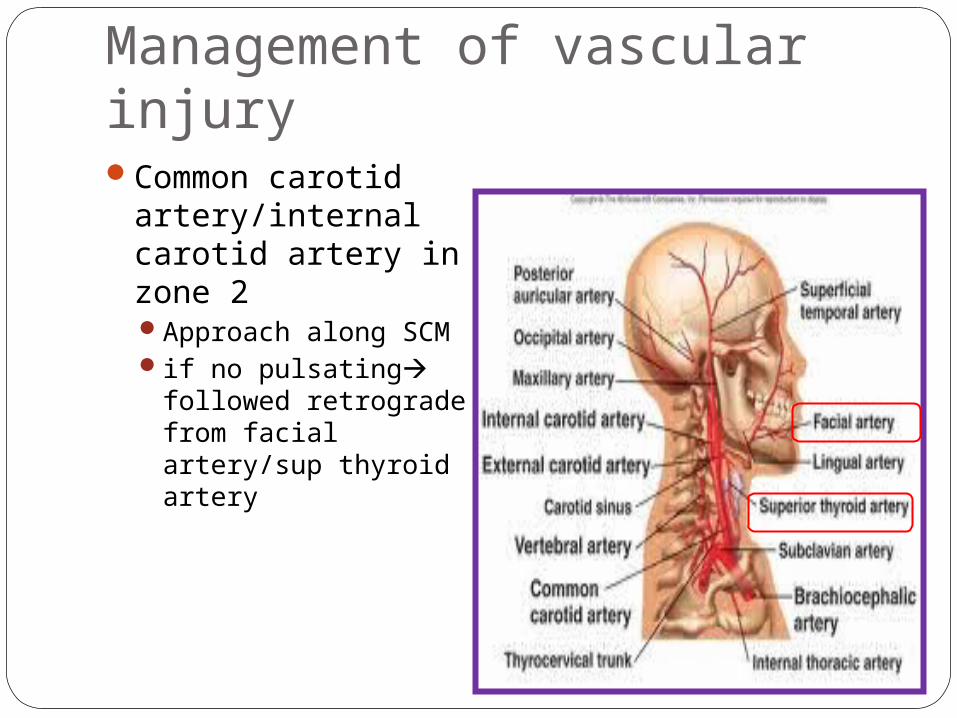
Management of vascular injuryCommon carotid
artery/internal carotid artery in zone 2 Approach along SCMif no pulsating
followed retrograde from facial artery/sup thyroid artery
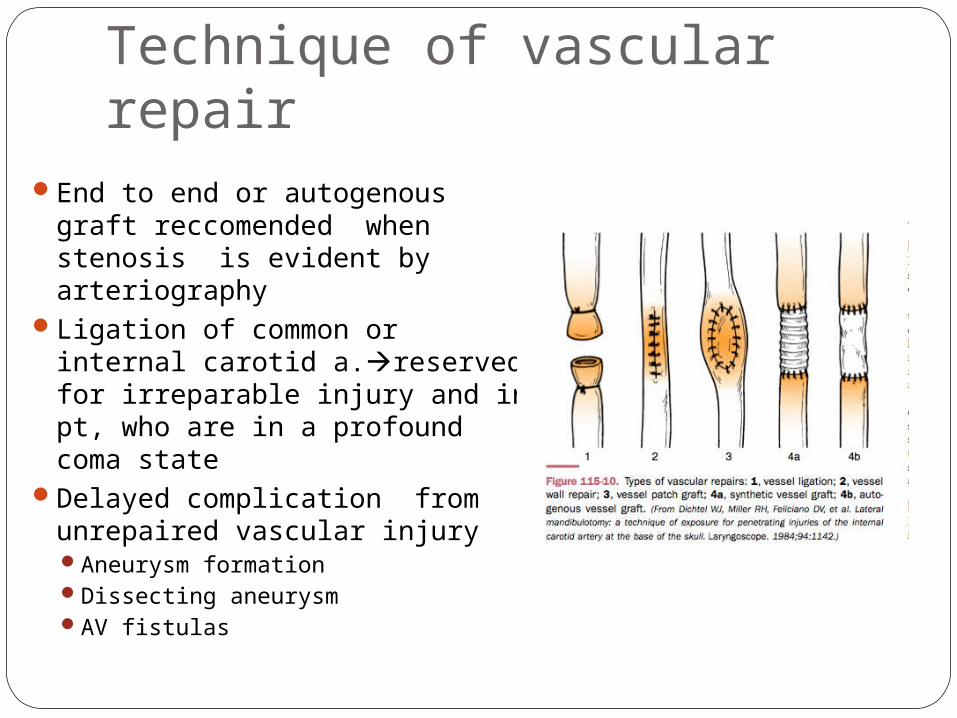
Technique of vascular repairEnd to end or autogenous graft
reccomended when stenosis is evident by arteriography
Ligation of common or internal carotid a.reserved for irreparable injury and in pt, who are in a profound coma state
Delayed complication from unrepaired vascular injury Aneurysm formationDissecting aneurysmAV fistulas
Technique of vascular repairIntervention radiologists used angiography
technique to treat vascular injury Embolization Zone 3 high incidence of multiple vascular
injury eventComplication of intervention angiography
Blood vessel injuryInadvertent balloon detachmentIschemic eventsPseudoaneurysm formationTreatment failure

Pharynx and esophageal injuryClinical sign and symptom neck exploration
subcutaneous emphysemaHematemesisHypopharyngeal blood
>50%of Pt. asymptomatic at presentationCombination of esophagoscopy and contrast
esophagographyMost sensitive for detected injury
Delayed explore & repair beyond 24 hrs after injury poorer outcome
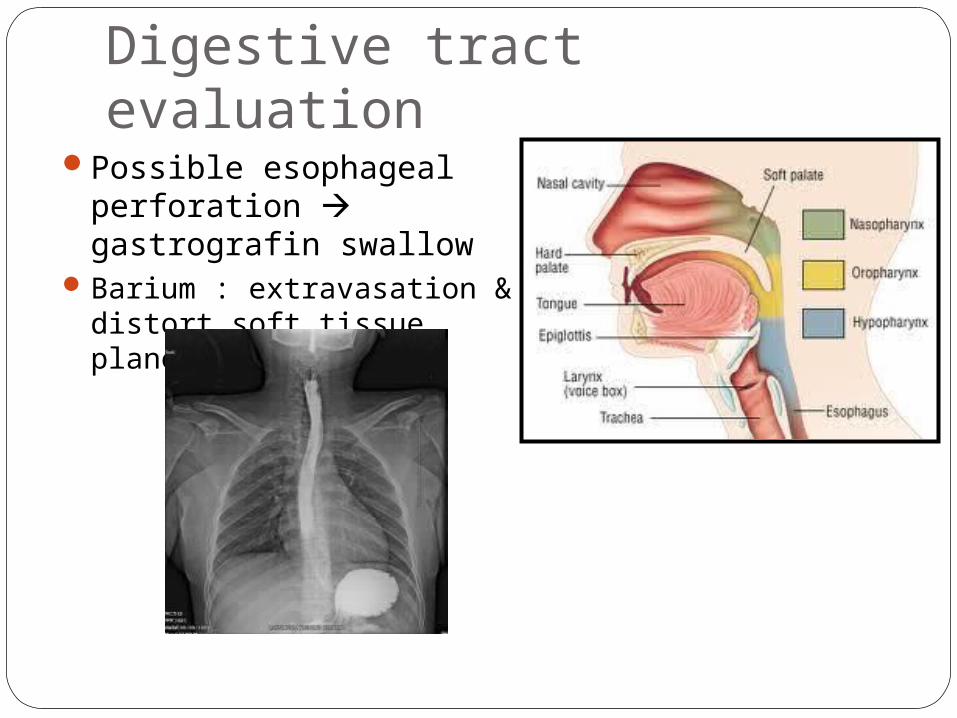
Digestive tract evaluationPossible esophageal
perforation gastrografin swallow
Barium : extravasation & distort soft tissue plane and toxic
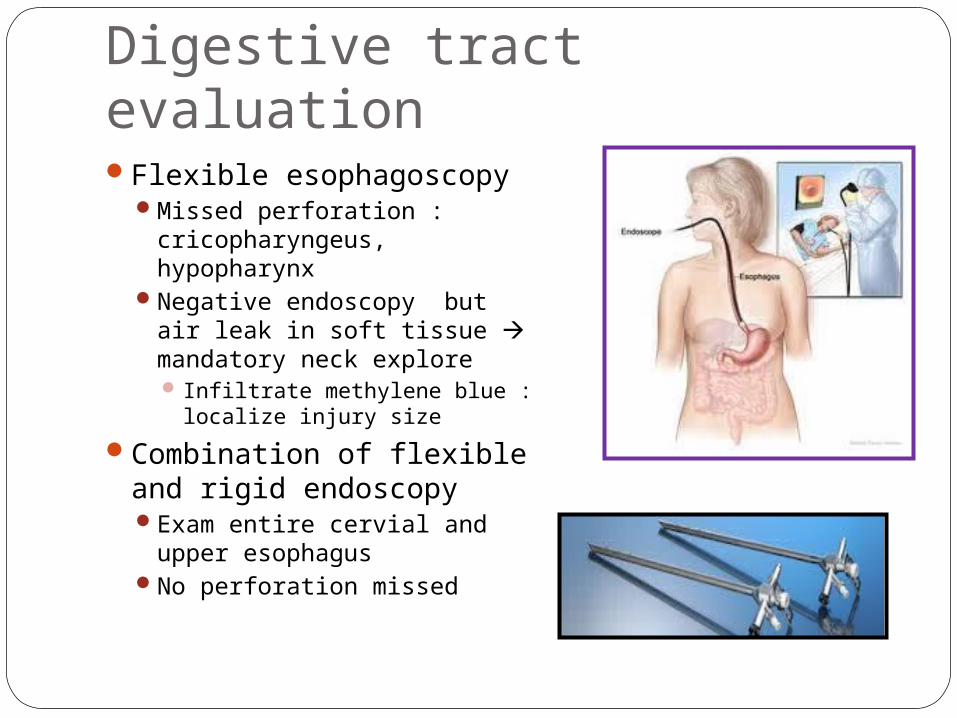
Digestive tract evaluationFlexible esophagoscopy
Missed perforation : cricopharyngeus, hypopharynx
Negative endoscopy but air leak in soft tissue mandatory neck explore Infiltrate methylene blue :
localize injury size
Combination of flexible and rigid endoscopyExam entire cervial and
upper esophagusNo perforation missed
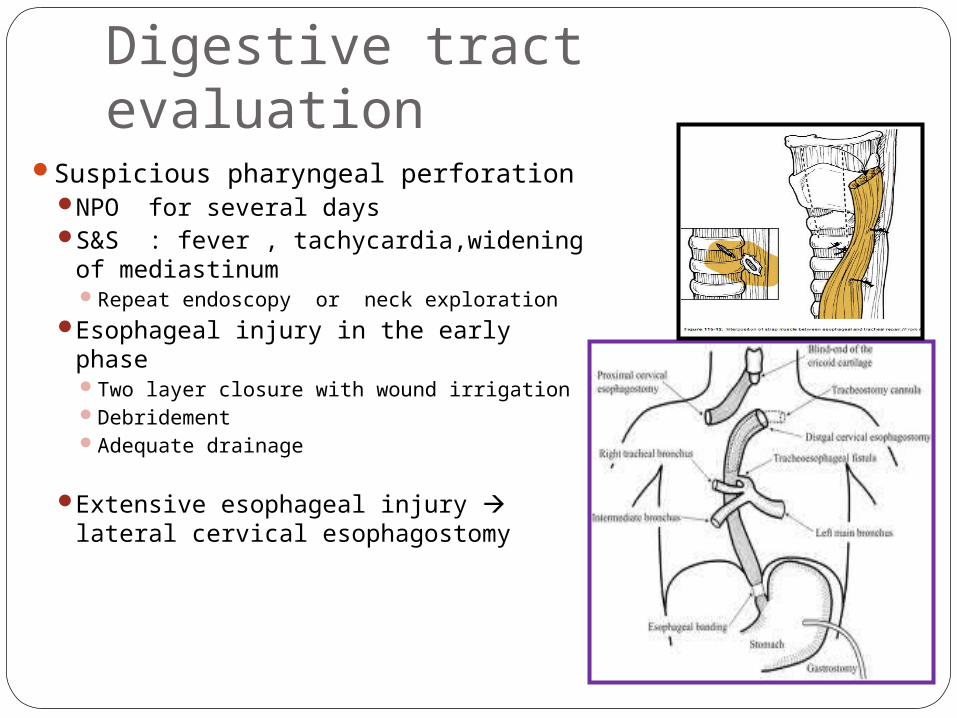
Digestive tract evaluationSuspicious pharyngeal perforation
NPO for several daysS&S : fever , tachycardia,widening of
mediastinumRepeat endoscopy or neck exploration
Esophageal injury in the early phaseTwo layer closure with wound irrigationDebridementAdequate drainage
Extensive esophageal injury lateral cervical esophagostomy
Digestive tract evaluationC-spine fx omitted rigid esophagoscopyClinical exam
F/U exam frequentlyMonitor V/SObserve period 48-72 hrs

Penetrating of hypopharynxSuperior to the level of arytenoid
cartilageIV ABONPO ทางปาก 5-7 daysPrimary closure not always necessary
Inferior to the level of arytenoid cartilageDependent portionExploration with primary watertight
closureUse absorbable suture with drainage of
adjacent neck spaceNPO 5-7 daysTreat liked esophageal injury
TreatmentConservative
Medical therapyAdequate ventilation & oxygenationFluid resuscitationMonitor neurolodic statusPain controlABOTetanus prophylaxis
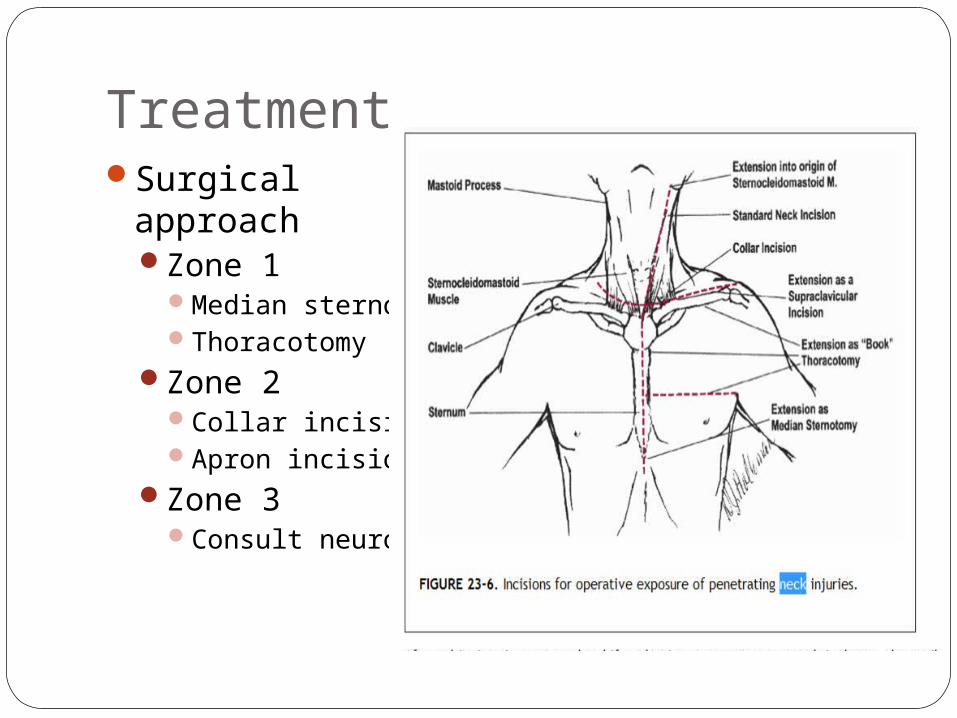
TreatmentSurgical approach
Zone 1Median sternotomyThoracotomy
Zone 2Collar incisionApron incision
Zone 3Consult neuroSx
Blunt neck traumamotor vehicle accidents and sports result in laryngeal, vascular, and digestive
injuryeasily underdiagnosed because their onset
can be delayedoccult cervical spine injury
Blunt neck traumacareful observation : delayed onset
slow progression of airway edema airway obstruction may not occur until several hours
after the injur
CT may be helpful to determine degrees of injury to the larynx and vessels
Blunt neck traumaBlunt injury to the cervical vessels can lead to
thrombosis, intimal tears, dissection, and pseudoaneurysm
Treatment options for blunt artery injuries are based onthe mechanism, type of injury, and location
Blunt neck traumaTreatments for blunt artery injuries include
surgery, anticoagulation, and observation.
Surgical intervention for blunt vascular injuries includes ligation, resection, thrombectomy, and stent placement






























